D r J u d i t h T a y l o r 1 , D r L a t a n a M u n a n g 2
1 N H S T a y s i d e , S c o t l a n d 2 N H S L o t h i a n , S c o t l a n d
The General Practitioner Assessment of Cognition (GPCOG): A Systematic
Review
Background
Early diagnosis and recognition of dementia
Characteristics of the ideal cognitive screening test?
Copyright issues with Mini Mental State Examination (MMSE)
GPCOG
Tool developed for dementia screening in a community population
Freely available online www.gpcog.com.au
Comprises 2 Steps 1) Cognitive Assessment
2) Informant Report
Longitudinal history
Step 1: Cognitive Test
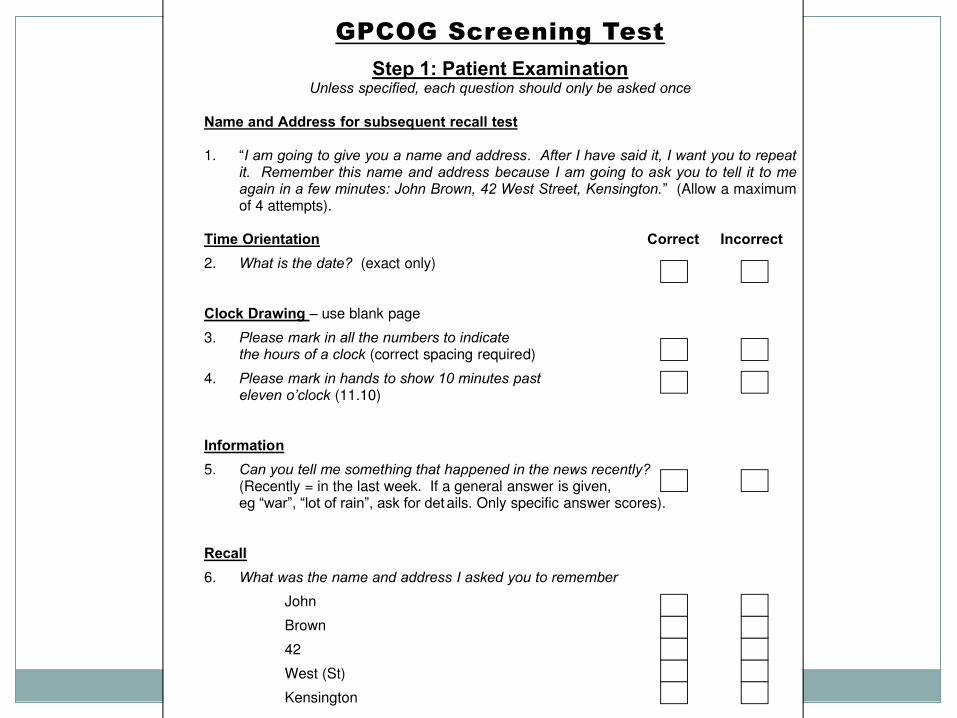
GPCOG Screening Test
Step 1: Patient Examination Unless specified, each question should only be asked once
Name and Address for subsequent recall test 1. “I am going to give you a name and address. After I have said it, I want you to repeat
it. Remember this name and address because I am going to ask you to tell it to me again in a few minutes: John Brown, 42 West Street, Kensington.” (Allow a maximum of 4 attempts).
Time Orientation Correct Incorrect
2. What is the date? (exact only) Clock Drawing – use blank page
3. Please mark in all the numbers to indicate the hours of a clock (correct spacing required)
4. Please mark in hands to show 10 minutes past eleven o’clock (11.10)
Information
5. Can you tell me something that happened in the news recently? (Recently = in the last week. If a general answer is given, eg “war”, “lot of rain”, ask for det ails. Only specific answer scores).
Recall
6. What was the name and address I asked you to remember
John
Brown
42
West (St)
Kensington
© Universit –
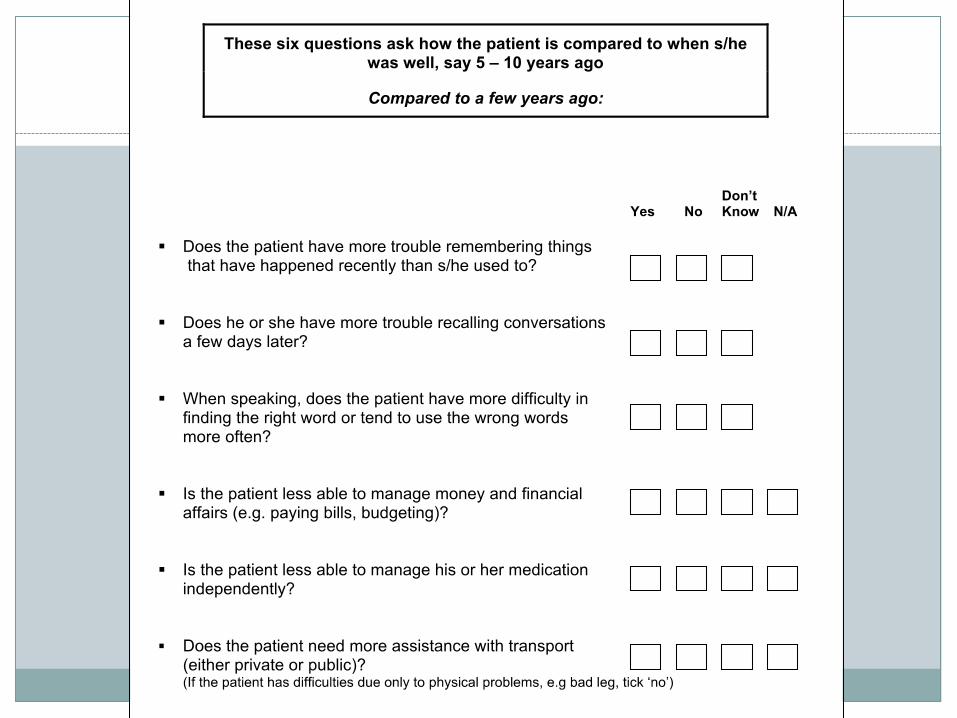
Step 2: Informant Report
Review of the GPCOG
Is the GPCOG a valid cognitive screening method?
Inpatient validation?
How does GPCOG compare to other conventional cognitive assessment tools?
Method
Medline and embase search
Terms “GPCOG” and “general practitioner assessment of cognition”
Exclusion: study protocols, inaccessible review articles, conference abstracts
Data extracted: sensitivity, specificity, positive predictive value, mean time to completion, populations studied and gold standard comparisons
Results
20 abstracts were retrieved
13 full papers eligible for inclusion
6 original research articles
7 reviews
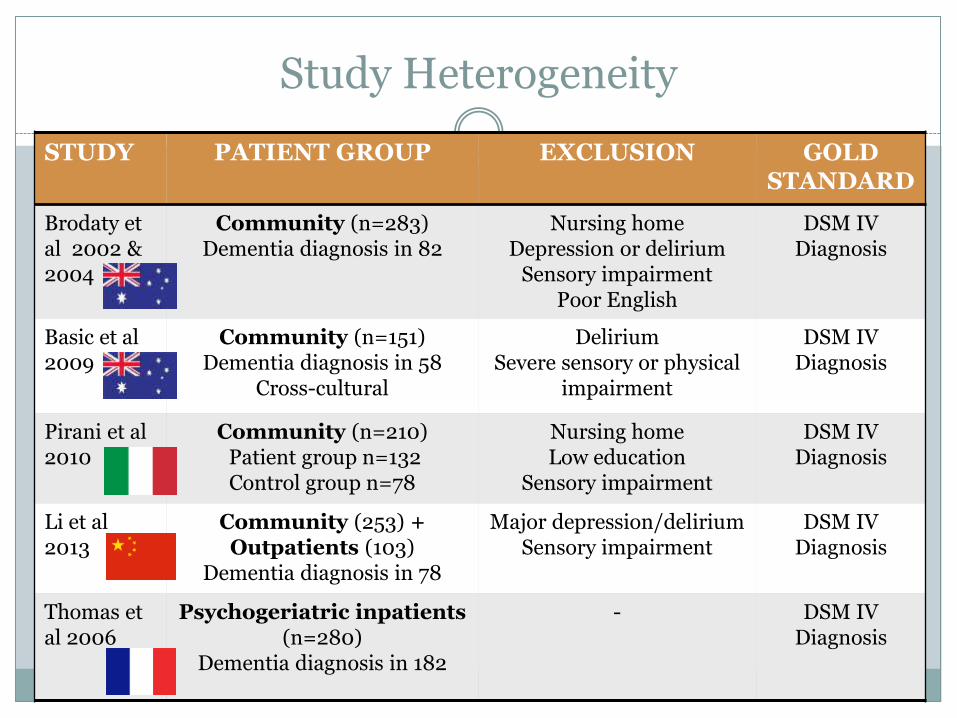
Study Heterogeneity
STUDY PATIENT GROUP EXCLUSION GOLD STANDARD
Brodaty et al 2002 & 2004
Community (n=283) Dementia diagnosis in 82
Nursing home Depression or delirium
Sensory impairment Poor English
DSM IV Diagnosis
Basic et al 2009
Community (n=151) Dementia diagnosis in 58
Cross-cultural
Delirium Severe sensory or physical
impairment
DSM IV Diagnosis
Pirani et al 2010
Community (n=210) Patient group n=132 Control group n=78
Nursing home Low education
Sensory impairment
DSM IV Diagnosis
Li et al 2013
Community (253) + Outpatients (103)
Dementia diagnosis in 78
Major depression/delirium Sensory impairment
DSM IV Diagnosis
Thomas et al 2006
Psychogeriatric inpatients (n=280)
Dementia diagnosis in 182
- DSM IV Diagnosis
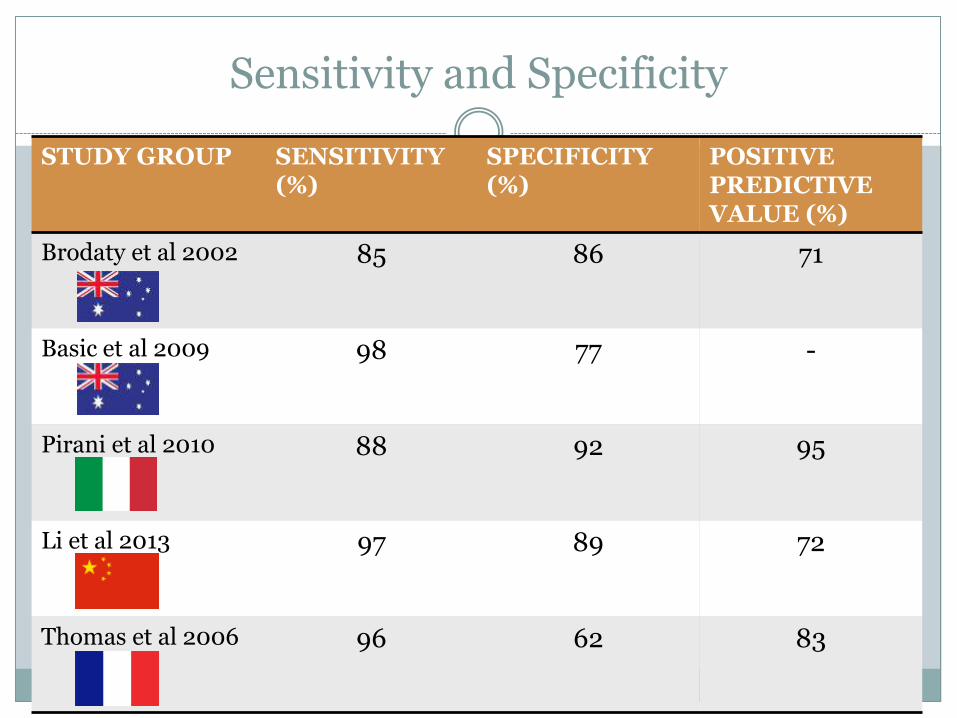
Sensitivity and Specificity
STUDY GROUP SENSITIVITY (%)
SPECIFICITY (%)
POSITIVE PREDICTIVE VALUE (%)
Brodaty et al 2002 85 86 71
Basic et al 2009 98 77 -
Pirani et al 2010 88 92 95
Li et al 2013 97 89 72
Thomas et al 2006 96 62 83
Mean Time to Completion
Reported in 3 trials
3.0 to 3.5 minutes for the patient section
1.2 to 2.2 minutes for the informant section
Mean Time to Completion
Reported in 3 trials
3.0 to 3.5 minutes for the patient section
1.2 to 2.2 minutes for the informant section
Mean less than 5 minutes to complete both in all studies
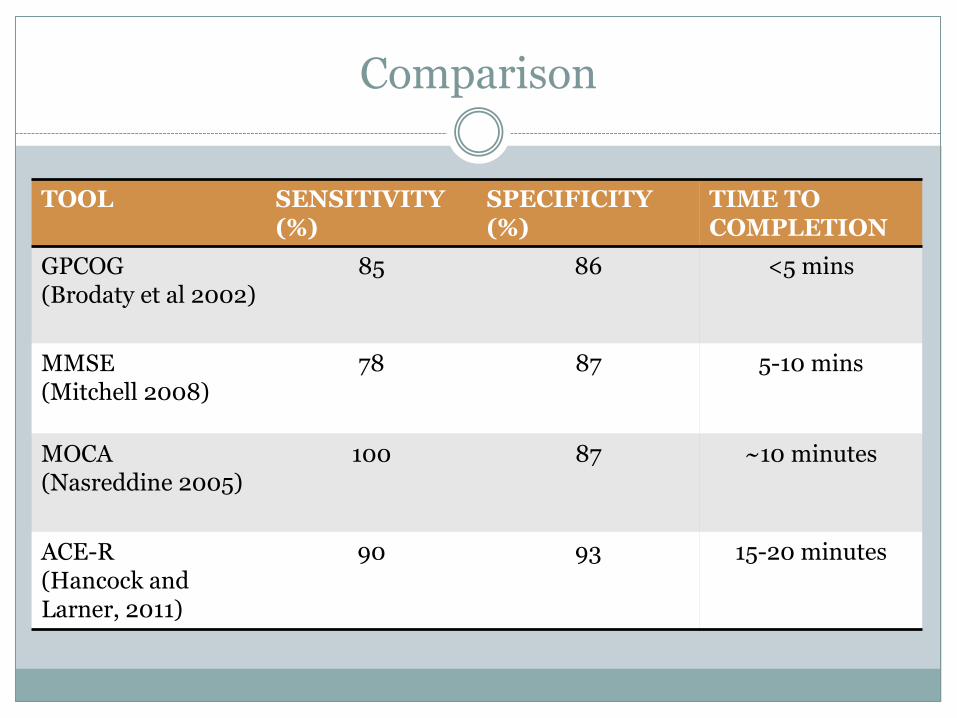
Comparison
TOOL SENSITIVITY (%)
SPECIFICITY (%)
TIME TO COMPLETION
GPCOG (Brodaty et al 2002)
85 86 <5 mins
MMSE (Mitchell 2008)
78 87 5-10 mins
MOCA (Nasreddine 2005)
100 87 ~10 minutes
ACE-R (Hancock and Larner, 2011)
90 93 15-20 minutes
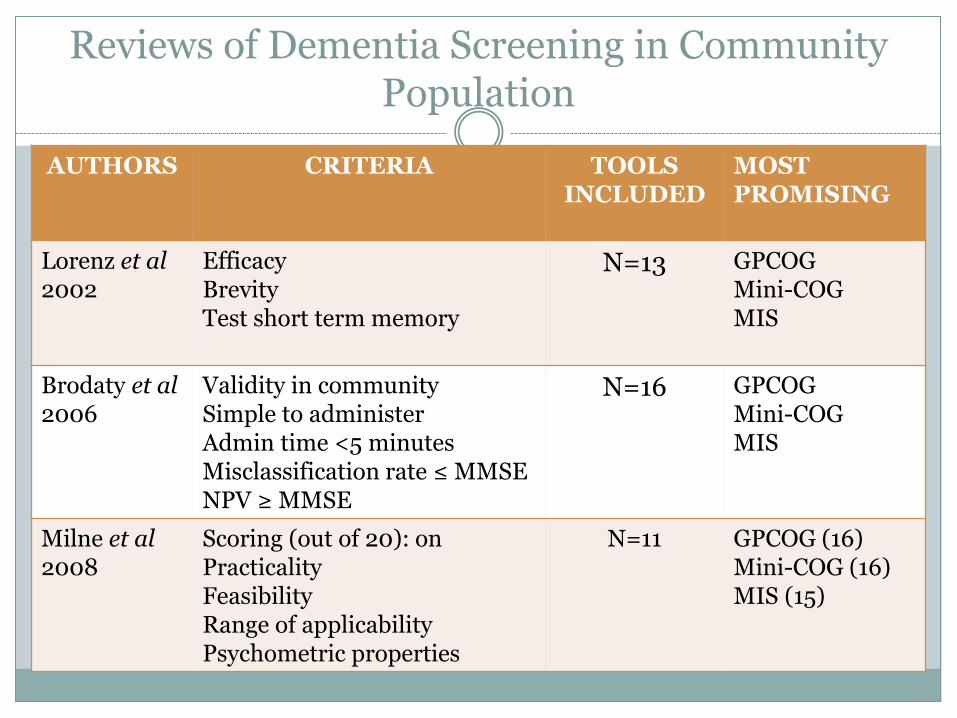
Reviews of Dementia Screening in Community Population
AUTHORS CRITERIA TOOLS
INCLUDED MOST PROMISING
Lorenz et al 2002
Efficacy Brevity Test short term memory
N=13 GPCOG Mini-COG MIS
Brodaty et al 2006
Validity in community Simple to administer Admin time <5 minutes Misclassification rate ≤ MMSE NPV ≥ MMSE
N=16 GPCOG Mini-COG MIS
Milne et al 2008
Scoring (out of 20): on Practicality Feasibility Range of applicability Psychometric properties
N=11 GPCOG (16) Mini-COG (16) MIS (15)
Informant Review
Brodaty et al 2002:
Informant review only available in 75% of cases.
Li et al 2013:
Lack of informant resulted in 41 exclusions (from initial 414 initially eligble participants)
GPCOG
STRENGTHS WEAKNESSES
Efficacy: comparable to MMSE Age bias
Rapid time to completion Challenges of fitting in with existing guidelines/clinician knowledge
Advantages of informant report
Challenge in availability of informant report
Acceptable to patients and GPs Not yet validated in general medical or geriatric inpatients
Tested in different languages / cultures
No education bias
Freely available online
Conclusions
GPCOG is a rapid and valid cognitive assessment tool in community populations
Compares favourably to commonly used cognitive assessment tools
Additional benefit of inclusion of informant history
Further Directions
Validation of cognitive asessment tools in the general inpatient population and nursing home population
Key Papers
Brodaty, H., Pond, D., Kemp, N. M., Luscombe, G., Harding, L., Berman, K., & Huppert, F. a. (2002). The GPCOG: a new screening test for dementia designed for general practice. Journal of the American Geriatrics Society, 50(3), 530–4.
Lorentz, W. J., Scanlan, J. M., & Borson, S. (2002). Brief screening tests for dementia. Canadian journal of psychiatry. 47(8), 723–33.
Brodaty, H., Kemp, N. M., & Low, L.-F. (2004). Characteristics of the GPCOG, a screening tool for cognitive impairment. International journal of geriatric psychiatry, 19(9), 870–4. doi:10.1002/gps.1167
Milne, A., Culverwell, A., Guss, R., Tuppen, J., & Whelton, R. (2008). Screening for
dementia in primary care: a review of the use, efficacy and quality of measures. International Psychogeriatrics, 20(05), 911–926.
Mitchell, A. J. (2009). A meta-analysis of the accuracy of the mini-mental state examination in the detection of dementia and mild cognitive impairment. Journal of psychiatric research, 43(4), 411–31.
Recommended


















