Sequencing DMTs in Clinical Practice
Gavin Giovannoni Blizard Institute, Barts and The London School of Medicine
December 2014

Disclosures
Over the last 15 years Professor Giovannoni has received personal compensation for participating on Advisory Boards in relation to clinical trial design, trial steering committees and data and safety monitoring committees from: Abbvie, Bayer-Schering Healthcare, Biogen-Idec, Canbex, Eisai, Elan, Fiveprime, Genzyme, Genentech, GSK, GW Pharma, Ironwood, Merck, Merck-Serono, Novartis, Pfizer, Roche, Sanofi-Aventis, Synthon BV, Teva, UCB Pharma and Vertex Pharmaceuticals.
Professor Giovannoni would like to acknowledge and thank Biogen-Idec for making available data slides on daclizumab for this presentation. He would also like to thank numerous colleagues for providing him with data and/or slides for this, and other, presentations.
Professor Giovannoni’s tour to Canada has been kindly sponsored by Biogen-Idec, therefore please interpret anything he says about Biogen-Idec’s products in this context.
This presentation has been designed and prepared by Professor Giovannoni with no input from any other parties.

.

IFNbeta
GA
Teri
DMF Fingo
Nz
Az
Treatment Complexity
2014
7 IFNbeta
GA
Teri
DMF
Fingo Nz
Az
Dac
Anti-CD20
2016
9

Copaxone-20
Copaxone-40 Synthon
IFNbeta
GA
Teri
DMF Fingo
Nz
Az
Treatment Complexity
2014
7 IFNbeta
GA
Teri
DMF
Fingo Nz
Az
Dac
Anti-CD20
2016
9
Betaferon
Rebif
Avonex Extavia
Plegridy

What is active MS?
2001 Clinical
2009 Clinical and MRI
2014 Clinical or MRI
Inactive MS: no relapses or MRI activity in the last 24 months
Active MS: relapses in the last 12 or 24 months and/or MRI activity in the last 12 months
Highly active MS: relapses in the last 12 months and MRI activity in the last 12 months
Rapidly-evolving severe MS (RES); two disabling attacks in a 12
month period and MRI evidence of activity during this period.

What is active MS?
2001 Clinical
2009 Clinical and MRI
2014 Clinical or MRI
Inactive MS: no relapses or MRI activity in the last 24 months (NEDA)
Active MS: relapses in the last 12 or 24 months and/or MRI activity in the last 12 months
Highly active MS: relapses in the last 12 months and MRI activity in the last 12 months
Rapidly-evolving severe MS (RES); two disabling attacks
in a 12 month period and MRI evidence of activity
during this period.

IFNbeta
GA
Teri
DMF
Treatment Ladder
DMF
Fingo
Nz Az

.

100 MSers
Who are the
responders?

?
20:80

?
40:60

Natalizumab STRATA: stable EDSS scores for up to 5 years
*P<0.0001
Kappos L et al. Presented at ECTRIMS; October 10–13, 2012; Lyon, France P520.
1 Year 2 Years 3 Years 4 Years 5 Years
Cessation/
Treatment Gap* Original Placebo
Original Natalizumab
Original Placebo – Now on Natalizumab
Mean
ED
SS
Sco
re
n = 380 707 381 707 280 552 385 709 274 569 230 479 205 462 194 427 174 393
13

?
80:20

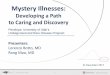
NEDA is a sensitive outcome
1.87
5.29
2.75
2.92
3.41
1.64
2.29
0 1 2 3 4 5 6
Dimethyl fumarate (DEFINE)
Natalizumab (AFFIRM)
Cladribine (CLARITY)
Fingolimod (FREEDOMS)
sc IFN β-1a (DoF)
Teriflunomide (TEMSO)
Alemtuzumab (CARE MS II)
Increase in proportion of NEDA patients relative to comparator
Patients with RRMS over 2 years. Increase in proportion of patients with NEDA versus placebo (except CARE MS II)
All data from post hoc analyses of randomized controlled trials in patients with RRMS. Table adapted from Bevan CJ and Cree BA. JAMA Neurol 2014;71:269-70, with the exception of: TEMSO. Freedman et al. Neurology 2012;78 [Meeting
Abstract s 1]: PD5.007; sc IFN b1-a sc. Data on file; CARE MS II. Coles AJ et al. Lancet 2012;380:1829-39
versus sc IFN b-1a
Slide courtesy Prof. Mark Freedman, EFNS-ENS Istanbul 2014

Relapses
Unreported relapses
Clinical disease progression
Subclinical relapses: focal MRI activity
Focal gray and white matter lesions not detected by MRI
Brain atrophy
Spinal fluid neurofilament levels
MS Iceberg
Clinical activity
Focal MRI activity
Hidden focal and diffuse MRI activity
Microscopic or biochemical pathology
Biomarkers

Control Multiple sclerosis
Slide courtesy of Dr Klaus Schmierer

Brain atrophy occurs across all stages of the disease
De Stefano, et al. Neurology 2010
n= 963 MSers

Association of MRI metrics and cognitive impairment in radiologically isolated syndromes
Amato et al. Neurology. 2012 Jan 31;78(5):309-14.

Treatment effect on disability predicted by effect on T2-lesion load and brain atrophy
Meta-analysis of treatment effect on EDSS worsening (y) vs effects on MRI lesions
and brain atrophy, individually or combined, in 13 placebo-controlled RRMS trials
(13,500 patients)
Sormani MP et al. Ann Neurol. 2014;75:43-49.

• Post-hoc analysis of a pivotal clinical trial of IFN β-1a IM1
• Treatment with IFN β-1a IM resulted in a 55% reduction in brain atrophy vs. placebo during the second year of a clinical trial (N = 140)
• Analysis of the MRI cohort of the European IFN β-1a IM dose comparison study2
• Derived from a double-dose study; all patients on-treatment; modelled from pre-treatment rate
IFN β-1a IM
BPF, brain parenchymal fraction; IFN β, beta-interferon; IM, intramuscular; MRI, magnetic resonance imaging; n.s., not significant. 1. Rudick RA, et al. Neurology 1999; 53:1698−1704; 2. Hardmeier M, et al. Neurology 2005; 64:236−240.
–1.06% per year
–0.33% per year
Treatment initiation
Month
0.795
0.800
0.805
0.810
0.815
0.820
0.825
0.830
–3 0 3 6 9 12 18 24 30 36 21 15 27 33
BP
F
p < 0.01
n.s.
Year 1
Year 2
Year 3
Month 4−12
Baseline− Month 4
p < 0.05
p < 0.01
n.s.
–1.6
–1.4
–1.2
–1.0
–0.8
–0.6
–0.4
0.0
–0.2
Annual MRI group (n = 368)
Frequent MRI subgroup (n = 138)
Re
lati
ve B
PF
chan
ge (
%)
–0.482% (+/ –0.58)
–0.228% (+/ –0.73)
–0.348% (+/ –0.61)
–0.393% (+/ –0.58)
–0.686% (+/-0.79)
–0.377% (+/-0.77)
–0.378% (+/-0.73)

TEMSO: 2-year, randomized, placebo-controlled Phase III trial of teriflunomide in patients with RMS (N = 1,088)
Change from baseline in white matter volume
Teriflunomide: white matter atrophy
RMS, relapsing MS. Wolinsky JS, et al. Mult Scler 2013; 19:1310−1319.
• Whole brain atrophy: − no significant effect
• Grey matter atrophy:
− no significant effect
Me
an ±
SE
chan
ge
fro
m b
ase
line
(m
l)
Week
Placebo Teriflunomide 7 mg Teriflunomide 14 mg
2.4
0.8
–0.8
–2.4
–4.0
–5.6
0 24 48 72 108
p = 0.0002
p = 0.0609
No. of patients
Placebo 358 329 309 270 256
7 mg 359 339 301 273 262
14 mg 355 328 293 273 260

Dimethyl fumarate
DEFINE: 2-year, randomized, placebo-controlled study of DMF in patients with RRMS (N = 1,237)1
CONFIRM: 2-year, randomized, placebo-controlled active reference (GA) comparator study of DMF in patients with RRMS (N = 1,430)2
BID, twice daily; DMF, dimethyl fumarate; TID, three times daily. 1. Arnold DL, et al. AAN 2012. Abstract IN3-2.002; 2. Miller D, et al. ENS 2012. O259.
Week 24−Year 2
−30% vs. placebo (p = 0.02)
−17% vs. placebo (p = 0.2478)
• Significant reduction in brain volume loss vs. placebo with DMF BID but not TID
• No significant reduction in brain volume loss vs. placebo with both doses
−6% vs. placebo
(p = 0.831)
−3% vs. placebo
(p = 0.562)
−16% vs. placebo
(p = 0.706)
Week 24−Year 2
Me
dia
n c
han
ge
in w
ho
le b
rain
vo
lum
e (
%)
Me
dia
n c
han
ge
in w
ho
le b
rain
vo
lum
e (
%)

-1.0%
-0.8%
-0.6%
-0.4%
-0.2%
0.0% Years 0-2
-0.82%
-0.80%
P=0.822†
Placebo (N=315) Natalizumab (N=627)
Year 0-1* Year 1-2
-0.40%
-0.56%
-0.43%
-0.24%
P=0.004†
P=0.002†
†Difference between treatments; ‡Change from baseline; Miller DH et al. Neurology 2007;68:1390-1401.
AFFIRM Study: natalizumab and brain atrophy
Mean
(S
E)
perc
en
tag
e c
han
ge i
n B
PF

Brain atrophy in natalizumab-treated patients: 3-year follow-up
Sastre-Garriga et al. MSJ 2014.
-0.6%
-1.4%
-0.1% -0.5%
-0.7%
-0.2%

Reduction in brain atrophy on alemtuzumab

• In all three studies: PBVC assessed for all patients, prospectively, using the SIENA method • Fingolimod significantly reduced brain volume loss over 2 years vs. placebo
• These reductions were observed after 6 months (first post-baseline scan) • Fingolimod significantly reduced brain volume loss over 1 year vs. IFN β-1a IM
Atrophy data from three fingolimod trials
SIENA, Structural Image Evaluation, using Normalisation, of Atrophy. ITT population with evaluable MRI images at baseline and end of core study phase (Month 24). p values are for comparisons over Months 0–6, Months 0–12, Months 0–24. TRANSFORMS: *** p < 0.001 vs. IFN β-1a IM. Wilcoxon rank sum test; FREEDOMS/FREEDOMS II: * p < 0.05; ** p < 0.01; *** p < 0.001 vs. placebo. Rank ANCOVA adjusted for treatment, region and baseline normalized brain volume. 1. Cohen JA, et al. N Engl J Med 2010; 362:402–415; 2. Kappos L, et al. N Engl J Med 2010; 362:387–401; 3. Radue EW, et al. ECTRIMS 2012. P724.
Me
an P
BV
C f
rom
bas
elin
e
TRANSFORMS1
Time (months)
−32%
reduction
0.0
–0.4
–0.6
–1.4
–0.2
–0.8
–1.2
–1.0
0 24 12
*** n = 429
n = 431
0.0
–0.4
–0.6
–1.4
–0.2
–0.8
–1.2
–1.0
0 24 12 6
FREEDOMS2
Time (months)
−35%
reduction
*
**
***
n = 357
n = 331
0.0
–0.4
–0.6
–1.4
–0.2
–0.8
–1.2
–1.0
0 24 12 6
FREEDOMS II3
Time (months)
−33%
reduction
* ***
*** n = 358
n = 355
Placebo Fingolimod 0.5 mg IFN β-1a IM

• For all annual BVL thresholds, significantly more NEDA-4 patients were in the fingolimod-treated group than in the placebo group
Results: NEDA-4 by Annual BVL Thresholds
aORs were derived from logistic regression of freedom from disease activity on treatment.
Kappos et al. ACTRIMS/ECTRIMS 2014. FC1.5
80% of subjects fail treatment on this criteria

Overview DMTs and brain atrophy
IV, intravenous.
Therapy Administration Reduction in PBVC
IFN β/GA SC IM
IFN β-1a IM: positive effect Year 2
Teriflunomide Oral Not significant
DMF Oral −30% (for BID in DEFINE); not significant for TID Not significant for both doses in CONFIRM
Fingolimod Oral –35% (FREEDOMS); –33% (FREEDOMS II); –32% (TRANSFORMS)
Natalizumab IV Significant in year 2
Alemtuzumab IV –42% (naive vs. IFN); –24% (previously treated vs. IFN)

Residual deficits: • Walking distance >500m
• Unable to run
• Exercise induces intermittent
sensory symptoms in L arm
• Mild urinary frequency
17-yr girl, myelitis
Jun-2000
1st-yr University
L-optic neuritis
Feb-2001
clumsy
left hand
Jan -2002
pins & needles
in legs
Oct-2003
R optic neuritis
Mar-2004
Brainstem
syndrome;
diplopia and
ataxia
Dec 2007
Cervical cord
relapse
weak L arm
with pain
Jan 2008
Bladder
dysfunction
depression,
anxiety and
fatigue
Reduced
mobility
Mild urinary frequency
No depression ,anxiety
or fatigue
Fully mobile
NEDA (no evident disease activity)
Feb-2008 to May-2014
IFN-beta
Feb-2001
Natalizumab
Jan-2008
ED
SS
IFN-beta Natalizumab Jun-2000 May-2014
6.0
3.5 3.5

MRI – progressive brain atrophy
Dec 2007 Jul 2010 Jul 2013
Is this patient in long-term remission?

No evidence of disease activity: NEDA-4
Gd, gadolinium. 1. Havrdova E, et al. Lancet Neurol 2009; 8:254–260; 2. Giovannoni G, et al. Lancet Neurol 2011; 10:329–337.
Treat-2-target
No evidence of disease activity defined as:1,2
× No relapses
× No sustained disability progression
× No MRI activity
× No new or enlarging T2 lesions
× No Gd-enhancing lesions
How do we add a brain atrophy metric to our definition of NEDA?
Normalisation of brain atrophy rates

Other discriminators
1. Safety (risk:benefit)
2. Tolerability
3. Adherence
4. Monitoring
5. Pregnancy
6. Regional / Cultural influences
7. Cost
8. Marketing

T2T-NEDA-ZeTo
T2T = treating-to-target; NEDA = no evident disease activity; ZeTo = zero tolerance
Choose therapy
A B C
Define the individual’s MS
Treatment failure?
• Patient’s preferences? • Your choice?
Individual measures: • Evidence of disease activity? • Tolerability/safety? • Adherence? • Drug or inhibitory markers? • NABs
Monitoring
• MS prognosis • Life style and goals • Shared goals for therapy
Rebaseline
Rebaseline: • IFNβ, natalizumab, fingolimod,
teriflunomide, DMF=3-6 months • Glatiramer acetate=9 months • Alemtuzumab=24 months
DMF, dimethyl fumarate.
Choose a therapeutic strategy
Maintenance-escalation Induction
Choose therapy
X Z
Rebaseline
Monitoring
Initiate or Switch or Escalate Rx Complete course / Re-treat
Breakthrough disease
Y
• Patient’s preferences? • Your choice?
No Yes Yes
• Only one licensed induction therapy at present

Choosing a therapeutic strategy
Maintenance therapies
• Continuous treatment
• Low to very high efficacy
• Reversible
• Perceived to be lower risk
• Examples • Laquinimod, GA, IFN-beta, teriflunomide, BG12,
fingolimod, natalizumab, daclizumab
• Breakthrough disease • Suboptimal or failure to respond
• NEDA reliable metric for efficacy
• Rebound activity • Highly likely
• Can be life threatening
• Pregnancy • Contra-indicated
• No potential for a cure • Rebound
• SPMS & progressive brain atrophy
Induction therapies
• Short-courses or pulsed therapy
• Very high efficacy
• Irreversible
• Perceived to be higher risk
• Examples • Mitoxantrone, cladribine, alemtuzumab, anti-
CD20 (?), BMT
• Breakthrough disease • Marker for retreatment
• NEDA unreliable to assess efficacy
• Rebound activity • Less likely
• Unlikely to be life-threatening
• Pregnancy • Strategy of choice
• Potentially curative • 15-20 year experiment
• BMT, alemtuzumab, cladribine

T2T-NEDA-ZeTo
T2T = treating-to-target; NEDA = no evident disease activity; ZeTo = zero tolerance
Choose therapy
A B C
Define the individual’s MS
Treatment failure?
• Patient’s preferences? • Your choice?
Individual measures: • Evidence of disease activity? • Tolerability/safety? • Adherence? • Drug or inhibitory markers? • NABs
Monitoring
• MS prognosis • Life style and goals • Shared goals for therapy
Rebaseline
Rebaseline: • IFNβ, natalizumab, fingolimod,
teriflunomide, DMF=3-6 months • Glatiramer acetate=9 months • Alemtuzumab=24 months
DMF, dimethyl fumarate.
Choose a therapeutic strategy
Maintenance-escalation Induction
Choose therapy
X Z
Rebaseline
Monitoring
Initiate or Switch or Escalate Rx Complete course / Re-treat
Breakthrough disease
Y
• Patient’s preferences? • Your choice?
No Yes Yes
• Only one licensed induction therapy at present

IFNbeta
GA
Teri
DMF
Treatment Ladder
DMF
Fingo
Nz Az

Time is brain
Natural course of disease
Later intervention
Later treatment
Treatment at diagnosis Intervention
at diagnosis
Time Disease Onset
Dis
abili
ty
Time is brain

Escalation to natalizumab is more effective than switching between IFN/GA
0
25
50
75
100
% P
ati
en
ts
Escalate to Natalizumab, n=106
Switch Between IFN/GA, n=161
Data from a postmarketing, prospective, observational study in 285 RRMS patients for whom treatment with IFNβ or GA therapy failed.
After failure of IFNβ or GA therapy, patients were switched to either natalizumab (n=106) or IFNβ/GA (n=161).
*There were no differences at 12 month between the two groups in proportions of patients free from relapse, disability progression, MRI
activity, and combined activity.
Prosperini L et al. Mult Scler. 2012;18:64-71.
No EDSS
Progression
No MRI
Activity
Disease
Activity Free
P<0.0001 P=0.0003 P<0.0001
51
36
51
21
83
67 77
59
No
Relapses
P<0.0045
Over 24 months*

65.4
87.3
52.9
32.2
46.7
78.9
31.5
13.6 0
25
50
75
100
Relapse-Free SAD-Free (6-month) MRI Activity-Free MS Disease Activity-Free
Alemtuzumab 12 mg
SC IFNβ-1a 44 μg
Escalation to Alemtuzumab Is More Effective Than Switching from IFN/GA to IFNβ-1a 3×/Week
OR=odds ratio; SC=subcutaneous; SAD=sustained accumulation of disability.
Hartung HP et al. Presented at AAN; March 16–23, 2013; San Diego, CA. P07.093.
% o
f P
ati
en
ts
CARE-MS II: Disease-Free Status over 2 Years
OR=3.03
P<0.0001
CO-CZ-0056l

Real-world comparative effectiveness of Fingolimod and Interferon/Glatiramer therapies in a switch population using
propensity-matched data from MSBase
p=0.019
0.00
0.25
0.50
0.75
1.00
Pro
porti
on o
f pat
ient
s N
OT
rela
psed
0 2 4 6 8 10 12Months since baseline
FINGOLIMOD IFN_COP
Time to first relapse on treatment by treatment arm within first 12 months of switch
p=0.000007
0.00
0.25
0.50
0.75
1.00
Prop
ortio
n of
pat
ient
s N
OT
disc
ontin
ued
0 2 4 6 8 10 12Months since baseline
FINGOLIMOD IFN_COP
Time to treatment discontinuation by treatment arm within first 12 months of switch
Mul t ip le Sc le ros is da taBase Spelman et al. ECTRIMS 2013
Conclusions: In general once on 1st-line/lower-tier therapy

TOP: earlier natalizumab treatment favours annualised relapse rate outcomes
P values from a negative binomial regression model adjusted for gender, baseline EDSS score (<3.0 vs ≥3.0l), relapse status in the prior
year (≤1 vs >1), prior DMT use (<3 vs ≥3), disease duration (<8 vs ≥8 years), and treatment duration (≥3 vs <3 years), except for the factor
of interest. Error bars represent 95% CIs.
DMT=disease-modifying therapy; CI=confidence interval.
Wiendl et al. Presented at ENS; June 8–11, 2013; Barcelona, Spain,. P372.

NEDA outcomes with alemtuzumab: 3-year follow-up of the CARE-MS studies
MRI, magnetic resonance image; CI, confidence interval.
Adapted from Havrdova E et al. Presented on ACTRIMS/ECTRIMS, 2014, FC1.4.
38 46 50
67 64
0
20
40
60
80
100
Year 1 Year 2 Year 3
Pro
po
rtio
n o
f
pati
en
ts, %
(9
5%
CI)
↑32.2% P=0.0062
↑45.8% P<0.0001
CARE-MS I: NEDA by year
SC IFNB-1a
ALEM 12 mg
174
369
170
356
—
349
SC IFNB-1a
ALEM 12 mg
187
405
173
434
—
393
27 31
44
56 55
0
20
40
60
80
100
Year 1 Year 2 Year 3
Pro
po
rtio
n o
f
pa
tie
nts
, %
(9
5%
CI)
↑61.2% P<0.0001
CARE-MS II: NEDA by year
↑84.3% P<0.0001

ECTRIMS 2013

ECTRIMS 2013

ECTRIMS 2013

ECTRIMS 2013

TEMSO & TOWER: Evaluation of the Effect of Teriflunomide in Subgroups Defined by Prior Treatment (Pooled Analyses)
Adjusted ARR by Prior Treatment Disability Progression by Prior Treatment
ARR, annualized relapse rate; DMT, disease-modifying therapy; RRMS, relapsing-remitting MS. Adapted from Freedman M et al. Presented on ACTRIMS/ECTRIMS, 2014, P046.
An
nu
aliz
ed r
elap
se r
ate
Pro
bab
ility
of
d
isab
ility
pro
gres
sio
n
0.423 0.464 0.303 0.463 0.536 0.329 0.794 0.641 0.472 0.0
0.2
0.4
0.6
0.8
1.0
>1 Prior DMT 1 Prior DMT No Prior DMT
0.072 0.201 0.178 0.218 0.345 0.176 0.298 0.299 0.238 0.0
0.1
0.2
0.3
0.4
>1 Prior DMT 1 Prior DMT No Prior DMT
Teriflunomide 14 mg Teriflunomide 7 mg Placebo
46.7%
41.6% 27.7%
16.4% 35.9%
30.2%
78.6%
33.4%
46.6%
5.0%
17.4%
20.8%
Patients (n) 41 32 36 189 193 192 498 547 523 Patients (n) 41 32 36 189 193 192 498 547 523
Post hoc analysis of pooled data of ARR and 12-week confirmed disability progression conducted on patient subgroups defined by prior MS therapy

T2T-NEDA-ZeTo
T2T = treating-to-target; NEDA = no evident disease activity; ZeTo = zero tolerance
Choose therapy
A B C
Define the individual’s MS
Treatment failure?
• Patient’s preferences? • Your choice?
Individual measures: • Evidence of disease activity? • Tolerability/safety? • Adherence? • Drug or inhibitory markers? • NABs
Monitoring
• MS prognosis • Life style and goals • Shared goals for therapy
Rebaseline
Rebaseline: • IFNβ, natalizumab, fingolimod,
teriflunomide, DMF=3-6 months • Glatiramer acetate=9 months • Alemtuzumab=24 months
DMF, dimethyl fumarate.
Choose a therapeutic strategy
Maintenance-escalation Induction
Choose therapy
X Z
Rebaseline
Monitoring
Initiate or Switch or Escalate Rx Complete course / Re-treat
Breakthrough disease
Y
• Patient’s preferences? • Your choice?
No Yes Yes
• Only one licensed induction therapy at present

Natalizumab • Continuous treatment (monthly infusions)
• Very high efficacy; high NEDA rates and significant proportion of treated subjects improve.
• Prevents end-organ damage (reduced brain atrophy yr-2)
• Reversible treatment effect
• Infusion reactions uncommon
• No short-term generalised immunosuppression
• Reduced immune surveillance increases risk of CNS infections; in particular PML if JCV-seropositive
• Breakthrough disease
• Re-baseline at 3-6 months
• Neutralizing antibodies to natalizumab reduce efficacy and cause infusion reactions
• Suboptimal or failure to respond
• NEDA reliable metric for efficacy
• Rebound activity
• Highly likely, can be life threatening
• Pregnancy
• Not recommended, natalizumab crosses placenta and has transient effects in baby
• No secondary autoimmunity
• No obvious secondary malignancy risk
• Monitoring: yes, blood and liver function tests early on, anti-natalizumab antibodies, JCV serology and annual MRI
• No potential for a cure
• Rebound
Alemtuzumab • Short-course pulsed therapy (2-5 annual cycles of treatment)
• Very high efficacy; significant proportion of treated subjects improve. Reported NEDA rates low, but not measured in correct epoch
• Prevents end-organ damage (reduced brain atrophy yr-2)
• Irreversible treatment effect
• Infusion reactions the norm
• Short-term generalised immunosuppression (8-12 weeks post infusion)
• Low risk of CNS and other infections after immune system reconstitution
• Breakthrough disease
• Re-baseline at 24 months
• Antibodies to alemtuzumab are transient and don’t appear to inhibit activity of drug
• Marker for retreatment
• NEDA unreliable to assess efficacy
• Rebound activity
• Less likely, unlikely to be life-threatening
• Pregnancy
• Fine once immune system reconstituted
• Potential for autoantibodies to cross placenta, for example neonatal hyperthyroidism
• Secondary autoimmunity; ~50% of patients with long-term follow-up - mainly thyroid related.
• Potential, but undefined, secondary malignancy risk
• Monitoring: yes, monthly blood and urine tests for secondary autoimmunity and annual MRI
• Potentially curative
• Long-term remission established in about 50% of treated patients
• Ongoing 15-20 year experiment, analogous to BMT

NEDA is a sensitive outcome
1.87
5.29
2.75
2.92
3.41
1.64
2.29
0 1 2 3 4 5 6
Dimethyl fumarate (DEFINE)
Natalizumab (AFFIRM)
Cladribine (CLARITY)
Fingolimod (FREEDOMS)
sc IFN β-1a (DoF)
Teriflunomide (TEMSO)
Alemtuzumab (CARE MS II)
Increase in proportion of NEDA patients relative to comparator
Patients with RRMS over 2 years. Increase in proportion of patients with NEDA versus placebo (except CARE MS II)
All data from post hoc analyses of randomized controlled trials in patients with RRMS. Table adapted from Bevan CJ and Cree BA. JAMA Neurol 2014;71:269-70, with the exception of: TEMSO. Freedman et al. Neurology 2012;78 [Meeting
Abstract s 1]: PD5.007; sc IFN b1-a sc. Data on file; CARE MS II. Coles AJ et al. Lancet 2012;380:1829-39
versus sc IFN b-1a
Slide courtesy Prof. Mark Freedman, EFNS-ENS Istanbul 2014

REBOUND AFTER NATALIZUMAB WITHDRAWAL
Rigau et al. Neurology. 2012 Nov 27;79(22):2214-6.

Case study
Question: “Prof G I have had 33 natalizumab infusions and I have just found out that I am JCV seropositive with an antibody index of 3.2. What should I do?”

PML





17% 85%
“The power of an infographic……less is more.”

>1,000,000 SlideShare views

www.clinicspeak.com

Truer risk of PML = Number or cases of PML
Number of JCV+ve exposed Msers**
Underestimate of the risk of PML
Number or cases of PML
Number of exposed MSers (JCV+ve & JCV-ve)*
=
* Please note this denominator is changing over time with a greater proportion of exposed MSers being JCV-ve; this will have the effect of under-estimating the risk of PML.
** This denominator is also changing over time by getting relatively smaller as the number of JCV+ve MSers stop natalizumab. Despite this this ratio will provide a more accurate estimate of the risk of getting PML.
What is the true PML risk?

Natalizumab Alemtuzumab
Asymptomatic PML? LP-JCV DNA & MRI
Option 1: Immediate switch (high risk if carry-over PML develops)
Natalizumab Alemtuzumab Oral bridging agent (Teriflunomide, DMF or Fingolimod)
Asymptomatic PML? LP-JCV DNA & MRI
Rebaseline MRI
Option 3: Bridging (low risk; mainly related to using a low efficacy bridging agent and using alemtuzumab after the bridging agent)
6-12 MONTHS
Natalizumab Alemtuzumab
Rebaseline MRI **
3-6 MONTH WASHOUT
Asymptomatic PML?* LP-JCV DNA & MRI
Option 2: Washout (intermediate risk; mainly related to rebound of MS disease activity)
* For this option the shorter the washout the more important the screen for asymptomatic PML becomes. ** PML screening and baseline MRI studies are don’t use the same types of scans hence the need for both.
Switching from natalizumab to alemtuzumab


MS disease activity in RESTORE: a randomized 24-week natalizumab treatment interruption study
Fox et al. Neurology 2014;82:1491–1498.

MS disease activity in RESTORE: a randomized 24-week natalizumab treatment interruption study
Fox et al. Neurology 2014;82:1491–1498.

MS disease activity in RESTORE: a randomized 24-week natalizumab treatment interruption study
Fox et al. Neurology 2014;82:1491–1498.

MS disease activity in RESTORE: a randomized 24-week natalizumab treatment interruption study
Fox et al. Neurology 2014;82:1491–1498.

Switching from natalizumab to fingolimod: a randomized, placebo-controlled study of patients with RRMS
Kappos et al. In Press 2014

Switching from natalizumab to fingolimod: a randomized, placebo-controlled study of patients with RRMS
Kappos et al. In Press 2014

Fingolimod after natalizumab and the risk of short-term relapse
Jokubaitis et al. Neurology 2014;82:1204–1211.

Fingolimod after natalizumab and the risk of short-term relapse
Jokubaitis et al. Neurology 2014;82:1204–1211.

Fingolimod after natalizumab and the risk of short-term relapse
Jokubaitis et al. Neurology 2014;82:1204–1211.

ACTRIMS-ECTRIMS 2014

ACTRIMS-ECTRIMS 2014

Fingolimod Alemtuzumab
Only treat with alemtuzumab once lymphocyte counts normalize*
2 to 6 12 MONTH WASHOUT
Option 2: Washout (intermediate risk; mainly related to rebound of MS disease activity)
* What constitutes a normal level post-fingolimod needs to be defined; I would be reluctant to give alemtuzumab to anyone with a total lymphocyte count below 1.0x109 .
Fingolimod Alemtuzumab
Option 1: Immediate switch (high-risk if persistent lymphopaenia occurs)
Treat with alemtuzumab before lymphocyte counts normalize
Fingolimod Alemtuzumab Bridging agent (IFN-beta, GA, Teriflunomide or DMF)
Only treat with alemtuzumab once lymphocyte counts normalize*
Option 3: Bridging (low risk; mainly related to MS rebound as a result of using a low efficacy bridging agent after fingolimod)
3-12 MONTHS
* What constitutes a normal level in this situation needs to be defined; I would be reluctant to give alemtuzumab to anyone with a total lymphocyte count below 1.0x109 .
Switching from fingolimod to alemtuzumab

Reconstitution of circulating lymphocyte counts in FTY720-
treated MS patients
Johnson et al. Clinical Immunology (2010) 137, 15–20

NABs

The incidence and significance of anti-natalizumab antibodies Results from AFFIRM and SENTINEL
Calebresi & Giovannoni, et al. Neurology 2007;69:1391–1403.

Pregnancy

Case Study
• 30 year old woman RRMS diagnosed 2001
• Two relapses, EDSS 1.0
• Started on natalizumab 300mg ivi monthly as part of a clinical trial
• NEDA (no evident disease activity) on natalizumab x 8 years
• Now wants to start a family; would you stop natalizumab?



Case 3
• 30 year old woman RRMS diagnosed 2001
• Two relapses, EDSS 1.0
• Started on natalizumab 300mg ivi monthly as part of a clinical trial
• NEDA (no evident disease activity) on natalizumab x 8 years
• Now wants to start a family; would you stop natalizumab?
• Natalizumab stopped
• Comes in 4 months later with a major spinal cord relapse
• MRI >50 Gd-enhancing lesions in the brain and a large Gd-enhancing lesions in the spinal cord with cord expansion


Considerations for Women of Childbearing Potential
Interferon β • In monkeys, increased rate of abortion. No malformations in
surviving animals
• Initiation of treatment is contraindicated during pregnancy
Glatiramer acetate
• Animal studies are insufficient with respect to effects on pregnancy;
embryonal/foetal development, parturition, and postnatal
development
• Contraindicated during pregnancy
Natalizumab
• Studies in guinea pigs and monkeys showed no evidence of
teratogenic effects or effects on growth of offspring
• Should not be used during pregnancy unless the clinical condition of
the woman requires treatment with natalizumab
Fingolimod
• Animal studies have shown reproductive toxicity, including foetal loss
and teratogenicity
• While on treatment, women should not become pregnant; if
pregnancy occurs, discontinuation of fingolimod is recommended
Animal studies, Clinical recommendations
Data from summary of product of characteristics (SmPC) for each therapy.

Considerations for Women of Child-bearing Potential
Teriflunomide
• Embryotoxic and teratogenic in rats and rabbits at doses in the
human therapeutic range
• Contraindicated in pregnancy
• Patient advised to contact physician if pregnancy is suspected;
institution of accelerated elimination may decrease risk to foetus
Alemtuzumab
• Dosing mice for 5 days during gestation resulted in significant
increases in dead or resorbed conceptuses and reduction in viable
foetuses
• Placental transfer and potential pharmacologic activity observed
• Contraception advised during treatment and for 4 months following
• Should be administered during pregnancy only if the potential benefit
justifies the potential risk to the foetus
• Thyroid disease poses special risks in women who are pregnant
(potential miscarriage, foetal effects such as mental retardation and
dwarfism, transient neonatal Graves’ disease)
Dimethyl fumarate • No malformations have been observed at any dose in rats or rabbits
• Should be used during pregnancy only if clearly needed and if the
potential benefit justifies the potential risk to the foetus
Animal studies, Clinical recommendations
Data from summary of product of characteristics (SmPC) for each therapy.

Conclusion
• DMT landscape is becoming increasingly complex – Changing role of clinical-nurse specialist and MSologist
• New tools are required to engage MSers in treatment decisions – Is not time some treatment algorithms?
• Treat-2-target of NEDA current paradigm – NEDA (zero-tolerance) vs. MEDA
– Expand to include end-organ damage metrics, e.g. BVL (NEDA-4)
• Most sequencing decisions are not evidence-based – scientific rationale
– registries and real-life data
– Head-2-head studies are needed
• Efficacy is not everything don’t forget safety , i.e. the risks and the benefits, tolerability, adherence, monitoring, pregnancy, etc…..
• Evidence-based stopping criteria

Rheumatoid arthritis End-stage joint disease

Questions
Recommended