Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
١
Citation : THE ENDOCRINE SYSTEM /V1 Author : Ass. Prof. Dr. Sa'ad Merza Alaraji Subjects : The Endocrine System ,The Hypothalamus and the Pituitary
Gland ,The Thyroid Gland ,The Adrenal Glands ,The Endocrine Pancreas ,Parathyroid Hormone, Vitamin D, and Calcitonin AndThe Hypothalamic‐Pituitary‐Gonadal Endocrine Axis.
Date : 2011 Abstract : A hormone is a chemical that is produced by the body and
has a specific regulatory effect on a target cell or organ. It is now recognized that almost every organ secretes hormones and that endocrine cells may be dispersed throughout the body (e.g., in the gut mucosa). Certain diseases commonly encountered in general medical practice, such as diabetes mellitus or thyroid disorders, are caused by a deficiency or an excess of specific hormones. Many other common diseases not directly caused by endocrine dysfunction have prominent endocrine components, including cancer and atherosclerosis.
Publication : University Of Babylon ,College Of Medicine, Dep. Of
Medical Physiology Volume :1 Number :1 Starting page: 1 Ending page: 14 Keywords: Endocrinology, endocrine systems , hormone ,
neurohormones , neurotransmitters , neuromodulators, Intercellular chemical signals , nervous system , Autocrine , Paracrine , Pheromones , Prostaglandins , Histamine , Thyroxine , insulin , Oxytocin , antidiuretic hormone , Acetylcholine, , epinephrine , steroid , peptide , cholesterol, Thyrotropin‐releasing hormone (TRH) , Corticotropin‐releasing hormone (CRH) , Growth hormone releasing factor (GRF), Somatostatin (growth hormone inhibiting hormone), Gonadotropin‐releasing

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
٢
hormone (GnRH), Prolactin‐inhibiting factor (PIF), Prolactin‐releasing hormone (PRH)
Type: Lecture
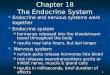
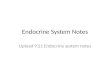
Location of Major Endrocrine Organs
TABLE – 1 : Summary of Hormones Produced by the Major Endocrine Organs Endocrine Gland
Hormone Released
Chemical Class
Target Tissue/Organ
Major Function of Hormone
Hypothalamus
Hypothalami
c releasing and
inhibiting hormones
Peptide Anterior pituitary
Regulate anterior pituitary hormoneThe hypothalamus is connected to the hypophysis directly by numerous nervous pathways and blood vessels. The secretion and release of hormones in the pituitary gland is initiated by certain releasing hormones (called ‘liberins”) and “statins”, which are formed in nerve cells in the hypothalamus and reach the pituitary through their axons or by the blood. These may either have a direct effect on the target organ (somatotrope hormones) or act first on the peripheral endocrine glands(hormonesthat reach their site of action via the bloodstream). Chemoreceptors in the hypothalamus constantly measure the concentration of hormone scirculating in the blood. Depending on the hormone

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
٣
level more or less
Thyrotropin‐releasing
hormone(TRH)
Peptide Anterior pituitary
Stimulates secretion of TSH and prolactin from Adenohypophysis (Anterior Lobe of the Pituitary Gland)
Corticotropin‐releasing hormone (CRH)
Peptide Anterior pituitary
Stimulates release of ACTH from Adenohypophysis
GrowthHormone‐releasing hormone (GHRH)
Peptide Anterior pituitary
Stimulates release of growth hormone from Adenohypophysis
Growth hormone inhibitory hormone (GHIH)
(somatostatin)
Peptide Anterior pituitary
Inhibits release of growth hormone from Adenohypophysis
Gonadotropin releasing
hormone(GnRH)
Peptide Anterior pituitary
(GnRH) Stimulates release of Gonadotropin ( LH and FSH) from Adenohypophysis
Dopamine or prolactin‐inhibiting factor (PIF)
Peptide Anterior pituitary
Inhibits release of prolactin from Adenohypophysis
prolactin‐ releasing
factor (PRF)
Peptide Anterior pituitary
Stimulates release of prolactin from Adenohypophysis
Posterior Pituitary
Antidiuretic (ADH)
Peptide Kidneys Are produced in the hypothalamus(in the supraoptic nuclei ) and transported by axons to the posterior pituitary where they are dumped into the blood,& are then transported in combination with "carrier" proteins called neurophysins down to the nerve endings in the posterior pituitary gland, requiring several days to reach the gland Stimulates& Increases water reabsorption( retention ) by kidneys and

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
٤
Vasoconstricts arterioles &increased blood pressure
Oxytocin Peptide Uterus, mammary
glands(breasts)
Are produced in the hypothalamus(in the paraventricular nuclei ) and transported by axons to the posterior pituitary where they are dumped into the blood& are then transported in combination with "carrier" proteins called neurophysins down to the nerve endings in the posterior pituitary gland, requiring several days to reach the gland, Stimulates uterine muscle contractions during labor & Stimulates milk ejection from breasts
Anterior Pituitary
Thyroid stimulating
(TSH)
Thyrotropin
Glycoprotein
Thyroid Stimulates synthesis and secretion of thyroid hormones (thyroxine and triiodothyronine Low blood levels of TSH causes release of TRH from hypothalamus, which in turn causes the release of TSH from the anterior pituitary
Adrenocorticotropic (ACTH)
Peptide Adrenal cortex
Trophic to adrenal cortex , Stimulates adrenal cortex Stimulates synthesis and secretion of adrenocortical hormones (cortisol,
androgens, and aldosterone)
(Gonadotropin) Follicle‐stimulating hormone (FSH)
Glycoprotein Gonads
Stimulates ovarian follicle development and Promotes sperm maturation in Sertoli cells of testes. Affect the gonads by stimulating gamete formation and production of sex hormones
(Gonadotropin) Luteinizing hormone (LH)
Stimulates Leydig cells of testes to secrete testosterone stimulates ovulation, formation of corpus luteum, and estrogen and progesterone synthesis in ovaries affect the gonads by stimulating gamete formation and production of sex hormones
Prolactin (PRL)
Protein Mammary glands
Required in lactation for mammary growth, initiation of milk secretion, and maintenance of Milk production Promotes development of the female breasts and secretion of milk, Prolactin is secreted near the end of pregnancy and prepares the breasts for milk production
Growth Hormone (GH)
Protein Soft tissue, bones
-Acute metabolic effects oppose insulin -Chronic growth-promoting effect via insulin-like growth factor 1 (IGF-1) -Stimulates Cell division, protein synthesis and bone growth and overall growth of most cells and tissues
Melanocytes stimulating Hormone(MS
H)
skin Causes melanocytes which located in a bundance between the dermis &epidermisof the skin

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
٥
Endorphins When ACTH is secreted ,several other hormones that have similar chemical structure are secreted simultaneously.The RNAthat causes a preprohormone that contain ACTH as only one of its subunits. Thiscontains (MSH), Endorphins, Enkephalins,Lipotropin
Enkephalins
Thyroid Thyroxine (T4) and
Triiodothyronie (T3)
Iodinated amino acid
All tissue Increases the rates of chemical reactions in most
cells, thus increasing body metabolic rate, regulates growth and development
Required for normal growth and development
Calcitonin Peptide Bones, kidneysand intestine Lowers blood calcium level Promotes deposition of calcium in the
bones and decreases extracellular fluid calcium ion concentration
Parathyroids
Parathyroid hormone
(PTH)
Peptide Bones, kidneys andintestine
• Regulates serum [Ca2+]• Increases Ca2+ resorp on from bone • Increases renal and intes nal Ca2+ absorp on • Increases renal phosphate excretion Raises blood calcium level Controls serum calcium ion concentration by increasing calcium absorption by the gut and kidneys and releasing calcium from bones
Adrenal Cortex
Glucocorticoids
(Cortisol)
Steroid All tissue Released in response to stress
Has multiple metabolic functions for controlling metabolism of proteins, carbohydrates, and fats; also has
anti-inflammatory effects Raise blood glucose level, stimulates breakdown of
protein
Mineralocoticoids
(Aldosterone)
Steroid Kidneys Decreases urinary Na+ excretion Reabsorb sodium and excrete potassium Increases renal sodium reabsorption, potassium secretion, and hydrogen ion secretion
Sex Hormones
Steroid Gonads, skin, muscles and
bones
Stimulates reproductive organs and brings on sex characteristics
Adrenal Medulla
Epinephrine and
norepinephrine
Modified amino acid
Cardiac and other muscles
Released in emergency situations, raises blood glucose level, “fight or flight” response
Same effects as sympathetic stimulation
Pancreas Insulin (β cells) Protein Liver, muscles, adipose tissue
• Promotes storage of glucose as glycogen in liver and muscle • Promotes uptake of glucose and storage as triglyceride in adipose tissue and liver Lowers blood glucose levels, promotes formation of glycogen Promotes glucose entry in many cells, and in this way controls carbohydrate metabolism

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
٦
Glucagon (α cells)
Protein Liver, muscles, adipose tissue
Increases blood glucose by promoting glycogenolysis, gluconeogenesis, andketogenesis in liver Increases synthesis and release of glucose from the liver into the body fluids
Testes Androgens (testosterone)
Steroid Gonads, skin, muscles and
bone
Required for male puberty; development and maintenance of male reproductive organs and secondary sex characteristics Stimulates male sex characteristics Promotes development of male reproductive system and male secondary sexual characteristics
Ovaries Estrogens Steroid Gonads, skin, muscles and
bones
Required for female puberty; development and maintenance of female reproductive organs and secondary sex characteristics Promotes growth and development of female reproductive system, female breasts, and female secondary sexual characteristics
Progesterone Steroid Gonads, skin, muscles and
bones
Supports secretory phase of endometrial cycle Important in maintenance of pregnancy Stimulates secretion of "uterine milk" by the uterine endometrial glands and promotes development of secretory apparatus of breasts
Thymus Thymosins Peptide T lymphocytes Stimulates production and maturation of T lymphocytes
Pineal Gland
Melatonin Modified amino acid
Brain Controls circadian and circannual rhythms, possibly involved in maturation of sexual organs
Placenta Human chorionic
Gonadotropins (HCG)
Maintains corpus luteum early in pregnancy Promotes growth of corpus luteum and secretion of estrogens and progesterone by corpus luteum
Human chorionic
somatomammotropin(hCS) (also called
human placental
lactogen, or hPL)
Supports breast development in pregnancy Regulates fuel metabolism of fetoplacental unit Probably helps promote development of some fetal tissues as well as the mother's breasts
Estrogens
Steroid
Promotes growth and development of female reproductive system, female breasts, and female secondary sexual
characteristics
Progesterone
Steroid
Stimulates secretion of "uterine milk" by the uterine endometrial glands and promotes development of secretory apparatus of
breasts
Kidney Renin Catalyzes conversion of angiotensinogen toangiotensin I (acts as an enzyme)
Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
٧
1,25‐Dihydroxycholecalciferol
Increases intestinal absorption of calcium and bone mineralization
Erythropoietin
Increases erythrocyte production
Heart Atrial natriuretic
peptide (ANP)
Increases sodium excretion by kidneys, reduces blood pressure
Adipocytes Leptin Inhibits appetite, stimulates thermogenesis
Stomach Gastrin
Stimulates HCl secretion by parietal cells of gastric mucosa
Secretin Stimulates pancreatic acinar cells to release bicarbonate and water
Cholecystokinin
(CCK) Also secreted from small intestine
• Stimulates release of pancreatic enzymes • Contracts gallbladder • Relaxes sphincter of Oddi • Inhibits stomach motility • Acts as satiety signal Stimulates gallbladder contraction and release of pancreatic enzymes
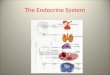
INTERCELLULAR COMMUNICATION SYSTEMS
The maintenance of homeostasis requires the coordination of cells, tissues, and organs. Most communication between cells is achieved by the release of chemical messengers. Neural communication occurs by rapid information transfer using electrical signals or chemical signals ; the release of neurotransmitters at synapses between neurons or at a target cell such as a muscle produces a response.

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
٨
‐ Endocrine communication occurs by the release of a chemical transmitter (Hormone) by specialized endocrine cells and is carried to a distant site of action via the blood.
‐ Neuroendocrine control is a hybrid of neural and endocrine communication in which neurons release a chemical transmitter (Neurohormone) that is carried to a distant site of action via the blood; for example, the release of an antidiuretic hormone from the axon terminals in the posterior pituitary gland.
‐ Paracrine communication involves cells that secrete chemical transmitters locally into the surrounding interstitial fluid; the target cells are near “Neighbors” and are reached by diffusion of the hormone rather than by its transport in the blood. somatostatin from pancreatic cellsdiffuse only as far as & cells of Islets to inhibit secretions
‐ Autocrine signaling occurs when a cell regulates itself by the release of a chemical messenger.

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
٩
‐ PHEROMONES:Are hormones secreted into external environment used to
communicate information(also used to attract opposite SEX).
The functions of the body are regulated by : 1-Nervous system 2-Endocrine system.
The nervous system exerts point-to-point control through nerves, similar to sending messages by conventional telephone. Nervous control is electrical in nature and fast. The endocrine system broadcasts its hormonal messages to essentially all cells by secretion into blood and extracellular fluid. Like a radio broadcast, it requires a receiver to get the message - in the case of endocrine messages, cells must bear a receptor for the hormone being broadcast in order to respond.
Chemical Classification Of Hormones Most hormones can be grouped into one of three major chemical classes: peptides, amines, and steroids. 1. Peptides are the largest group of hormones. Peptide hormones are generally water soluble and do not require carrier molecules in the blood. 2. Amines are a small group of hormones that includes the catecholamines (dopamine, epinephrine, and norepinephrine) and the thyroid hormones. Thyroid hormones are also derived from the amino acid tyrosine but are poorly soluble in water and do require carrier proteins in the blood. 3. Steroid hormones are synthesized from cholesterol and include cortisol, aldosterone, testosterone, estrogen, and progesterone. Steroid hormones are not stored in vesicles and rapidly diffuse out of the cell once synthesized due to their high lipid solubility. Steroids generally require carrier proteins in the blood due to their low water solubility. The properties of steroid hormones are compared to peptide hormones in Table :2.
TABLE -2 : Properties of Different Chemical Classes of Hormones

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
١٠
Hormone Characteristic Peptide Hormone* Steroid HormoneWater soluble Yes No
Uses carrier protein in plasma No YesIs stored in vesicles prior to secretion Yes No
Receptor location at target cell Plasma membrane Intracellular
Mechanism of action Mainly second messengers Mainly altered gene expression
Speed and duration of action Usually fast onset but short-acting responses
Usually slow onset but long-lasting responses
*The amine class has variable characteristics; catecholamines have properties more like peptidwhereas thyroid hormones share many of the characteristics of steroids.
PLASMA HORMONE CONCENTRATION The magnitude of a response to a hormone depends on how many receptors are occupied at the target cell, which in turn depends on the free hormone concentration in the extracellular fluid. The plasma free hormone concentration is affected by: 1. The rate of hormone secretion. 2. The rate of hormone elimination. 3. The extent of hormone binding to plasma proteins.
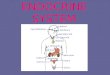
Feedback Control Of Hormone Secretion Feed back regulation: is a primary mechanism governing hormonal secretary control. Positive feed back control: elevated serum level of one hormone stimulate secretion of another hormone. Negative feed back control: increased circulating level of one hormone suppressing secretion of another hormone. In most cases, the rate of hormone secretion is under negative feedback control (Figure :1). Simple negative feedback occurs when a hormone, or a response to a hormone, directly inhibits further secretion of that hormone.

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
١١
Figure -1 : Negative feedback control secretion : Simple negative feedback in which a hormone, or a response to the hormone, inhibits further hormone secretion.
For example, insulin secretion by the β cells in the pancreas causes a decrease in the blood glucose concentration, which directly inhibits further insulin release.
Figure -2 : Negative feedback control secretion : Complex (hierarchical) negative
feedback in which a hormone secreted from a primary target gland exerts negative feedback on the hypothalamus and pituitary gland.
For some hormones, the plasma hormone concentration is strongly influenced by a rhythmic pattern of secretion. For example, the steroid hormone cortisol has a distinctive circadian (day/night) pattern of secretion, with the highest hormone concentration in the early morning hours and less concentration during late afternoon and evening.
Hormone Transport In Blood Only free hormone molecules can diffuse out of capillaries and bind to their receptors at the target cell. Binding of a hormone to plasma proteins reduces the free concentration available. For example, steroids and thyroid hormones are poorly soluble in water and must bind to plasma proteins to be carried in plasma; typically, more than 90% of the total hormone concentration is protein bound. The protein bound hormone fraction remains in the plasma and is inactive. The half‐life of protein‐bound hormones is generally long because the protein‐bound fraction acts as a reservoir of the hormone. Water‐soluble hormones such as peptides and catecholamines dissolve easily in the blood plasma and are able to freely diffuse
Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
١٢
from the plasma to their site of action. Water‐soluble hormones that are not extensively protein bound tend to have a faster onset of action and act for shorter periods of time (e.g., catecholamines) than do hormones with a high fraction bound to carrier proteins in plasma (e.g., thyroid hormones). Thyroid hormones and steroid hormones are good examples. Thyroid hormones are small molecules of modified amino acids with a half‐life of 7 days for thyroxin and 8‐24 hours for triiodothyronine. Thyroxin is more tightly bound to TBG than triiodothyronine. Steroid hormones such as cortisol which is transported tightly bound to CBG (transcortin, as the human serum protein is called) has a half‐life of about 90 minutes whereas aldosterone and angiotensin II which circulate free in serum have half‐lives of about 15 minutes and 1‐3 minutes, respectively.
Peripheral Conversion of Hormones
In some instances an inactive or less active form of a hormone may be secreted by an endocrine cell into the general circulation and then converted to a more active form by another tissue. This type of peripheral conversion occurs in blood, liver, kidney, lung, and in the target tissues of some hormones. These tissues contain enzymes capable of interconversion of hormones. Examples: 1. As much as 60% of plasma testosterone in women results from peripheral conversion in liver of androstenedione (weak androgen), which is normally secreted by the adrenal cortex; 2. Renin is a proteoly c enzyme from the kidney and is released into the blood stream in response to a fall in blood pressure. Renin converts angiotensinogen to angiotensin I in blood and, in turn, angiotensin I is converted in the lungs to angiotensin II, a powerful vasopressor and stimulator of aldosterone secretion from the adrenal cortex; 3) Testosterone is secreted by tes cular Leydig cells and is converted to a more potent form, 5 alpha‐dihydrotestosterone, in the target cell; and 4) The liver converts thyroxine T4 (less ac ve) to triiodothyronine T3 (more active).

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
١٣
Hormone Receptors And Intracellular Signaling
A response to a particular hormone is seen only in cells with specific receptors for that hormone. Receptors are proteins that may be in the cell membrane (cell mem. receptors) (e.g., peptide hormones and catecholamines), in the cell cytoplasm (cytoplasmic receptors) (e.g., steroid hormones), or in the nucleus (Nuclear receptors) (e.g., thyroid hormones). The response to a hormone is affected by the number of receptors; Downregulation(Decrease in No. & affinity of receptors if hormone level is high ) or Upregulation(Increase in No. & affinity of receptors if hormone level is low) of the receptor number determines the sensitivity of a target cell to a hormone.
Ass. Prof. Dr. Saad Merza Husain Alaraji
٧٥
References:
Ayuk J.; Sheppard, M.C. ( 2006). Growth hormone and its disorders. Postgrad. Med. J. ;82:24.
Barrett ,K. E. ; Barman, S. M. ;Boitano ,S. ; Brooks, H. L. ( 2010 ) . Ganong's Review of Medical Physiology .23rd Edition; The McGraw-Hill Companies, Inc. ; United States of America.
Boissy, R.E.; Nordlund, J.J.( 1997). Molecular basis of congenital hypopigmentary disorders in humans: A review. Pigment Cell Res. ;10:12.

Endocrinology Dr. Sa'ad Merza Alaraji
University Of Babylon ,College Of Medicine, Dep. Of Medical Physiology
١٤
Brent, G.A. ( 2008 ). Graves' Disease. N. Engl. J. Med. ;358:2594.
Buzi ,F.; Mella, P.; Pilotta, A.; Prandi, E.; Lanfranchi ,F.; Carapella, T. ( 2007). Growth hormone receptor polymorphisms. Endocr. Dev. ;11:28.
Dohan, O.; Carrasco, N. ( 2003 ). Advances in Na+/I- symporter (NIS) research in the thyroid and beyond. Mol. Cell. Endocrinol. ;213:59.
Fauquier, T.; Rizzoti, K.; Dattani, M.; Lovell-Badge, R.; Robinson, I. ( 2008 ). CAF: SOX2-expressing progenitor cells generate all of the major cell types in the adult mouse pituitary gland. Proc. Natl. Acad. Sci. USA ;105:2907.
Glaser, B. ( 2003 ). Pendred Syndrome. Pediatr. Endocrinol. Rev. ;1(Suppl 2):199. Kibble,J.D; Halsey, C. R. ( 2009 ) . Medical . LANGE The Big Picture , New York.
Goldstein J.L. ;Brown, M. S. ( 2001 ) . The cholesterol quartet. Science ;292:1510.
Goodman ,H. M. ( 2000 ): Handbook of Physiology, Section 7: The Endocrine System. Oxford University Press .
Guyton, W.F. ; Hall .( 2006 ) Textbook of Medical Physiology .11th Edition, The McGraw-Hill Companies, Inc. ; United States of America.
Hindmarsh, P.C.; Dattani ,M.T. ( 2006). Use of growth hormone in children. Nat. Clin. Pract. Endocrinol. Metab. ;2:260.
hormone biosynthesis: The case for the steroidogenic acute regulatory (StAR) protein. Proc. Soc. Exp. Biol. Med. ;217:123.
Larsen, P. R. ( 2oo3 ). Williams Textbook of Endocrinology, 9th ed. Saunders Co. New York , USA.
Peeters, R.P.; Van der Deure, W.M.; Visser, T.J. ( 2006 ). Genetic variation in thyroid hormone pathway genes: Polymorphisms in the TSH receptor and the iodothyronine deiodinases. Eur. J. Endocrinol. ;155:655.
Stocco, D. M. ( 1998 ). A review of the characteristics of the protein required for the acute regulation of steroid
White, P.C. ( 1994 ). Disorders of aldosterone biosynthesis and action. N. Engl. J. Med. ;331:250.
Thank You
Recommended