THE GERIATRIC GIANTS
MEDICINE 400
Jane Courtney
Hollywood Private Hospital
30th June 2008

Immobility
Instability
Incontinence
Impaired intellect/memory

Impaired vision
Impaired hearing
Delirium
Poly-pharmacy
Care provision

Assessment
Multi-disciplinary
Functional - adl’s
- iadl’s
Problem oriented

FALLS

INCIDENCE
– 30% community dwellers >65 years– 50% long term care– 60% fall in last year

CONSEQUENCES
• 10 –15% fracture• Decrease in functional status• 2% injurious falls result in death
COSTS
• 8% ED presentations >70 years• 33% of these admitted• Median stay 8 days

RISKS
• Rarely single cause

Falls usually occur when a threat to the normal homeostatic mechanisms that maintain postural stability is superimposed on age-related declines in balance,ambulation and cardiovascular function.
Threat
•Acute illness
•Environmental stress
•Unsafe walking surface

RISK FACTORS
• Age• Female• Past fall• Cognitive impairment• Lower limb weakness• Balance disturbance

RISK FACTORS
• Psychotropic meds• Arthritis• Past CVA• Orthostatic hypotension• Dizziness
AGE RELATED FUNCTIONAL DECLINE
• Visual• Proprioceptive• Vestibular

ENVIRONMENT
• FOOTWEAR• HOME MODIFICATIONS• BEHAVIOUR• SAFETY DEVICES• SOCIAL INTEGRATION
DISEASE RELATED FUNTIONAL DECLINE

neurological
• CVA• Parkinsons• Cerebellar• Neuropathy• Dementia• Delerium• Epilepsy

cardiovascular
• Arrythmia• Orthostatic hypotension• Anatomical• Vasomotor instability

GIT
• Bleeding • D&V• Defecation syncope

metabolic
• Hypothyroid• Hypoglycemia• Hypokalemia• hyponatremia
UGS
• Micturition syncope• Nocturia• Incontinence

musculoskeletal
• Arthritis• Myopathy• Deconditioning
Psychiatric
• Anxiety• Depression

medications
• Antihypertensives and cardiac• Antidepressants• Antipsychotics• Benzodiazepines• Levadopa• Narcotics
toxins
• Alcohol

MECHANISM
• SYNCOPE /HYPOTENSION• SEIZURE• DIZZINESS / BALANCE• GAIT DISTURBANCE• PAIN / WEAKNESS• MECHANICAL FALL

FUNCTIONAL IMPAIRMENT
• BP regulation• Central processing• Gait• Neuromotor function• Postural control• Proprioception• Vestibular• vision
EVALUATION
• History esp of fall• Examination esp BP, balance, vision, gait• Get up and go• Divided attention• Tests
PREVENTION
• Strength and balance• Education• Medications• Environmental mods
PREVENT COMPLICATIONS
DEMENTIA
Causes of Cognitive Impairment
J-0
1 Delirium
• Sepsis• Hypoxia• Biochemical disturbancesCalcium, sodium, glucose,urea,hepatic

DEFINITION
• An acute organic mental syndrome characterized by:
• Global cognitive impairment• Reduced consciousness• Disturbed attention• Psychomotor activity• Sleep-wake cycle disturbance

2 Neurological disease
• Brain tumour• Stroke• Subdural
3 Psychiatric Disease
• Depression• Anxiety• Alcohol or other substance abuse

4 Medications

5 “Classics”
• Thyroid• B12• Folate

6 Benign Forgetfulness

7 Dementia

Definition of Dementia• The development of multiple cognitive deficits manifested by both
memory impairment and one or more of the following– Aphasia -Apraxia -Agnosia– Disturbance in executive functioning
• These cognitive deficits cause significant impairment in social or occupational functioning
• The course is characterized by gradual onset and continuing cognitive decline
• The cognitive deficits are not due to other CNS, systemic, or substance-induced conditions
• The deficits do not occur exclusively during the course of a delirium• The disturbance is not better accounted for by another Axis I disorder
A-2
Reference: DSM-IV, pp 133-155.

CRITERIA FOR DIAGNOSIS
• MEMORY IMPAIRMENT• OTHER COGNITIVE IMPAIRMENT
– Language, motor skills, perception• ADL IMPAIRMENT• INSIDIOUS ONSET• DETERIORATING• NO OTHER CAUSE
– Systemic,neurological, psychiatric

CRITERIA FOR DIAGNOSIS
• PATHOLOGY- autopsy or brain biopsy

Comparison delirium and dementia
• Sudden onset• Usually reversible• Short duration• Fluctuations• Altered consciousness• Associated illness• Inattention• Always worse at night• Impaired variable recall
• Insidious onset• Slowly progressive• Long duration• Relatively stable• Normal consciousness• Not associated• Attention not sustained• Can be worse at night• Memory loss
TYPES OF DEMENTIA
• PRIMARY NEURODEGENERATIVE– CORTICAL
• Alzheimer’s disease• Fronto-temporal dementias (Pick’s disease)
– SUBCORTICAL • Progressive supra nuclear palsy• Huntington’s• Lewy Body Disease
TYPES OF DEMENTIA
• VASCULAR– Multi-infarct– Biswangers disease
• INFECTIVE– Creutzfeld-jacob– AIDS– Neurosyphilis

TYPES OF DEMENTIA
• TRAUMA– Sub dural– Dementia pugulistica– radiotherapy
• NORMAL PRESSURE HYDROCEPHALUS

TYPES OF DEMENTIA
• ASSOCIATED WITH OTHER DISEASES– Parkinson’s– Wilson’s– Multiple sclerosis– Tumours– Vasculitis

Alzheimer’s Disease Diagnosis• Acquired decline in cognitive function of an
insidious and progressive nature– Loss of memory – Impairment of at least one of;
• Language• Perception• Praxis• Problem solving, planning, organization• Judgement, insight or abstract thought
– Decline in ability to perform activities of daily living
A-1
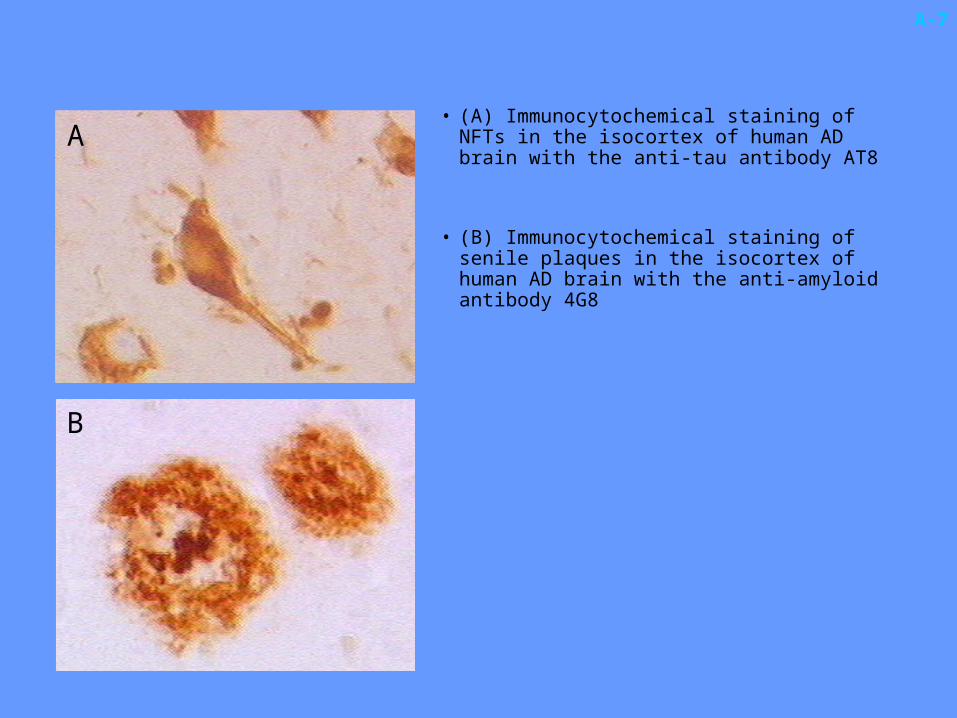
• (A) Immunocytochemical staining of NFTs in the isocortex of human AD brain with the anti-tau antibody AT8
• (B) Immunocytochemical staining of senile plaques in the isocortex of human AD brain with the anti-amyloid antibody 4G8
A-7
A
B

Cholinergic Hypothesis• Role
– Acetylcholine (ACh) is an important neurotransmitter in areas of the brain involved in memory formation (eg. hippocampus, cerebral cortex, and amygdala)
• Impact– Loss of ACh occurs early in AD and correlates with the
impairment of memory• Treatment approach
– Enhancement or restoration of cholinergic function may significantly reduce the severity of cognitive loss
A-9
Reference: Mayeux R, et al. N Engl J Med. 1999;341:1670-1679.

TREATMENT
Overall Management
• Is it Alzheimers? OR what?• Are there any reversible components?• Any specific treatments?• Educate and support carer/family.• Treat symptoms as they arise.• Treat intercurrent problems.

Medications
• Can cause cognitive impairment
• Can treat memory loss (Alzheimer’s, DLB)
• Can treat symptoms
• Can prevent (vascular)

Cause Cognitive Impairment
• Sedatives• Antidepressants• Analgesics• “SIADH”• Antiepileptics• Specials
– Digoxin, cimetidine, lithium.

Treat Memory
• Cholinergics• ?oestrogens• Vitamin E• Selegeline

Treat Symptoms
• Treat family• Non pharmacological• Antipsychotics• Benzodiazepines• ANTIDEPRESSANTS

Drug Utilization Trends in Dementia
T-5
Source: NDTI (Diagnosis codes: 3310, 2900, 2901, 2902, 2903, 2904), 1999.
Numberof Drug
Uses(000)
0
500
1000
1500
1995 1996 1997 1998 1999
AriceptRisperdalHaldolAtivanVitamin EZoloftZyprexa

Feature ComparisonDose
Drug MoA Binding Escalation Dosing
Reminyl® AChEI, Competitive, 4-week steps bdnAChR reversible (od)
Aricept® AChEI Noncompetitive, 4/6-week steps odreversible
Exelon® AChEI Pseudo- 1-week steps bidirreversible
T-10
AD REM 8 59
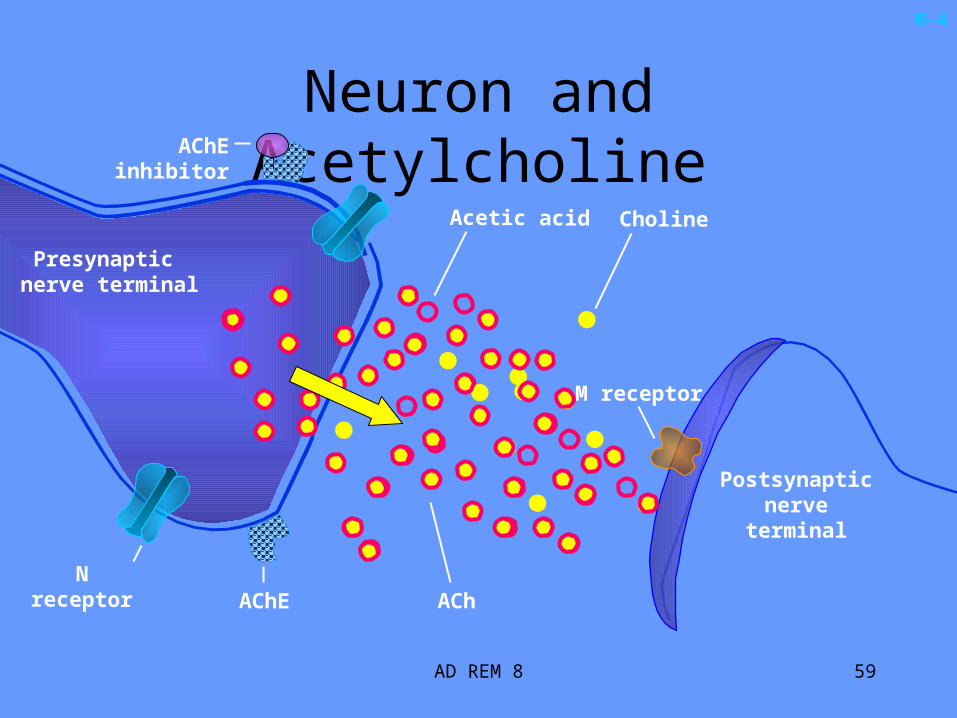
Neuron and Acetylcholine
M-4
Postsynaptic nerve terminal
N receptor
Presynaptic nerve terminal
M receptor
ACh
Acetic acid Choline
AChE
AChE inhibitor
AD REM 8 60
Acetic acid Choline
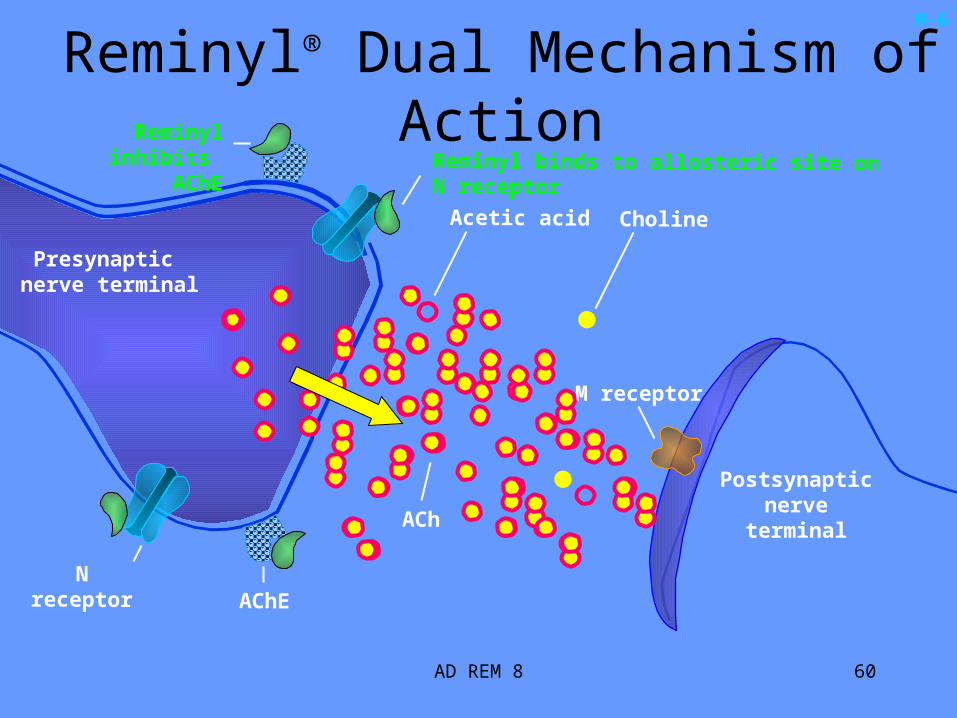
Reminyl® Dual Mechanism of ActionM-6
Postsynaptic nerve terminal
Presynaptic nerve terminal
N receptor
M receptor
ACh
AChE
Reminyl binds to allosteric site on N receptorReminyl inhibits
AChE

INCIDENCE
• 15% - 30% community-dwelling• 30% hospitalized• 50% long-term care
Predisposes to
• Rashes• Pressure sores• Urinary tract infections• Falls• Fractures• Increased risk of institutional care
Incontinence is abnormal at any age.
Prevalence increases with age.
At no age does it affect the majority of individuals.
Even with severe dementia not all people are incontinent
NEW INCONTINENCE MUST BE INVESTIGATED
INCONTINENCE IS A SYMPTOM
• Transient or established.• Urge, stress or overflow.• Clinical.

Transient• D delirium• I infection• A atrophic vaginitis• P pharmaceuticals• P psychological (depression)• E excessive output• R restricted mobility• S stool impaction
pharmaceuticals• Anticholinergics • Alpha agonists (men)• Alpha antagonists (women)• Calcium channel blockers• ACE inhibitors (cough)• Diruretics• Sedatives (and alcohol)
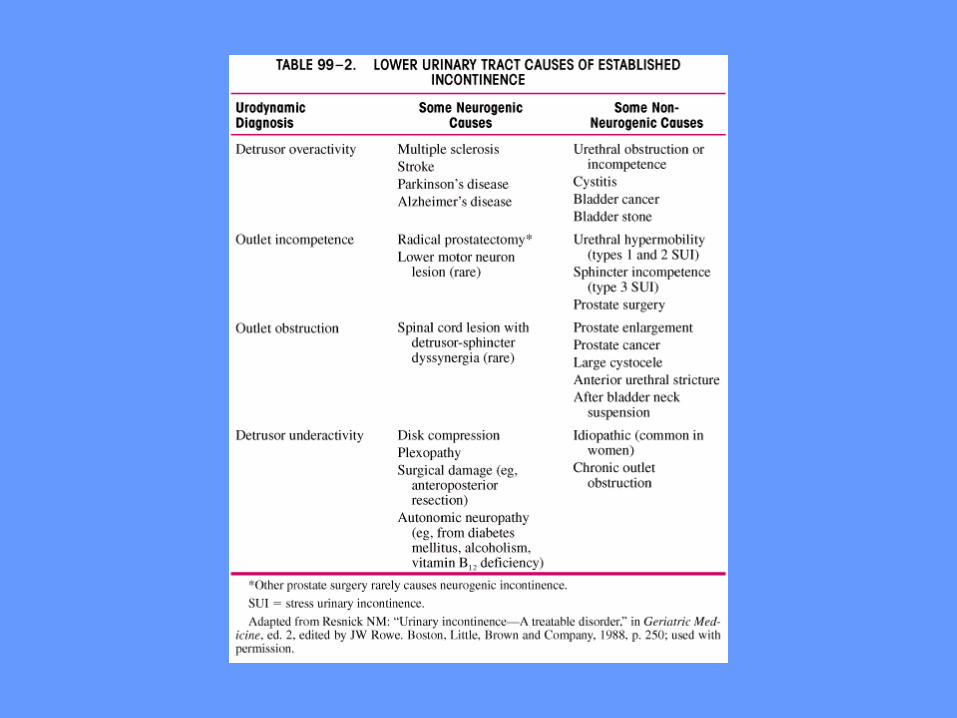
Established
Patho-physiological mechanismsdetrusor overactivitydetrusor underactivityobstructionoutlet incontinence
Each can be either neurogenic or non-neurogenic


WHAT DO WE DO?
HISTORY
EXAMINATION
INVESTIGATIONS.

TYPE
FREQUENCY
PATTERN
MEDICAL
MEDICATIONS
FUNCTION

FULL PHYSICAL….GUIDED
PELVIC
RECTAL
NEUROLOGICAL
STRESS

VOIDING CHART
U&E, CALCIUM, GLUCOSE
URINALYSIS+/- MSU
RESIDUAL VOLUME
ULTRASOUND
URODYNAMICS
CYSTOSCOPY

TREATMENT
FIRST THE CAUSE IN TRANSIENT
STRESS- PELVIC FLOOR EXERCISES
- WEIGHT LOSS
- OESTROGEN
- SURGERY
OBSTRUCTION - ALPHA ANTAGONIST
- SURGERY
DO - ANTICHOLINERGIC
DU - CATHETER
PADS, BOTTLES, COMMODES

A LAST WORD ABOUT POLYPHARMACY
THE GERIATRICIAN’S PEN
v’s A BALANCING ACT
Recommended