J. Endocrinol. Invest. 7: 29, 1984
Serum thyroglobulin determinations in the differential diagnosis of congenital hypothyroidism
F. Pacini*, R. Lari*, P. La Ricca***, L. Grasso*, F. Di Bartolo***, G.F. Fenzi*, M. Ciampi*, S.G. Gragnani***, L. Baschieri*, and A. Pinchera** *Cattedra di Patologia Medica 2, **Gattedra di Endocrinologia e Medicina Costituzionale, Universita di Pisa, Via Roma 67, 56100 Pisa, and ***Divisione Pediatrica, Ospedale Civile di Cecina, 57023 Cecina, Italy
ABSTRACT. The value of serum thyroglobulin (Tg) determination in the differential diagnosis of congenital hypothyroidism was assessed by serum Tg measurements in 14 patients with proven congenital hypothyroidism, in 3 subjects with transient perinatal hypothyroidism, in 3 newborns with congenital thyroxine binding globulin (TBG) deficiency and in 34 normal controls. Serum Tg was undetectable in all 6 cases with thyroid agenesis, normal or moderately elevated in the 4 cases with ectopic thyroid, markedly increased in the 4 cases with dyshormonogenic goiter and normal in the 3 caseswith transient hypothyroidism and in the 3 with TBG deficiency. The present data indicate that serum Tg measurements may be useful in the differentiation of athyreotic hypothyroidism from other conditions of congenital hypothyroidism.
INTRODUCTION Thyroglobulin (T g) is secreted by the thyroid gland and is detectable in the serum of normal adult subjects (1-3). Serum Tg is elevated in patients with hyperstimulated thyroids and in patients with metastatic differentiated thyroid cancer while it is low or undetectable in those free of recurrent disease after total thyroidectomy (4-6). T 9 is always detectable in the cord blood of normal newborns with mean values higher than those in normal adults and in pregnant women at delivery (7 -11). We confirmed these findings in a very large population of newborns and demonstrated that 1'g remains detectable during the. first week of life (12). Recently a few studies in newborns with congenital hypothyroidism have suggested that serum Tg measurements may be useful in the diagnosis of this condition (13, 14). In the present study we re port the results of serum Tg measurements in a group of newborns and children with proven congenital hypothyroidism of different etiologies, some of whom were detected in our screening program for congenital hypothyroidism and others referred to us from other institutions. In addition, 3 newborns with congenital thyroxine binding globulin (TBG) deficiency and 3 with transient hypothyroidism were studied.
MATERIALS AND METHODS Congenital hypothyraid subjects. A total of 14 patients
Key-words: Thyroglobulin, congenital hypothyroidism, TBG
Correspondence. F. Pac,n, MD. Cattedra di Patologia Medica 2. Universita di Pisa. V,a Roma 67. 56100 Pisa.ltaly
Rece,ved July 10. 1983; accepted September 10. 1983
29
with congenital hypothyroidism (6 newborns detected during our screening program and 1 newborn and 7 children diagnosed during the first year of life referred from other institutions) were available for study. In the seven patients diagnosed at birth, thyroxine (T4 ) and thyrotropin (TSH) were measured in dried filter paper spots obtained at 3-4 days of life . Hypothyroidism wa.s confirmed in all patients by measurements of serum concentrations of T 4' TSH, triiodothyronine (T 3) and T3
resine uptake (T 3U), at a later life. ' A thyroid scan was performed in all cases after more than 18 months of age. Serum Tg'was measured in all patients either before institution of thyroid medications and after withdrawal of therapy. In one patient serum cord blood was also available.
Transient hypothyroidism. This condition was present in 3 newborns in whom thyroid hormone levels were in the hypothyroid range at birth, but were in the normal range when they were recalled.
Congenital TBG deficiency. Three infants with congenital TBG deficiency were detected during our screening program for congenital hypothyroidism. They were diagnosed on the 'basis of low T4 and normal TSH values with high T3U and low TBG values. Two were males with absent TBG and 1 was a female with low but detectable serum TBG concentration.
Normal contrals. Eight infants (1-3 months of age) and 26 children (5-16 years old) were studied as the normal control population for these age groups.
Serum Tg measurements. Serum Tg was measured by radioimmunoassay as previously described·(2). All sera were screened for the presence of anti-T 9 autoantibodies and were negative in all subjects.

F. Pacini, R. Lari, P. La Ricca, et al.
Serum T4 , T3 , T3U, TSH, TBG and spotT4 andTSH were all measured using commercial kits (T3 , T4 and T3U kits were from Miles Lab., Cavenago, Milano; TSH kit was from Diagnostic Product Corporation, Los Angeles, California; TBG kit was from Corning, Medfield, Massachussets; spot T 4 and spot TSH kits were from Biodata, Roma).
RESULTS
In 7 patients in whom hypothyroidism was diagnosed during the first week of life Tg was measured in serum sampies collected during the first two months of life. In the 7 patients who were not screened at birth, hypothy-
roidism was detected during the first year of life and Tg measured on serum sampies obtained at the time of referral to our clinic, between the age of 3 and 16 years; they were off thyroid replacement therapy. Results of thyroid function tests, Tg measurements and thyroid scans in patients with congenital hypothyroidism, transient hypothyroidism and congenital TBG deficiency are summarized in Table 1. In 6 patients hypothyroidism was due to thyroid agenesis. In 8 patients with undetectable or low T 4 and high TSH values, thyroid scan revealed the presence of an ectopic (sublingual) thyroid in 4, and a diffuse goiter in the other 4. In 3 subjects hypothyroidism was suspected on the basis of low T 4 and high TSH values on blood spot but they were
Table 1 - Tg, thyroid hormones, TSH, TBG and thyroid scan in subjects with congenital hypothyroidism, transient hypothyroidism, congenital TBG deficiency and in normal subjects.
Blood spot 1.2 SERUM
Subject Sex T4 TSH Tg T3U T4 T3 TSH TBG Age ThyrOid scan No !lg/dl !lU/mi ng/ml % !lg/dl ng/dl !lU/mi !lg/ml
Congenltal hypothyroidism
M 7.8 > 200 < 1253 33 < 1.5 < 37.5 > 100 30 days Agenesis
2 4.2 185 < 1.25 27.9 < 1.5 < 37.5 >100 45 days Agenesis
3 <125 312 < 1.5 < 37.5 88 10 years Agenesis
2.8 >200 < 1.25 19A < 1.5 51 >100 22 days Agenesis
1.9 >200 < 1.25 < 1.5 < 37.5 > 100 14 days Agenesis
6 3.5 >200 < 1.25 < 1.5 >100 14 days Agenesis
M 3.0 > 200 200 38.4 4.6 156 > 100 30 days Ectop'c
8 44 28.5 2.9 129 100 12 years Ectop'c
9 M 167 50.1 < 1.5 < 37.5 66 3 years Ectopic
10 M 45.1 2.9 82.0 100 16 years Ectop'c
11 500 33 < 1.5 < 37.5 45 16 years Goitre4
12 1000 3.1 >100 8 years GOitre4
13 1000 4.8 >100 9 years GOitre5
14 M 450 2.5 > 100 7 days Goitre6
Congenltal TBG deflciency
15 M 2.3 < 12.5 82 85.2 28 55.0 3.3 < 0.5 27 days Normal
16 M 2.6 < t2.5 41 52.5 2.0 80.0 2.6 < 0.5 28 days Normal
17 4.8 < 12.5 130 717 6.9 201 < 0.5 125 48 days Normal
Transient hypothyroidlsm
18 M 7.2 > 200 96 24.8 5A 204 23.9 21 days Normal
19 M 3.1 52 120 31.5 < 1.5 154 > 100 30 days Normal
54 300 9.3 247 1.2 3 months
20 7.2 130 106 44A .11.0 319 15 60 days Normal
Normal controls
(8)7 68± 11 8 38± 1.8 8A ± 0.6 211 ± 16 2.4 ± OA 1-3 months
(26)7 15± 22 30 ± 0.9 7.0 ± 0.3 203 ± 6.6 2.6 ± 02 5-16 years
1 Blood spot determinations were carried out in day 3-4 of life; they are available only in newborns detected in our screening program
2Normal spot T4 and spot TSH values in our laboratory are> 7.2119/dl and < 5011U/ml, respectively. 31n this patient Tg was also undetectable in the cord blood serum.
4Perchlorate dlscarge test positive. 5Dehalogenase defect.
6Not yet studled 7Number in parenthesis represents the number of subjects studied. 8M± SE
30

1000
100
E "Cl c (9 f-
10
1.25 nd
Agenesis n:=6
-
-
---••••• 0
HYPOTHYROID Sub- With
lingual gOltre n=4 n=4
00
0
•
• 0
0
0
1--- 1---
Transient Hypo-TBG Normals
n=3 n=3 n = 34
• • • • • • • • • -. • 0 • ·0
000
00
D~: o 0
0 0
0 000
---- -- ---00
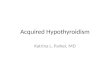
Fig.1 - Serum Tg levels in subjeets with eongenital hypothyroidism due to different etiologies, in patients with eongenital TBG delieieney and in normal subjeets. Closed eireles indieate subjeets between 1 and 3 months 01 age, open eireles indieate ehildren 01 more than 3 years 01 age. In the normal group, solid bar represents the mean lor elosed eire/es, open bar is the mean lor open eireles. The broken horizontalline is the limit 01 deteetability 01 our assay. Tg eoneentrations are in log seale. nd = not deteetable.
Serum thyroglobulin in congenital hypothyroidism
considered to have transient hypothyroidism since their hormone levels were in the normal range when tested again 20 to 45 days after birth. In 3 additional subjects, spot T 4 value was low and spot TSH undetectable. T 3U and TBG measurements in the sera of these newborns revealed congenital TBG deficiency. As shown in Figure 1, serum Tg values were undetectable « 1.25 ng/ml) in the 6 patients with thyroid agenesis, normal or mOderately high in those with ectopicthyroid (m ± SE = 1 04 ± 46 ng/ml) and extremely high in those with dyshormonogenic goiter (737 ± 151 ng/ml). In patients with transient hypothyroidism or TBG deficiency, serum Tg values were always detectable with mean values of 107 ± 6.9 and 69 ± 9.6 ng/ml, respectively. Serum Tg values in normal subjects between 1 and 3 months of age were 68 ± 11 ng/ ml and in normal subjects between 5 and 16 years of life were 15 ± 2.2 ng/ ml. The effects of thyroid replacement therapy on serum T 9 values are shown in Table 2. As expected in patients with undetectable serum Tg values while off thyroid therapy, no change was observed after institution of thyroid medications. Serum Tg values in patients with thyroid tissue decreased significantly' from pretreatment values when on thyroid replacement therapy. A decrease in serum TSH was also observed.
DISCUSSION Congenital hypothyroidism is a disease affecting about 1 in 3,000-4,000 newborns (15). Currently, most screening programs for detecting this condition are based on T 4 and TSH measurements on dried filter paper blood spots during the first week of life and, if hypothyroidism is suspected, on serum T4 and TSH values. With this procedure the differential diagnosis between the various forms of congenital hypothyroidism is usually not possible and is delayed until a thyroid scan can be carried out, usually at about 2 years of life,
Table 2 - Serum Tg and TSH belore and alter institution 01 replaeement therapy with I-thyroxine in hypothyroid subjeets.
Patients diagnosis Belore therapy U nder therapy No Tg' TSH2 Tg TSH
Thyroid agenesis < 1.25 > 100 < 1.25 <0.6
2 Thyroid agenesis < 1.25 > 100 < 1.25 3.9
3 Thyroid agenesis < 1.25 88 < 1.25 <0.6
4 Thyroid agenesis < 1.25 > 100 < 1.25 <0.6
8 Eetopie thyroid 44 > 100 25 <0.6
7 Eetopie thyroid 200 > 100 40 <0.6
1 Tg is In ng/ml; 2TSH is in JlU I ml
31

F. Pacmi, R. Lari, P. La Rlcca, el al.
after temporary withdrawal of thyroid hormone replacement therapy. Our data in subjects with congenital hypothyroidism of different etiologies, suggest that serum T 9 determinations are useful in the differential diagnosis of congenital hypothyroidism before a thyroid scan is performed. In agreement with previous observations (13, 14, 16) in newborns with congenital hypothyroidism, serum Tg was undetectable in all our subjects with thyroid agenesis. In one of these patients, Tg was also undetectable in the cord blood. Unfortunately, cord blood was not available in the other patients. In contrast, normal or elevated serum Tg values were observed when hypothyroidism was due to ectopic thyroid or to a dyshormonogenic goiter. The small number of cases in these groups do not permit a cut-off point which could differentiate between these two conditions, although serum T 9 values in the goitrous patients were significantly higher than in those with ectopic thyroid. Two other studies (17, 18) reported detectable serum Tg in patients with ectopic thyroid and undetectable in athyreotic sUbjects, findings which are in agreement with the present data. However, in 3 out of 10 hypothyroid patients with thyroid gland in a normal position on scanning, Black et al. (17) found no detectable serum Tg. Similarly, one of the 3 goitrous patients studied by Czernichow et al. (18) had undetectable plasma Tg values. These findings were taken as evidence of a structural abnormality of T 9 or failure of its synthesis. We did not observe similar patients in our series, but agree that this possibility should be ruled out in the absence of detectable circulating.T g. To our knowledge data on serum Tg in newborns with congenital TBG deficiency have been not previously reported. The present study indicates that the finding of normal serum Tg in association with low serum T4 and normal serum TSH provides some additional support to the suspicion of congenital TBG deficiency, a condition which is encountered in screening programs with a frequency of about 1 in 8,000-9,000 newborns (19, 20). Finally, serum T 9 determination cannot differentiate patients with transient hypothyrodism from those with permanent congenital hypothyroidism with functioning thyroid tissue.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the cooperation of Or. Marla Carta SorClni and Or. Vincenzo Macchia. who provided so me of the serum sampies fram hypothyroid subjects, and Or. LE Braverman for helpful suggestion in the preparatlon of the manuscript.
REFERENCES
1. Van Herle A, Vassart G, Dumont JE. Control of thyroglobulin synthesis and secretion. N. Engl. J. Med. 301. 307, 1979.
32
2. Pacini F., Pinchera A, Giani C, Grasso L, Doven F., Baschieri L. Serum thyroglobulinin thyroid carcinoma and other thyroid disorders. J. Endocnnol. Invest. 3 283,1980.
3. Gardner DF., Rothman J, 'Utiger R.D. Serum thyroglobulin in normal subjects and patients with hyperthyroidism due to Graves' diseClse. effects 01 T 3' iodide, 131 1 and antithyroid drugs. Clin. Endocrinol. (Oxl.) 11. 585, 1979.
4. Van Herle A.J., Uller R.P. Elevated serum thyroglobulin a marker 01 metastases in differentiated thyroid carcinomas. J. Clin.lnvest. 56 272,1975.
5. Pacini F., Pinchera A, Giani C., Grasso L., Baschieri L. Serum thyroglobulin concentration and 131_1 whole body scans in the diagnosis 01 metastases Irom differentiated thyroid carcinoma (alter thyroidectomy). Clin. EndocrinoL (Oxl.) 13 107, 1980.
6. Shlossberg A.H., Jacobson JC, Ibbertson HK Serum thyroglobulin in the diagnosis and management 01 thyroid carcinoma. Clin. Endocrinol. (Oxt.) 10. 17, 1979.
7. Torrigiani G, Doniach D., Roitt I.M. Serum thyroglobulin levels in healthy subjects and in patients with thyroid disease. J. Clin. Endocrinol. 29. 305, 1969.
8. Van Herle A.J., Uller R.P., Matthews NL, Brown J. Radioimmunoassay lor measurement olthyroglobulln in human serum. J. Clin.lnvest. 52.1320,1973.
9. Pezzino V., Filetti S., Belliore A, Proto S., Donzelli G, Vigneri R. Serum thyroglobulin levels in the newborn. J. Clin. Endocrinol. Metab. 52 364, 1981.
10. Roti E., Gnudi A., Braverman L.E, Robuschi G., Emanuele R., Bandini P., Benassi L., Pagliani A., Emerson CH Human cord blood concentrations 01 thyrotropin, thyroglobulin, and iodothyronine alter maternal administration 01 thyrotropin-releasing hormone. J. Clin. EndocrinoL Metab. 53 813, 1981.
". Pacini F, Grasso L, Giani C., La Ricca P., Fenzi GF, Pinchera A, Monzani F., Ciampi M, Bartalena L. Tireoglobulina circolante nel neonato. comportamento lisiologico e possibile applicazione netto screening delI'ipotiroidismo congenito. J. EndocrinoL Invest. 4 (Suppl. 1).177,1981.
12. Giani C, La Ricca P, Grasso L, Ciampi M, Taddei p, Lari R., Fenzi G.F. Serum thyroglobulin levels in normal and hypothyroid newborns. Ann. Endocrinol. (Paris) 42 72A, 1981.
13. Osotimehin B., Black EG, Hoffenberg R. Thyroglobulin concentration in neonatal blood: a POSSI
ble test for neonatal hypothyroidism Br. Med. J. 2. 1467, 1978.
14. Ket JL, de Vijlder J.J.M., Bikker H., Gons MH, Tegelaers H.H. Serum thyroglobulin levels. The physiological decrease in inlancy and the absence in athyroidism. J. Clin. EndocrinoL Metab. 58 1301, 1981.

15. The Newborn Committee 01 the European Thyroid Association. Progress report on neonatal screening lor congenital hypothyrodism in Europe. In: Burrow G.N. (Ed.), Neonatal thyroid screening. Raven Press, New York, 19'80, p .. 107.
16. Roitt IM., Torrigiani G. Identilication and estimation 01 undegraded thyroglobulin in human serum. Endocrinology 81: 421, 1967.
17. Black E.G., Bodden J., Hulse A., Hoffenberg R. Serum thyroglobulin and hypothyroid neonates. Clin Endocrinol. (Oxl.) 16: 267, 1982
18. Czernichow P., Schlumberger M., Pomarede R., Fragu P.
33
Serum thyroglobulin in congenital hypothyroidism
Plasma thyroglobulin measurements help determIne the type 01 thyroid delect in congenital hypothyroidism. J. Clin. Endocrinol. Metab. 56: 242, 1983.
19. Carta Sorcini M., Fiore L., Tomarchio S., Carta S, Romagnoli C., Curr6 V, Segni G. Pilot study lor congenital hypothyroidism, preliminary report. J. Endocrinol. Invest. 3: 181, 1980.
20. Dussault J.H., Marvin L.M., La Franchi S., Murphey W.H. Regional screening lor congenital hypothyroidism results 01 screening one million North American inlants with lilter paper spot T4-TSH. In: Burrow G.N. (Ed.), Neonatal thyroid screening. Raven Press, New York, 1980, p. 155.
Recommended