647
DOMPERIDONE AND LACTATION
SIR,-ln only two studies of the use of dopamine antagonists toaugment lactationl-4 were drug levels (metoclopramide2 andsulpiride3) measured in breast milk (see table). Although nosignificant side-effects were observed in the infants, dopamineantagonists given to nursing rats have been reported to affectdopamine mediated responses in the offspring at 4 weeks of age. 5Domperidone, a structurally different dopamine antagonist, raisesthe mean serum prolactin level in normal women from 8 1 to 110 - 9 9nglml after one 20 mg dose.6Its effect on lactation should be similarto that of other dopamine antagonists. Because its primary action isperipheral rather than central and because it does not cross theblood-brain barrier in any significant amount7 domperidone doesnot provoke extrapyramidal effects and is expected to cross lessfreely into breast milk. Before investigating the lactogenicproperties of domperidone in breast feeding mothers we did a pilotstudy to assess safety.Two patients whose babies were temporarily unable to take breast
milk because of prematurity were given domperidone 10 mg 8hourly from day 3 to day 6 of the puerperium. Breast milk wasexpressed about four times a day. Five serum samples were collectedat the time of routine venepunctures. Samples were stored at- 2Q°C before measurement of domperidone by radioimmunoassayat the laboratory of Janssen Pharmaceutica, Beerse, Belgium (seetable).
DOPAMINE ANTAGONIST SECRETION IN HUMAN BREAST MILK AFTER
ORAL ADMINISTRATION
*MetoclopramIde 10 mg, with sampling 2 h after a smgle dose. Sulpmde 50 mg twice dailyfor 7 days with sampling 2 h after a morning dose. Dompendone 10 mg 8-hourly for 4 dayswith serum sampling 1 75- h after a dose and sampling of all milk.
Measurement of a drug in all the breast milk produced during aperiod of treatment may more accurately reflect the drug exposureof a breast-feeding infant than does the usual measurement inindividual samples expressed 2 h after a single dose, possiblyproduced before a significant maternal plasma level has beenachieved.Our results indicate that domperidone is secreted in considerably
smaller amounts in breast milk relative to the therapeutic dosagethan is either metoclopramide or sulpiride, and justify the furtherinvestigation of the lactogenic effect of domperidone, with
monitoring of breast milk levels.
Department of Obstetrics and Gynaecology,Johannesburg Hospital,and University of the Witwatersrand,
Parktown 21a3, South Africa G. J. HOFMEYR
B. VAN IDDEKINGE
Department of Obstetrics and Gynaecology,Baragwanath Hospitaland University of the Witwatersrand
1 Kauppila A, Kivinen S, Ylikorkala O Metoclopramide increases prolactin release andmilk secretion in puerperium without stimulating the secretion of thyrotropin andthyroid hormones. J Clin Endocrinol Metab 1981, 52: 436-39.
2 Lewis PJ, Devenish C, Kahn C. Controlled trial of metoclopramide in the initiation ofbreast feeding Br J Clin Pharmac 1980, 9: 217-19.
3 Aono T. Shioji T, Aki T, Hirota K, Nomura A, Kurachi K. Augmentation of puerperallactation by oral administration of sulpiride J Clin Endocrinol Metab 1979; 48:478-82
4 Mikorkala O, Kauppila A, Kivinen S, Viinikka L. Sulpiride improves inadequatelactation Br Med J 1982, 285: 249-51
5 Engel JA, Lundborg P Behavioural and biochemical effects in offspring of nursing ratsexposed to dopamine receptor antagonists 13th Congress of CollegiumInternationale Neuro-Psychopharmacologicum 1982. abstr. vol. I: 198.
6 Brouwers JRBJ, Assies J, Wiersinga WM, Huizing G, Tytgat GN Plasma prolactinlevels after acute and subchronic oral administration of domperidone and ofmetoclopramide a cross-over study in healthy volunteers Clin Endocrinol 1980; 12:435-40
7 Laduron P, Leysen J Domperidone A specific in vitro dopamine-antagonist devoid ofin vivo central dopaminergic activity Biochem Pharmacol 1979; 28: 2161-67
SURVIVAL OF LOA LOA IN BANKED BLOOD
SIR,-The transmission of infectious agents is a well-recognisedrisk of blood transfusion. Screening of donors by asking aboutexposure histories and by laboratory tests has reduced the risk inrespect of hepatitis B, malaria, and syphilis. However, in countrieswhere haematogenous parasitic nematodes are common,transfusion of microfilariae is less easy to avoid because the donor
may have no symptoms. Transmission of the microfilariae ofWuchereria bancrofti via transfusion of fresh and banked blood hasbeen recorded; 1-3 but less is known about the transfusion of otherblood nematodes. We have studied the survival of Loa loa in bankedblood.A 26-year-old Nigerian man, who had recently emigrated to the
United States, sought medical attention for recurrent fevers whichhad been present since childhood. He had a history of intermittentsoft tissue swellings, but physical examination was remarkable onlyfor mild cervical lymphadenopathy. Sheathed microfilariae
diagnostic of L. loa were found in the peripheral blood smear. Themicrofilariae were eliminated with diethylcarbamazine (after bloodhad been taken for the experiment described below).Venous blood was collected at the midday peak of his filaraemia; 10 ml
volumes were mixed wnh I’ 5 ml of either acid citrate dextrose B (ACD-B) orcitrate phosphate dextrose (CPD) in plastic blood bank transfer packs (PL-146;Fenwal Laboratories, Deerfield, Illinois). The bags were stored at 1-6°C for21 days.Samples of the stored venous blood from both the CPD and ACD-B bags
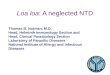
were taken via an injection port at midday after 0, 1, 7, 9, 11, 14, 18, and 21 daysof storage. Equal volumes of blood and a red cell lysing agent (’Zap-oglobin’;Couter Diagnostics, Hialeah, Florida) were mixed; 10 1 of this mixture werethen immediately counted for microfilariae in a haemocytometer chamber (fig.1). At least 100 pi of the lysed blood mixture were counted on each samplingday. On days 1 and 21 blood stored in ACD-B was also sampled via gravity flowthrough an in-line 40 m blood filter (’Ultipor’, Pall Biomedical Products,Glen Cove, NY).The concentration of motile microfilariae decreased during
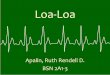
storage. The initial concentration of microfilariae (all motile) was1564±190/ml of preserved venous blood; this number includedindividual organisms as well as intertwined "medusa" forms (fig. 2).During the first 18 days of storage, the motile microfilaria countsteadily decreased to 66% of the initial concentration. Beyond 18days, however, the count fell sharply, to 3707o by day 21. Similarresults were obtained in blood preserved with ACD-B.
Filtration of stored blood on day 1 reduced the concentration ofmicrofilariae by 80%. After 21 days of storage, filtration removed92% of the microfilariae which had survived. No medusa formswere found in the filtered blood, but their absence alone cannotnumerically account for the observed reduction in total number oforganisms.The transfusion of nematode microfilariae can result in fever,
rash, and headache.2,4 Acute inflammation in viscera may occur asthe microfilariae are destroyed. The infestation will last only aslong as the transfused microfilariae survive. In one experimentL. loa microfilariae persisted for at least four days after transfusion,and other microfilariae survived in the recipient for several yearsafter transfusion.4 4
As many as 13 million people may be infected with L. loa inendemic areas of Africa. Many millions more throughout thedeveloping world are infected with other microfilariae. Althoughsymptoms are not frequently reported after transfusion of
microfilariae, the problem could grow as transfusion services in
1. Bird GWG, Menon KK Survival of Microfilaria bancrofti in stored blood. Lancet 1961;ii: 721.
2. Hawking F. The transference of Microfilaria bancrofti into natural and unnatural hostsAnn Trop Med Parasit 1940; 34: 121-29.
3. Knott J The periodicity of the microfilariae of Wuchereria bancrofti. Trans Roy SocTrop Med Hyg 1935; 29: 59-64
4. Gonnert R Zur lebensdauer menschlicher Mikrofilarien Zentbl Bakt Parasit InfekOrig 1943, 149: 75-81
5. Wolfe MS Parasites, other than malaria, transmissible by blood transfusion In:
Greenwalt TJ, Jamieson GA, eds. Transmissible disease and blood transfusion.New York: Grune and Stratton, 1974 267-77.
6. Connor DH, Neafie RC, Meyers WM. Loiasis In: Binford CH, Connor DH, eds.
Pathology of tropical and extraordinary diseases Washington. Armed ForcesInstitute of Pathology, 1976. 356-59
7. Stoll NR This wormy world J Parasitol 1947; 33: 1-18

648
Fig. 1-L. loa microfilaria in banked blood ( x 2075).
Fig. 2-L. loa microfilarial medusae in haemocytometer chamber.
Lines (white) are 0- 025 mm apart (x 1050).
endemic areas expand. Post-transfusion morbidity apart, transfusedmicrofilariae may elicit a reaction mimicking blood incompatibilityor even help to propagate the disease if the transfusion recipientwere bitten by a suitable vector.Our study suggests that, although refrigerated storage alone will
not ensure the disappearance of L. loa from stored banked blood, alarge proportion of the microfilariae can be removed by filtration.Further work is needed to find out if blood filtration can become a
useful, practicable safety precaution for transfusion in endemicareas.
We thank Dr Eric Ottesen of the National Institute of Arthritis andInfectious Diseases who brought this patient to our attention.
Clinical Center Blood Bank,National Institute of Health,Bethesda, Maryland 20205, USA
JAMES P. AUBUCHONWALTER H. DZIK
IRON DEFICIENCY AND STANOZOLOL THERAPY
SIR,-Anabolic steroids are now being recommended for thetreatment of a variety of vascular disordersl-3 so it is important toidentify side-effects. Disturbed liver function, increased sensitivityto warfarin, and fluid retention are well recognised complications.In view of the effect of androgens in aplastic anaemia, a rise inhaemoglobin might be expected with anabolic agents. Normalindividuals showed no change in haemoglobin after six weeks ofstanozolol therapy5 but the lack of observations on Hb and red blood
1. Jarret PEM. The role of stanozolol in the treatment of the postphlebitic syndromeScott Med J 1981, s81-s83.
2. Cunliffe WJ, Dodman B, Roberts BE, Tebbs EM. Clinical and laboratory double blindinvestigation of fibrinolytic therapy in cutaneous vasculitis. In: Davidson JF,Samama MM, Desnoyers PC, eds Progress in chemical fibrinolysis and
thrombolysis, vol. 1. New York: Raven Press. 1975 3253. Walker ID Anabolic steroid therapy in arterial disease. A review Scott Med J 1981,
s85-s904 Jarret PEM, Morland M, Browse NL The complications of stanozolol and their
clinical management In Davidson JF Ed Progress in chemical fibrinolysis andthrombolysis vol 4. Edinburgh’ Churchill Livingstone, 1979; 317-21.
RBC INDICES BEFORE AND AFTER THREE MONTHS OF TREATMENT
WITH STANOZOLOL
H’
i i n
’Paired t tests.
cell (RBC) indices after longer periods of treatment prompted thefollowing study.Sixteen patients taking 10 mg stanozolol daily in a trial of
fibrinolytic enhancement therapy in intermittent claudication
experienced a significant fall in mean cell haemoglobin (MCH) afterthree months of treatment. The RBC count did not changesignificantly but Hb and mean cell volume (MCV) also fell (seetable). These results were contrary to the expected rise in Hb andRBC count. After exclusion of one patient (who was iron deficientat baseline) six patients remained on therapy for a year or
more, and four of these showed red cell indices suggestive of irondeficiency, which was confirmed by biochemical measurement andferritin assay. In one of these four stanozolol was discontinuedwithout iron supplementation: the red cell indices and iron statuspromptly returned to normal.All these patients showed an increase in fibrinolytic activators
while on therapy but there was no clinical or biochemical evidenceof gastrointestinal bleeding to explain the iron deficiency. Onepatient was studied in detail and showed a normal red cell survival.There was no faecal red cell loss as judged by isotope studies. Thefour patients with iron deficiency all ate diets poor in iron. In suchpatients the increase in muscle bulk induced by the anabolic steroidsmay cause utilisation of iron at the expense of Hb, this beingreflected in a change in RBC Hb.Patients taking stanozolol for long periods should have RBC
indices and liver function monitored regularly.
Withington Hospital,Manchester M20 8LR D. A. TABERNER
CALMODULIN AND CYSTIC FIBROSIS
SIR,-Sorscher and Breslow suggest that both increased
epithelial reabsorption of sodium and raised intracellular calciumcause the pathogenesis of cystic fibrosis.Calmodulin is a highly acidic monomer with four distinct calcium
binding sites. It affects many calcium-dependent activities andmodulates cyclic AMP metabolism. Calmodulin is increased incultured skin fibroblasts from patients with cystic fibrosis2 and insome sputum specimens from patients with cystic fibrosis
(unpublished). I suggest that the increased intracellular calciumnoted in patients with cystic fibrosis could be caused by an increasedor abnormal calmodulin. This abnormal or increased calmodulinmolecule would cause intracellular calcium-stimulated increases insodium reabsorption through an amiloride-sensitive pathway andthe resultant reabsorption of water, as suggested by Sorscher andBreslow. ,
Also acting in patients with cystic fibrosis would be those factorswhich block sodium reabsorption and cause hypocalcaemia. Suchfactors are calcitonin and the various thyroid gland hormones.These too have been found to be increased in patients with cysticfibrosis.3,4
3178 SW Fairmount Blvd,Portland, Oregon 97201, USA J. P. KILBOURN
5. Preston FE, Burakowski BK, Porter NR, Malia RG The fibrinolytic response tostanozolol in normal subjects. Thrombosis Research 1981; 22: 543-51.
1. Sorscher EJ, Breslow JL Cystic fibrosis: a disorder of calcium-stimulated secretionand transepithelial sodium transport? Lancet 1982; i: 368-70.
2. Gnegy ME, Erickson RP, Markovac J. Increased calmodulin in cultured skipfibroblasts from patients with cystic fibrosis. Biochem Med 1981, 26: 294-98
3. Becker KL, Nash D, Silva OL, Snider RH, Moore CF Increased serum and urinarycalcitonin levels in patients with pulmonary disease. Chest 1981; 79: 211-16
4. Segall-Blank M, Vagenakis AG, Shwachman H, Ingbar SH, Braverman LE Thyroidgland function and pituitary TSH reserve in patients with cystic fibrosis. J pediatr1981, 98: 218-22.
Recommended