Surgery for Cervical Myelopathy
Peter Jarzem MD FRCSC
Spine Surgeon,
McGill University,
Montreal Canada

Surgery for Cervical Myelopathy
Peter Jarzem MD FRCSC
Spine Surgeon,
McGill University,
Montreal Canada

Disclosure
• Family Ownership of a physiotherapy clinic
• On the Publication committee for a surgical device manfacturer
• None of the devices or techniques will be discussed


Disclosure
• Family Ownership of a physiotherapy clinic
• On the Publication committee for a surgical device manfacturer
• None of the devices or techniques will be discussed

Outline
• Review 3 Cases
• Review the literature as it pertains to the cases
Objectives
• Learn when surgical referral is appropriate
• Gain awareness of some surgical techniques



Determining patient’s suitability for surgery
• 6 questions:
– 1)Is their documented deterioration?
– 2) Is the patient stable or improving?
– 3) Is the problem severe enough to warrant surgery?
– 4) Is the Patient Medically Fit?
– 5) Is the problem seen on advanced imaging consistent with the patients history and physical
– 6) Is there an underlying medical problem mimicking a cervical myelopathy ?
• => a highly selected population of patients

Baron E, Youn W. CERVICAL SPONDYLOTIC MYELOPATHY A Brief review of its pathophysiology, clinical course and diagnosis. Neurosurgery 60 (Suppl 1): S-35-S-41, January 2007

Baron E, Youn W. CERVICAL SPONDYLOTIC MYELOPATHY A Brief review of its pathophysiology, clinical course and diagnosis. Neurosurgery 60 (Suppl 1): S-35-S-41, January 2007
12% of CSM attributed to Spondylosis are later found to be something
else

Case 1: Mr Mild Milo Path
• 50 year old right handed male
• PHx hypertension
• Neck pain and more recently numbness in both hands stocking and glove distribution right > left
• Active in Karate
• Patient has normal function in sports and work activities
• No complaints related to function of upper, lower limbs, or of bowel.bladder

Case 1: Mr Mild Milo Path
• Physical Exam
• Normal pupils/cranial nerves
• Brisk triceps and lower extremity reflexes, hoffman and babinski on Rt. One beat ankle clonus
• Power and sensation objectively normal
• Subjective decrease in sensation to light touch in hands

Case 1





• Conclusions. The 3-year follow-up study did not show, on the average, that the surgery is superior to conservative treatment for mild and moderate forms of
Conclusions. The 3-year follow-up study
did not show, on the average, that the
surgery is superior to conservative
treatment for mild and moderate forms of
spondylotic cervical myelopathy.

How would you treat Case 1?

How would you treat Case 1?
• We told patient that he could probably be safely observed for one year and asked him to come to our clinic after one year.
• Advised against sports that risk a blow to the head or falls.

• 64 year old rt handed male
• Phx hypertension, elevated cholesterol, and low back surgery
• Fell down stairs hitting his head 3 days ago
• Discharged from another ER
• Has neck pain, arm weakness and numbness since his fall
• Patient cannot dress or feed himself. Is able to walk, but requires assistance
Case 2: Mr Central Path


• Physical exam shows 2-3/5 power in upper extremities rt worse than lt
• Numbness both limbs from elbows to fingers.
• Unsteady gait
• Normal sensation and power both legs
• Diminished reflexes UE, hyperreflexia LE
• Positive babinski bilat
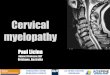
Case 2: Mr Central Path


Central cord Injury
• A syndrome characterized by disproportionately more loss of motor power in the upper extremities than the lower extremities
• Patients frequently complain of acute loss of power and sensation following a minor injury
• Typically there are no fractures

Acute decompression is a valid option

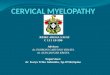
Laminoplasty
Spinous
process
lamina


• Now 4 weeks post operative
• Has improved hand power and sensation
• Too early to comment on final outcome
Case 2: Mr Central Path

• 70 year old female with progressive weakness of the arms legs last 3 mo
• Notes increasing difficulty walking and feeding himself particularly in the past 1 week
• PHx of Rheumatoid arthritis, hypertension, numerous joint replacements
• Subjective weakness and numbness in all extremities
Case 3: Mrs Tre Progessif

Physical Exam
• Multiple joint deformities, obese
• Weak in both upper and lower extremeties
• Altered sensation, decreased sensation of all four limbs
• Positive hoffmans, babinskis
• Hyperreflexia in both upper and lower extremeties

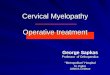
flexion extension


How to Treat? • Early treatment is important
• Historical high mortality rate in severely disabled patients
• Decompression from an anterior or posterior approach can lead to important functional recovery (Shen et al, Rheum Arth:Eval and surg tx, Spine J, 2004)
• Recovery is similar to patients with Cervical spondylotic myelopathy

• 81 pts with CSM
• Prospective between 2005 - 2007
• Age, sex, period of time since symptom onset, comorbidities

• Recovery reach a plateau at 6 months post surgery

Furlan et al, J Neurosurg Spine 2011
• Age and and number of previous medical conditions both predict complications and recovery from surgery.


• Patient made a good recovery
• Was able to self care, and walk around the house following 6 months of care
Case 3: Mrs Tre Progessif

Summary
• A high index of suspicion is required to detect an early or acute myelopathy. There are many etiologies
• Early myelopathy can be treated by observation
• Moderate or severe myelopathy is best treated with surgical decompression

Thank-you
Recommended