10/2/11
1
Deanna Rogers PT, CCRP Good Life Physical Therapy for Animals
Stretching
Outline
Flexibility Benefits of stretching Effects of stretching Anatomy, physiology and neurology of stretching End feels Precautions with stretching How to stretch
Flexibility and Stretching
Flexibility is the ability of the tissue to relax and respond to elongation forces1
Stretching addresses the flexibility of muscles, periarticular tissues, tendons, ligaments and skin
Stretching/flexibility deal with the intrinsic properties of the muscles and joints to go through an optimal range of motion2

10/2/11
2
Benefits of Stretching
Increase range of motion and promote fluid movement
Improve flexibility by elongating the tissue
Help relax muscles and reduce soreness3 Improve circulation and reduce stress (Mayo Clinic)
National Arthritis Foundation Reduce joint pain and stiffness Increase strength Reduce inflammation
Effects of Stretching
With regular long term stretching there are changes in the surrounding connective tissue and an increase the elasticity of the mm-tendon unit”2
There are also remodeling in the muscle where there is an addition of sarcomeres to the muscle (DeDeyne 2001)2 and changes the concentration and arrangement of the collagen within the muscle (Goldspink et al 1974, Williams and Goldspink 1978, Witzman et al 1982)
Passive stretching may reduce mm atrophy due to changes in the length of the mm fibers4,5,6 Study on mice – intermittent mm stretching helped to prevent atrophy
and loss of sarcomeres of immobilized tissues with varying durations in minutes per day of stretching
Decreased intramuscular connective tissue that develop during immobilization on those mice that received stretching
Effects of Stretching
Stretch tolerance – this is the theory that stretching may elicit an analgesic effect resulting in increased pain threshold without actual changes in the muscle stiffness (Magnusson 1988, Shrier 1999, Law et al 2009)7 May with neurological problems or chronic
musculoskeletal pain get continued muscle stiffness but improved joint ROM
10/2/11
3
Muscle Anatomy & Physiology
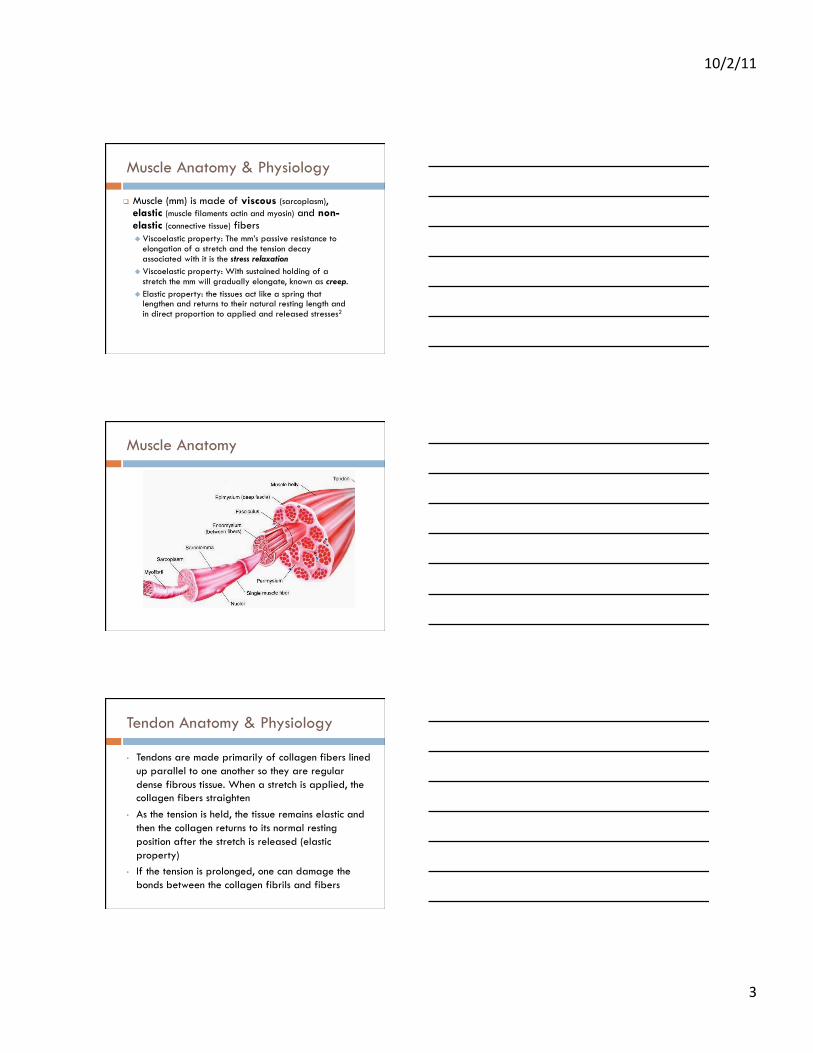
Muscle (mm) is made of viscous (sarcoplasm), elastic (muscle filaments actin and myosin) and non-elastic (connective tissue) fibers Viscoelastic property: The mm’s passive resistance to
elongation of a stretch and the tension decay associated with it is the stress relaxation
Viscoelastic property: With sustained holding of a stretch the mm will gradually elongate, known as creep.
Elastic property: the tissues act like a spring that lengthen and returns to their natural resting length and in direct proportion to applied and released stresses2
Muscle Anatomy
Tendon Anatomy & Physiology
• Tendons are made primarily of collagen fibers lined up parallel to one another so they are regular dense fibrous tissue. When a stretch is applied, the collagen fibers straighten
• As the tension is held, the tissue remains elastic and then the collagen returns to its normal resting position after the stretch is released (elastic property)
• If the tension is prolonged, one can damage the bonds between the collagen fibrils and fibers
10/2/11
4
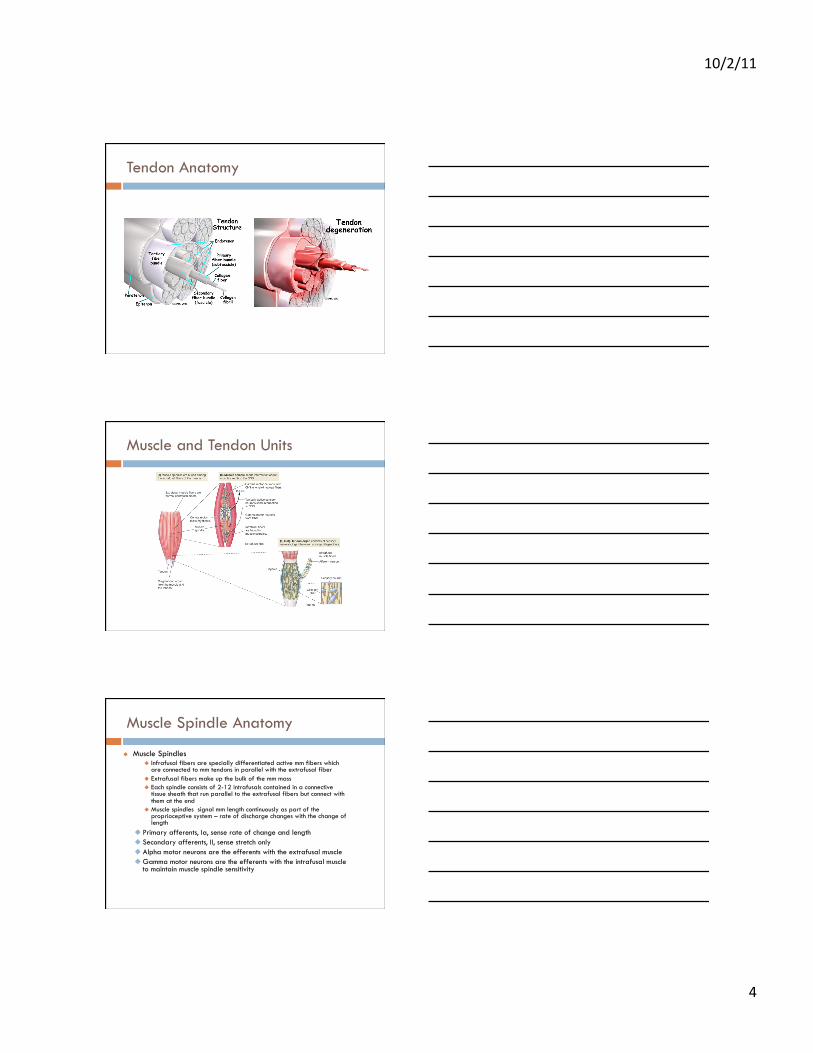
Tendon Anatomy
Muscle and Tendon Units
Muscle Spindle Anatomy
Muscle Spindles Infrafusal fibers are specially differentiated active mm fibers which
are connected to mm tendons in parallel with the extrafusal fiber Extrafusal fibers make up the bulk of the mm mass Each spindle consists of 2-12 intrafusals contained in a connective
tissue sheath that run parallel to the extrafusal fibers but connect with them at the end
Muscle spindles signal mm length continuously as part of the proprioceptive system – rate of discharge changes with the change of length
Primary afferents, Ia, sense rate of change and length Secondary afferents, II, sense stretch only Alpha motor neurons are the efferents with the extrafusal muscle Gamma motor neurons are the efferents with the intrafusal muscle
to maintain muscle spindle sensitivity

10/2/11
5
Muscle Spindles and Golgi Tendon Organs
• The receptors called proprioceptors or mechanoreceptors of the muscle spindle monitors the velocity and degree of the muscle stretch – When a muscle is stretched rapidly, the mm spindle contracts
which stimulates the primary afferent fibers and results in increased mm tension – monosynaptic stretch response
– there is less stimulation of the Ia and II spindle afferent fibers when the stretch is slow
• The proprioceptors or mechanoreceptors of the Golgi tendon organ detects the mm tension during a mm contraction, signaling the force of the contraction and inhibits contraction of the mm if there is too much force
Muscle Spindle Neurology
Muscle Spindle & GTO Neurology
10/2/11
6
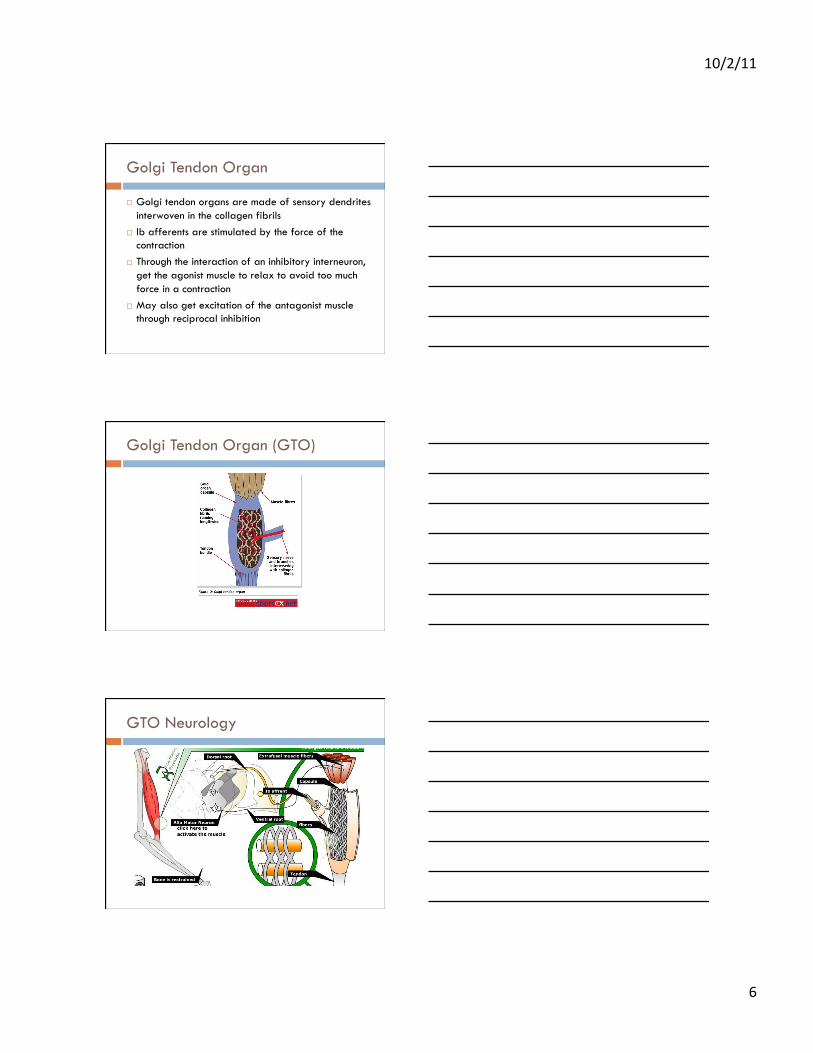
Golgi Tendon Organ
Golgi tendon organs are made of sensory dendrites interwoven in the collagen fibrils
Ib afferents are stimulated by the force of the contraction
Through the interaction of an inhibitory interneuron, get the agonist muscle to relax to avoid too much force in a contraction
May also get excitation of the antagonist muscle through reciprocal inhibition
Golgi Tendon Organ (GTO)
GTO Neurology

10/2/11
7
Muscle Spindle & GTO Neurology
Neuromodulation of Stretching
• Modulation of reflexes Inhibition of agonist due to activation of golgi
tendon organ so the stretching muscle relaxes May also get excitation of antagonist by the
golgi tendon organ Desensitization of stretch reflex due to
activation of muscle spindles by holding for 15-30 seconds – spindle reduces its’ opposing signaling2
Tissue Involvement with Hypomobility
• With tightness there may be shortening of the muscle belly itself
• There can also be restrictions in the skin, especially around scars
• Contractures are where there is shortening of muscles and tissue around joint that then limit ROM1 – Myostatic contractures have a musculotendinous
junction that is shortened – Scar tissue adhesions which can progress to fibrotic
adhesions (like a tie down) – Pseudomyostatic contracture where the muscle is
hypertonic and in a chronic state of contraction

10/2/11
8
End Feels
End feel is the quality of resistance and sensation at extremes of restricted movements or pain8,9.
Different sensations of movement barriers can be perceived according to the tissues limiting motion, the anatomical region, and pathological change. Cyriax, Kaltenborn and Paris describe a number of characteristic end-feels
Done passively, gently and with overpressure at end range – if there is pain at the end range, test with extreme caution10
Intrarater reliability good but interrater reliability is poor10
Capsular vs Noncapsular Patterns
Capsular patterns which indicate hypomobility of the entire joint capsule and vary for each joint. Typically accompany degenerative changes, arthritis, prolonged immobilization or acute joint trauma with effusion. Capsular patterns are more empirical data than research but basically each joint can have varying degrees of restrictions in certain motions8
Noncapsular patterns typically occur with intra-atricular mechanical blocks or extra-articular lesions
Types of End Feels8-11
Bony end feel - hard and often abrupt (elbow extension & should be painless). When accompanying a restriction it can suggest hypertrophic bony changes like those of DJD or possible malunion of bony segments following healing of a fracture
Capsular end feel – firm and leathery (shoulder ext rotational) Soft or Boggy – stiffness occurring early in the range and
increasing through the range often in a capsular pattern (acute inflammation, synovitis, soft tissue swelling)
Hard – tight resistance with a thick quality to it and definite stopping point after a smooth, friction free movement (chronic inflammation, scar tissue or shortened connective tissue, frozen shoulder)
Muscular or tissue stretch end feel – firm and rubbery/springy and less abrupt than capsular with a more subtle stopping point - often has an elastic resistance quality to it towards the end of the range (SLR, MCP extension, knee extension)

10/2/11
9
Types of End Feels
Soft end feel or mushy which is often tissue approximation – can be due to mm hypertrophy or tumors (elbow or knee flexion)
Muscle spasm end feel – movement stopped fairly abruptly with some rebound due to mm contracting reflexively. Can be early in the range so called an “early muscle spasm” or late in the range so called “late muscle spasm”. It’s often painful. Can be accompanied by capsular patterns of restrictions such as DJD with osteophyte formation, acute inflammation, or instability
Springy rebound end feel – occurs unexpectedly in the range and is springy. Usually indicates internal derangement end feel and often is in a noncapsular pattern (meniscal tear)
Empty end feel - the mms don’t contract to prevent the movement as that would cause compression of tissue but movement stops at the insistence of pt due to pain (acute bursitis)
Types of Stretching
Static stretching – slow elongation of the tissue, holding for a period of time, then returning to resting length
Dynamic stretching – slow cyclical elongating, holding and stretching doing exaggerated movements that are sport specific
Ballistic stretching – repetitive bouncing motion where the tendons are rapidly stretched and immediately relaxed
Proprioceptive neuromuscular facilitation – alternating activation of the shortened muscle with passive elongation developed by Dr.Herman Kabat in the 1950s
Resistance stretching – the targeted muscle is taken through resistance while doing eccentric and concentric contractions2
Precautions with Stretching
Overstretching – can result in poor soft tissue support so the joint may loose some stability and therefore result in injury1
The muscle will show its greatest resistance to a stretch if the stretch is done rapidly so advised to do stretch slowly to avoid eliciting the stretch reflex (Chambers 2004)2
Be cautious with older patients or those tissue exposed to chronic tightness as the collagen becomes less elastic, more dense and less stretch is needed before plastic deformation. Some studies show this can be minimized with stretching (Basey, E. J et al internet)2
Older patients will have increased mm stiffness and lower stretch tolerance

10/2/11
10
Precautions with Stretching
Do not do on cooled tissues - heated tissues can result in needing lower loads with significantly longer elongation benefits. Knight and colleagues (2001) showed benefit with stretching after active exercises, superficial heat, or ultrasound with the tissue having the deep heat of the ultrasound showing the most active and passive ROM improvements2
Can get improvements in range of motion even with 10-30 seconds of massage to musculotendinous unit (Huang et al 2010)12
How to Stretch
Frequency May need to be 2-3 times a day to 3x/week
depending upon the pt’s needs
Duration Hold 15-30 seconds for2-4 repetitions
Intensity Pt should be able to relax, should not be painful and
can try to gently increase range upon pt’s exhalation
How to Stretch….
American College of Sports Medicine recommends 15-30 second holds at 2-4 reps (2006)
Longer durations and more repetitions have not been found to produce significant benefits – more is just more
Slow rates of stretching permit greater stress relaxation and creep than faster rates
Slow rates of elongation limit stimulation of the stretch reflex
10/2/11
11
How to Stretch ….
Stretching 3-5 days per week may result in measureable increases in flexibility
Need rest periods between intense stretching sessions to allow adaptive remodeling
Consider cooling tissues in elongated position if you feel your results are not long lasting
Can take 2-3 weeks before seeing a difference Stretching should not be painful. Stretch to the point
of the limitation of the movement – not to pain. This is the “endpoint” of the stretch
Key Components to Stretching
• Make sure you are in a comfortable position • Allow the patient time to relax in their position • Support joint with both hands on your patient
– Stabilize the bone proximal to the joint – Stabilize the bone distal to the joint
• Slowly move the distal bone and with no signs of pain • Go to the point of resistance (endpoint) and then back off just a little
and HOLD • HOLD x 15-30 seconds • Slowly release • Repeat x 2-4 repetitions • Two joint stretches – may need less force
Thank You ….
Recommended


![Relationship Between Internal Derangement of ... Miguel... · 2013 [Relationship Between Internal Derangement of Temporomandibular Joint and Changes in Body Posture] VIII | Escola](https://img.pdfslide.us/doc/110x75/5e9a4966dd2b54332a11340c/relationship-between-internal-derangement-of-miguel-2013-relationship.jpg)