Single tube 10-color bulk lysis assay for sensitive detection of residual plasma cell neoplasms: MSKCC experienceMikhail Roshal MD, PhDDirector of Technical Flow Cytometry Development,Department of Laboratory MedicineMemorial Sloan-Kettering Cancer CenterNew York, NY

MSKCC Cell Marker Laboratory
• Malignant Cell Immunophenotyping– 30 neoplastic samples/day– Leukemia, Lymphoma, Plasma cell neoplasms– Nearly all samples are for follow-up – MRD detection if B-ALL, AML, PCN, lymphoma– Ongoing clinical trial support

Early diagnosis, optimal treatment: Better overall survival in myeloma
Sigurður Yngvi Kristinsson, MD, PhDProfessor of HematologyUniversity of Iceland and Karolinska University Hospital
Email: [email protected]: @sykristinsson

@sykristinsson

“What is the purpose of your trip, sir?“

Myeloma survival improvingEarly detectionTreatment of early diseaseBetter responsesScreening?
“Makes sense“

Melphalan
1960 1970 1980 1990 2000
Melphalan-prednisone
Autologous SCT
VADInterferons Thalidomide
Multiagent chemotherapy regimens
Tandem ASCT
Management of multiple myeloma
BortezomibLenalidomide
2010
CarfilzomibPomalidomide

Survival in multiple myeloma has increased with the introduction of novel agents
Kristinsson SY et al. JCO 2007;25:1993-1999Waxman A et al. Blood 2010, epub ahead of printTuresson et al. JCO 2010;28:830-4
Brenner H et al. Blood; 111:2521-6Kumar SK et al. Blood 2008;111:2516-20

Myeloma-specific survival by age and year of diagnosis for the 1st 10 years after diagnosis (SEER 1973-2009)
Kristinsson, SY, et al. Leukemia 2014

We need new drugs!

CarfilzomibPomalidomideVorinostat
PanobinostatElotuzumabDaratumumabAnd many more dude

• Current guidelines suggest life-long clinical follow-up of people with MGUS
• The impact of diagnosing and conducting clinical follow-up of MGUS on myeloma survival is unclear
MGUS

Does follow-up for MGUS matter?

The Role of Diagnosis and Clinical Follow-up of Monoclonal Gammopathy of Undetermined Significance on Survival in Multiple Myeloma
Sigurdardottir EE, et al and Kristinsson SY. JAMA Oncol. 2015

The Role of Diagnosis and Clinical Follow-up of Monoclonal Gammopathy of Undetermined Significance on Survival in Multiple Myeloma
Sigurdardottir EE, et al and Kristinsson SY. JAMA Oncol. 2015

The Role of Diagnosis and Clinical Follow-up of Monoclonal Gammopathy of Undetermined Significance on Survival in Multiple Myeloma
Sigurdardottir EE, et al and Kristinsson SY. JAMA Oncol. 2015

Go R et al. Clin Lymph, Myel &Leuk 2015
SEER study on more than 17,000 myeloma patients

Follow-up of MGUS is important

“Makes sense“

We can improve survival in asymptomatic patients
Mateos MV et al NEJM 2013

Kristinsson SY, et al. NEJM 2013

We can get great response rates
Korde N et al. JAMA Onc 2015

New diagnostic criteria for myeloma
Rajkumar VS et al. Lancet Oncol 2014

“Makes sense“
We are not waiting for fractures or other symptomes any more

Should we screen for MGUS?

Wilson and Jungner classic screening criteria
1. The condition sought should be an important health problem.2. There should be an accepted treatment for patients with recognized disease.3. Facilities for diagnosis and treatment should be available.4. There should be a recognizable latent or early symptomatic stage.5. There should be a suitable test or examination.6. The test should be acceptable to the population.7. The natural history of the condition, including development from latent to declared disease, should be adequately understood.8. There should be an agreed policy on whom to treat as patients.9. The cost of case-finding (including diagnosis and treatment of patients diagnosed) should be economically balanced in relation to possible expenditure on medical care as a whole.10. Case-finding should be a continuing process and not a “once and for all” project.

Which should we screen?• Elderly?• Obese?• Race?• Osteporosis?• Prior autoimmune disease?• Family history?

Potential harm of screening• Cost• Psychological harm• Low risk of progression• Unnecessary evaluations
– Bone marrow, X-ray, MRI etc• Only non-aggressive disease is captured

Thoushalt notScreen
Outside a
Clinical trial

Thanks!
Karolinska University HospitalMagnus BjörkholmÅsa DerolfMalin HultcrantzEbba Lindqvist
University of IcelandSigrún Helga LundElín Edda SigurðardóttirGuðbjörg JónsdóttirVilhjálmur SteingrímssonMaríanna ÞórðardóttirKristrún AradóttirIngigerður Sverrisdóttir
Icelandic Heart AssociationVilmundur GuðnasonGuðný Eiríksdóttir
Karolinska InstitutetTherese M-L AnderssonSandra ElorantaPaul W DickmanCaroline Weibull
National Institutes of HealthLynn R. GoldinRuth PfeifferMary L McMaster
Sahlgrenska University HospitalUlf-Henrik MellqvistCecilia Blimark
Skåne University HospitalIngemar Turesson
Umeå University HospitalAnders Wahlin Memorial Sloan Kettering
Ola LandgrenNeha KordeSham Mailankody

Thanks!
Support from
Stockholm County CouncilKarolinska Institutet FoundationsThe Swedish Cancer SocietyCancer Society in StockholmClinical Scientist Training Programme – KISwedish Blood Cancer SocietyMemorial fund of Ásrún EinarsdóttirLandpitali Research FundUniversity of Iceland Research FundThe Icelandic Research FundEU-grant (Marie-Curie)


Imaging-guided biopsies to capture residual disease and perform molecular characterization of MRD
Jens Hillengass MD
Department of Hematology and OncologyUniversity of Heidelberg
andDepartment E010 Radiology
German Cancer Research Center

Jens Hillengass University of Heidelberg
Growth patterns of multiple myeloma

Jens Hillengass University of Heidelberg
Minimal Diffuse Focal Mixed Salt andPepper
Baeuerle 2009 Radiologyn = 100 (MGUS and myeloma) 23 (23%) 34 (34%) 4 (4%) 36 (36%) 4 (4%)
Hillengass 2010 JCOn = 149 (indolent myeloma) 69 (46%) 38 (26%) 20 (13%) 22 (15%)
Staebler 1996 AJRn = 53 (myeloma all stages) 5 (10%) 12 (23%) 18 (34%) 13 (25%) 5 (9%)
Baur 2002 Cancern = 77 (myeloma all stages) 20 (26%) 24 (31%) 22 (28%) 9 (12%) 2 (3%)
Moulopoulos 2010 Leukemian = 82 (myeloma all stages) 18 (22%) 26 (31%) 34 (41%) 4 (4%)
Baur 1996 Rofon = 61 (symptomatic myeloma) 7 (11%) 15 (25%) 20( 33%) 14 (23%) 5 (8%)
Kusumoto 1997 Br. J. Haematoln = 61 (symptomatic myeloma) 11 (18%) 26 (43%) 11 (18%) 13 (21%)
Lecouvet 1998 Radiologyn = 80 (symptomatic myeloma) 19 (24%) 26 (32%) 35 (44%)
Moulopoulos 2005 Ann Oncoln = 142 (symptomatic myeloma) 11 (8%) 40 (28%) 71 (50%) 20 (14%)
Fonti 2008 J Nucl Med.n = 33 (symptomatic myeloma) 6 (18%) 13 (39%) 6 (18%) 8 (24%)
20%
20%
30%
30%
Growth patterns of multiple myeloma

Moulopoulos 2012 AJRJens Hillengass University of Heidelberg
Prognostic significance of growth patterns in initial MRI

Walker 2007 JCO, Hillengass 2013 Leukemia, Hillengass 2010 JCO, Bartel 2009 Blood, Zamagni 2011 Blood
MRI
PET-CT
Jens Hillengass University of Heidelberg
Prognostic significance of growth patterns in initial MRI

Jens Hillengass University of Heidelberg
Focal lesions in PET

initial after therapy
Courtesy of Stefan DelormeJens Hillengass University of Heidelberg
Diffusion weighted imaging

Jens Hillengass University of Heidelberg
Growth patterns of multiple myeloma

Jens Hillengass University of Heidelberg Walker 2007 JCO
Prognostic significance of residual lesions in MRI

Jens Hillengass University of Heidelberg
Prognostic Significance of residualfocal lesions after therapy
Hillengass 2012 Haematologica
p = 0.001
Prognostic significance of residual lesions in MRI

Jens Hillengass University of Heidelberg Hillengass 2012 Haematologica
Prognostic significance of residual lesions in MRI

initial after transplant
Jens Hillengass University of Heidelberg Hillengass 2012 Haematologica
Prognostic significance of residual lesions in MRI

Zamagni 2015 Clin Cancer ResJens Hillengass University of Heidelberg
Prognostic significance of residual lesions in PET-CT
Retrospective analysisN = 282 (73% treated with ASCT)

Jens Hillengass University of Heidelberg
Prognostic significance of residual lesions in PET-CT
N = 189 PET-CT after therapy88% ≧ VGPR55% CR
=> 29% of pts. in CR had residual lesions in PET-CTMedian PFS of PET + 44 monthsMedian PFS of PET - 84 months
Zamagni 2015 Clin Cancer Res

Jens Hillengass University of Heidelberg
Prognostic significance of residual lesions in PET-CT
Zamagni 2015 Clin Cancer Res

Jens Hillengass University of Heidelberg
Focal lesions at relapse
Walker 2007 JCO
Pattern at relapse
FL present in 54 patients (71%)
-20 patients (26%) with new MRI-FLs outside initial involvement
-21 (28%) larger than the original lesions
-11 (15%) with increase in size and new MRI-FLs

Primary aims
•Investigation of the genetic heterogeneity of malignant cells from focal lesions in different parts of the bone marrow compared with a “random sample” of the pelvis•Detection of different clones within a single lesion•Investigation of the clonal composition of residual lesions after systemic therapy
Jens Hillengass University of Heidelberg
Project

Work Plan
Initial work-upImaging
Whole-body-MRI with DWI, DCE-MRIPET-CT
Sample acquisitionRandom sampleBiopsy of up to 5 focal lesions
Sequential work-upafter systemic treatment if residual lesions are detectable
Initially
Post Treatment
Jens Hillengass University of Heidelberg
Project

Random BM-sample or
sample of FL
Ficoll
WBMLysis
MNC
MACS
CD138+ MMC
Flow (MRD)
FACSAria
Plasma cell content [%]
RNA DNA
iFISH
GEP SequencingJens Hillengass University of Heidelberg
Project

Jens Hillengass University of Heidelberg
Project

Jens Hillengass University of Heidelberg
Project

Jens Hillengass University of Heidelberg
Project

Jens Hillengass University of Heidelberg
Project

Jens Hillengass University of Heidelberg
Project

Project
Personnel• Jens Hillengass
=> Project supervision
• Hartmut Goldschmidt/ Jens Hillengass => Identification of
patients
• Sandra Sauer MD (hematologist) => Coordination
• Michaela Hillengass =>
Case management
• Jost Kloth MD (radiologist) =>
Identification of lesions
• Jennifer Mosebach (radiologist) => Image evaluation
• Stefan Hemmer MD (orthopedic surgeon) => Approval of lesions
Jens Hillengass University of Heidelberg

Thank you very much for your attention
S.D.G

Flow MRD Basics
• Most important parameters in MRD detection is number of cells analyzed AND quality of the sample.– Critical to establish precise sample handling
standards and numbers of cells standards– Critical to define when sample is NOT optimal
for analysis– Particularly important for definition of
“negative”• Incremental gains from adding additional
informative markers

Plasma Cell MRD History at MSKCC
• 25+ plasma cell flows/week. Peak 10-15/day• Gen 1: 4-color 7 tube (including isotypes) panel up to 500K cells
lyse/stain – Extremely time consuming (required a dedicated tech and
instrument) Difficult to analyze– Roughly 95% sensitive compared to morphology
• Gen 2:– One tube 8-color panel stain/lyse (up to 1.0 million cells)-
200ul. of marrow • CD38 CD138 CD56 CD117 CD19 CD45 cy kappa lambda• Very high sensitivity IF marrow is cellular (theoretically
0.0005%)• More sensitivity than FISH on sorted cells, IgH
(conventional)• Number of cells acquired depends on sample cellularity

Gen 3: for 10-color MRD with bulk lysis
• Consensus for using CD38, CD138, CD56, CD117, CD81, CD27, CD19, CD45 , kappa, lambda-10 currently suggested markers
• 10-color instruments are becoming more widespread (Navios/Canto 10)
• Efficient utilization of limiting resources – instrument time, sample amount, analysis time, digital
storage) vs. multi-tube panels– Acquisition of 5 million cells/tube =15-25 minutes+150 Mb
file• Reduces need for inferential reasoning and eliminates file
merging

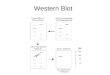
MM MRD workflow
Clinical sample
Sample preparationprior to MPF
Sample acquisition time
MRD assessment
Data storage
Single-tube protocol
5 x 106 cells required
reagents for 1 tube
20-25 mins / case
? time
Data from 1 tube
Two-tube protocol
1 x 107 cells required
reagents for 2 tubes
40-50 mins / case
? time (inferential reasoning)
Data from 2 tubes
? Sufficient material for additional tests: cytogenetics , molecular etc.
Doubling of reagent costs
Doubling of dedicated lab technician time and reduced availability of FACS
instrument

Panel Comparison
• Previous panel:CD38 BV510/CD19 BV421/kappa-FITC/lambda-PE/CD117 PC5.5/CD56 PC7/CD138 APC (B-A38) APC/CD45 APC-H7
• New PanelCD27 BV605/ CD38 BV510/ CD81 PB//kappa FITC/lambda PE/CD117 PC5.5/CD19 PC7/CD138 (B-A38) APC/CD56 APC-R700/CD45 APC-H7 (Final version)

Accuracy/Sensitivity Assessment
• 53 (final version) samples from patients with plasma cell disorder follow-up (20 post transplant, pre (22) and unknown (2)) unselected sample leftovers– 8 color number of cells range: (74K-596K, Mean 383K)– 10 color (38K-8700K, Mean 5900K)
• 10 samples from patients with “other “ disorders: lymphoma, MDS, thrombocytopenia
• Compare to predicate method• Analyst blinded to results obtained by another method

Example of 10-color analysis

Accuracy PCN Patients
2 Method Comparison: % Neoplastic PC in WBC
Discrepant samples post transplant

Patient Outcome

Precision/Linearity/Limit of Detection
• 5 abnormal Plasma cell sample spiked into a normal samples in triplicate• 4 sequential 10X dilutions (3 points in triplicate)• All samples independently processed and stained• Measure precision at each level• Establish precision near lowest expected abnormal cell numbers • Measure recovery at each level• Range 4500-30 cells

Precision/Linearity/Limit of Detection
MM MRD LINEARITY abnormal PC # Total PC #
abnormal pc % of WBC
abnormal pc % of total PC total PC %of WBC WBC #
Tube 1 4538.0 11811.0 0.3300% 38.4218% 0.61% 1374666
Tube 2
773.0 8406 0.0360% 9.1958% 0.36% 2019964725.0 8537 0.0380% 8.4924% 0.38% 1815533723.0 8615 0.0370% 8.3923% 0.37% 1849434
CV 3.8 1.2 2.7 5.0 2.7 5.8mean 740.3 8519.3 0.0370% 8.6935% 0.37000% 1894977
Tube 3
123.0 9970 0.0057% 1.2337% 0.57% 2146026101.0 10244 0.0066% 0.9859% 0.44% 1463180115.0 8992 0.0075% 1.2789% 0.43% 1543416
CV 9.9 6.8 13.6 13.5 16.3 21.7mean 113.0 9735.3 0.0066% 1.1662% 0.48000% 1717541
Tube 4
27.0 11970 0.0014% 0.2256% 0.54% 184547830.0 12606 0.0016% 0.2380% 0.57% 185416433.0 14585 0.0016% 0.2263% 0.60% 2052792
CV 10.0 10.4 7.5 3.0 5.3 6.1mean 30.0 13053.7 0.0015% 0.2299% 0.0 1917478
Tube 5 0.0 1010 0.0000% 0.0000% 0.21% 272866

Precision/Linearity/Limit of Detection
Recovery slightly increases with fewer abnormal cells

Practical Points
• 10-color assay is highly sensitive single tube assay• Theoretical sensitivity is still dependent on sample
quality/number of cells• Approximately 4 hours from sample to report• 5-6 sample batch is ok• Cocktail (surface and light chain) is stable for at least 2 weeks• 15-25 minute instrument time/sample• 150 Mb file• 15 minute import/analysis/reporting time on average• Limited analysis of “other” populations
– Assess presence of mast cells/immature myeloid precursors/B-cell precursors
– Dedicated tubes run for other disorders as indicated

Euroflow vs. 10 PC: Cell Numbers in MSKCC# Events 10C PC Tube # Events EuroFlow
5195356 3704581 23782174767567 3192946 23229301967763 1396119 9947505225656 2857943 29345025964189 3351625 33006934840782 3692511 24157943062964 1422475 10899646000000 3443175 26385755424060 2631025 17060645076271 1835450 16403025986407 3303268 26629906000000 3566177 18759012406885 2065600 9050504860198 4575511 20857256116838 5031300 35449006000000 4602250 33839756000000 4576445 486827510000000 5729045 5660176
4741443 3360708 25700766041259 6000000 50936745729316 3055708 28068856000000 4661975 35844936000000 6000000 16344124607295 5351200 18030136000000 6000000 50957486114018 4485808 36452756000000 4210250 28512752299225 2126000 12763881259504 1236993 9560763473324 3539728 21456283037395 2728306 11896255807403 4351150 33941846000000 4547450 41456505017601 4335548 38682086000000 5136100 35568805600889 3900950 28617021215018 3121100 6209902085615 2588975 1746216000000 6000000 52226946941345 6183046 36275256000000 6000125 487822510000000 6104025 56690256000000 6000000 3096200
• 4 ml of marrow split in half between Euroflow and MSKCC tests
• Entire sample used unless >30 million
• 45 marrows attempted:• 39 > 3 million (10
PC)• 35 >3 million: EF1,
20> 3 million EF2• Head to head analysis
comparison in collaboration with Dr. Orfao

Thank You
Recommended