SITUATION ANALYSIS: EYE CARE IN INDONESIAEYE CARE IN INDONESIAAllya Alwi, MD
Ministry Of Health Of Indonesia
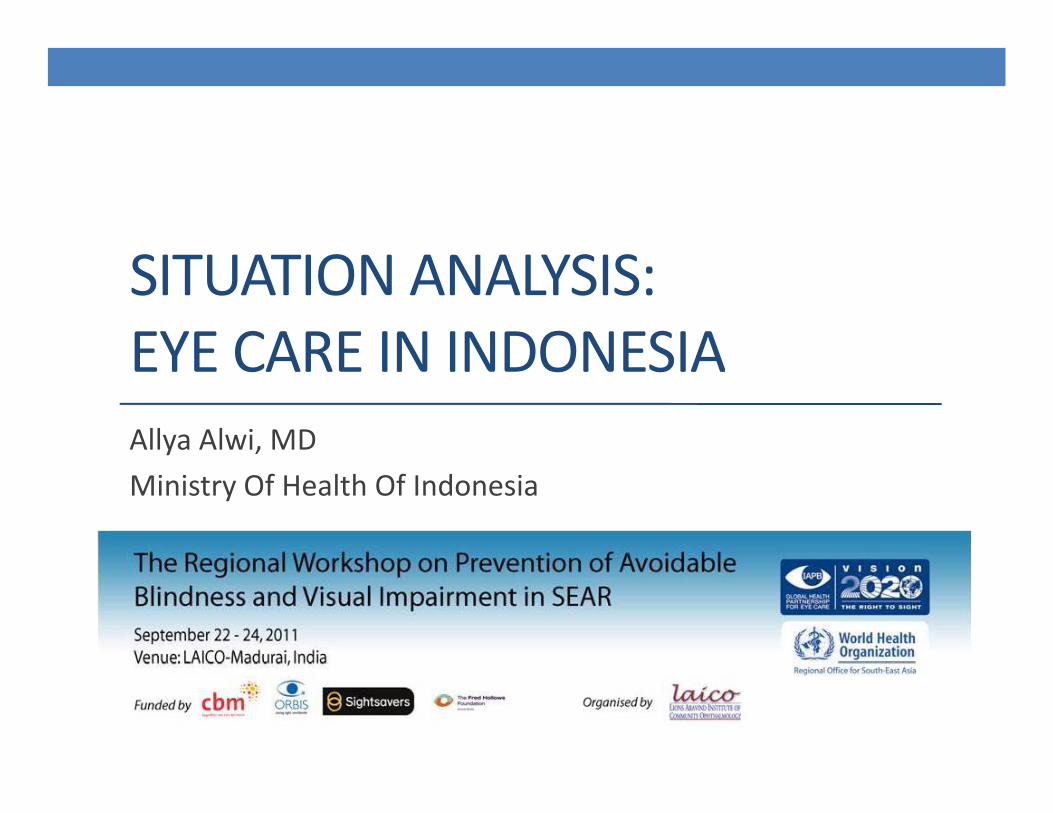
Prevalence of Blindness in IndonesiaPrevalence of Blindness in Indonesia• Basic Health Research, MoH 2007
• Blindness 0.9 % (based on Visual Acuity < 3/60)• Low Vision 4.8 % • Disease specific prevalence
• Cataract : 1 8 %• Cataract : 1.8 %• Glaucoma : 0.5 %• Color Blindness : 0.7 %• Refractive Disorder
S h l A Child 32 % (81 9 % d i h l )• School Age Children : 32 % (81.9 % not corrected with glasses)• Young Adults : 45.1 % (80.2 % net corrected with glasses)
• Cause of Childhood Blindness at School for The Blind in Java (2007)• Hereditary disease : 31.9 %Hereditary disease : 31.9 %• Intrauterine : 1.5 %• Perinatal / neonatal : 5.4 %• Postnatal / infancy / childhood : 28.5 %• Unknown : 32.7 %
59.9 % Avoidable (33.3 % preventable; 26.6 % treateble)
Prevalence of Blindness in IndonesiaPrevalence of Blindness in Indonesia
• Eye and Ear National Health Survey 1993‐1996 ( MoH)y y ( )• Prevalence of Blindness (VA ≤ 3/60) 1,5 %
• Cataract (0,78 %), Glaucoma (0,20%), Refractive Disorders (0,14%)
OBJECTIVE1 STRENGTHENADVOCACY TO INCREASEOBJECTIVE 1. STRENGTHEN ADVOCACY TO INCREASE MEMBER STATES POLITICAL, FINANCIAL AND TECHNICAL COMMITMENT INORDER TOELIMINATEAVOIDABLECOMMITMENT IN ORDER TO ELIMINATE AVOIDABLE BLINDNESS AND VISUAL IMPAIRMENT
Current PracticesCurrent Practices • Directorate of Basic Health Efforts is the designated coordinator of the Eye Health programs in the Ministry of Health
• The National Committee of Visual Impairment and Blindness Prevention has been formed since 2005 by Ministerial Decree, and now it is in the process of being renew and upgraded to Presidential Decree • The Member of this Committee consist of MoH, Cross Sectors Stakeholder, NGO’s, and Professions
E C h b i d l l f H l h S i ( i• Eye Care has been integrated on every level of Health Services (primary, secondary, tertiary). The care given depends on the availability of human resources, equipments and infrastructures
WSD i b i t i 2005 i th f f f• WSD is being commemorate every year since 2005, in the form of free cataract operations, community seminars and counselling
OBJECTIVE2 DEVELOPAND STRENGTHENNATIONALOBJECTIVE 2. DEVELOP AND STRENGTHEN NATIONAL POLICIES, PLANS AND PROGRAMMES FOR EYE HEALTH ANDPREVENTIONOFBLINDNESS ANDVISUALAND PREVENTION OF BLINDNESS AND VISUAL IMPAIRMENT
Current PracticesCurrent Practices • Development of National Policies , Plans and Programs:
• Constitution of Health (36; 2009)• Management of visual impairment as one of the implementation of Health Care• Management of visual impairment is a join responsibility between Government, Local Government and
Community• National Strategy Plans for Visual Impairment and Blindness Prevention to Achieve Vision 2020 (2005)
• Healthy Eye 2020• Strategy :
• The forming of the national, Provincial & Districts Committee to coordinate resources and activities• Increasing cross sectors advocacies and communications • Development of partnership• Increasing program management and service infrastructure• Increasing quality and quantity of Human Resources• Mobilization of support from private sectors community and NGO’s• Mobilization of support from private sectors, community and NGO’s
• National Coordination Annual Meeting on The Development of Sensory Health Programs(which include the prevention of avoidable blindness and visual impairment programs)
• Cross Programs, Cross Sectors and NGO’s annual meetingE H lth P i t t d ith th H lth P (S h l H lth P• Eye Health Programs are integrated with other Health Programs (School Health Programs – Early Detection and periodic monitoring; Work Force Health Programs ‐ Work Force Protection; Nutrition programs – Vitamin A Supply)
• Eye Care for the poor is given with Government Insurance (Jamkesmas)• Cataract operationsCataract operations• Glasses prescriptions• Other Curative Eye Services
OBJECTIVE 3. INCREASE AND EXPAND RESEARCH FOR THEPREVENTIONOFBLINDNESS ANDVISUALTHE PREVENTION OF BLINDNESS AND VISUAL IMPAIRMENT
Current PracticesCurrent Practices
• Researches are very limitedy
• Sporadically done by Eye Department of University in Indonesia
• Nationally, The Basic Health Research conducted by MoHaccommodate Eye Health Data
OBJECTIVE4 IMPROVECOORDINATIONBETWEENOBJECTIVE 4. IMPROVE COORDINATION BETWEEN PARTNERSHIPS AND STAKEHOLDERS AT NATIONAL AND INTERNATIONAL LEVELS FORTHEPREVENTIONOFINTERNATIONAL LEVELS FOR THE PREVENTION OF BLINDNESS AND VISUAL IMPAIRMENT
Current PracticesCurrent Practices• Partnership with NGO’s :
• WHO :• Facilitating situation analysis and the making of National Action Plans on Visual Impairment and Blindness Prevention
• CBM• Support Cataract programs
• HKI• Vitamin A distribution
• Gapopin• Gapopin• Administration of Glasses
• Mata Hati• Support Cataract Operations
• Bank Mata• Cornea Donor
• Partnership with other stakeholders : Profession (PERDAMI / IOA) :• Profession (PERDAMI / IOA) :• Giving input to government in establishing national policies• Facilitate and resource person in training and meetings
OBJECTIVE 5. MONITOR PROGRESS IN ELIMINATION OF AVOIDABLE BLINDNESS ATNATIONAL REGIONALANDAVOIDABLE BLINDNESS AT NATIONAL, REGIONAL AND GLOBAL LEVELS
Current PracticesCurrent Practices
• Monitoring and Evaluation of Eye Health Programs is done by :g y g y• Routine Report System (Provincial Health Office)
• Supervision (MoH, Province and District Health Office)
B i H lth R h• Basic Health Research
• Periodic Reports to WHO
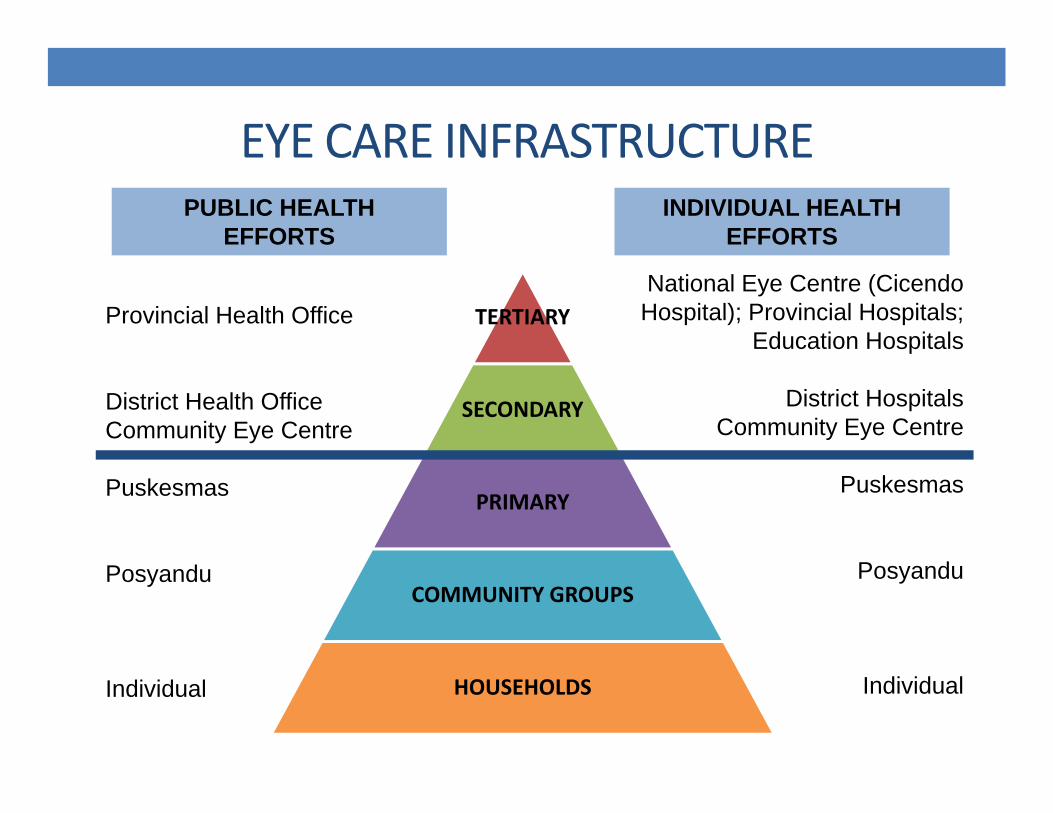
EYE CARE INFRASTRUCTUREEYE CARE INFRASTRUCTUREPUBLIC HEALTH
EFFORTSINDIVIDUAL HEALTH
EFFORTS
TERTIARYProvincial Health OfficeNational Eye Centre (CicendoHospital); Provincial Hospitals;
Education Hospitals
SECONDARYDistrict Health OfficeCommunity Eye Centre
District HospitalsCommunity Eye Centre
PRIMARYPuskesmas Puskesmas
COMMUNITY GROUPSPosyandu Posyandu
HOUSEHOLDSIndividual Individual

DISTRIBUTION OF OPHTHALMOLOGISTS IN INDONESIA
1 3% 1 9%17,3%9,6%
1,9%
0,3%
0,1%
68,5%1,8% 0,5%
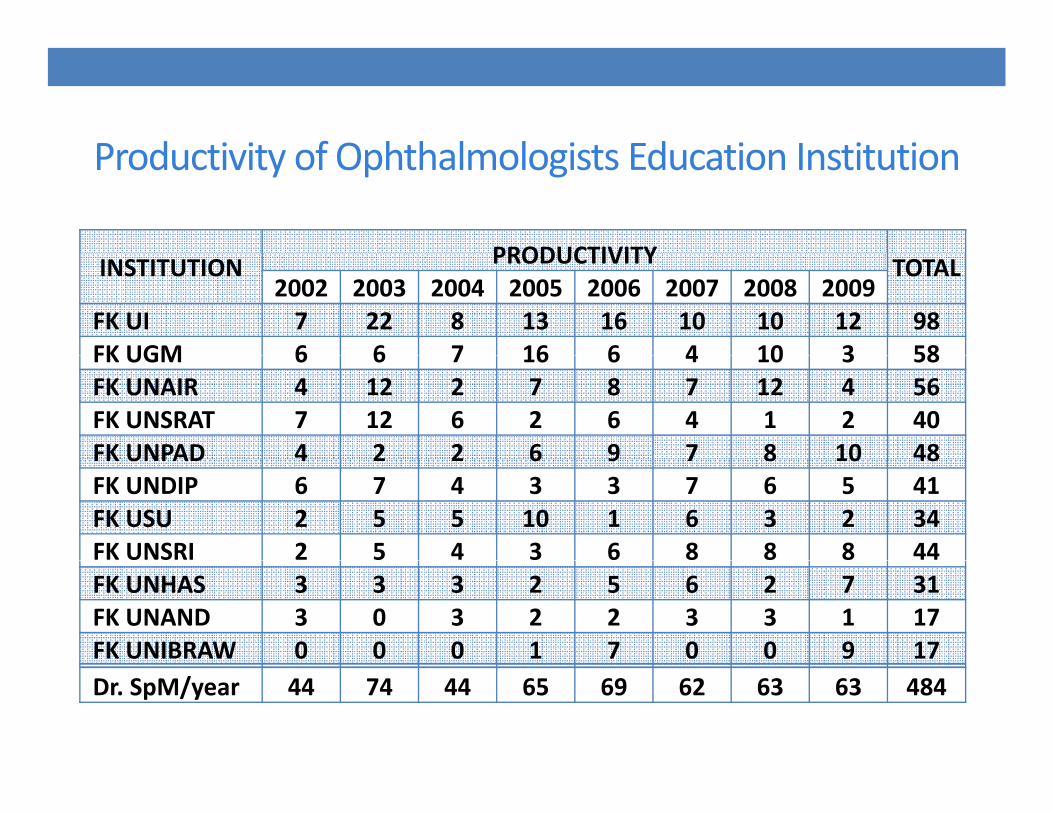
Productivity of Ophthalmologists Education InstitutionProductivity of Ophthalmologists Education Institution
PRODUCTIVITYINSTITUTION PRODUCTIVITY TOTAL 2002 2003 2004 2005 2006 2007 2008 2009
FK UI 7 22 8 13 16 10 10 12 98FK UGM 6 6 7 16 6 4 10 3 58FK UGM 6 6 7 16 6 4 10 3 58FK UNAIR 4 12 2 7 8 7 12 4 56FK UNSRAT 7 12 6 2 6 4 1 2 40FK UNPAD 4 2 2 6 9 7 8 10 48FK UNPAD 4 2 2 6 9 7 8 10 48FK UNDIP 6 7 4 3 3 7 6 5 41FK USU 2 5 5 10 1 6 3 2 34FK UNSRI 2 5 4 3 6 8 8 8 44FK UNHAS 3 3 3 2 5 6 2 7 31FK UNAND 3 0 3 2 2 3 3 1 17FK UNIBRAW 0 0 0 1 7 0 0 9 17Dr. SpM/year 44 74 44 65 69 62 63 63 484
TRAININGSTRAININGS
• Trainings are limitedg
• MoH is training 2 person / province / year in programs management and case management
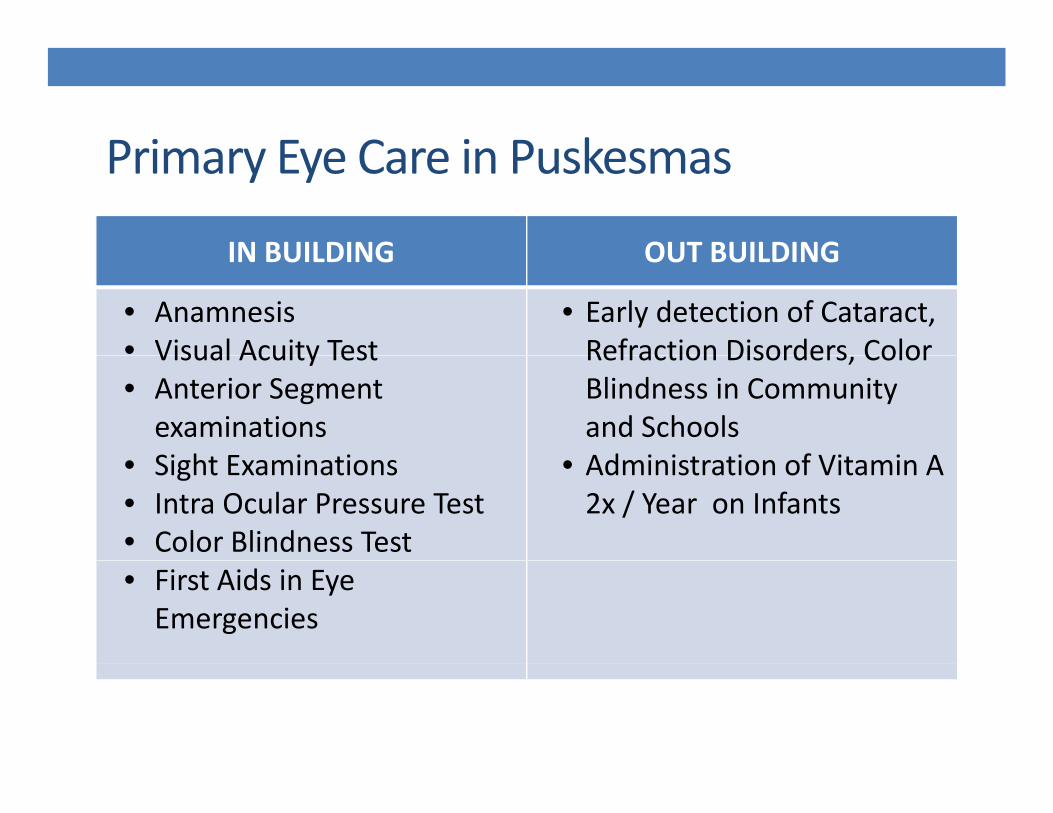
Primary Eye Care in PuskesmasPrimary Eye Care in Puskesmas
IN BUILDING OUT BUILDINGIN BUILDING OUT BUILDING
• Anamnesis• Visual Acuity Test
• Early detection of Cataract, Refraction Disorders ColorVisual Acuity Test
• Anterior Segment examinationsSi ht E i ti
Refraction Disorders, Color Blindness in Community and SchoolsAd i i t ti f Vit i A• Sight Examinations
• Intra Ocular Pressure Test• Color Blindness Test
• Administration of Vitamin A 2x / Year on Infants
• First Aids in Eye Emergencies
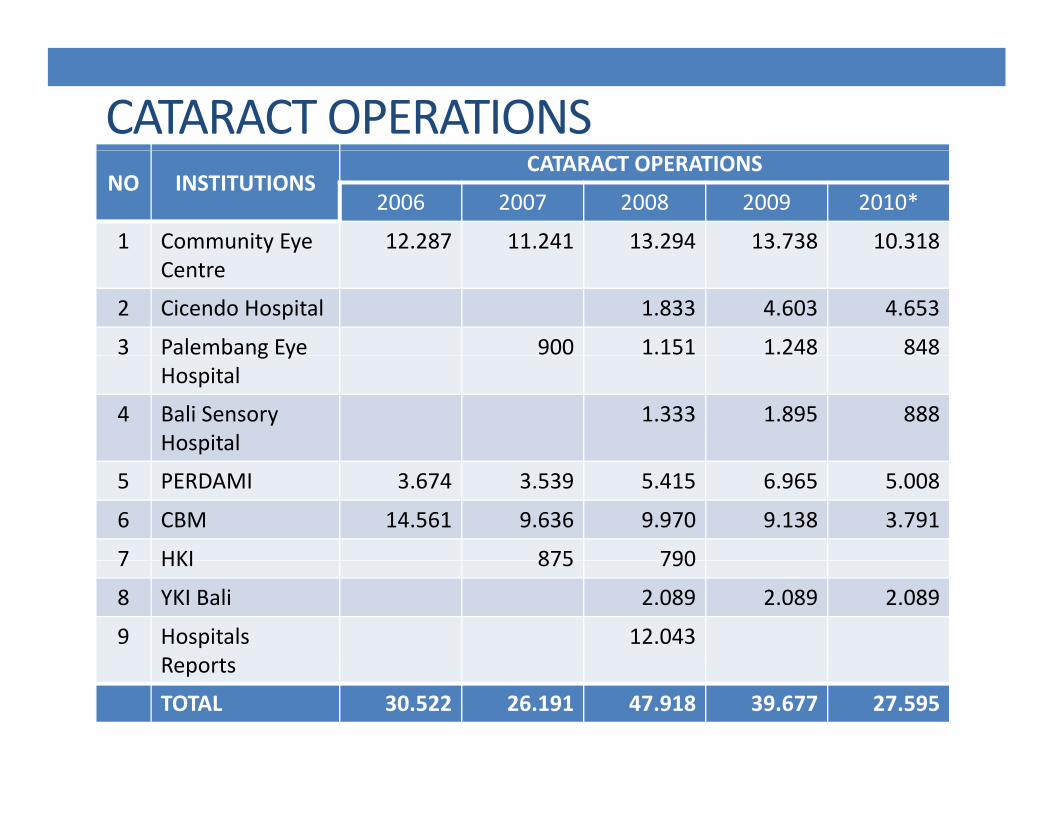
CATARACT OPERATIONSNO INSTITUTIONS
CATARACT OPERATIONS
2006 2007 2008 2009 2010*
1 Community Eye 12.287 11.241 13.294 13.738 10.318Centre
2 Cicendo Hospital 1.833 4.603 4.653
3 Palembang Eye 900 1.151 1.248 848g yHospital
4 Bali Sensory Hospital
1.333 1.895 888
5 PERDAMI 3.674 3.539 5.415 6.965 5.008
6 CBM 14.561 9.636 9.970 9.138 3.791
7 HKI 875 7907 HKI 875 790
8 YKI Bali 2.089 2.089 2.089
9 Hospitals Reports
12.043Reports
TOTAL 30.522 26.191 47.918 39.677 27.595
CHALLENGES IN DEVELOPING EYE HEALTH PROGRAMS
d h d b• Limited Human Resources with uneven distribution
• Lack of medical equipment and infrastructure
• Expensive cost of operations• Expensive cost of operations
• Poor data reporting and recording
• Lack of research ac o esea c
• Low socio – economic status of community
• Not enough funding (not a priority program)
• Geographic Conditions of Indonesia
SUMMARYSUMMARY
The prevalence of blindness in Indonesia is still high• The prevalence of blindness in Indonesia is still high
• The Human Resources and Infrastructures for Eye Care are limited with uneven distribution
• With limited funding, partnerships with NGO’s are still needed
• The National Committee need to be strengthen
THANK YOU
Recommended