Shock
Metropolitan Community CollegeFall 2013
Jane Miller, RN MSN

Objectives• Define pathophysiology of shock, including
classifications.
• Identify physiologic events during shock if progresses.
• Identify etiology of shock including hypovolemic, cardiogenic, distributive, and obstructive shock.
• Identify clinical manifestations, treatment modalities, and nursing interventions for each type of shock. Identify the potential for multiple organs dysfunction syndrome.
• Define intervention activities for shock prevention.

Shock• Not a disease
• Decrease in tissue perfusion due to– Alteration in blood or plasma volume– Alteration in peripheral vascular resistance– Alteration in the hearts ability to pump
• Can lead to – Multiple organ dysfunction syndrome (MODS)– Death
Shock Syndromes• Hypovolemic or low-volume– loss of blood/fluid volume
• Distributive or high-space– Factors that affect the blood vessels
• Mechanical or obstructive– Factors that affect the heart

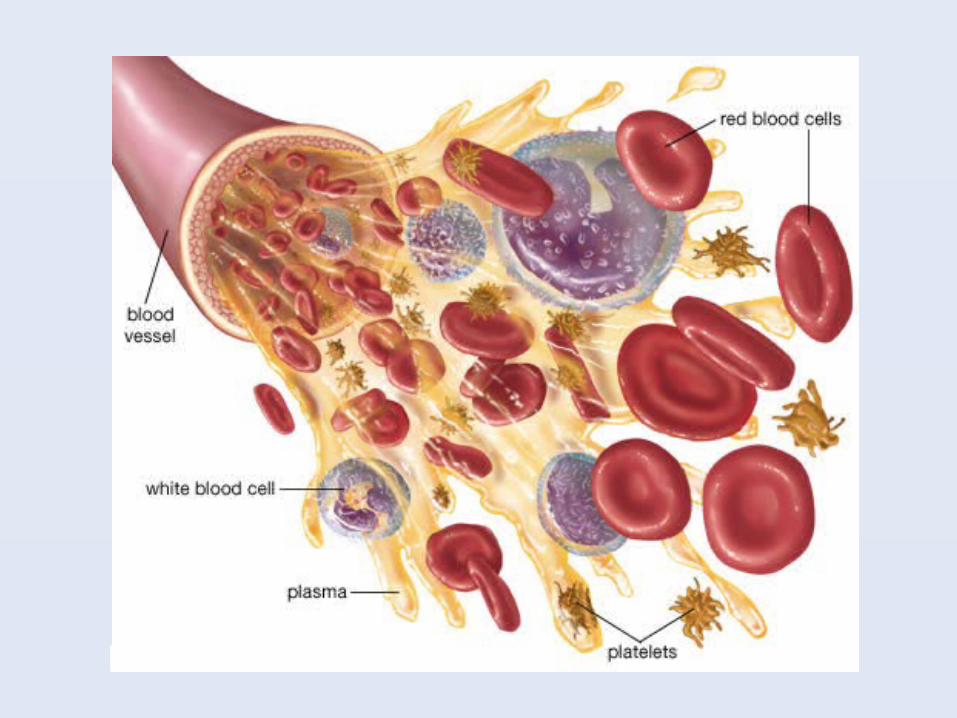
Blood Composition
• Red blood cells– Transport oxygen and carbon dioxide to
and from cells
• White blood cells– Protect against foreign matter
• Platelets– Form a plug at the site of injury
• Plasma– Liquid that blood cells are suspended in

Regulation of Blood Pressure
• Stroke Volume (SV)– Amount of blood leaving the left ventricle
with each heart contraction
• Cardiac Output (CO)– Amount of blood leaving the left ventricle
per minute CO = HR x SV
• Peripheral Vascular Resistance (PVR)– Resistance to the flow of blood by vascular
musculature and diameter of the blood vessels

Regulation of Blood Pressure
BP = CO x PVR
Or
BP = HR x SV x PVR

Regulation of Blood Pressure
When you have a decrease in HR, SV, or PVR what do you get?
A decrease in BP and subsequently tissue perfusion

Pathophysiology of Shock
• Results from inadequate tissue perfusion
• Inadequate tissue perfusion impairs cellular metabolism
• Impaired cellular metabolism results in impaired oxygen and glucose use
• If this is not corrected cellular death occurs
Normal Cellular Function
• Nutrients are broken down into ATP
• ATP is used for cellular functions
• ATP can be synthesized aerobically or anaerobically
• Aerobic metabolism is more efficient
• Anaerobic is not only less efficient it produces lactic acid.

Pathophysiology of Shock
Sodium
H2O
Potassium
This increase of sodium and H20 into the cell causes potassium to exit, cellular swelling, eventual rupture and cell death
A lack of oxygen changes the cell metabolism from aerobic to anaerobic

Impaired Glucose Use
• Impaired cellular metabolism also produces insulin resistance
• As the body responds to the stress it produces more glucose to assist in healing
• Because the body doesn’t use the glucose properly blood glucose levels rise
• Insulin resistance and glucose toxicity further impair cell metabolism

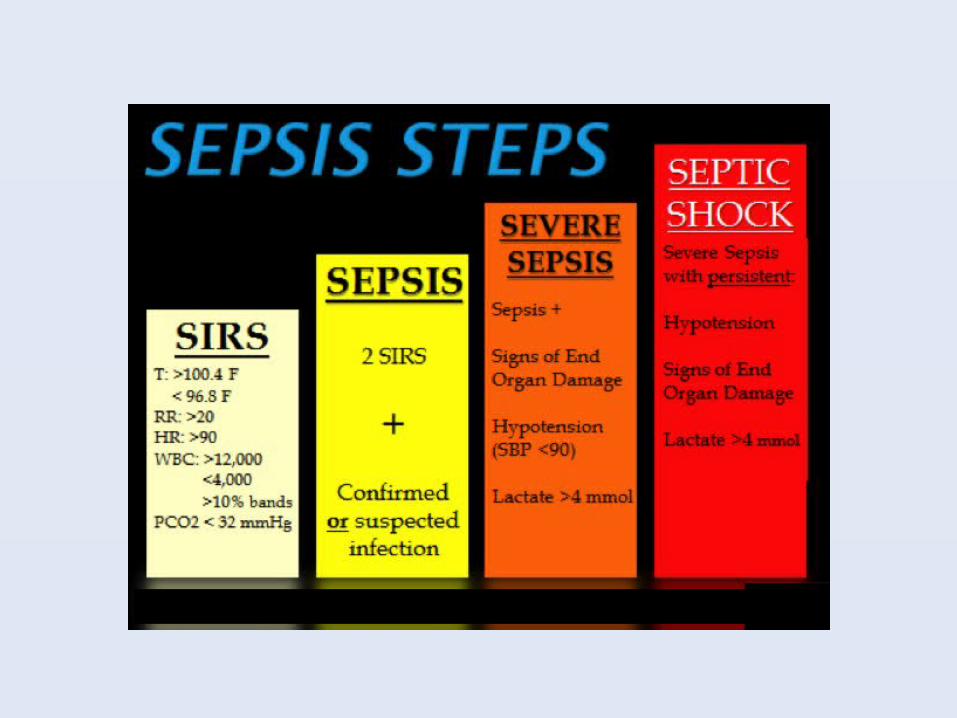
SIRS
• Systemic inflammatory response syndrome
• Often associated with septic shock
• First phase of shock
• Presents much like sepsis– HR - PaCO2
– RR– Temp– WBC


Signs of Shock• Neurological– Altered mental status– Seizures– Coma
• Cardiovascular– Cardiac output declines–HR increases– Dysrhythmias– Absence of peripheral pulses
• Genitourinary– Decreased filtration– Decreased urinary output
• Integumentary– Pale and fragile
• Musculoskeletal– Weakness and wasting
• Lungs– Increased RR– Decreased O2 saturation
– ARDS
Shock Syndromes• Hypovolemic or low-volume– loss of blood/fluid volume
• Distributive or high-space– Factors that affect the blood vessels
• Mechanical or obstructive– Factors that affect the heart

Hypovolemic Shock
• Can result from a loss of blood, plasma, or body fluids
• Hemorrhagic shock is most common– Trauma, GI bleeds, ruptured AAA
• Other causes– Diarrhea– Vomiting– Inadequate repletion of fluid loss
• Burns, heat stroke, third spacing

Decreased Blood Volume
Decreased Cardiac Output
Decreased Venous Return
Decreased Stroke Volume
Decreased Tissue Perfusion

Medical Management
• Correct the underlying cause– e.g. stop the bleeding, vomiting,
diarrhea
• Restore intravascular volume
• Redistribute fluid volume

Mechanical Shock
• A condition that slows or obstructs blood flow in or out of the heart– Ineffective pump– Physical obstruction
• A decrease in blood flow through the heart decreases stroke volume and cardiac output
• Hypotension• Decreased tissue perfusion

Decreased Cardiac Function
Decreased Blood Pressure
Decreased Stroke Volume
Decreased Cardiac Output
Decreased Tissue Perfusion

Mechanical Shock
• Two different types– Cardiogenic• When the heart is unable to pump
effectively• MI, ruptured ventricle, cardiomyopathy
– Obstructive• Physical obstruction• Cardiac tumor, massive PE, cardiac
tamponade

Medical Management
• Limit further myocardial damage and preserve healthy myocardium
• Remove source of obstruction
• Improve cardiac function by increasing cardiac contractility and decrease ventricular afterload

Mechanical Assistive Devices
• A mechanical assistive device may be needed if first line treatments fail– Intra-aortic balloon pump– Left or right ventricular assist devices
• Last option–Heart transplant

Distributive Shock
• A precipitating event causes massive vasodilation
• Blood pools in the periphery• Decreased venous return results in
decreased stroke volume and cardiac output
• Hypotension• Decreased tissue perfusion
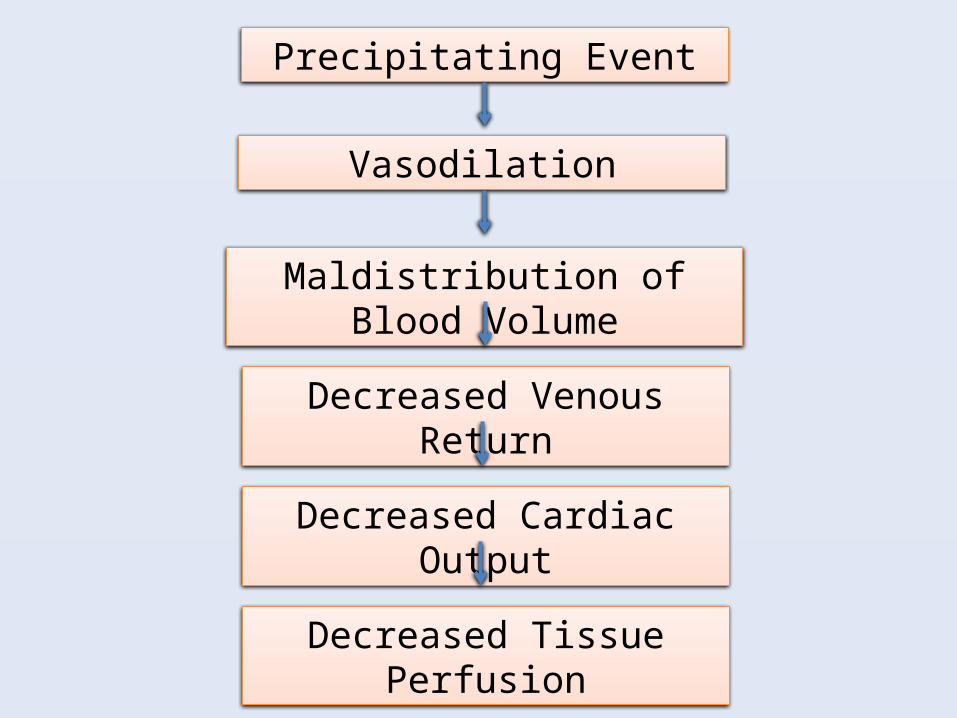
Precipitating Event
Vasodilation
Maldistribution of Blood Volume
Decreased Venous Return
Decreased Cardiac Output
Decreased Tissue Perfusion

Distributive Shock
• Three different types– Anaphylactic shock• Insect bites, medication allergies, food
allergies
–Neurogenic shock• Spinal cord injury, anesthetic agents, severe
pain
– Septic Shock• Bacterial and viral infections

Anaphylactic Shock
• Results from an antigen-antibody reaction
• Symptoms are usually immediate• Blood pooling in the periphery• Pulmonary vasocontriction• Maintenance of an airway is critical

Neurogenic Shock
• Imbalance between the sympathetic and parasympathetic stimulation of vascular smooth muscle
• This causes vasodilation• Caused by injury or medications that
affect the spinal cord or medulla• Clinical symptoms may be different–Hypotensive, bradycardic, vasodilation
Septic Shock
• Occurs when an infectious agent causes systemic decompensation
• Acute circulatory failure characterized by persistent hypotension unexplained by other causes
• 3 principle actions occur with sepsis– Inflammation– Coagulation– Fibrinolysis
Nursing Management• Prevention• 2 large bore IVs• Place patient in modified
trendelenburg position• Monitor for signs of transfusion
reaction• Monitor for fluid overload and
pulmonary edema• Monitor VS, especially temperature

• Apply oxygen, administer meds, monitor labs
• Monitor for skin breakdown, turn q 2 hrs, and provide skin care
• Watch for DVT• Monitor ECG• Wound care• I&O• Enteral or parental nutrition• ROM• Emotional support for patient and
family
• Medications– Vasopressors– Inotropes– Antiemetics & antidiarrheals– Antibiotics– Insulin– Corticosteriods– Blood thinners and clot busters– Opiods– Antianxiety– Sedation– rhAPC
This is not a complete list of medications and some listed will not
be appropriate for all clients experiencing shock

MODS
• Multiple Organ Dysfunction Syndrome– End result of severe sepsis
– Triggered by a critical injury or disease process that initiates a massive systemic inflammatory response
• Multiple injuries, burns, hypovolemic shock, acute pancreatitis, ARDS, acute renal failure
• Does not require an infectious trigger

Pathophysiology
• Primary or early MODS–Hypoperfusion that triggers inflammatory
and stress responses
• Secondary or late MODS– Excessive inflammation following the initial
insult–Manifested in organs distant from the
original injury– Three primary mechanisms: inflammation,
coagulation, and fibrinolysis

Clinical Manifestations & Diagnosis
• Depend on the area or areas affected
• Early MODS is difficult to monitor
• Late MODS follows a specific pattern–Measured using the SOFA score– Evolves over 14 days to weeks
• Diagnostic tests are specific to the organ system(s) that are failing
Treatment
• Prevention is key• Antibiotics• Intubation• Fluid resuscitation• Vasopressors• Analgesics• Sedation• Enteral feedings• Glucose monitoring

Nursing Management
• Hand hygiene and skin care • Monitoring of VS• Positioning• Decrease oxygen demands– Pain and anxiety meds– Rest
• Emotional support• Frequent patient assessments
Resources
• Osborn, Wraa & Watson chapter 61• YouTube video on shock– http://www.youtube.com/watch?
v=CbM4UihE1TQ
Recommended