Faina Nakhlis
Division of Surgical OncologyDana Farber Cancer Institute
1st Annual IBC Patient Forum
May 13, 2017
Surgery for Inflammatory Breast Cancer (IBC): How and Why

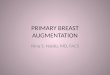
Histologic Evaluation
Dermal lymphatic invasionGrade 3 invasive ductal carcinoma
Image-guided core needle biopsy +/- skin punch biopsy

Initial Evaluation
Peau d’orange (dermal lymphatic invasion)
Unresectable disease
1. Neoadjuvant systemic therapy for cytoreduction
2. Modified radical mastectomy
3. Chest wall and regional nodal radiotherapy*
*Morris, Journal of Surgical Oncology 1983; Dawood et al. Annals of Oncology 2011

What is the Role of Surgery in IBCSurvival in 28 patients with IBC (23 patients with stage III disease) with and without surgery, 1969-1980
Hagelberg, Jolly, Anderson, Am Journal of Surgery 1984

What is the Role of Surgery in IBCRecurrence and survival in 107 patients with IBC with and without surgery, 1958-1985
Fields et al, Cancer 1989
Multivariate Analysis

What is the Role of Surgery in IBCResponse to chemotherapy, receipt of surgery and outcomes in 178 IBC patients
1974-1993, median follow-up 89 months (22-223 months)
Fleming et al, Ann Surg Oncol 1989

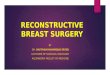
What is a Modified Radical Mastectomy
Mastectomy (total, simple) + Axillary lymph node dissection

Why Mastectomy
The cancer is often present throughout the breast at the time of diagnosis

Why Axillary Lymph Node Dissection?
Axillary lymph nodes are almost always involved at diagnosis and it may be unsafe to not to remove them

Drains
Round Jackson-PrattRound Blake Flat Jackson-Pratt

Why Should Immediate Reconstruction Not Be Done in IBC?
The amount of involved skin can go beyond what is clinically visible

Patterns of Breast Reconstruction in Patients Diagnosed with Inflammatory Breast Cancer: the Dana Farber Cancer
Institute’s Inflammatory Breast Cancer Program Experience
F. Nakhlis, M.M. Regan, Y.S. Chun, L.S. Dominici, J.R. Bellon, L. Warren, E.D. Yeh, H.A. Jacene, K. Hirko, A. Hazra, J Hirshfield-
Bartek, T. A. King, B. Overmoyer
SABCS 2015 Poster

Background
• Immediate reconstruction is not advised in IBC patients due to lack of safety data for skin-sparing mastectomy
• Data on breast reconstruction outcomes in IBC patients are scant
• Our experience with breast reconstruction in IBC patients was reviewed

Methods
• Retrospective analysis of IRB-approved DFCI IBC database
• Patients included in the analysis• Stage III IBC
• Sufficient response to preoperative chemotherapy to achieve resectability
• No preoperative radiotherapy
• No loco-regional progression or distant metastasis during preoperative chemotherapy

Results
Stage III IBC patients* (1997-2014), n=167
Immediate reconstruction,
n=12
Delayed reconstruction,
n=18
No reconstruction, n=135
*In two patients breast reconstruction took place but no information about reconstruction details and follow-up is available

Immediate Reconstruction, n=12*
Reconstructive Option Number of Patients
Tissue expander 3
Single stage implant 3
DIEP flap 1
TRAM flap 4
Latissimus Dorsi flap 1
*Eleven out of 12 patients with immediate reconstruction underwent surgery outside of DFCI

Delayed Reconstruction, n=18
Reconstructive Option Number of Patients
Tissue expander 1
TRAM flap 9
DIEP flap 5
Latissimus Dorsi and tissue expander 1
Latissimus Dorsi flap 2

Complications After Delayed Reconstruction
ComplicationDelayed Reconstruction
(N=18)
Reoperation for flap donorsite wound dehiscence
1 (6%)
Reconstruction loss 1 (6%)
Total Complications 2 (12%)

Future Direction
• Exploration of the role of local therapy (surgery and radiation) in stage IV IBC
•Axillary and extra-axillary lymphatic drainage in IBC and the potential for sentinel node mapping
Recommended