Surgery of early detected non palpable suspicious breast lesions
By
Mohamed Ezzat Almahdy
Resident of surgical oncology
Oncology center Mansoura university

Acknowledgement
First and above all, my greatest thanks to mighty ALLAH, the most merciful, the most gracious for helping us all to complete this work.
I would like to express my special thanks to
Prof. Dr. Nazem Shams Professor of surgery, Faculty of Medicine, Mansoura University.
Prof. Dr. Tamer Fady Professor of surgery, Faculty of Medicine, Mansoura University
Prof. Dr. Omar Farouk Assistant professors of surgery, Faculty of Medicine, Mansoura University
for there fatherly encouragement, helpful supervision and continuous guidance during execution of this work.
I wish to express my gratitude to all my professors and colleagues at the surgical oncology unit in the Oncology Center, Mansoura University.

Introduction

Breast cancer is the most common cancer among women.
With the increased utilization of national screening programs, breastcancer is more frequently being detected as non-palpable lesion (upto 35 % in UK).
Precise localization of non-palpable lesions is an essential step toguarantee cancer clearance without compromising cosmetic results.
The most important factor in improving the survival is earlydetection.

Screening
The aim of screening for breast canceris to identify pre invasive disease orinvasive disease before dissemination.
Recent studies consider radiology themost appropriate way for screening.

Mammography
The most specific and the most sensitive method for screening onceinvolution of the breast tissue has occurred.
Breast ultrasound
US increases the sensitivity of screening if it is used withmammography for women shown to have dense breasts.
Breast MRI
It is an important screening tool in high-risk women.

Suspicious breast lesionsThe BIRADS system is a widely accepted riskassessment tool for breast lesions
Category 0: Need Additional Evaluation.
Category 1: Normal study.
Category 2: Benign.
Category 3: Probably Benign.
Category 4: Suspicious.
Category 5: Highly Suggestive of Malignancy.
Category 6: Biopsy Proven Malignancy.

Methods of localization1. Orthogonal localization.
2. Wire guided localization(WGL).
3. Perforated grids.
4. Charcoal localization
5.Methylene blue or toluidineblue dye injection.
6.Intra-operative US
7.Vacuum-assisted breast biopsysystem(VABB)(Mammotome®)8.Hematoma directed US-Guided(HUG) excision9.The breast lesion excision system(BLES)10. Metal skin marker.11. Breast metallic marker.12. MRI guided localization.13.Radio guided Occult LesionLocalization (ROLL).
14. Magnetically guided localization

1. Orthogonal localization
In which measurementsare given for exact locationof the lesion as regarddepth of the lesion anddistance from nippleareola complex.
It seems to be simple butto a great extent notaccurate and leads to largevolume of tissue excision.

2. Wire guided localization (WGL)It is currently the gold standard localization method.
However, the wire may be displaced, migrate or becometransected. Repositioning can be complicated by bruises within thepreviously punctured tumor site
Resection procedure, specimen and tumor cut along the needle, which is still in the tumor

2. Wire guided localization (WGL)

3. Perforated grids
It facilitate WGL by using aperforated compressionplate. This device is used inconjunction with a self-retaining wire, and its useresults in accurateplacement of the wire tip inclose proximity to the lesion. Marks of perforated grids with suspicious lesion ( arrow)

4. Charcoal localization
It is rapid and technically easy to perform with minimal patientdiscomfort.
The technical problems detected during charcoal localization includeblockage of the needle tip, difficulty in advancing the needle, andresidual linear tattooing of the skin after surgery in some cases.
Photomicrograph of the specimen after the US-tattoo shows a small infiltrative
ductal cancer. Adjacent to the mass, charcoal markings are observed as black
(arrows)

5. Methylene blue or toluidine blue dye injection.
It is accurate if done immediately preoperative but unfortunately they have tendency for rapid dispersion into adjacent healthy breast tissue forcing surgeon to excise more tissue volume.
It is used nowadays mostly for sentinel LN biopsy.

6. Intra-operative US.
It is a reliable, accurate, time efficient, technically feasible and helpfultool in Operative Room (OR), not only for tumor localization, but also forsurgical cut margin assessment.

7. Vacuum-assisted breast biopsysystem(VABB)(Mammotome)®
Allows localization, aspiration,resection, and removal of breastlesions that are visualized by US.
It vacuums, cuts, and removestissue samples, which are passedthrough the probe’s hollowchamber into a collection tray.

The main drawback ofMammotome ® isdifficulty of pathologicalmargin assessment if thelesion was proved to bemalignant due to multipledivisions of the lesion intosmall pieces.

8. Hematoma directed US-Guided (HUG) excision.
After VABB hematomas naturally fill the cavity, some authorssuggested that US could be used to localize the actual biopsy site ofnon-palpable breast lesions without a needle.
It makes Mammotome (VABB) not only a less invasive diagnosticprocedure, but also a localization procedure.

9. Breast Lesion Excision System (BLES).
It is a new advance for large biopsy procedure, with minimal complications.
Probe of BLES with the excised specimen

It avoids the problem of specimen slicing as in Mammotome
A specimen radiograph shows BIRADS 5 micro calcifications. This was confirmed as a DCIS.

10. Metal skin marker
It is placed inside the skin infront of the lesion that isvisible on two views , it isalso simple but inaccuratefor deep lesions and a largetissue volume will beexcised.

11. Breast metallic marker
It is also implanted under USguidance in breast cancer site totag the tumor bed in case ofcomplete or almost completeresponse to neoadjuvant therapy.
It is a localization method for theexpected non-palpable breastcancer after neoadjuvanttherapy.

12. MRI guided localization
When a suspicious lesion is found by MRI, localization with additionalmammographic or sonographic aid is always necessary , as MRIguided localization is much more difficult.
Woman with history of right BCS.
(A)BIRADS 4 oval mass (arrow) in the superomedial
quadrant of the left breast.
(B) US shows an intraductal oval mass (arrow), which was
not detected by the initial US.

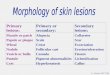
13. ROLL & RSL Radio guided Occult lesion Localization (ROLL) is highly effective localization
method as compared with WGL and can be used also to detect the sentinellymph node during the same injection.
Radio guided Seed Localization (RSL) involves percutaneous injection of asmall titanium seed radiolabelled with RAI inside the non-palpable lesion, Buta separate injection of radio colloid that can migrate to the axillary nodes isnecessary for SLNB.
Lumpectomy performed with constant feedback from the gamma probe allowing a
uniform lumpectomy specimen

14. Magnetically guided localizationRecently, Douek et al.(2015) reported the use of superparamagnetic iron
oxide (SPIO) as an alternative to the use of radioisotopes for SLNB, SPIOalso has a brown-black appearance, which acts as a visual stain.
A potential limitation of magnetic tracers is their visibility on MRI as anartefact during post-surgical follow up; however, the excision of theinjection site overcomes such problems.
Ahmed, M., Rubio, I. T., Klaase, J. M., & Douek, M. (2015). Surgical treatment of non palpable primary invasive and in situ breast cancer. Nature Reviews Clinical Oncology, 12(11), 645-663.

Aim of the work
The aims of this study are:
1. Encouraging the policy of screening.
2. Evaluation of the suitable methods for localization according to low income
countries resources.
3. Increasing the rate of BCS in management of breast cancer in Egypt.

Patients and Methods

This study was designed to be a prospective from June 2014 toOctober 2015.
32 patients with 35 non-palpable suspicious lesions ( BIRADS 4&5)were included in this study.

Inclusion criteria
Patients with non-palpable suspicious lesion.
Patients fit for general anesthesia.
Accepting consent of both localization and surgical procedure.

Exclusion criteria:
Patients with suspicious palpable breast lesion.
Patients with non-palpable non suspicious breast lesion, i.e. BIRADS3 or less
Patients unfit for general anesthesia.

Wire Guided Localization (WGL)After US localization of the lesion by breast radiologist, Insertion of theguide wire from a point at the site of planned surgical incision or near toit was done.
Breast localizing needle with a guide wire containing “V” shaped hook

Exact depth of the lesion, wire direction and angle of insertion were
obtained to facilitate intraoperative lesion identification.
All cases with WGL underwent surgical excision in the same day of
localization.
insertion of guide wire using US guidance

Wire in place with skin marking for planned incisions

Operative field during surgical procedure

Specimen after excision and orientation for pathological examination

US Guided Injection of Charcoal Suspension
After a breast radiologist identifies the lesions by US, 1-3 cc of thecharcoal suspension was injected on the superficial aspect of thelesion with continuous injection during needle withdrawal creating ablack track to the point of skin entry.
Prepared sterilized charcoal suspension

Exact depth of the lesion, needle directionand angle of insertion with the skin wererecorded to facilitate intraoperative lesionidentification.
Cases who offered Charcoal localizationunderwent surgical excision after one to sixdays.

Charcoal injection under US guidance

Skin mark of charcoal staining

Charcoal mark easily detected at the superficial aspect of the lesion

Specimen after surgical excision and orientation for pathological assessment

Microscopic picture of a benign lesion with charcoal particles (black color to the left)

Microscopic picture of a malignant lesion with charcoal particles (black color to the left)

RESULTS

WGL was used for 15 lesions in 14 patients, while Charcoal localization was used for 20 lesions in 18 patients.
15
20
GWL 42.8 %
Charcoal 57.2 %

Pathologic assessment revealed 12 malignantlesions and 23 benign lesions.
12
23
Malignant34.5%
Benign 65.5%

All BIRADS 4a lesions were benign. Three BIRADS 4blesions out of twelve were malignant. Four BIRADS4c lesions out of six were malignant. And five BIRADS5 lesions out of six were malignant.
4a 4b 4c 5
0
2
4
6
8
10
12
14
Malignant
Benign
Chart showing percentage of malignant lesions in each BIRADS category

All benign lesions were managed by excision, which was done in 21patients. Eight patients were offered BCS, Two patients weremanaged by MRM. NSM and LDF reconstruction offered for only onecase.
21
8
2 1
WLE
BCS
MRM
NSM & LDF
Diagram showing different surgical options offered for patients

Wire transection occurred during surgical excision in only one case.Remaining part of the wire and suspicious lesion were successfullyidentified.
Needle blockage during Charcoal injection occurred in two cases.One of them was managed by needle replacement, while other onewas managed by using the spinal needle trocar.

Discussion

Ko et al. reported using Charcoal localization for 164 lesions. Only 69 lesions of them were BIRADS 4 or 5 while 95 lesions were BIRADS 3.
In our study, we used WGL for 15 lesions and Charcoal localization for 20 lesions all of them were BIRADS 4 or 5.
We excluded BIRADS 3 lesions for more accurate indications and outcomes.

In the literature, 9–63% of non-palpable breast lesions are found tobe malignant.
In our study, we performed 35 localization procedures. Twelvelesions (35%) were malignant.
Rissanen et al. Reported Using WGL for 425 lesions. 27% of themwere malignant.

In our study, mean size of the lesions was 10.9 mm (4-20 mm) depending on lesion maximal diameter.
In their study Ko et al. reported that mean size of non-palpable lesions was 10 mm (4-32 mm)
In a study done by Ivanovic et al. they reported using WGL combined with intraoperative US for 32 lesions of a size up to 30 mm.
Canavese et al. reported lesion maximum diameter ranged from 3 mm to 38 mm.

In our study, Cases who offered Charcoal localization underwent surgical excision after 1-6 days.
Ko et al. reported time interval from three to 57 days in charcoal localization.
Ernst et al. and Canavese et al. reported performing surgical excision for all their cases of WGL arm in the same day of localization.
We also performed surgical excision for all cases offered WGL in the same day.

In our study, there was no difference inaccuracy of localization between bothmethods.
Rose et al. performed 219 excisionprocedures using charcoal localization and292 excision procedures using WGL with nodifference in accuracy between bothmethods.

However the charcoal localization has some superiorities over the other methods which could be summarized in the following:
Stable with no tissue dispersion.
No reaction reported.
Low cost.
No interference with histopathology.
No need for particular equipment or instruments.

Conclusions and Recommendations

In conclusion, Charcoal localization is a very simple, safe andaccurate method and we recommend to use it widely in communitiesof low resources.
As regard accuracy of WGL and its wide spread usage and greatexperience gained in using this method there will remain a place forwire localization.

Recommended