Cardiovascular Services
The Heart and Beyond:Diseases of theCirculatory System
Mobeen A. Sheikh, M.D.

Cerebrovascular disease• Ischemic stroke• Transient Ischaemic Attack (TIA)
Peripheral arterial disease (PAD)Intermittent claudication
• Pain on walkingSevere limb ischaemia
• Rest pain• Gangrene, necrosis
Cardiovascular disease• Heart Attack• Angina (stable/unstable)
Atherosclerosis affectsall arterial beds
CardiovascularServices

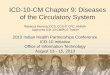
Where does PAD fit?
• Atherosclerosis is commonlyfound in more than onearterial bed
• PAD is often overlooked asone of the manifestations ofatheroscelerosis
PAD
MIStroke
Data from CAPRIE study (n=19,185). Figure adapted from Coccheri S. Eur Heart J 2002; 4 (Suppl B): B46-B49
CardiovascularServices

PAD Prevalence
• 10-12 million in U.S.
• 30% symptomatic
• < 40% treatedHirsch AT, JAMA 2001;286:1317-24.
CardiovascularServices

Ankle Brachial Index (ABI)
Systolic ankle pressure (mm Hg)
Systolic brachial pressure (mm Hg)
•Simple diagnostic tool
•Use Doppler ultrasound probeand sphygmomanometer
•Office based
•Non invasive
•Patient lying flat
CardiovascularServices

Ankle Brachial PressureIndex
High. May be due to arterial wallstiffening, especially in patients withdiabetes
>1.3
Consider referral to vascular specialist ifpatient has classic PAD symptoms
0.9
Confirms PAD diagnosis. Initiatemanagement and consider referral ifquality of life issues
<0.9
Indicates severe disease. Consider referralto vascular specialist
≤0.5
CardiovascularServices

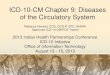
Projected Increasein the Prevalence of PAD
0
2
4
6
8
10
12
14U
.S.I
ndi
vidu
als
(Mill
ion
s)
40-59 60-69 70+ Total
20002020
Prevalence rate: 3% 8% 19%
Chart from the 1999 Advisory Board Company. Source: Criqui NW et al., N Engl J Med (1992); Newman AB et al.,Arteriosclerosis, Thrombosis, and Vascular Biology (1999); U.S. Census Bureau(http://www.census.gov/population/projections/nation/nas)

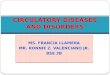
818
2332
39
86
0
20
40
60
80
100
ProstateCancer*
Hodgkin'sDisease
BreastCancer*
PAD ColorectalCancer*
LungCancer*
Pat
ient
s(%
)
*American Cancer Society. Cancer Facts and Figures, 2000.†Criqui MH et al. N Engl J Med. 1992;326:381-6.
Relative 5-Year Mortality Rates
*
†

Cause of Death in PAD Patients
50
25
15
10
0 10 20 30 40 50 60
CAD
nonvascular
CVA
abdominalvascular
* percentage of deathsattributed to a given cause
CardiovascularServices

Increased risk vs general population (%)
Original event Heart Attack Stroke
Heart Attack
Stroke
Peripheral arterial disease
5–7 x greater risk1
(includes death)3–4 x greater risk2
(includes TIA)
2–3 x greater risk2
(includes angina andsudden death*)
9 x greater risk3
4 x greater risk4
(includes only fatal MIand other CHD death†)
2–3 x greater risk3
(includes TIA)
Risk of a Second Vascular EventRisk of a Second Vascular Event
CardiovascularServices

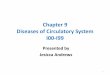
“Global Vascular Care”

Ischemia inIschemia inButtock, hip,Buttock, hip,Thigh and calfThigh and calf
Thigh,Thigh,calfcalf
Calf, ankle,Calf, ankle,footfoot
Obstruction inObstruction inAorta orAorta oriliac arteryiliac artery
Femoral arteryFemoral arteryor branchesor branches
PoplitealPoplitealarteryartery
Common Sites of Claudication

Why Endovascular Therapy?
• Minimally Invasive
• Increased safety
• Patient comfort
• Patient preference
• Less Expensive
• Glamorous
CardiovascularServices

SFASFAInterventionIntervention

SFA Intervention - Nature of the Problem
Contraction
Torsion
Flexion
Compression
CardiovascularServices

Nitinol self-expanding stent
CardiovascularServices

CardiovascularServices

• Unique helical patternenables multi-dimensional flexibility– Bending up to 180°
or twisting withoutkinking
– High radial strength– Low shear stresses
Choosing the Right Stent
CardiovascularServices

VIABAHN™ Endoprosthesis
• ePTFE lining with anexternal nitinol support
• No foreshortening• Easy deployment• 5 – 13 mm diameters• 2.5 – 15 cm lengths• 75 cm and 110 cm
working lengths• 8 Fr to 12 Fr sheaths
required
CardiovascularServices

Alternative Strategies:Debulking First
CardiovascularServices

FoxHollow SilverHawk
• Excises large volumesof plaque from de novoand restenotic lesions
• Single-operator,monorail catheter thatcan treat multifocaland multivesseldisease
SilverHawk System
CardiovascularServices

Magnified Cutter View
CardiovascularServices

Plaque Excised: 293 mg
CardiovascularServices

Renal Artery Stenosis

10 clues to the diagnosis ofRenovascular Disease
• Onset of HTN before 30 or after 55 yrs• Exacerbation of previously well controlled hypertension• Malignant hypertension• Resistant hypertension• Epigastric bruit (sound heard through stethoscope• Unexplained elevation of blood tests for kidney function• Elevation of blood tests for kidney function while
receiving ACE inhibitors• Shrunken kidney or size discrepancy• Atherosclerosis elsewhere• “Flash”pulmonary edema or recurrent CHF






Update on Carotid StentingUpdate on Carotid Stenting

CardiovascularServices

CardiovascularServices

Mednova, Neuroshield
Filter wire, EPI
Angioguard, Cordis
Different types of protection devices
7.5mmRX ACCUNETTM
12 mm

Recommended