1
Emanuel P. Rivers, MD, MPH
Vice Chairman and Research Director
Emergency and Surgical Critical Care Medicine
Henry Ford Hospital
Clinical Professor, Wayne State University
Detroit, Michigan
Institute of Medicine, National Academies
Steroid Use in The Critically IllUpdate - 2015

2
What do these individuals havein common?
CORTISOL
Role of cortisol in maintaininghomeostasis during critical illness

3
Surgery and
Trauma
Drugs
Intense heat/cold
Metabolism
• Stimulation of gluconeogenesis– Amino acids to glucose in liver cells
• Reduction of protein stores in allcells except the liver
– Decreased protein synthesis, increasedcatabolism in muscle
• Mobilization of fat from adiposetissue
Cardiovascular
• Improves vascular tone:– Permissive effect on catecholamine and
vasoactive peptide synthesis.
– Enhances small vessel contractility in response tocatecholamines.
– Reverse adrenergic receptor desensitization.
– Inhibits NO-synthase in vascular endothelial cells.
– Inhibits phospholipase A2 and arachidonic acid.
• Increases contractility or stroke volume.
• Maintains fluid distribution and plasmavolume.Inflammation
Cortisol: Role in Inflammation
• Stabilizes lysosomal membranes
• Decreases permeability ofcapillaries
• Decreases migration of WBCs
• Attenuates SIRS– Reduces production of cytokines
– IL-1, IL-6, TNF-
(Guyton, 2000)(Munford, Am J Respir Crit Care Med, 2001)
(Briegel, Clin Investig, 1994)
Inhibition of NF-kB by cortisol
Modified from:Donato D, Am JResp Crit Care1996
SLeX
ICAM-1/2 E - Selectin
L-Selectin
CD11/18
‘Rolling’ ‘Sticking’ ‘Migration’
Activation
Endothelium
ICAM-1/2
Glucocorticoids
Tissue Injury
PMN - EC - Interactions
CD 11b/18

4
Macrophage
Migration
Inhibition
Factor
(Reichlin, NEJM, 1993)(Chrousos, NEJM, 1995)(Soni, Am J Med, 1995)
(Beishuizen, J Clin Endo & Meb, 2001)
Surgery and
TraumaDrugs
Infection (Sepsis) Intense heat/cold
Adrenal Insufficiency
ContemporaryAdrenal Dysfunction
Surgery and
Trauma
Intense heat/cold
DrugsCorticosteroids, Ketoconazole, Etomidate, Megesterol acetateRifampin, Phenytoin, Metyrapone, Mitotane
Primary AIHypothermia (primary AI)Autoimmune adrenalitisHIV infection, DrugsCytomegalovirus infectionAntiphospholipid syndromeMetastatic carcinomaSystemic fungal infectionsHistoplasmosis, Cryptococcus, Blastomycosis,TuberculosisAcute hemorrhageDisseminated intravascular coagulationMeningococcemiaAnticoagulation
Secondary AIPituitary or metastatic tumorPituitary surgery or radiationEmpty-sella syndromeCraniopharyngiomaSarcoidosis, histiocytosisPostpartum pituitary necrosisHIV infectionHead traumaGlucocorticoids

5
Additional Conditions
• Burns
• Head injury
• Failure to wean
• Subarachnoid hemorrhage
• Cardiogenic Shock and AMI
• Stroke
Cortisol Properties and Kinetics
• Comprises 95% of all glucocorticoid activity
• Small amount of mineralocorticoid activity
• 90-95% bound to CBG (transcortin), album.
• T½ of 60-90 min
• Circadian secretion (normal)– high am 20 ug/dL– low midnight 5 ug/dL
• Normal: 15-25 mg/day
• Stress:– 150 - 300 mg/day– level of 40-60 ug/dl– loss of diurnal variation

6
Critically Ill – High Risk
Hyponatremia and hyperkalemiaHypoglycemia (rare) or normoglycemiaHypotension resistant to volume resusc.Hyperdynamic circulationEosinophilia (usually mild)(Angelis M., J Am Coll Surg, 1996)
Classic Findings
Pituitary deficiencies (gonadotropin,thyroid, diabetes insipidus)Hyperpigmentation (rare)Vitiligo (rare)Weakness, fatigueAnorexia, weight lossNausea, vomiting, diarrheaAnemiaMetabolic acidosisUnexplained feverUnexplained mental status changes
Symptoms and Signs Suggestive ofHypoadrenalism in Critically Ill Patients
Cortisol Response in Critical Illness
Cortrosyn Stimulation Test
ACTH250 ugACTH1 ug
Random Cortisol Considered AdrenalInsufficiency in Critical Illness
Zaloga and Marik, Chest and Crit Care Med, 2001, 2002
<22
Fredlund, Hosp Prac, 1984<20
Chernow, Txt of Crit Care, 1989<20
Jurney, Chest, 1987<18
Soni, Am J Med, 1995<18
Devins, Crit Care Prac, 1991<15
Abboud, Mayo Clin Proc, 1986<15
Kidess, Mayo Clin Proc, 1993<15
Grinspoon, Clin Endo and Metab, 1994<13
McKee, Lancet, 1982<13
Knowlton, J Int Care Med, 1989<10
ReferenceCortisol (ug/dL)
25-30
Chernow, Crit Care Med, 1993

7
Cortisol Response and 28-day Mortality
82%T0 > 34, cortisol < 9Poor
67%T0 < 34, cortisol < 9
T0 > 34, cortisol > 9
Intermediate
26%T0 < 34, cortisol > 9Good
MortalityCortisol (T0), cortisolPrognosis
(Annane, JAMA, 2000)
Controversies in the Diagnosis

8
The Science of Cortisol MeasurementsSandwich Assay
cortisol
albumin or CBG
Bound or Total Free
Micropore Membrane
RIA
• ACTH– CST will vary during illness
– Decreased response to ACTH
• Albumin and CBG
• Protein binding– albumin
– volume of distribution
– hormone levels (i.e. estrogens)
– drugs
• Reduced metabolism– Decreased excretion
– Decreased breakdown
• Increased receptor resistance
• Inflammation
• Free fraction most important

9
• Whether serum free cortisol concentrations arecorrelated better with outcomes such as deathremains speculative.
– Patients with low albumin are sicker and tend todo poorly
– The dose of the ACTH – controversial
– More study is needed with free levels.
An Immunologic Balance
When Do You Treat?
ER or GPU ICU
The Harmonic Frequency of Inflammation

10
Hydrocortisone equivalent (g)
Hydrocortisone equivalent doses on 1st day- 70 kg body weight -
0,34
0,30
0,30
0,30
0,30
Less than 300 mg per day
Cortisol Response and 28-day Mortality
82%T0 > 34, cortisol < 9Poor
67%T0 < 34, cortisol < 9
T0 > 34, cortisol > 9
Intermediate
26%T0 < 34, cortisol > 9Good
MortalityCortisol (T0), cortisolPrognosis
(Annane, JAMA, 2000)

11
Design: Randomized, double-blind,
multi-center
Patients: Septic shock
Intervention:
Hydrocortisone (50 mg every six hours)
Fludrocortisone (50 ug once per day)
Main Outcome: 28-day survival innonresponders to CST
Effect of Low Doses of Hydrocortisone andFludrocortisone on Mortality in
Patients with Septic Shock(Annane JAMA 2002)
229 Non-respondersRandomized
115 Treatment &
114 controls
10% decrease in
28-day mortality
17% reduction invasopressors use
New Perspective andControversies on Steroids in
Critical Illness

12
No OutcomeBenefit
13
Now what should I do about steroids?
The Original Trial
• 8 hour time frame
• Minimal steroid use
• 56% mortality
The Corticus Trial
• 72 hour time frame
• Excluded patientstreated – over 50%
• Less severe patients –30 - 40% mortality
• Similar benefit withhigher mortality
14.5% Reductionin Vasopressor
Use if Optimized
Hold steroid useuntil the patient
has beenresuscitated and
endpoints met(6-8 hours)
• Septic shock patients presenting to the ED:– Adequate volume resuscitation– Vasopressor dependency
• Adrenal dysfunction is common in high-risk ED patients.
• 19% incidence of adrenal dysfunction in ED patients.
ACADEMIC EMERGENCY MEDICINE 1999; 6:626–630

14
• The effects of low or high APACHE II score and early or latehydrocortisone initiation are additive.
• In patients with high APACHE score (= 19), the early initiation ofhydrocortisone increased the survival rate from 19.8% to 41.2% (p= 0.021).
• Likewise, in patients with low APACHE score (< 19), the earlyinitiation of hydrocortisone increased the survival rate from 55.0%to 83.3%.

15
Crit Care Med 2009 Vol.37,No.3
AVP stimulates cortisollevels and cortisol inhibits
AVP
• Significant interaction between vasopressininfusion and corticosteroid treatment (p<0.008).
• In patients:
–Steroids, NE and vasopressin:
• Mortality - 35.9%
–Norepinephrine alone:
• Mortality - 44.7%, p<0.03
Crit Care Med 2009 Vol.37,No.3

16
• Patients who did not receive corticosteroids, butvasopressin:– increased mortality was seen compared with norepinephrine
(33.7%vs.21.3%, respectively, p<0.06).
• Patients who received vasopressin infusion:
– corticosteroids significantly increased plasma vasopressinlevels by 33% at 6 hours (p<0.006)
– 67% at 24 hours (p<0.025) compared with patients whodid not receive corticosteroids.
Crit Care Med 2009 Vol.37,No.3

17
Alternative Uses of Steroids

18
• For all trials, regardless of duration of treatment and dose, use ofsupra-physiologic corticosteroids doses did not significantly affectmortality.– Methylprednisolone 30 mg/kg
– Dexamethasone 3-6 mg/kg
• Physiologic doses:– Short course of less than 7 days
– Hydrocortisone <300 mg/day is in.
• Targeting high risk patients:– Treating patients insensitive to catecholamines.
– After adequate volume resuscitation.
– Treat early
• Improved efficacy:– After adequate resuscitation
– Vasopressin
– Treat within 9 hours in severe illness
• Need better laboratory diagnosis:– Cortisol levels and stimulation test are inaccurate

ECMO for Adults: It Not Just About the Heart
Kaysie Banton, MD FACSTrauma Medical Director – UMN Health
Disclosures
• No financial disclosures
• I don’t endorse any specific branded product.
• ECMO for respiratory support outside of CPB in the OR is an off-label use of the equipment and technology.
Minnesota is for Outdoors People

Ice Fishing
November 15, 2013 Little Rock Lake, MN
Transported in full arrest

Active rewarming
ECMO for rewarming
ECMO for rewarming

ECMO for Rewarming Pulmonary Edema
ECMO for Rewarming Pulmonary Edema
• Restoration of spontaneous circulation was achieved in 32 patients (54.2%)
• 12 patients (20.3%) survived hypothermia.
• In multivariate analysis, ECMO-assisted resuscitation showed a 6.6-fold higher chance for survival (relative risk: 6.6, 95% confidence interval: 1.2–49.3, P = .042).
Hospital Course
• Arrived 11/15 20:30
• Decannulated 11/20 3:00 PM
• 5 day ECMO run
• Decannulated to mechanical ventilation
• Discharged to LTACH 12/27
• Home in January – back at work

Hospital Course1.S/P Cardiopulmonary arrest2.Acute respiratory failure, s/p ECMO3.Spontaneous left pneumothorax- resolved4.Spontaneous right pneumothorax- resolved5.Acute renal failure-- required hemodialysis, last run 12/13/136.Anemia of critical illness7.Thrombocytopenia--improved 8.Multiple organism Pneumonia- resolved9.Bacteremia- resolved10.Leukocytosis stable 11.Bilateral pleural effusions s/p Chest tube drainage 12.Mesenteric fluid collection s/p percutaneous drain placement13. Acalculous cholecystitis with cholecystomy tube
University of Minnesota
University of Minnesota

First Respiratory ECMO
ECMO for ARDS
5/28/2012 14:20pH Arterial: 7.19 (LL)pCO2 Arterial: 62 (H)PO2 Arterial: 53 (L)Bicarbonate Arterial: 23Base Deficit Art: 6.0
5/28/2012 16:42pH Arterial: 7.23 (L)pCO2 Arterial: 61 (H)PO2 Arterial: 39 (LL)Bicarbonate Arterial: 25Base Deficit Art: 4.1
How it works
• Sweep– CO2 elimination
• Flow– Blood flow
• FdO2– Fractional Delivered O2

Dual lumen cannula
ECMO
Does it work for respiratory failure in adults?
• 1971: NIH trial in moribund patients - 90% mortality.
• 1986 Gattinoni: 49% survival (nonrandomized)
• 1992 Morris: No survival benefit over computerized vent management

ARDS Management
ECMO for Adult ARDS1988 – 2010 Annual and Cumulative
University of Minnesota volume
In 2008: 17 Cases/2400 HoursIn 2013: 39 Cases/5000 Hours
Projected 2014: 62 Cases/10,239 Hours

Why such a drastic increase?
• Old news- CESAR trial
• New news- OSCILLATE, OSCAR trials
• Advances– Cannulation
– Transport
– Management
• Survival
Old News- CESAR Trial UK
High Frequency Oscillatory Ventilation
OSCILLATE Trial • 47% in the HFOV group died in-hospital, vs. 35% receiving conventional
low-tidal volume ventilation – RR for death with HFOV was 1.33 [1.09 - 1.64; p=0.005].
– Trial stopped for harm at this point, short of planned 1,200 patient enrollment
• Those in the HFOV arm also:– Required more sedatives (8 mg/hr of midazolam vs 6 mg/hr)
– Received paralytic agents (83% vs. 68%);
– Required vasopressors or other vasoactive drugs (91% vs. 84%, p=0.01) • and for longer: 5 days vs. 3 days (p=0.01).
Niall Ferguson et al. High-Frequency Oscillation in Early Acute Respiratory Distress Syndrome. OSCILLATE Trial. NEJM Jan 2013.

High Frequency Oscillatory Ventilation
OSCILLATE Trial • 47% in the HFOV group died in-hospital, vs. 35% receiving conventional
low-tidal volume ventilation – RR for death with HFOV was 1.33 [1.09 - 1.64; p=0.005].
– Trial stopped for harm at this point, short of planned 1,200 patient enrollment
• Those in the HFOV arm also:– Required more sedatives (8 mg/hr of midazolam vs 6 mg/hr)
– Received paralytic agents (83% vs. 68%);
– Required vasopressors or other vasoactive drugs (91% vs. 84%, p=0.01) • and for longer: 5 days vs. 3 days (p=0.01).
Niall Ferguson et al. High-Frequency Oscillation in Early Acute Respiratory Distress Syndrome. OSCILLATE Trial. NEJM Jan 2013.
Success with specific indications
Success with specific indications
Success with specific indications
The Journal of Thoracic and Cardiovascular Surgery c Volume 145, Number 4
The Journal of Thoracic and Cardiovascular Surgery c September 2012
Bridge to Transplant
Advances in cannulation

Advances in Cannulation
Advances in Transport
• Older circuits very bulky
• Many places to snag
and inadvertently
decannulate
Advances in Transport
• Much smaller circuits
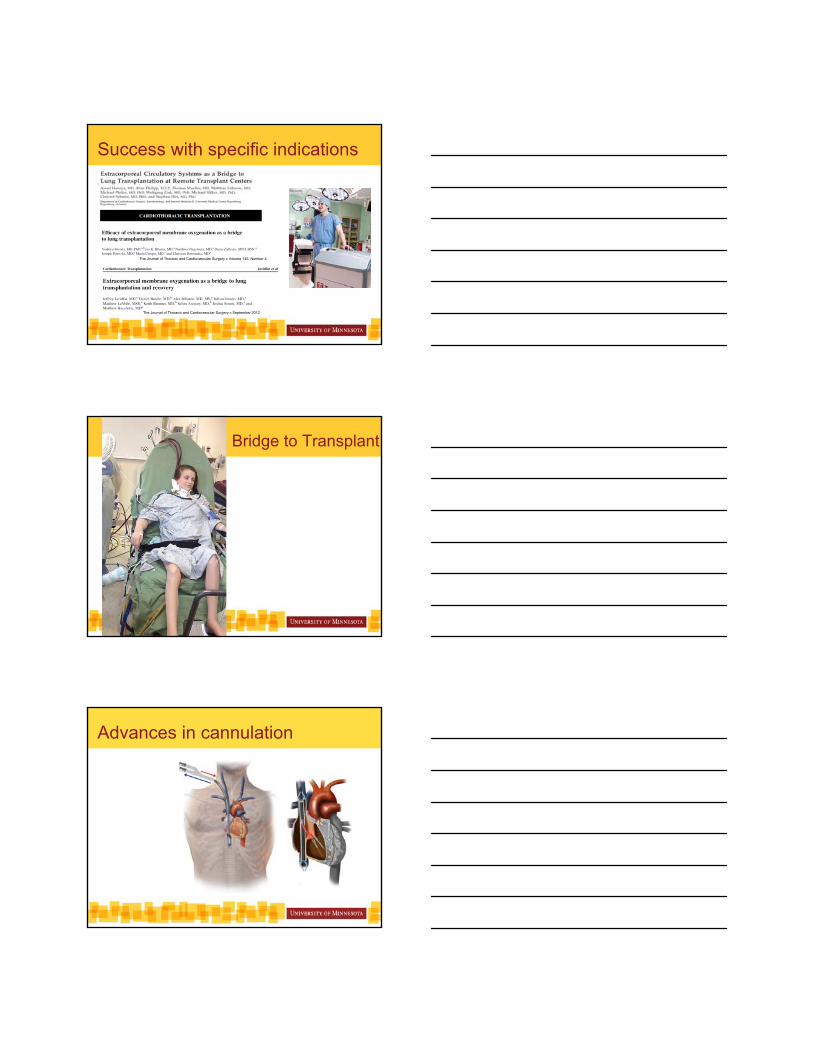
ELSO Registry July 2012
International Overall Patient Outcomes
Total Surv ECLS Surv to DC Neonatal Respiratory 25,746 21,765 85% 19,232 75% Cardiac 4,797 2,928 61% 1,912 40% ECPR 784 496 63% 304 39% Pediatric Respiratory 5,457 3,556 65% 3,061 56% Cardiac 5,976 3,855 65% 2,913 49% ECPR 1,562 843 54% 630 40% Adult Respiratory 3,280 2,094 64% 1,808 55% Cardiac 2,312 1,243 54% 891 39% ECPR 753 276 37% 207 27% Total 50,667 37,056 73% 30,958 61%
New Algorithm Earlier to ECMO
ECLS- Patient Complications
• Blood loss
Circuit priming
Bleeding
• Thrombocytopenia
Platelet interactions with circuit
• Thrombosis/thromboembolism
Thrombus formation in circuit
• Air embolism
• Catheter infection and sepsis

Indications
• Hypoxemic respiratory failure
• Hypercapnic respiratory failure
• Respiratory failure as a bridge to transplant
• Severe pulmonary air leaks
• Failure to wean from cardiopulmonary bypass in the OR
• Heart failure
• Massive pulmonary embolism
• Cardiac arrest
Patient selection-hypoxemia• Potentially REVERSIBLE acute respiratory failure
• Severe ARDS– PaO2/FiO2 < 120
• Despite– PEEP ≥ 15
– Protective lung ventilation
– Prone positioning
– Correction of volume overload (diuresis or CRRT)
– Optimization of perfusion (restoration of oncotic pressure, intravascular volume, and inotropes)
Patient selection-hypercapnia
• Obstructive lung disease or primary hypercapnic respiratory failure
• Permissive hypercapnia for ARDSNet ventilator management
• Uncompensated hypercapnia, pH < 7.2 despite conventional management
• Inability to maintain safe inflation pressure (Pplat < 30 cm H2O)– PaCO2 deemed too high despite appropriate conventional
mechanical ventilation
– Concomitant severe metabolic acidosis
– High intracranial pressures

Contraindications
No absolute contraindications
• Avoid for IRREVERSIBLE causes, unless bridge to transplant
• Severe medical co-morbidities– Documented irreversible brain injury
– Severely immunocompromised host without chance of recovery
– Malignancy with limited life expectancy
– Irreversible multi-system organ failure or other futile condition
– s/p prolonged cardiac arrest with prolonged chest compressions and likely anoxic brain injury
Relative Contraindications
• Mechanical ventilation with high inflation pressures (Pplat > 30 cm H2O) or high oxygen concentrations (FiO2> 0.8) for ≥7 days
• Advanced age
• Weight > 125 kg or BMI > 45
• Contraindications to anticoagulation– Recent or expanding CNS hemorrhage
– Active hemorrhage
• Inability to receive blood products
• Bridge to lung transplant in patient not previously listed
ECMO

Thank you!
References1. Extracorporeal Life Support Organization Database. http://www.elso.org/Registry/DataRequest.aspx
2. Ferguson,N et al. High-Frequency Oscillation in Early Acute Respiratory Distress Syndrome. OSCILLATE Trial. NEJM Jan 2013.
3. Giesbrecht GG. Cold stress, near drowning and accidental hypothermia: a review. Aviat Space Environ Med 2000; 71:733.
4. Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, Hibbert CL, Truesdale A, Clemens F, Cooper N, Firmin RK, Elbourne D; CESAR trial collaboration. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009 Oct 17;374(9698):1351-63
5. Ruttman et al Prolonged extracorporeal membrane oxygenation-assisted support provides improved survival in hypothermic patients with cardiocirculatory arrest. J of Thor Cardiovasc Surg 2007 134:3 594–600
6. Soar J, Perkins GD, Abbas G, et al. European Resuscitation Council Guidelines for Resuscitation 2010 Section 8. Cardiac arrest in special circumstances: Electrolyte abnormalities, poisoning, drowning, accidental hypothermia, hyperthermia, asthma, anaphylaxis, cardiac surgery, trauma, pregnancy, electrocution. Resuscitation 2010; 81:1400.

Lori B. Sweeney, MD
VCU Health System
Simplifying Glucose Control
in the ICU
What we know for certain
High blood glucose correlates with severity of illness
High glucose correlates with mortality
Blood sugars >200 mg/dl result in glucosuria
Blood sugars > 200 mg/dl impair wound healing
Blood sugars <40 mg/dl may result in cardiac and brain ischemia
IV insulin is the safest method of administration
Meta-analysis pre-NICE SUGAR

Meta-analysis post-NICE SUGAR
Death more frequent in tight glycemic control
arm
< or = 180 mg/dl
0.5% hypoglycemia
Severe hypoglycemia (<40 mg/dl)
Mortality difference: some studies suggest an increase of nearly 10% in patients with hypoglycemia, controlling for severity of illness
15% verses 25%
2009 American Association of Clinical Endocrinologists and American Diabetes Association consensus statement on the management of inpatient hyperglycemia
In the intensive care unit (ICU), the threshold to start treatment is a BG of <or=180 mg/dL
I.V. insulin is the treatment of choice in critically ill patients because of its rapid onset and offset of action
Once i.v. insulin is started, the BG should be maintained between 140 and 180 mg/ dL
A lower BG target (110-140 mg/dL) may be appropriate in selected patients. Targets of <110 mg/dL or >180 mg/dL are no longer recommended

Special Populations
Myocardial Infarction
Post-CABG
Prolonged mechanical ventilation
Neurological
Goal may be closer to 110 mg/dl
Renal Insufficiency
Insulin algorithm
Blood glucose testing no less frequent than every two hours
Insulin infusion rate should not be stopped when glucose values consistently fall below the glucose target range but above hypoglycemia (should have variable dosing regimens algorithms)
Staff should be knowledgeable or protocol should address anticipated changes in insulin requirement: interruption of nutrition, new renal failure
Should allow for transition to subcutaneous insulin regimen

Insulin algorithm
Continued, steady progress is more important than rapid achievement of goal (remember hypoglycemia is risky)
Should include hypoglycemia order set
Continuous IV Insulin Protocol
See handout : Adult Inpatient IV Insulin Infusion Orders
Goal established at the start
4 hours stability before increasing BG check to 2 hr interval
Start at insulin-sensitive doses (you make about 24 units of insulin every 24 hours
Hypoglycemia algorithm
Anticipated need for increased insulin after meal

Hypoglycemia (nurse-based therapy)
For treatment of BG below 70 mg/dl in a patient with an altered level of consciousness:
administer 25 ml dextrose 50% IV and start IV dextrose
5% in water at 100 ml/h
In a patient with an altered level of consciousness and no available IV access
give glucagon 1 mg IM, limit X 2
Recheck BG and repeat treatment every 15 minutes until blood glucose is 80 mg/dl, X 2-3 readings
Hypoglycemia (nurse-based therapy)For treatment of BG below 70 mg/dl in a patient who is alert and able to eat and drink, administer 15-20 g of rapid acting carbohydrate such as:
one 15-30 g tube of glucose gel
4 ( 4g) glucose tabs
4-6 ounces orange or apple juice
6 ounces “regular” sugar sweetened soda
8 ounces skim milk
For treatment of BG below 70 mg/dl in an alert and awake patient who is NPO or unable to swallow:
administer 20 ml dextrose 50% IV and start IV dextrose
5% in water at 100 ml/h
Emergent Perioperative Hyperglycemia Management
Perioperative complications are higher in patients with hyperglycemia (as evidenced by glucose of 180 mg/dl or greater)
Risk is greater in patients without previous diagnosis of diabetes
Must rule out DKA before surgery to address the electrolyte and acid-base derangements
HHS patients need volume resuscitation before surgery
Realistic goal is 110-180 mg/dl

Emergent Perioperative Hyperglycemia Management
All patients receiving insulin before surgery require insulin in the perioperative period
Surgical performance measure is glucose <180 mg/dl in the 18-24 postoperative period (will likely influence reimbursement)
Frequent blood sugar measurements in an effort to identify glucose > 160 mg/dl, as IV insulin is reasonable at this value
IV insulin is best administered per established safe and efficacious protocol
If patient is not eating, IV insulin is best
Parenteral Nutrition
Provide calories equal to 100-120% estimated basal energy expenditure (Harris-Benedict equation)
Permissive underfeeding for obese patients or marked hyperglycemia/hypertriglyceridemia
Obtain blood glucose before start
Limit dextrose to 150-200 gms on day 1
Parenteral Nutrition
2 glucose values > 150, add 0.1 units of regular insulin per gram of dextrose
If renal failure then 0.05 units per gram
Increase by 0.05 units up to maximum of 0.2 units/gram
Then consider permissive underfeeding
Try not to increase glucose content until glycemic control is achieved
If hypoglycemia occurs: was PN discontinued? Otherwise, decrease by 50%

Tube Feeding
Pts without DM: short acting insulin until tube feeds reach 30-40 ml/hour, especially if there is higher chance for discontinuationGlucose should be checked before each feeding
and no sooner than 4 hours after prior feedingA very reasonable starting point is 1 unit for every
15 gms of carbs, remember you can make orders “responsive” If the 4hour post-feed glucose is greater than 160
mg/dl, then increase by 10-20%
Tube feeding continued
Once tube feeds are greater than 40 ml/hr for at least 12 hours, then consider intermediate acting insulin
Dosed before tube feeds: 1 single dose for 12 hours tube feeds or q 8 hours for continuous tube feeds
0.2-0.4 units/kg is a reasonable starting dose (remember peak will be around 3-5 hours)
What is the most common cause of
hypoglycemia using such an
approach?
Switching to SQ insulin Estimate 24 hour basal insulin requirements of 24 hours using
the last 8 hours requirement X 3, then take 80% If not stable, then be conservative and overlap with the drip Options: give 1/3 dose as NPH Q 8 H
give 1/2 dose as Glargine/Detemir Q 12 Hgive full dose as Glargine/Detemir Q 24 H
Remember overlap IV insulin, 1-3 hours or less if glucose falls below 100 mg/dl
Sliding Scale: 1 U/15 g carbohydrate (insulin sensitive) to 2-3 U/15 g carbohydrate (insulin resistant)
BG Unit of rapid acting insulin
<80 none
80-100 4

Insulin sensitivity factor 1500/Total daily dose of insulin equals the mg/dl of glucose
than 1 unit or rapid acting insulin will reduce from baseline
1500/25 = 60 mg/dl
Blood glucose Units of rapid acting
<80 none
80-100 4
101-160 5
What about the severely insulin resistant ICU patient?
Extreme Insulin Resistance
51 y/o male admitted with fever and probable sepsis secondary to perirectal abscess
Intubated and hypotensive on catecholamine infusion
Outpatient medications unknown at the time of admission
Family members report “diet-controlled diabetes”

Extreme Insulin Resistance
Blood sugar on admission was 678 mg/dl
Blood pressure 69/42, HR 112 bpm
Exam: morbidly obese, +acanthosis nigricans
Insulin per protocol: 29 units regular insulin per protocol
Blood glucose 390 mg/dl
Extreme Insulin Resistance Usually multiple concurrent etiologies
Most often occurs in obese patients (high underlying insulin resistance)
Underlying mechanisms: sympathetic activation, pro-inflammatory cytokines Unrestrained lypolysis
Impaired insulin secretionGlucose productionCortisol secretion
Step-wise approach
Is it really insulin resistance?

Is insulin reaching the patient?
Concurrent with a new bag or syringe of insulin
Infusion connected into maintenance IV or other tubing
Connections tight
Good blood return
Step-wise approach
Is it really insulin resistance?
Underlying electrolyte abnormalities?
Hypercalcemia, Hypocalcemia, Hyperkalemia, Hypomagnesemia
Step-wise approach
Is it really insulin resistance?
Underlying electrolyte abnormalities?
Culprit medications or change in nutrition?

Nutrition and medications Change in nutrition: TPN, Intralipid
New medication: review the medication list
(catecholamines, corticosteroids, propofol, megace, octreotide)
Discuss with pharmacy (which medications can be changed from lipid or glucose emulsion/diluent/)
Extreme insulin resistance
TPN: Add regular insulin to the TPN itself
No more than 50% of the total daily insulin dose
Decreases the risk of hypoglycemia
Steroid-induced hyperglycemia
Major effect 6-8 hours after administration
Results primarily in post-prandial excursion

NPH timed with steroids0.1 units/kg per 10 mg prednisone (or steroid equivalent) up to a maximum of 0.4 units/kg
Lasts 6-8 hours, longer in renal dysfunction
If not at at goal increase next dose by 10-20%
Clore JN, Thurby-Hay L. Glucocorticoid-induced hyperglycemia. Endocr Pract. 2009 Jul-Aug;15(5):469-74.
Questions?

Telemedicine: New Horizons in Healthcare
Kaysie L. Banton, MD Department of Surgery, Trauma,
Critical Care
Disclosure
• Disclosure of Relevant Financial Relationships
– I have no financial relationships to disclose.
• Disclosure of Off-Label and/or investigative Uses
– I will not discuss off label use and/or investigational use in my presentation.
Learning Objectives
• Understand that Telemedicine encompasses a wide range of technologies and uses from simple to sophisticated.
• Review limits of telemedicine.
• Understand the most common Telemedicine programs

• The practice of medicine and/or teaching of the medical art, without direct physical physician-patient or physician-student interaction, via an interactive audio-video communication system employing tele-electronic devices.
What is it?
• Requires some type of electronic communication
• Providing scarce resources
• Low tech to extremely high tech

Low Tech Versions
• Minimal equipment to purchase
• No new software
• Limited in ability to gain additional information Depends on cellular access or internet access
• Quick, nearly ubiquitous, low cost
iHealth apps
iHeath/iPhone apps
• Fitness/Activity tracker
• Sleep monitor
• O2 Sat monitor
• BP monitor– Wrist
– Arm
– Docking station
• Body analysis scale
• Regular scale
• Pulse oximeter
• Smart-Gluco Monitoring System
• iHealth align

Example - Mayo
• Tele Hand Trauma – Hand specialists
– Pictures taken of actual patients and transmitted via iPads
Allows visual decision for acuity decision making
Collaboration UMN/UW
• Post operative wound surveillance project
• Ask patients to text pictures of surgical wounds and answer questionnaire 3 times over first month after surgery in lieu of post operative visit with surgeon
• Provider evaluates photos and questionnaire
Medium Technology
• Requires some type of hardware at user end
Tele - Dermatology
• http://www.youtube.com/watch?feature=player_detailpage&v=KWOUF9Tlleo
Tele - Otolaryngology

ROP standard image set (right eye).
Walter M. Fierson et al. Pediatrics 2015;135:e238-e254
©2015 by American Academy of Pediatrics
Tele - Ophthalmology
High Tech
• High up front investment in high tech equipment and/or software– At hub and at each site
• Training
• 24h staffing
• Lots of data
Technology can become obsolete very quickly
High Tech Examples
• U of M Health Tele-ICU– 24h Critical Care Nurse
– 24h Intensivist
• Real-time cardiac and vital sign monitoring
• High definition two way audio-visual communication set up in each ICU bed at 5 ICUs (soon a 6th to be added)

Tele ICU
• Does require in-house physician to place lines, intubate, perform examination
• Does NOT require in-person presence to write orders, change vent, adjust medications, run codes or to communicate with patient or loved ones– End of Life Conversations in the Tele ICU
research project
Highest Tech
• Remote Surgery 2001– Lindbergh Operation
• Highly trained specialists at both sites
• Surgical Robot
– Military TraumaPod 2025
– Space Station TeleSurgery
– Oceanic Aquarius underwater Base
• Remote Surgical Telementoring

Oceanic Aquarius underwater Base
The da Vinci surgical robot. Image: Intuitive Surgical Systems
Telementoring
TeleTrauma/TeleTriage
• Several states do ED based Trauma Room evaluations
• Used in mass casualty situations and disasters with high frequency
• Provide oversight of severe trauma patients with experienced ED and TS specialists when needed
• Improved mortality rates
• Increased transfers while reducing transfer times
• Telemedicine for Disaster management
• Military use
• Mass Casualty
• TeleMentoring

Tele ICU Trauma
• Working to provide additional Trauma Surgeon evaluation of trauma patients admitted to ICU within the FV system
Tele Stroke Programs
Key interventions in Acute Stroke
• Differentiate stroke from mimics
• IV t-PA
• Triage for endovascular treatment
• Initiate treatment for other neurological emergencies

Pooled DataTime to Treat
Lancet 2004; 363: 768–74
ATLANTIS, ECASS, and NINDS rt-PA stroke trials
Potential Thrombolysis CandidatesNINDS Recommendations
Time Interval Time Target
Door to Triage 10 minutes
Access to neurological expertise
15 minutes
Door to CT completion 25 minutes
Door to CT interpretation
45 minutes
Door to treatment 60 minutes
Door to monitored bed 3 hours
Limited Delivery of Established Treatments
• Median Time to arrival to ED between 3-6 hours
• Paul Coverdell National Acute Stroke Registry: 48% arrive within 2 hours.
• IV t-PA treatment rates: 0.5%-4%
• Endovascular Numbers are worse.

Barriers
• Need for disease expertise
• Not enough stroke neurologists
• Not enough radiologists
• Need 24/7/365
• Time limitations
Stroke Systems of Care
• Joint commission Designation
• Quality Measures
• State Systems
• Minnesota Dept of Health: – stroke ready hospital
– primary stroke center
– comprehensive stroke center
STRokE DOC trial
• 234 patients randomized to Telemedicine consultation vs. telephone consultation
• Correct treatment decision: 98% telemedicine, 82% telephone
• No difference in functional outcome or mortality
Lancet Neurol. 2008 Sep;7(9):787-95

Telemedicine/Telestroke
• Improve time to treatment
• Increase number of patients treated with IV t-PA
• Prevents unnecessary transfers
• Better triage
• Improves Imaging interpretation times
• Early mobilization of resources (Angiography Suite/endovascular/OR/ICU)
• Identify potential research candidates

What's Next
• Telepresence
• Research Trials– UCSF using iHealth data
• Transitional Care monitoring
• Chronic Disease management– Currently non-physician providers communicating
to physician from patient bedside
– VA home monitors
• Virtual Support Groups
Summary
• Limitless use
• Quickly changing field
• Will incorporate technology that we haven’t even imagined yet

Is Cardiac Arrest in the Hospital a Preventable Event?
Raúl J. Gazmuri MD, PhD, FCCM
Resuscitation Instituteat Rosalind Franklin University
andCaptain James A. Lovell Federal
Health Care Center(Section of Critical Care Medicine)
53nd Annual Weil/UC San Diego Symposium on Critical Care & Emergency Medicine
(April 12, 2015)
In Hospital Cardiac Arrest
• Extrapolation of the incidence of in-hospital cardiac arrest reported by GWTG suggests that each year 209,000 (quasi CI; 192,000–211,000) people are treated for in-hospital cardiac arrest
• In 2011, survival to discharge was 24.2% (95% CI, 23.5%–24.9%) for patients of any age; 23.9% (95% CI, 23.2%–24.6%) for adults; and 40.2% (95% CI, 34.2%–46.2%) for children (excluding neonates)
Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation 2013 January 1;127:e6-e245
In Hospital Cardiac Arrest
• In 2011, 17.6% (95% CI, 17.0%–18.3%) of patients of any age or 17.7% (95% CI, 17.1%–18.4%) of adults and 14.1% (95% CI, 9.8%–18.3%) of children (excluding neonates) had VF or pulseless VT as the first recorded rhythm
• Of these, 43.0% (95% CI, 41.0%–45.0%) of adults and 52.8% (95% CI, 36.5%–69.1%) of children (excluding neonates) survived to discharge
Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation 2013 January 1;127:e6-e245

In Hospital Cardiac Arrest• Up to 2/3 of hospital cardiac arrests are
considered preventable (Hodgetts et al. Resuscitation, 2002;54:115-23)
• 118 arrest cases compared with 132 non-arrest controls (Hodgetts et al. Resuscitation, 2002;54:125-131)
• Abnormal respiratory rate (p=0.013)• Abnormal breathing indicator (p<0.001)• Abnormal pulse (p<0.001)• Reduced systolic blood pressure (p<0.001)• Abnormal temperature (p<0.001)• Reduced pulse oximetry (p<0.001)• Chest pain (p<0.001)• Nurse or doctor concern (p<0.001)
• A significant proportion of hospitalized patients experience serious adverse events during their stay.
• These events include cardiac arrest, respiratory failure requiring emergency intubation, unplanned ICU admissions, and death.
• Most of these events are not abrupt but preceded by hours of physiologic deterioration (e.g., 6 to 8 hours) that can recognized (e.g., tachypnea, tachycardia, hypotension, decreased O2
saturation, and changes in mentation).
FIRST CONSENSUS CONFERENCE ON MEDICAL EMERGENCY TEAMS (METS)(Critical Care Medicine 2006;34:2463–2478)
Efferent Limb(response)
Afferent Limb(recognition)
RAPID RESPONSE SYSTEM(Critical Care Medicine 2006;34:2463–2478)
Event Detection
Patient Deteriorates
TriggerMET/RRT/CCO/
MERS
Crisis Resolved Cardiac Arrest Team
Trauma Team
CodeTeam
Specialized Resources
Administration Oversees Function
Data Collection and Analysis for Performance Irovement

JCAHO 2011NPSG16.01.01 has been moved to the standards for
Critical Access Hospitals and Hospitals (PC.02.01.19, HR.01.05.03, PI.01.01.01)
• PC.02.01.19 The hospital recognizes and responds to changes in a patient's condition. Note: Hospitals are not required to create "rapid response teams" or "medical emergency teams" in order to meet this standard. The existence of these types of teams does not mean that all of the elements of performance are automatically achieved.
• EP #1. The hospital has a process for recognizing and responding as soon as a patient's condition appears to be worsening.
JCAHO 2011NPSG16.01.01 has been moved to the standards for
Critical Access Hospitals and Hospitals (PC.02.01.19, HR.01.05.03, PI.01.01.01)
• EP #2. The hospital develops written criteria describing early warning signs of a change or deterioration in a patient's condition and when to seek further assistance
• EP #3. Based on the hospital's early warning criteria, staff seek additional assistance when they have concerns about a patient's condition.
• EP #4. The hospital informs the patient and family how to seek assistance when they have concerns about a patient's condition.
• Organizations like the American Heart Association, Institute for Healthcare Improvement, and Society for Critical Care Medicine are promulgating some form of RRS, and many hospitals are implementing them.
• Although the structure may vary, they all rely on the prompt identification and treatment of acutely critically ill hospitalized patients.
RAPID RESPONSE SYSTEMS(Critical Care Medicine 2006;34:2463–2478)

• The data about effectiveness of RRS has been controversial:
• Several single-center studies have shown a reduction in the rate of cardiac arrests by using before-and-after RRS implementation studies.
• However, meta-analyses have questioned whether there are benefits and have suggested that further research is required (Chan PS et al. Arch Intern Med 2010;170:18-26; McGaughey J et al. Cochrane Database of Systemic Reviews 2007;3:CD005529.9)
RAPID RESPONSE SYSTEMS
In Hospital Cardiac Arrest
• Before-after evaluation of implementing an early warning score system (Drower et al. N Z Med J. 2013 Nov 1;126(1385):26-34)
• 600-bed tertiary teaching hospital in New Zealand during the two 12-month periods between March 2009 and March 2011
• 168 cardiac arrests during the 24 month period • The incidence cardiac arrests dropped from 4.67 to 2.91 per
1000 admissions (mean difference 1.77, 95%CI 0.59-2.94)
• The number of cardiac arrests dropped from 8.5 to 5.5 arrests per month (mean difference 3.0, 95%CI 0.78-5.22)
• Introduction of an EWS system in addition to an existing cardiac arrest team response decreased the incidence of in-hospital cardiac arrests in a tertiary hospital in New Zealand

J Community Hosp Intern Med Perspect. 2015 Apr 1;5(2):26716. doi: 10.3402/jchimp.v5.26716. eCollection2015.Modified Early Warning System improves patient safety and clinical outcomes in an academic community hospital.Mathukia C1, Fan W1, Vadyak K1, Biege C1, Krishnamurthy M2.Author informationAbstractBACKGROUND AND OBJECTIVE:Severe adverse events such as cardiac arrest and death are often heralded by abnormal vital signs hours before the event. This necessitates an organized track and trigger approach of early recognition and response to subtle changes in a patient's condition. The Modified Early Warning System (MEWS) is one of such systems that use temperature, blood pressure, pulse, respiratory rate, and level of consciousness with each progressive higher score triggering an action. Root cause analysis for mortalities in our institute has led to the implementation of MEWS in an effort to improve patient outcomes. Here we discuss our experience and the impact of MEWS implementation on patient care at our community academic hospital.METHODS:MEWS was implemented in a protocolized manner in June 2013. The following data were collected from non-ICU wards on a monthly basis from January 2010 to June 2014: 1) number of rapid response teams (RRTs) per 100 patient-days (100PD); 2) number of cardiopulmonary arrests 'Code Blue' per 100PD; and 3) result of each RRT and Code Blue (RRT progressed to Code Blue, higher level of care, ICU transfer, etc.). Overall inpatient mortality data were also analyzed.RESULTS:Since the implementation of MEWS, the number of RRT has increased from 0.24 per 100PD in 2011 to 0.38 per 100PD in 2013, and 0.48 per 100PD in 2014. The percentage of RRTs that progressed to Code Blue, an indicator of poor outcome of RRT, has been decreasing. In contrast, the numbers of Code Blue in non-ICU floors has been progressively decreasing from 0.05 per 100PD in 2011 to 0.02 per 100PD in 2013 and 2014. These improved clinical outcomes are associated with a decline of overall inpatient mortality rate from 2.3% in 2011 to 1.5% in 2013 and 1.2% in 2014.CONCLUSIONS:Implementation of MEWS in our institute has led to higher rapid response system utilization but lower cardiopulmonary arrest events; this is associated with a lower mortality rate, and improved patient safety and clinical outcomes. We recommend the widespread use of MEWS to improve patient outcomes.
Rapid Response System (RRS)
Integration of MERS with CODE System (May 2011-Present)
Medical Emergency Response System (MERS)
Unique number to call ICU for Physiological Deterioration based on EWS (Nov 2006-Apr 2011)
List of Early Warning Signs (EWS)
Pager to ICU fellow (Jul 2,000-Oct 2006)

0
10
20
30
40
50
60
70
80
2004 2005 2006 2007 2008
CARDIAC ARREST CODES OUTSIDE ICU (%)
MERSMERS
0.0
1.0
2.0
3.0
4.0
5.0
6.0
RTW MED ICU OTHER
MERS DISPOSITION /1000 DISCHARGES (2007)
0
1
2
3
4
5
6
RespiratoryRate
Heart Rate AcuteMentalStatusChange
Use ofRespiratoryAccessoryMuscles
SystolicBlood
Pressure
Repeatedor
Prolongedseizures
OxygenSaturation
UrineOutput
AcuteBleeding
Arterial pH SerumSodium
MOST COMMON MISSED WARNING SIGNS

Table 3: ADVANCED CLINICAL DETERIORATION (ADULT PATIENTS)
CLINICAL PARAMETER THRESHOLD FOR RRS ACTIVATION
Respiratory Rate <8 or >28 breaths/min
Oxygen Saturation < 90% on O2 or FiO2 > 60%
Use of Respiratory Accessory Muscles Yes
Heart Rate < 40 or > 140 beats/min
Systolic Blood Pressure < 80 or > 200 mm Hg
Arterial pH < 7.25 units
Serum Potassium > 6.5 mEq/L
Repetitive Seizure Episodes Yes
Marked Change in Mental Status Yes
Chest Pain Yes
Advanced clinical deterioration represents a stage in which values for any of the listed parameter substantially deviate from acceptable values reaching levels indicative of a potential life-threatening condition, and therefore identifies a need of emergency evaluation and likely transfer to a higher level of care.

SO220%
Systolic BP18%
Respiratory Rate15%
Mentation13%
Chest Pain13%
Res Acc Muscles
10%
HR4%
Seizures4%
Syncope2%
Urine1%
WARNING SIGNS (MERS; n = 110)March 2010 – April 2011
AFFERENT LIMB AT FHCC(Recognition and Activation)
A dedicated red phone rings in the CCU
• An ICU nurse receives the call, collects basic information, and passes the call to the ICU resident.
• The ICU resident assesses the information given and provides guidance:
• Transfer patient to ED
• Assess at bedside
• Ask for more information
• Request to CODE aactivation
EFERENT LIMB AT FHCC(Response)


RAPID RESPONSE SYSTEM at FHCC
• The efferent limb works well without having a “dedicated team” using instead the ICU and ED resources.
• For calls originating outside the main hospital, the typical response is to instruct transfer of the patient to the ED.
• In 60% or more of the calls the patient is moved to a higher level of care.
• The ED is an safe and effective place for rapid evaluation and triage of a patient suffering physiological deterioration, and circumvents treatment delays inherent to deploying and ill equipped team to remote areas
• For call originating in med-surg units, proper response is bedside assessment to determine whether direct ICU admission is warranted
RAPID RESPONSE SYSTEM at FHCC
• A RRS call is not a CODE call.
• A RRS call implies there is physiological deterioration but at a pace that allows a brief discussion to initiate a response that is commensurate to the clinical situation.
• RRS also enables reductions in false codes.
• The option for activating the CODEremains available through the process (~1%)
RAPID RESPONSE SYSTEM at FHCC

Table 1: RAPID RESPONSE SYSTEM (FY 2013 and FY 2014)
CODES FY-2013 FY-2014
Total CODES, n 30 28
Response Time, average min 2.2 2.9
Total Resuscitative CODES, n (%) 13 (43) 12 (43)
ROSC (n) 4 8
24 hour Survival (n) 0 7
28 day Survival (n) 0 7
Total Resuscitative CODES Outside ICU/ED/OR, n (%) 2 (15) 4 (33)
Total Non-Resuscitative CODES, n (%) 17 (57) 16 (57)
Appropriate (n) 15 8
Inappropriate (n) 2 8
CLINICAL DETERIORATION
Total Calls for Clinical Deterioration (n) 185 202
Calls from building 134, n (%) 86 (46) 106 (52)
Calls from building 133, n (%) 61 (33) 62 (31)
Calls from building 131, n (%) 29 (16) 31 (15)
Calls from other locations, n (%) 9 (5) 3 (2)
Calls for Clinical Deterioration Converted to CODES, n (%) 3 (1.6) 1 (0.5)
Disposition
Stay in or Return to the Ward of Origin, n (%) 64 (34) 69 (34)
Transfer to ICU, n (%) 87 (47) 97 (48)
Transfer to 133-MEDSURG, n (%) 27 (15) 28 (14)
Other, n (%) 7 (4) 8 (4)
Resuscitative CODES refers to CODES in which a resuscitation intervention was used (i.e., chest compressions, defibrillation). Non-resuscitative CODES refers to deployment of the CODE team but without delivering a resuscitation intervention and considered appropriate when the event could have placed the patient at risk of a life-threatening event or was perceived at such by the caller.
• More than 200,000 patients suffer cardiac arrest in the hospital every year in the United States
• Most of cardiac arrest (~2/3) occur after progressive physiological deterioration over hours (even days) and are potentially preventable
• Rapid Response Systems can recognize and intervene to avert preventable in-hospital deaths; with the recognition arm being the most critical
• In the event of a cardiac arrest, resuscitation efforts can benefit from enhanced monitoring capabilities guiding the effort based on physiological measurements, and also benefit from available therapeutic capabilities
SUMMARY
Recommended