
A boon or A bane..???
SPLINTING
BY VIGNESH PRABHU.T C.R.I

WHAT IS SPLINT..???It is defined as rigid or flexible device that
maintains in position of a displaced or movable part , also used to keep in place
and protect an injured part.
Splinting in dentistry ..??“the joining of 2 or more teeth into a
rigid unit by means of fixed or removable restorations or devices.

History..!!! A Phoenician mandible from 500BC found in modern day Lebanon which has two carved ivory teeth attached to four natural teeth
by gold wire.Obin and Arvin's (1951) -self curing internal splint.
Harrington(1957) modified the splint by incorporating cemented stainless steel wire.
Ward & Weinberg (1961) – developed new techniques using a plastic matrix or using wire reinforcement.
Splints have thus come a far way to INTRACORONAL BONDABLE FIBER SPLINTING of the present.

Should reduce movement 3 dimensionally
Centre of rotation of the affected teeth must be located in the remaining supporting bone.
No inflammation
Minimum one third of bone support remaining.
Should allow for oral hygiene methods
Should not irritate soft tissues.
principles

objectives
To provide rest
For redirection of forces
For redistribution of forces
To preserve arch integrity
CONTINUE…
Restore of functional stability
Psychological well being
To stabilize mobile teeth during surgery , especially during regenerative therapy
To prevent the eruption of unopposed teeth

Indications To stabilize moderate to advance tooth mobility, that
cannot be reduced by other means that has not responded to occlusal adjustment and periodontal therapy.
Stabilize teeth in secondary occlusal trauma
Stabilize teeth with increased mobility which interfere with normal masticatory function
Facilitate scaling and surgical procedures.
Prevent tipping & drifting of teeth.
Prevent extrusion of unopposed teeth.
Stabilize teeth after acute dental trauma i.e. .sub luxation , avulsion.etc.

CONTRA INDICATIONS
Moderate to severe tooth mobility in the presence of periodontal inflammation & or primary occlusal trauma
Insufficient number of firm/ sufficient firm teeth to stabilize mobile teeth.
Prior occlusal adjustment has not been done on teeth with occlusal trauma or interferences.
Patient not maintaining oral hygiene.
When the sole objective of splinting is to decrease tooth mobility following the removal of splint.

classification
According to the period of stabilization
According to the type of material
According to the location on the tooth
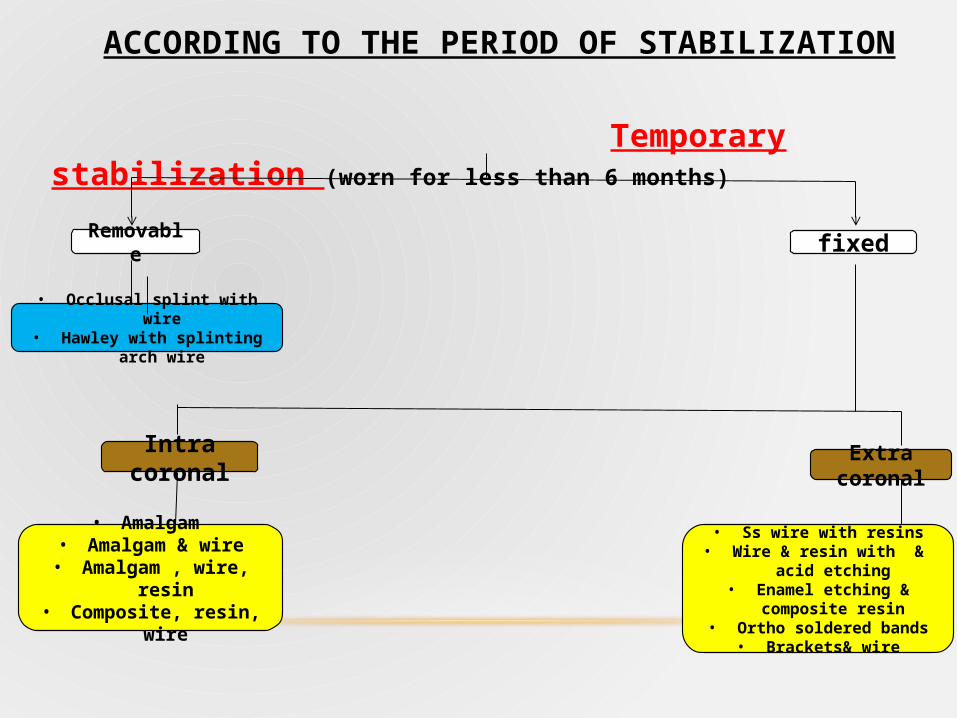
ACCORDING TO THE PERIOD OF STABILIZATION
Temporary stabilization (worn for less than 6 months)
Removable fixed
• Occlusal splint with wire• Hawley with splinting arch wire
Intra coronal Extra coronal
• Ss wire with resins• Wire & resin with & acid etching• Enamel etching & composite
resin• Ortho soldered bands• Brackets& wire
• Amalgam • Amalgam & wire
• Amalgam , wire, resin• Composite, resin, wire

PROVISIONAL STABILZATION
• To be used for months up to several years e.g. acrylic splints, metal band
• permanent splints ; used definitely
Removable / fixed • Extra / Intra coronal• Full / Partial veneer crowns
soldered together• Inlay / Onlay soldered together

ACCORDING TO THE TYPE OF MATERIAL
• Bonded composite resin button splint.
• Braided wire splint.
• A- SPLINTS
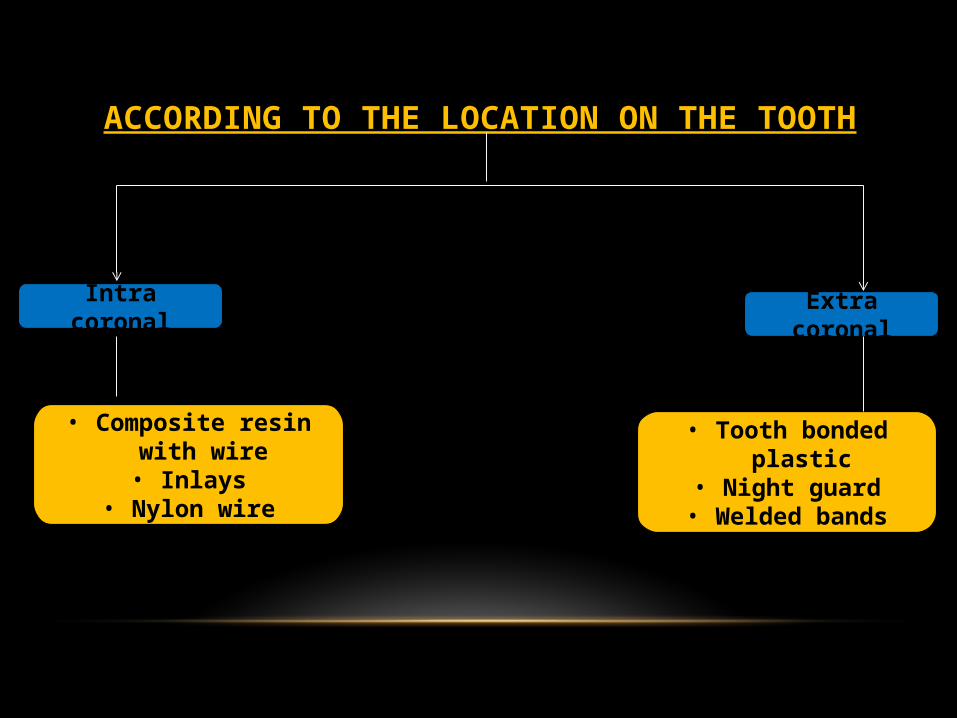
ACCORDING TO THE LOCATION ON THE TOOTH
Intra coronal Extra coronal
• Tooth bonded plastic• Night guard• Welded bands
• Composite resin with wire• Inlays
• Nylon wire
COMMONLY USED SPLINTS
• Splinting for anterior teeth
• Splinting of posterior teeth
Direct bonding system
Intra coronal wire
Acrylic wire resin splint
Intra coronal amalgam wire splints
Bite guard
Rigid occlusal splint
Composite splint
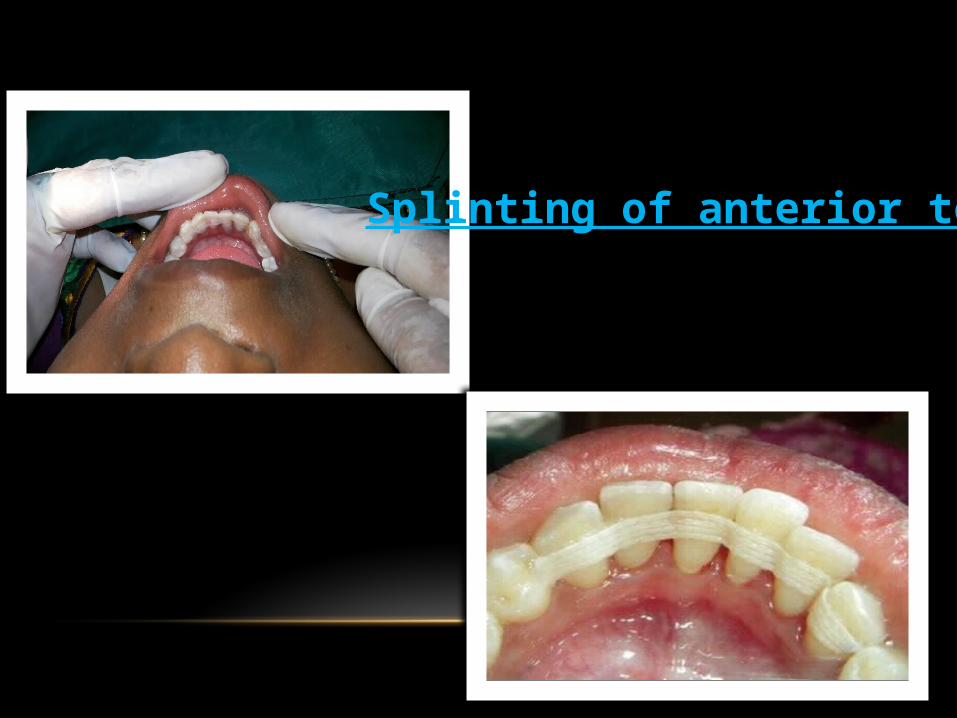
Splinting of anterior teeth

Splintee Tooth that needs support
Splinters Adjacent teeth that provide support.

Direct bonding system
Acid etching Bonding agent
Composite curing

INTRA CORONAL WIRE SPLINT Slot preparation Ss wire adapted into the slot
Sealed with resin

VARIATION OF THE “A” SPLINT
A 1mm deep M / D box is prepared parallel to the long axis of tooth
SnF/CA(OH)2 varnish is applies & threaded pin is then placed.
Ss is wire is adapted around the pin .

SPLINTING FOR POSTERIOR TEETH

INTRA CORONAL AMALGAM WIRE SPLINTS

BITE(NIGHT) GUARD
Bruxism with occlusal wear
Primary or secondary occlusal traumatism.
Anterior open bite with trauma.
Impinging over bite with periodontal involvement.
Following orthodontic treatment.( as retainer).
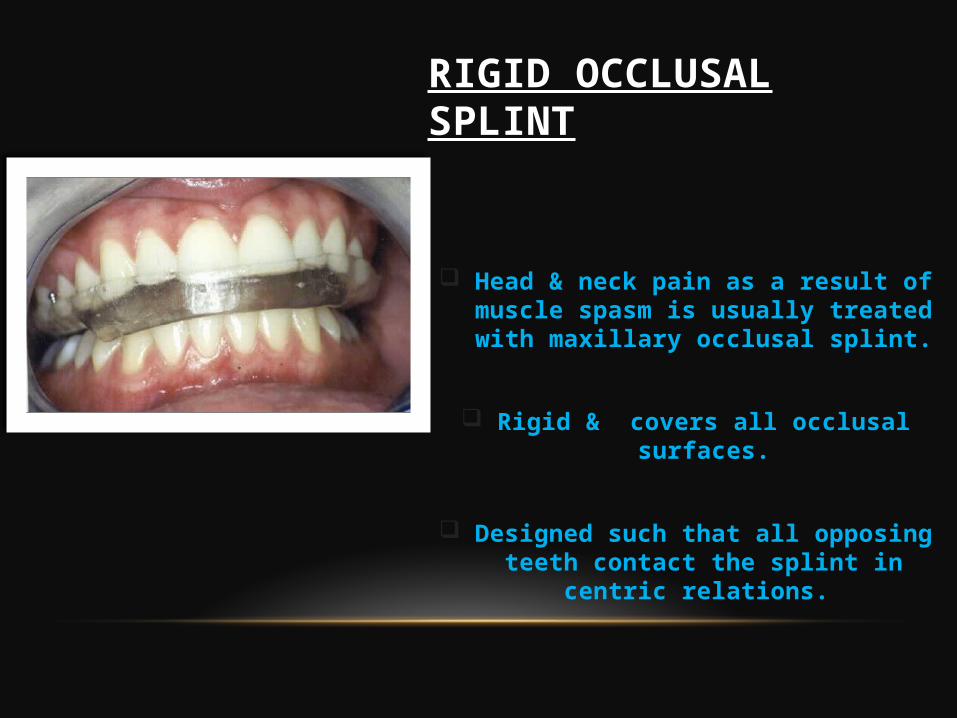
RIGID OCCLUSAL SPLINT
Head & neck pain as a result of muscle spasm is usually treated with maxillary occlusal splint.
Rigid & covers all occlusal surfaces.
Designed such that all opposing teeth contact the splint in centric
relations.

FIBER REINFORCED SPLINTING
Fibre reinforced splinting

PROCEDURECoronoplasty Acid etching
Flowable composite

It have good flexural strength and do not require mechanical
retention.
Faster & easier technique.
Superior in all properties compared to all other
splinters.
Composite curing
Post operative
Strength
• May establish final stability & comfort for patient with occlusal trauma.
• Helpful to decrease mobility and accelerate healing following acute trauma to the teeth.
• Allows remodelling of alveolar bone and PDL for orthodontically , splinted teeth.
• Helpful in decreasing mobility favouring regenerative therapy.
• Distributes occlusal forces over a wider area.

Weakness
Hygienic
Mechanical
Biological

REFRENCES
World workshop 1989 iii -4
Lemmerman k; rationale for stabilization JP 1976; 47 (7) : 405 – 411.
Trochtchberg delhi : combined amalgam – wire acrylic splint jp 198: 39 : 255 – 259/
Singer B : intracoronal aesthetic splinting comp. 1996: 17 (5) : 459- 48.
Leib et al : occlusal bite splint comp .1996: 17 (11) : 1081 -1090.
The periodontics syallabus 2nd ed 82- 85.

Doubts???

`
Recommended

















