Small Buttons, Large Consequences:
Programming Considerations for Smart
Pump Interoperability Implementation
Megan Holsopple, PharmD, BCPS
Medication Utilization Coordinator
Center for Medication Utilization
Froedtert & the Medical College of Wisconsin

Presentation Overview
• Review key considerations for smart pump
programming prior to interoperability
implementation
• Discuss considerations for data set
upgrades post-interoperability
2

Froedtert Health
Froedtert Hospital
585 inpatient beds
Infusion Clinic Services
Community Memorial Hospital
198 inpatient beds
Infusion Clinic Services
St. Joseph Hospital
70 inpatient beds
Infusion Clinic Services
Drexel Town Square
Primary Care
Urgent Care
Infusion Clinic Services
Moorland Reserve Health Center
Primary Care
Urgent Care / Emergency Department
Infusion Clinic Services
Town Hall Health Center
Primary Care
3

Froedtert’s Interoperability Journey

Project Timeline F
eb
rua
ry 2
01
6
Pro
ject K
ick-O
ff | T
ea
m M
ee
t n
’ Gre
ets
March 2016 – June 2016
Infusion Standardization
Smart pump profile condensing
Nursing Workflow Meetings
Connectivity Testing/Virtual Server Expansion
August 2016
Full Medication Testing
August – November 2016
Residual Medication Testing
Super-user training
Nursing education
November 2016
Implementation
De
ce
mb
er
20
16
– C
urr
en
t
Sm
art
Pu
mp
Ma
inte
na
nce
Re
po
rt E
va
lua
tio
n
April 2016
Targeted Medication
Testing
(20-30 medications)
Project Milestones
5

Baseline Requirements
• Barcode Medication Administration
• Smart Pumps
– Guardrails Editor® software upgrade
– Updated smart pump devices
• Servers and wireless connectivity
6

The Basics!
• Standardized infusion concentrations and
dosing units1,2
– No more than 2 concentrations if possible
– A single dosing unit for each medication
1. ASHP Standardize for Safety. https://www.ashp.org/-/media/assets/pharmacy-practice/s4s/docs/s4s-iv-adult-continuous-infusion-guiding-
principles.ashx?la=en. Accessed April 2, 2018.
2. ISMP’s Medication Safety Alert! Smart Pump Custom Concentrations Without Hard “Low Concentration” Alerts.
http://www.ismp.org/newsletters/acutecare/showarticle.asp?id=16 Accessed April 2, 2018. 7

Reviewed and aligned 270
continuous and intermittent
infusion concentrations!
Interoperability Groundwork
8

Pump and eHR Evaluation
Identifying eRX differences
at each hospital
Identifying any existing defaults:
1. Concentration
2. Base solution
3. Base Volume
4. Dosing Recommendations
5. Administration Practices
6. Compounding Practices
1
2 3
4
5
9
6

How Many Profiles Are in Your
Smart Pump? A. 3 – 5
B. 6 – 8
C. 9 – 12
D. More than 12
10

Out-of-Scope Areas
Pre-Interoperability
• 14 Total Profiles
Interoperability
• 7 Total Profiles
11

Smart Pump Profile Condensing
Pre-Interoperability
• 14 Total Profiles
Interoperability
• 7 Total Profiles
12

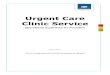
Interoperability Data Set Space
Available Programming
Space 14%
Programmed Space 86%
Figure 1. Pre-Interop Data Set (n=14 profiles)
Available Programming
Space 56%
Programmed Space 44%
Figure 2. Interoperability Data Set (n=7 profiles)
13

Profiles and Configurations
Interoperability
• 7 Total Profiles
14

Pump and eHR Interface
• Three requirements:
– Main ingredient dose, volume, and rate
– Identifier (ie, alias)
– Ability for medication to auto-insert a flowsheet
15

Pump and eHR Interface
• Three requirements:
– Main ingredient dose, volume, and rate
– Identifier (ie, alias)
– Ability for medication to auto-insert a flowsheet
16

Standardizing Alias Nomenclature
• Used first 3-5 letters of
medication name
• Identified standardized
concentration or dose
vs. a “wild-card” entry
• Denoted continuous “C” vs.
piggyback “PB” at the end
and used “BB” for bolus
from bag entries 17

Pump and eHR Interface
• Three requirements:
– Main ingredient dose, volume, and rate
– Identifier (ie, alias)
– Ability for medication to auto-insert a flowsheet
eHR
generating
values flowsheets
18

Project Timeline F
eb
rua
ry 2
01
6
Pro
ject K
ick-O
ff | T
ea
m M
ee
t n
’ Gre
ets
March 2016 – June 2016
Infusion Standardization
Smart pump profile condensing
Nursing Workflow Meetings
Connectivity Testing/Virtual Server Expansion
August 2016
Full Medication Testing
August – November 2016
Residual Medication Testing
Super-user training
Nursing education
November 2016
Implementation
De
ce
mb
er
20
16
– C
urr
en
t
Sm
art
Pu
mp
Ma
inte
na
nce
Re
po
rt E
va
lua
tio
n
April 2016
Targeted Medication
Testing
(20-30 medications)
Project Milestones
19

Sample Testing Example
20

Troubleshooting
21

Clinical Advisory Use
• Combination medication infusions
– Example: VD-PACE (cisplatin, etoposide,
cyclophosphamide)
22

Blacklisted Medications
• Will not prompt the nurse to scan the
pump when selected for administration
• Blacklisted medications:
– Investigational medications
– Patient-controlled analgesia
– Technology limitations
• Penicillin dosing and concentration in million units
in the eHR and units in smart pump
• Blood factor products
• Immune globulin titratable infusions
23

Project Timeline F
eb
rua
ry 2
01
6
Pro
ject K
ick-O
ff | T
ea
m M
ee
t n
’ Gre
ets
March 2016 – June 2016
Infusion Standardization
Smart pump profile condensing
Nursing Workflow Meetings
Connectivity Testing/Virtual Server Expansion
August 2016
Full Medication Testing
August – November 2016
Residual Medication Testing
Super-user training
Nursing education
November 2016
Implementation
De
ce
mb
er
20
16
– C
urr
en
t
Sm
art
Pu
mp
Ma
inte
na
nce
Re
po
rt E
va
lua
tio
n
April 2016
Targeted Medication
Testing
(20-30 medications)
Project Milestones
24

Data Evaluation
• Available data
– eHR
– Smart pump
– Staff feedback
• Data presentation
– Raw
– Verbal
25

Pump Near Miss Report
26

Compliance
• Ability to drill down
– Area
– Clinician
– Medication
– Number of attempts
27

Near Miss Report Details
28

Compliance
• Goal of 90% compliance using smart pumps
• Update drug libraries based on reports
29

How often do you implement
smart pump changes?
A. Monthly
B. Quarterly
C. Semi-Annually
D. Annually
E. No established frequency
30

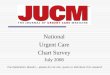
Data Set Transfer Frequency
Monthly Upgrade Advantages
• Accountability process with
compliance report
evaluation
• Addressing pump and eHR
mismatches
• Ability to address shortage
issues and new formulary
medications
Monthly Upgrade Disadvantages
• Multiple circulating datasets
being used in patient care
• Maintenance of smart pump
data set
Monthly following interoperability through August 2017 the
changed to bimonthly
31

0.32%
0.81%
98.87%
0.34%
100.00% 99.66%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Feb. 2018 Update Dec. 2017 Update Oct. 2017 Uptake
Perc
en
t o
f P
um
ps
Bimonthly Update
Dec-17
Oct-17
Aug-17
Jul-17
Mar-17
32

290
348 383 398 406 422
448 461
223
320 337 351 357 366 376 393
548
665
744 771
790 827
850 869
0
100
200
300
400
500
600
700
800
900
1000
Day 0(data setpush day)
Day 1 Day 2 Day 3 Day 4 Day 5 Day 6 Day 7
To
tal
Nu
mb
er
of
Ala
ris
Pu
mp
s (
n=
10
92)
Oct-17Dec-17Feb-18
33

Internal Resources
34

Conclusions
• Infusion alignment and standardization of
concentrations will help streamline
interoperability work
• Standardized nomenclature for alias
assignment will help make interpretation of
interface failures easier
• Test, test, and test some more!
35

Future Vision…
• Optimization of smart pump
reporting tools
• Out-of-scope areas that
implement BCMA will adopt
interoperability technology
• The same smart pump
technology will be utilized across
the Froedtert enterprise
36

Acknowledgements
Project Management Office
• Lisa Vance Coss
• Nanda Kothinti
Pharmacy and Nursing Informatics
• Brian Dekarske
• Kaleb Fitch
• Lisa Knoebel
• Matt Selsing
• Jody Thompson-King
• Carlos Ortiz
• Tina Wagner
• Amy Wolf
Nursing
• Rose Gaskell
• All super-users!
FMLH Dept. of Pharmacy
• Kristin Hanson
• Shannon Werner
Biomed
• Jovo Acamovic
• Jon Mackay
Vendor Support
• BD
• EPIC
37

Small Buttons, Large Consequences:
Programming Considerations for Smart
Pump Interoperability Implementation
Megan Holsopple, PharmD, BCPS
Medication Utilization Coordinator
Center for Medication Utilization
Recommended