J Clin Pathol 1985;38:1278-1280
Solitary "necrotic nodule" of the liver: a probablepathogenesisCL BERRY
From the Department ofMorbid Anatomy, The London Hospital Medical College, London
SUMMARY Examination of two lesions in the anterior margin of the liver suggested that the originof the so called "solitary necrotic" nodule lies in non-malignant tissue. An origin in sclerosinghaemagioma seems probable.
In 1983 Shepherd and Lee described five cases of anunusual lesion in the liver; four were described indetail and the other added as a note.' The lesionswere described as having a "completely necroticcore" and a hyalinised fibrotic capsule containingelastic fibres. The central areas of the cores con-tained reticulin in two cases, and an illustration ofthis suggested to me that the lesions might haveoriginated in sclerosing haemangiomas.The authors pointed out the importance of liver
nodules to surgeons making exploratory investiga-tions and emphasised the importance of an aware-ness of potentially confusing benign lesions thatmight be mistaken for metastases. Their differentialdiagnoses included several infectious processes,including visceral larva migrans, but sclerosinghaemangioma was mentioned only in passing.The two lesions described in this paper were dis-
Accepted for publication 9 July 1985
covered in a study of 1000 consecutive necropsies,in which the liver was cut in 1*5 cm slices along thesaggital axis in an attempt to determine the inci-dence of benign lesions (CL Berry, data in prepara-tion).
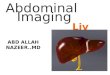
CASE REPORTSCase 1 An 85 year old man was admitted to hospitalwith a diagnosis of cardiac failure. He died shortlyafter admission. He had had diabetes mellitus for 10years, which had been controlled without insulin,and he had had a prostatectomy 20 years before.There was no other relevant history. At necropsysacral and ankle oedema were found. He had died asa result of left ventricular failure due to calcific aor-tic stenosis with ischaemic heart disease. His livershowed a pattern of chronic venous congestion.Three cysts (all about 1 5 cm in diameter) were seenin the right lobe. Towards the anterior margin of thelobe a firm white lesion was seen (Fig. 1).
Fig. 1 Liver lesion in case 1.
1278
copyright. on S
eptember 13, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.38.11.1278 on 1 Novem
ber 1985. Dow
nloaded from

Solitary "necrotic nodule" of the liver: a probable pathogenesis
AC,~~~~~~~~~~~~~~',
VA.
k{~ie .1-kr g a
,, _
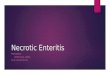
Fig. 2 Acellular area from case 1 (Elastic van Gieson.) x150.
NA
0A~~~Ar/P~~~~~~~~~~~~~~J
tA\~~~~i
4Z~~~fp6
dl-l.1 ~...F-
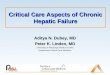
Fig. 3 Montage ofcomplete lesions in case 2, showing "feeder" vessels at lower part offrame, which fihl a clearlyhaemangiomatous part ofthe lesion. Higher up the frame fewer vascular spaces and more sclerotic tissue, some ofwhich is calcifying, can be seen. Predominant sclerosis in upper margin and other levels is evident. (Haematoxylinand eosin.) x 12*5.
1 279
copyright. on S
eptember 13, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.38.11.1278 on 1 Novem
ber 1985. Dow
nloaded from

1280
Case 2 A 76 year old man was admitted to hospitalsuffering from senile dementia. He developed bron-chopneumonia after four weeks and died. Dementiahad developed after a prostatectomy three yearsbefore admission. At necropsy a left nephrectomyscar was evident and the kidney was missing. Thishad been removed after a crushing injury in the sec-ond world war, during which he had worked as a fueltank cleaner. There was severe bronchiectasis andbronchopnuemonia affecting both lower lobes, andthe right ventricle was hypertrophied.When the liver was cut a solitary lesion 1 cm in
diameter was found in the right lobe, close to theanterior margin. The lesion was firm, and was whiteat its margins with a shading toward pink at onepole. It was clearly demarcated from surroundingliver cells.
Material and methods
The specimens were fixed in nominally bufferedformalin, processed to paraffin, and sectioned at5 ,um. Thy were stained with haematoxylin andeosin and elastic van Gieson in step sections.
Results
MICROSCOPYCase I The lesion was composed of acellular hyalineeosinophilic material that was essentially feature-less. When several levels were examined occasionalsmall vessels were seen in this apparentlyhomogeneous material. Elastic stains showed someareas with a pattern resembling that of Fig. 1 ' in thepaper of Shepherd and Lee but most contained littleelastic (Fig. 2). The pattern of collagen, however,appeared to outline vascular spaces when assessed atthe margins and at several levels.Case 2 "Feeder' vessels, filling a clearly haeman-giomatous part of the lesion, were seen. The lesion
Berry
contained four vascular spaces and more sclerotictissue, some of which was calcifying. Sclerosis wasalso a predominant feature.
Discussion
Schultz and Hort,2 in a study of 11 581 hepaticmetastases, showed that 40% of lesions reached thehepatic surface and that in only 12% of cases werelesions confined to the deep aspects of the liver. Aliver mantle 1 cm thick amounts to around 46% ofthe liver mass, and although only 40% of this isvisible in the patient during life,3 the value tosurgeons of inspecting the liver surface in the man-agement of malignant disease is clear from thesedata.
Solitary lesions in the liver should not be assumedto be metastases if biopsy has not been performed.Shepherd and Lee concluded that they hadidentified a new source of potential confusion if suchbiopsies were not done and that the lesion had adistinct, if uncertain, pathogenesis.'The lesions have features that resemble a "scler-
osed" haemangioma, and it seems that the lesion incase 2 illustrates the way in which the lesion mayevolve.
References
Shepherd NA, Lee G. Solitary necrotic nodules of the liversimulating hepatic metastases. J Clin Pathol 1983;36: 1181-3.
2 Schultz W, Hort W. The distribution of metastases in the liver: aquantitative post mortem study. Virchows Arch A1981;394:89-96.
3McBride C. Das Lebermalignom. Temp Med 1979;2:25-30.
Requests for reprints to: Professor CL Berry, Departmentof Morbid Anatomy, The London Hospital Medical Col-lege, The London Hospital, London El 1BB, England.
copyright. on S
eptember 13, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.38.11.1278 on 1 Novem
ber 1985. Dow
nloaded from
Recommended