Nat
iona
l Can
cer
Inst
itute
Survivorship Care Plans: Who is Using them and Why?
Julia H. Rowland, Ph.D., Director
Office of Cancer Survivorship National Cancer Institute • National Institutes of Health • DHHS
15th Annual Living with Breast Cancer Symposium
Suburban Hospital, Bethesda, MD
Saturday, November 2, 2013
0
2
4
6
8
10
12
14
16
18
20
1977 1982 1987 1992 1997 2002 2007 2012 2017 2022
Nu
mb
er i
n M
illi
on
s
Year
15+ years
10-<15 years
5-<10 years
1-<5 years
<1
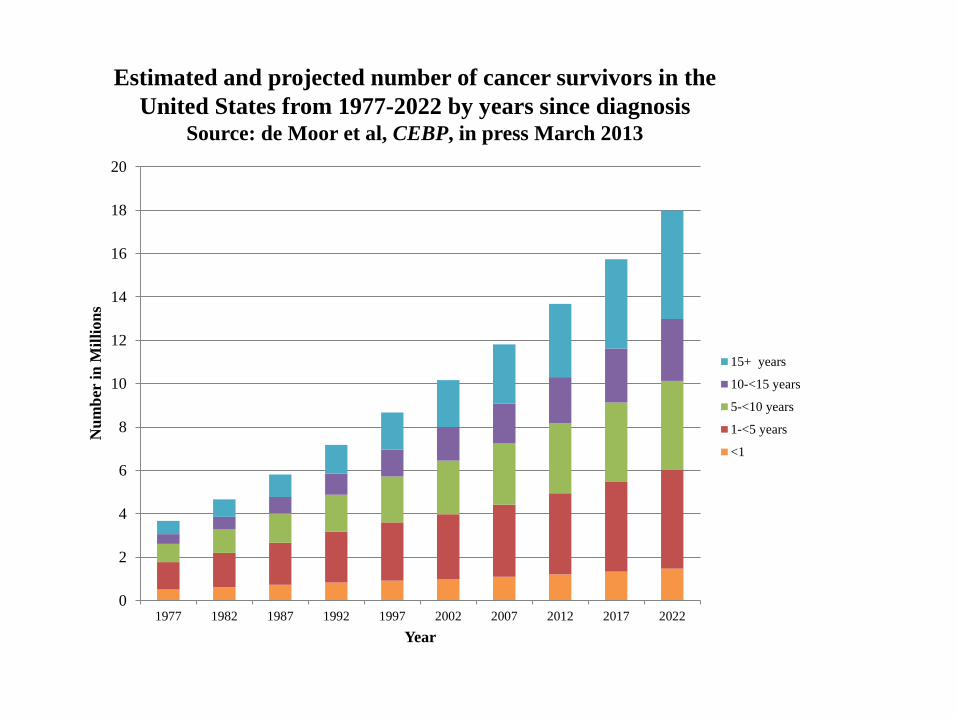
Estimated and projected number of cancer survivors in the
United States from 1977-2022 by years since diagnosis Source: de Moor et al, CEBP, in press March 2013
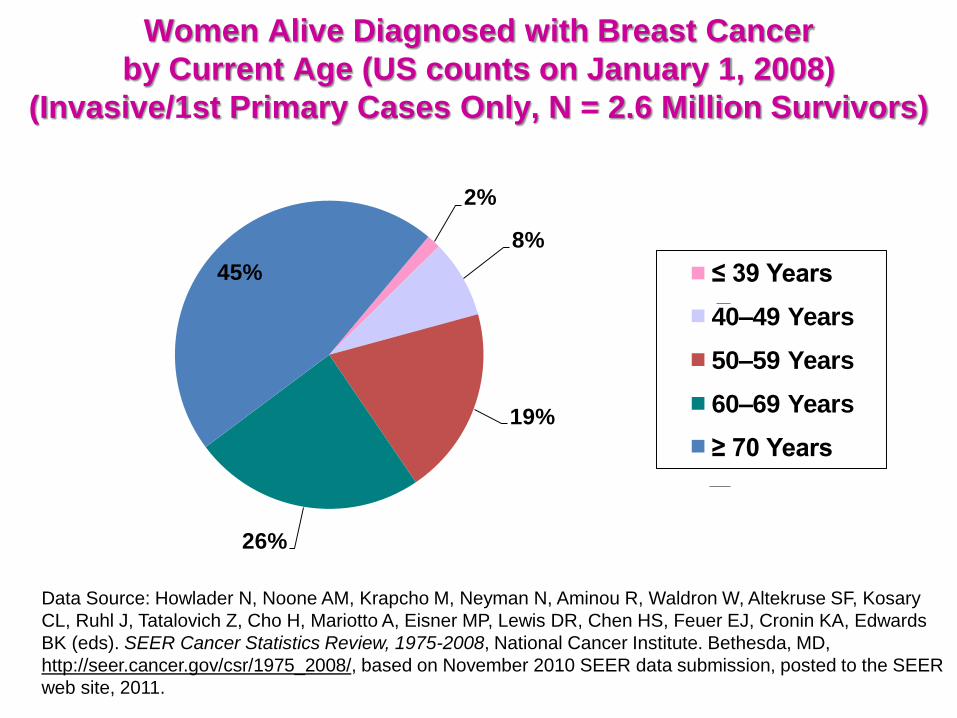
Women Alive Diagnosed with Breast Cancer
by Current Age (US counts on January 1, 2008)
(Invasive/1st Primary Cases Only, N = 2.6 Million Survivors)
2%
8%
19%
26%
45% ≤ 39 Years
40–49 Years
50–59 Years
60–69 Years
≥ 70 Years
Data Source: Howlader N, Noone AM, Krapcho M, Neyman N, Aminou R, Waldron W, Altekruse SF, Kosary
CL, Ruhl J, Tatalovich Z, Cho H, Mariotto A, Eisner MP, Lewis DR, Chen HS, Feuer EJ, Cronin KA, Edwards
BK (eds). SEER Cancer Statistics Review, 1975-2008, National Cancer Institute. Bethesda, MD,
http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posted to the SEER
web site, 2011.
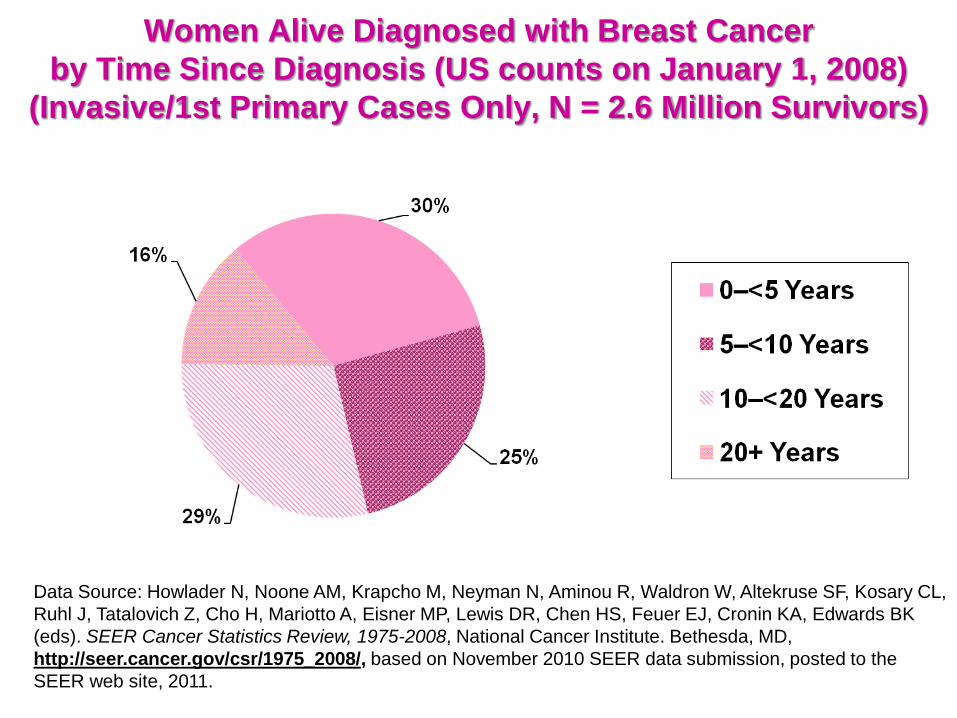
Women Alive Diagnosed with Breast Cancer
by Time Since Diagnosis (US counts on January 1, 2008)
(Invasive/1st Primary Cases Only, N = 2.6 Million Survivors)
Data Source: Howlader N, Noone AM, Krapcho M, Neyman N, Aminou R, Waldron W, Altekruse SF, Kosary CL,
Ruhl J, Tatalovich Z, Cho H, Mariotto A, Eisner MP, Lewis DR, Chen HS, Feuer EJ, Cronin KA, Edwards BK
(eds). SEER Cancer Statistics Review, 1975-2008, National Cancer Institute. Bethesda, MD,
http://seer.cancer.gov/csr/1975_2008/, based on November 2010 SEER data submission, posted to the
SEER web site, 2011.
Nat
iona
l Can
cer
Inst
itute
Chronic Effects of Cancer Treatment
• Physical/Medical (e.g., pain, fatigue, memory problems, lymphedema, sexual impairment, amputations)
• Psychological (e.g., depression, anxiety, uncertainty, isolation, altered body image)
• Social (e.g., changes in interpersonal relationships, concerns regarding health or life insurance, job lock/loss, return to school, financial burden)
• Existential and Spiritual Issues (e.g., sense of purpose or meaning, appreciation of life)
Nat
iona
l Can
cer
Inst
itute
Cancer Survivors at Increased
Risk for Late Effects
Disease recurrence/ new cancers
Cardiovascular disease
Obesity/Diabetes
Osteoporosis
Functional decline
Poor quality of life
Nat
iona
l Can
cer
Inst
itute
History of a movement…
Nat
iona
l Can
cer
Inst
itute
Selected Recommendations from the
President’s Cancer Panel & IOM Reports
• When treatment ends, all survivors should
receive a summary record that includes
important disease characteristics and
treatments received.
• In addition, they should be provided with a
follow-up care plan incorporating available
evidence-based standards of care.
Nat
iona
l Can
cer
Inst
itute
Treatment Summary (per IOM) - 1
1. Diagnostic tests performed and results
2. Tumor characteristics (e.g., site, stage and grade,
hormone receptor status, and marker information)
3. Dates of treatment initiation and completion
4. Surgery, chemotherapy, radiotherapy,
transplantation, hormonal therapy, gene, or
other therapies provided, including agents used,
treatment regimen, total dosage, identifying number and title
of clinical trials (if any) indicators of treatment response, and
toxicities experienced during treatment
Nat
iona
l Can
cer
Inst
itute
Treatment Summary (per IOM) - 2
5. Psychosocial, nutritional and other
supportive services provided
6. Full contact information on treating institutions
and key individual providers
7. Identification of a key point of contact and
coordinator of continuing care
Nat
iona
l Can
cer
Inst
itute
Follow-up Care Plan (per IOM) - 1
1. The likely course of recovery from treatment
toxicities, as well as the need for ongoing
health maintenance/adjuvant therapy
2. A description of recommended cancer
screening and other periodic testing and
examinations, and the schedule on which they
should be performed (and who should provide them)
3. Information on possible late effects and long-
term effects of treatment and symptoms of such
effects
Nat
iona
l Can
cer
Inst
itute
Follow-up Care Plan (per IOM) - 2
4. Information on possible signs of recurrence and
second tumors
5. Information on the possible effects of cancer on
marital/partner relationship, sexual functioning,
work, and parenting, and the potential future
need for psychosocial support
6. Information on the potential insurance,
employment, and financial consequences of
cancer and, as necessary, referral to counseling, legal aid, and
financial assistance
Nat
iona
l Can
cer
Inst
itute
Follow-up Care Plan (per IOM) - 3
7. Specific recommendations for healthy behaviors (e.g., diet, exercise, healthy weight, sunscreen use, immunizations,
smoking cessation, and osteoporosis prevention). When
appropriate, recommendations that first-degree
relatives be informed about their increased risk
and the need for cancer screening (e.g., breast cancer,
colorectal cancer, and prostate cancer)
8. As appropriate, information on genetic counseling
and testing to identify high-risk individuals who could
benefit from more comprehensive cancer surveillance,
chemoprevention, or risk-reducing surgery
Nat
iona
l Can
cer
Inst
itute
Follow-up Care Plan (per IOM) - 4
9. As appropriate, information on known effective
chemoprevention strategies for secondary
prevention (e.g., tamoxifen in women at high risk for breast
cancer)
10. Referrals for specific followup care providers
(e.g., rehabilitation, fertility, or psychology), support groups,
and /or the patients’ primary care provider
11. A listing of cancer-related resources and
information (e.g., internet-based sources and telephone
listings for major cancer support organizations)
Nat
iona
l Can
cer
Inst
itute
Follow-up Care Plan (per IOM)
Main Domains to Cover:
1. Surveillance for recurrence or new cancer
2. Assessment and treatment or referral for
persistent effects (e.g., pain, fatigue, sexual dysfunction,
functional impairment, depression, employment issues)
3. Evaluation of risk for and prevention of late
effects (e.g., second cancers, cardiac problems, osteoporosis);
health promotion
4. Coordination of care (e.g., including frequency of visits, tests
and who is performing these)
Nat
iona
l Can
cer
Inst
itute
What are the standards for
survivorship care planning today?
Nat
iona
l Can
cer
Inst
itute
ASCO (American Society of Clinical
Oncology) Quality Oncology Practice
Initiative (QOPI) Indicators
FU Care (2008):
Was a treatment summary generated?
Was a copy given to the patient?
Was a copy given/sent to the provider(s)?
Nat
iona
l Can
cer
Inst
itute
CoC Standards: Phase in for 2015
Standard 3.3:
1) A survivorship care plan is prepared by the
principal provider who cared for the patient
with input from the patient’s other care
providers
2) The survivorship care plan is given to the
patient on completion of treatment
Nat
iona
l Can
cer
Inst
itute
CoC Standards: 2015
3) The written or electronic survivorship care
plan contains a record of care received,
important disease characteristics, and a
follow-up care plan incorporating available
and recognized evidence based standards
of care, when available. Minimum care plan
standards should reflect those from the IOM
Fact Sheet: Cancer Survivorship Care
Planning.
Nat
iona
l Can
cer
Inst
itute
State of the “art” of SCP
Sabatino SA et al. Receipt of cancer treatment summaries and
follow-up instructions among adult cancer survivors: results
from a national survey. J Cancer Surviv Mar 7, 2013 (ePub)
• Of survivors diagnosed in the past 4 years, 58% stated they
received some form of written instructions
Salz T et al. Survivorship care plans in research and practice. Ca
Cancer J Clin 2012;62:101-117
• Despite the favorable view of these by providers and survivors
• Fewer that half (43%) of NCI designated centers deliver SCPs to
breast and colorectal survivors
• Of those that do, NONE include all of the IOM recommended
elements
Nat
iona
l Can
cer
Inst
itute
Survivorship care planning
• Who should do this?
• When and where is this done?
• Are there evidence-based algorithms for
care?
• What impact does this care planning have
on: patients, providers, systems, burden of
cancer
• Who should provide what care to whom?
(Oncologists, PCP, CNP); role of medical
homes?
Nat
iona
l Can
cer
Inst
itute
Current Templates
ASCO:
http://www.asco.org/sites/www.asco.org/files/breast_
surveillance_flow_sheet_9.21.12_0.pdf
Journey Forward:
http://journeyforward.org
LiveSTRONG:
http://www.livestrongcareplan.org/
In spite of the uncertainties, there can still be
good quality of life after cancer!
Recommended

















