Psychiatry Overview
Inflammatory Bowel DiseaseSonia Friedman MD
Associate Physician, Brigham and Women’s Hospital
Division of Gastroenterology, Department of Medicine
Associate Professor, Harvard Medical School

Sonia Friedman, MD
• Yale Medical School• Medicine Residency @ Hospital
of the University of Pennsylvania• Gastroenterology Fellowship @
Mount Sinai Medical Center • Associate Professor of Medicine
@ HMS– Clinical focus: Crohn’s disease and
ulcerative colitis– Research focus: IBD and
reproduction

Conflict of Interest
• No conflicts of interest

Key Learning Objectives
• Diagnosis and evaluation of inflammatory bowel disease type and severity
• Medical management of inflammatory bowel disease

Overview of Inflammatory Bowel Disease (IBD)
INDETERMINATECOLITIS2
10%-20% of IBD patients
Colitis32%
Ileitis22%
Ileocolitis45%
CROHN’SDISEASE3
Pancolitis47%
Left-sideddisease
25%
ULCERATIVE1
COLITIS
IBD>1.6 million persons in US
Proctitis28% % at time
of diagnosis
1. Loftus EV, et al. Gut. 2000;46:336-343; 2. Marion JF, et al. In: Kirsner JB, ed.
Inflammatory Bowel Disease. 5th ed. Philadelphia, Pa: WB Saunders Co; 2000:315-
325; 3. Loftus EV, et al. Gastroenterology. 1998;14:1161-1168.

Ulcerative Colitis Crohn’s Disease
Age-Specific Incidence of IBD*
*Per 100,000 population
Reprinted with permission from Lashner BA. In: Stein SH and Rood RP, eds. Inflammatory Bowel Disease: A Guide for Patients and Their Families. Philadelphia, Pa: Lippincott-Raven Publishers; 1999:23-29.
10
0
2
4
6
8
0 20 40 60 80
10
0
2
4
6
8
0 20 40 60 80
Age (yrs) Age (yrs)

UC: Presenting Symptoms
• Bloody diarrhea
• Abdominal cramping
• Tenesmus
• Weight loss
• Fevers
• Symptoms depend upon extent and severity of inflammation

Endoscopic Spectrum of SeverityUC – Spectrum of Disease
Normal
Moderate
Mild
Severe
Reprinted with permission from AGA Clinical Teaching Project. IBD. 3rd ed. 2002.

Classification of UC Severity
MILD• <4
stools/day ± blood
• Normal ESR• No signs of
toxicity
MODERATE• ≥4
stools/day± blood
• Minimal signs of toxicity
SEVERE• >6 bloody
stools/day
• Fever
• Tachycardia
• Anemia or ESR
FULMINANT• >10 stools/day• Continuous bleeding• Toxicity• Abdominal
tenderness/distension• Transfusion requirement• Colonic dilation on x-ray
Truelove SC, Witts LJ. Br Med J. 1955;2(4947):1041-8; Kornbluth A, Sachar DB. Am J Gastroenterol. 2010;105(3):501-23.

CD: Presentation
• Diarrhea
• Chronic abdominal pain and tenderness
• Weight loss
• Fever
• Perianal disease
• Symptoms vary with location of disease

CD: Clinical Features
⚫ Abdominal pain
⚫ Tenderness
⚫ Diarrhea
⚫ Weight loss
⚫ Cramps
⚫ Distention
⚫ Vomiting
⚫ Diarrhea
⚫ Pain
⚫ Air/feces in urine
⚫ Types– Enteroenteric– Enterovesical– Retroperitoneal– Enterocutaneous
Inflammation Obstruction Fistulization
Adapted with permission from AGA Gastroenterology Teaching Project. 3rd ed. 2002.

Crohn’s Disease: Severity• Remission: Asymptomatic either spontaneously or after medical or
surgical intervention and not on steroids.
• Mild to moderate: Ambulatory and able to tolerate an oral diet, no dehydration, toxicity, abdominal tenderness, mass, obstruction, or > 10 percent weight loss.
• Moderate to severe: Failed treatment for mild to moderate or prominent symptoms such as fever, weight loss, abdominal pain and tenderness, intermittent nausea or vomiting, or anemia.
• Severe-fulminant disease: Persisting symptoms despite conventional glucocorticoids or biologics as outpatients or individuals presenting with high fevers, persistent vomiting, intestinal obstruction, significant peritoneal signs, cachexia or evidence or an abscess

Indications for Biologic Therapy in IBD
Indications for Early Treatment in Crohn’s Disease (CD)
• Complex fistula
• Deep ulceration on endoscopy
• Young age (Age<30)
• Steroid dependence/resistance
• High risk anatomy
• Severe disease activity (weight loss, low albumin and/or hemoglobin)
Indications for Early Treatment in Ulcerative Colitis (UC)
• Moderate to Severe UC
• Steroid-dependent, refractory UC
• Refractory Pouchitis
• Maintenance of disease in remission



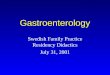
The image demonstrates a new gastrocolic fistula (solid white arrows). Multifocal involvement of the small bowel and terminal ileum is also present (dashed white arrows).

39 year-old male with Crohn’s disease MRI shows a defect in the internal sphincter at the 6:00 position of the mid anal canal (open white arrow) communicating with a 1.1 cm intersphincteric collection (black arrow). Wide defect in the external sphincter at the 7:00 position (solid white arrow) leads to a moderate sized perianal abscess in the ischioanal fossa.

Newer Management Concepts For Moderate to Severe IBD
• Treat early in disease
• Treat aggressively with “top down” biologics
• Check drug levels
• Dual therapy (immunomodulator + biologic)
• Aim for deep remission (histologic and endoscopic remission)

What are the data on efficacy and safety of biologic agents?

Currently Approved Biologics for IBD
Initial cA2 (Infliximab)
NEJM (1997)
Infliximab approved for
Crohn’s disease(1998)
Infliximab approved for
ulcerative colitis (2005)
Adalimumab approved for
Crohn’s disease (2007)
Certolizumab Pegol approved
for Crohn’s disease (2008)
Natalizumab approved for
Crohn’s disease (2008)
Adalimumab approved for
ulcerative colitis (2012)
Golimumab approved for
ulcerative colitis (2013)
Vedolizumab approved for
Crohn’s Disease (2014)
Vedolizumab approved for
ulcerative colitis (2014)
Ustekinumab approved for
Crohn’s Disease (2017)
Ustekinumab approved for ulcerative colitis 2019

Anti-TNF Therapies – Approved for IBD
• Infliximab (IFX): chimeric mouse/human anti-TNF-⍺ antibody • 75% human IgG1 isotype
• Adalimumab (ADL)/Golimumab (GOL): fully human monoclonal anti-TNF-⍺ antibodies• 100% human IgG1 isotype
• Certolizumab pegol (CIMZIA): antigen-binding fragment (Fab') of a humanized monoclonal antibody coupled to polyethylene glycol (No Fc portion)
• 95% human IgG1 isotype
CD and UC CD UC

Clinical Remission in UC
0%
40%
30%
20%
10%
Infliximab 10 mg/kg
Infliximab 5 mg/kg
Placebo
ACT: Infliximab 8 Weeks1
0%
40%
30%
20%
10%
Infliximab 10 mg/kg
Infliximab 5 mg/kg
Placebo
ACT: Infliximab 54 Weeks1
0%
40%
30%
20%
10%
Golimumab 100 mg
Golimumab 50 mg
Placebo
PURSUIT: Golimumab 54 Weeks4
0%
40%
30%
20%
10%
Golimumab 400/200 mg
Golimumab 200/100 mg
Placebo
PURSUIT: Golimumab 6 Weeks3
0%
40%
30%
20%
10%
Adalimumab Placebo
ULTRA 2 Adalimumab 8 Weeks2
0%
40%
30%
20%
10%
Adalimumab Placebo
ULTRA 2: Adalimumab 52 Weeks2
1Rutgeerts P, et al. N Engl J Med. 2005;353(23):2462-76; 2Sandborn WJ, et al. Gastroenterology. 2012;142(2):257-65; 3Sandborn WJ, et al. Gastroenterology. 2014;146(1):85-95; 4Sandborn WJ, et al. Gastroenterology. 2014;146(1):96-109.
*P<.05 vs. placebo; **P <.01 vs. placebo
*
****
** **
**
** **
**
Patients failing 5-ASA/Steroids/Immunomodulators

Cyclosporine vs. Infliximab for Severe UC
There were no significant differences between IFX and cyclosporine in adverse drug-related events, post-operative complications, or mortality.
Narula N, et al. Am J Gastroenterol. 2016;111(4):477-91.

Efficacy of Anti-TNF Therapies for Crohn’s Disease
*5 mg/kg dose.**Maintenance trial with 80/40 mg induction dosing. Randomized responders = CR-70 at week 4. Week 26 remission among randomized responders on 40 mg every other week dosing.
ACCENT I*(infliximab)2
Pa
tie
nts
(%
)PRECISE 2
(certolizumab)3P
ati
en
ts (
%)
CHARM**(adalimumab)1
24
60
40
0
20
40
60
80
Week 4 Response Week 26 Remission
Overall Remission Week 26
Pa
tie
nts
(%
)
1Colombel JF, et al. Gastroenterology. 2007;132(1):52-65; 2Hanauer SB, et al. Lancet. 2002;359(9317):1541-9;
3Schreiber S, et al. N Engl J Med. 2007;357(3):239-50.

Anti-TNF Agents: Adverse Events
• Immunogenicity
• Injection site reactions
• Infections
• Bacterial, viral, fungal and granulomatous (TB, histo, Listeria, etc)
• Lymphoproliferative disorders
• Autoimmunity
• Lupus-like symptoms
• Psoriasiform lesions
• Demyelinating disorders
• Worsen or de novo congestive heart failure
• Hepatotoxicity (rare)
• Malignancies
• T cell lymphoma (young men thiopurine combo therapy)
• Lymphoma (patients seronegative for EBV)
• Cutaneous
• Reactivation of:
• Latent TB
• HBV
• Herpes zoster
Di Sario A, et al. Curr Drug Saf. 2016;11(1):55-61; Murdaca G, et al. Expert Opin Drug Saf. 2015;14(4):571-82.

Adalimumab SC 160/80/40 mg Vedolizumab IV 300 mg
VARSITY Results: Overall Clinical Remission at Week 52 in UC
CI, confidence interval; IV, intravenous; SC, subcutaneous; TNF, tumour necrosis factor.aClinical remission: Complete Mayo score of ≤2 points and no individual subscore >1 point. bData from full analysis set, which includes all randomized patients who received at least 1 dose of study drug. cAnti-TNF subgroup analysis was prespecified and produced nominal p values.
Schreiber S et al. J Crohns Colitis. 2019;13(Suppl 1):S612–3. Abstr OP34. ECCO 2019 [oral presentation].
Overall clinical remissiona at week 52b
Pa
tie
nts
, %
OverallPrimary analysis
Anti-TNF naïvec
Subgroup analysisAnti-TNF exposure/failurec
Subgroup analysis
P=0.0061
∆ = 8.8% (2.6%, 15.0%)
P=0.0070
∆ = 9.9% (2.8%, 17.1%) ∆ = 4.2% (-7.7%, 16.1%)
P=0.4948

VARSITY: Mucosal Healing at Week 52 in UC
Adalimumab SC 160/80/40 mg Vedolizumab IV 300 mg
Mucosal healinga at week 52b
Pa
tie
nts
, %
OverallPrimary analysis
Anti-TNF naïvec
Subgroup analysisAnti-TNF exposure/failurec
Subgroup analysis
P=0.0005
∆ = 12.0% (5.3%, 18.6%)
P=0.0005
∆ = 13.6% (6.0%, 21.1%) ∆ = 5.6% (-7.6%, 18.8%)
P=0.4136
CI, confidence interval; IV, intravenous; SC, subcutaneous; TNF, tumour necrosis factor.a Mucosal healing defined as Mayo endoscopic subscore of ≤1 point. bData from full analysis set, which includes all randomized patients who received at least 1 dose of study drug. cAnti-TNF subgroup analysis was prespecified and produced nominal p values.
Schreiber S et al. J Crohns Colitis. 2019;13(Suppl 1):S612–3. Abstr OP34. ECCO 2019 [oral presentation].

Vedolizumab: Maintenance in Crohn’s
Feagan BG, et al. N Engl J Med. 2013;369(8):699-710.
P values vs. placebo
GEMINI IIWeek 52

Where do we position Vedolizumab?
• In patients unresponsive or intolerant to conventional therapies and anti‐TNF agents → however, can be used first-line
• In patients with unusual or other immune conditions such that additional systemic immune modification may be relatively contraindicated– Organ transplant patients– Hereditary or acquired immune deficiencies– Elderly patients– Cancer patients (skin cancers)
• Probably not patients with certain extraintestinal manifestations given gut selectivity

Ustekinumab for UC
NEJM 2020.

Ustekinumab: Maintenance for Crohn’s Disease
Primary and Major Secondary End Points in IM-UNITI
Feagan BG, et al. N Engl J Med. 2016;375(20):1946-60.
Pa
tie
nts
(%
)

Where should we position Ustekinumab?
• Possibly 1st line therapy in CD?
• After failures of anti-integrins or anti-TNFs?
• In patients with concomitant Psoriasis?

Safety Pyramid for IBD medications
VDZ
UST
Anti-TNF (monotherapy)
Thiopurines
Combination Therapy (Anti-TNF + Thiopurine)
Steroids
Safest

Advantages of Small Molecules in IBD
• Low-molecular weight
• Oral administration
• Resist gastric degradation
• Rapidly enter the systemic circulation
• Short half-life
• Lack immunogenicity
• Easier to manufacture than biologics, which may improve cost effectiveness
• Bind to specific intracellular targets.

Tofacitinib in UC: OCTAVE Phase 3 TrialClinical Response and Remission: Week 8
TNF Rxed
80
60
40
20
0Placebo Placebo10 mg
BIDTNF
Naive
Tofacitinib 10 mg BID
32.
8
59.
9
8.2
25.
212.
6
P<.01
P<.00
1
Clinical Remission
Clinical Response
OCTAVE 1
Placebo
80
60
40
20
0Placebo10 mg
BIDTNF
NaiveTNF Rxed
Tofacitinib 10 mg BID
29
55
4
22.
112
P<.001
P<.00
1
Clinical Remission
Clinical Response
OCTAVE 2
Sandborn WF, et al. NEJM. May 2017.

Tofacitinib Has A Rapid Effect As Early As 3 Days in UC Induction
aP<0.01 vs placebo; bP<0.001 vs placebo.Hanauer S et al. Clin Gastroenterol Hepatol. 2019;17:139-47.
Pa
tie
nts
, %
Reduction from baseline stool
frequency subscore of ≥1 point
Pa
tie
nts
, %
Reduction from baseline in both
Mayo stool frequency and Mayo
rectal bleeding subscore of ≥1 point
Day Day
a
bb
b b b b bb b
b b b
a
bb
b b b b bb b
b b b
Placebo Tofacitinib

Herpes Zoster (Shingles) in Tofacitinib-Treated UC Patients
Among 1157 (1612.8 PY) patients treated with tofacitinib
• 65 (5.6%) developed HZ on tofacitinib, IR - 4.07 (95% CI: 3.14–5.19)
– 51 (74%) involved 1 or 2 adjacent dermatomes
– 12 events in 11 patients were multidermatomal
– 6 events in 6 patients were disseminated
▪ 3 diffuse cutaneous rashes
▪ 2 ocular and skin lesions
▪ 1 HZ encephalitis
• 43% women
• Median age = 52 years (18-80)
• Median time to develop HZ = 324 days (13-1185)
• Dose-dependent (highest in 10 mg BID group)
BID, twice daily; CI, confidence interval; HZ, herpes zoster; IR, incidence rate; PY, patient-years.Winthrop KL et al. Inflamm Bowel Dis. 2018. 24(10):2258-2265.

Tofacitinib Boxed Warning
Available at: https://www.fda.gov/drugs/drug-safety-and-availability/fda-approves-boxed-warning-about-increased-risk-blood-clots-and-death-higher-dose-arthritis-and. Accessed December 11, 2020.
➢ Tofacitinib should be reserved for use following a TNF antagonist

Interim Data From Ongoing Rheumatology Trials: Tofacitinib
Available at: https://www.fda.gov/drugs/drug-safety-and-availability/fda-approves-boxed-warning-about-increased-risk-blood-clots-and-death-higher-dose-arthritis-and. Accessed December 11, 2020.
Tofacitinib 10 mg BID Anti-TNF
Pulmonary embolus19 cases in
3,884 patient-years3 cases in
3,982 patient-years
All-cause mortality45 cases in
3,884 patient-years25 cases in
3,982 patient-years

FDA Approves Ozanimod (Zeposia) for Ulcerative Colitis
(Zeposia) for Ulcerative ColitisUlcerative Colitis• Ozanimod (0.92 mg), an oral medication taken once daily, is
the first sphingosine-1-phosphate (S1P) receptor modulator approved for moderate to severe UC.
• Reduces lymphocyte migration into the intestine
• Reduces the # of lymphocytes in the peripheral blood
• For induction and maintenance of UC
• Clinical remission week 10 vs placebo 18% vs 6%, (p <0.0001)
• Clinical remission week 52 vs placebo 37% vs 19% (p <0.0001)
Abstract LB02, UEG Research Prize 2020 Session and Abstract LB10 from True North study

Non-response: Definitions
• Primary non-response: A patient does not respond to a loading dose of a biological agent when he/she receives it for the first time. Is this patient a non-responder to all drugs targeting the same pathway?
• Secondary non-response: A patient has responded to biological therapy at onset, but loses response or becomes intolerant to the molecule. This patient may respond to dose adjustment or is likely to benefit from other agents targeting the same pathway. If antibodies to initial drug, can switch within class.

Drug antibody negative
Sub-therapeuticInfliximab/Adalimumab
concentration
Reactive Testing Algorithm: Anti-TNF Therapy
Secondary loss of response (disease activity confirmed)
Change drug class or surgery
Dose escalate
Drug antibody positive
Therapeutic infliximab/adalimumab
concentration
High level of antibody
Consider dose escalation, addition of immunomodulator, or
change anti-TNF
Low level of antibody
Change to different anti-TNF
Modified from Khanna R, et al. Aliment Pharmacol Ther. 2013;38(5):447-59.

Positioning of Biologics in UC and CD
• The earlier the better…
• In the patients that need them…
• With (short-term?) combination therapy…
• And therapeutic drug monitoring

Eye
inflammation*
Liver andbile duct
inflammation
Skin lesions
Arthritis and joint pains
Kidney
stones
Growth failurein children
Lower
bone density*
Subfertility*
IBD: Systemic Complications
*Higher incidence in women.
Gallstones
Ovaries
Uterus




Musculoskeletal Disorders in IBD
•Sacroiliitis
•Peripheral arthritis
•Ankylosingspondylitis
Reprinted from the Clinical Slide Collection on the Rheumatic Diseases, copyright 1991, 1995, 1997. Used by permission of the American College of Rheumatology.
Reprinted with permission from Berens DL. Roentgen Features of Ankylosing Spondylitis. Clin Ortho.1971;74:20-33.


AGA Recommendationsfor Managing Osteoporosis
IBD patient:
Any of:
-Prolonged steroid use
(>3mo consec or recurrent
courses)
-Low trauma, fragility fracture
-Postmenopausal or male age
>50
-Hypogonadism
DXA
T score >-1
Basic Prevention:
-Ca/Vit D
-exercise
-smoking cessation
-avoid alcohol
-minimize
corticosteroids
-treat hypogonadismT score -2.5 to -1
Prevention and:
-repeat DXA 2 years
-Prolonged CS consider BP
and DXA 1 year
T score <-2.5
Vert Fracture
Regardless of DXA
Prevention and:
-Screen other causes low BMD
-Bisphosphonate therapy or
-Refer to bone specialist
Gastroenterology 2003;124:795-841

Relative Risk of Colon Cancer Based on Extent of UC (and Crohn’s colitis)
0
20
2
10
14
18
ProctitisAll Cases
6
Left-Sided Pan-colitis
8
12
16
4
Ekbom A, et al. N Engl J Med. 1990;323:1228-1233.

Risk Factors for Colon Cancer in IBD
• Strictures that cannot be passed
• Extensive colitis
• Long duration of disease
• Active disease
• Primary sclerosing cholangitis
• Family history of colon CA

Take Home Messages
• Treat early
• Treat aggressively for moderate to severe IBD
• Use dual therapy
• Use drug levels to guide therapy
• Treat to endoscopic and histologic remission
• The risk of a serious side effect is much less than the risk of a complication from the IBD itself

Question• A 22 y/o man recent diagnosed with Crohns’ disease presents
to your clinic to discuss treatment options. He is a non-smoker and does not drink alcohol. His only medication is Lialda. A recent endoscopy reveals superficial aphthae limited to the terminal ileum. He describes rare, intermittent abdominal pain and 2-3 BMs daily. Recent labs suggest a CRP of 2.8mg/dL (nl<3mg/dL), serum albumin: 4.8. He denies a history of perianal complications.
Which of the features of his disease puts him is considered high risk?A. Young ageB. Non-smoking statusC. Superficial ulcersD. Terminal ileal diseaseE. Serological markers

Question• A 22 y/o man recent diagnosed with Crohns’ disease presents
to your clinic to discuss treatment options. He is a non-smoker and does not drink alcohol. His only medications is Lialda. A recent endoscopy reveals superficial aphthae limited to the terminal ileum. He describes rare, intermittent abdominal pain and 2-3 BMs daily. Recent labs suggest a CRP of 2.8mg/dL (nl<3mg/dL), serum albumin: 4.8. He denies a history of perianal complications.
Which of the features of his disease puts him is considered high risk?A. Young ageB. Non-smoking statusC. Superficial ulcersD. Terminal ileal diseaseE. Serological markers
Age < 30 is a risk factor for increased disease severity

Question Which of the therapies for IBD has the highest risk for immunogenicity (drug antibody development)?
A. Vedolizumab
B. Ustekinumab
C. Infliximab
D. Adalimumab
E. Golimumab

Question Which of the therapies for IBD has the highest risk for immunogenicity (drug antibody development)?
A. Vedolizumab
B. Ustekinumab
C. Infliximab
D. Adalimumab
E. Golimumab
Infliximab is 25% mouse protein and thus has the highest immunogenicity

QuestionA 38 year old man with a medical history notable for Crohn’s disease, currently on infliximab at 5mg/kg every 8 weeks, presents in follow up with worsening abdominal pain, frequent bowel movements up to 15 daily, to discuss next options. Serum CRP is 56mg/dL. Infliximab trough level obtained prior to his last infusion was 12μg/mL (adequate therapeutic level is >5μg/mL); no antibody level detected.
After providing induction therapy, what would be the next best therapeutic option in managing his disease?
A. Start azathioprineB. Increase the infliximab dose to 10mg/kgC. Discontinue infliximab and start the biosimilar: inflectraD. Discontinue infliximab and start ustekinumabE. Decrease interval between infliximab infusions to every 4 weeks

QuestionA 38 year old man with a medical history notable for Crohn’s Disease, currently on Infliximab at 5mg/kg every 8 weeks, presents in follow up with worsening abdominal pain, frequent bowel movements up to 15 daily, to discuss next options. Serum CRP is 56mg/dL. Infliximab trough level obtained prior to his last infusion was 12μg/mL (adequate therapeutic level is >5μg/mL); no antibody level detected.
After providing induction therapy, what would be the next best therapeutic option in managing his disease?
A. Start azathioprineB. Increase the infliximab dose to 10mg/kgC. Discontinue infliximab and start the biosimilar: inflectraD. Discontinue infliximab and start ustekinumabE. Decrease interval between infliximab infusions to every 4 weeks
IFX does not work here even when the level is therapeutic so it is
necessary to switch drug class

References• Alexandersson B, Hamad Y, Andreasson A, Rubio CA, Ando Y, Tanaka K, Ichiya T, Rezaie R, Schmidt PT. High-definition
Chromoendoscopy Superior to High-definition White-light Endoscopy in Surveillance of Inflammatory Bowel Diseases in a Randomized Trial. Clin Gastroenterol Hepatol. 2020 Apr 27:S1542-3565(20)30594-2. doi: 10.1016/j.cgh.2020.04.049.
• Bernstein CM, Burchill C, Targownik L et al. Events within the first year of life, but not the neonatal period, affect risk for later development of inflammatory bowel diseases. Gastroenterology 2019; 156(8):2190-2197.
• Brenner E, Ungaro RC, Gearry et al. Corticosteroids, but not TNF antagonists, are assocaited with adverse COVID-19 outcomes in patients with inflammatory bowel diseases: results from an international registy. Gastroenterology. 2020;doi.org/10.1053/j.gastro.2020.05.032
• Bellaguarda E, Hanauer ST. Checkpoint-inhibitor-induced colitis. Am J Gastroenterol. 2020; 115:202-210.
• Levine A, Wine E, Assa A et al. Crohn’s Disease Exclusion Diet Plus Partial Enteral Nutrition Induces Sustained Remission in a Randomized Controlled Trial. Gastroenterology 2019;157(2):440-450.
• Mahadevan U, Robinson C, Bernasko N, et al. Inflammatory Bowel Disease in Pregnancy Clinical Care Pathway: A Report From the American Gastroenterological Association IBD Parenthood Project Working Group. Am J Obstet Gynecol. 2019;220(4):308-323.
• Ng SC, Kaplan GG, Tang W et al. Population Density and Risk of Inflammatory Bowel Disease: A Prospective Population-Based Study in 13 Countries or Regions in Asia-Pacific. Am J Gastroenterol. 2019;114(1) :107-115.
• Sands BE, Peyrin-Biroulet L, Loftus EV Jr, Danese S, Colombel JF, Törüner M, Jonaitis L, Abhyankar B, Chen J, Rogers R, Lirio RA, Bornstein JD, Schreiber S; VARSITY Study Group. Vedolizumab Versus Adalimumab for Moderate-to-Severe Ulcerative Colitis. N Engl J Med. 2019 Sep 26;381(13):1215-1226.
• Sands BE, Sandborn WJ, Panaccione R, O'Brien CD, Zhang H, Johanns J, Adedokun OJ, Li K, Peyrin-Biroulet L, Van Assche G, Danese S, Targan S, Abreu MT, Hisamatsu T, Szapary P, Marano C; UNIFI Study Group. Ustekinumab as Induction and Maintenance Therapy for Ulcerative Colitis. N Engl J Med. 2019 Sep 26;381(13):1201-1214.
• Singh S, Allegretti JR, Siddique SM. AGA technical eview on the management of moderate to severe ulcerative colitis. Gastroenterology. 2020;158(5):1465-1496.
•
Recommended