Sedation For Medically-Compromised
Patients
Is ASA Grading Out-dated?
Dr Yusof (Joe) Omar MBBCh, DA, MRCA, PDD (Pain & Sedation)
Sedationist Senior Teaching Fellow, Eastman CPD, UCL
2016
ASA I A normal healthy patient
ASA II A patient with mild systemic disease
ASA III A patient with severe systemic disease
ASA IV A patient with severe systemic disease
that is a constant threat to life

Mrs X
66years old, retired, smoker, Alcohol 8-10u/w
Lung disease, emhysema, usual Sats 87-89%
Depression, under psychiatrist’s care.
Steroids in the past
Excessive thirst, pt thinks she may have Diabetes.
Drugs: Inhalers only
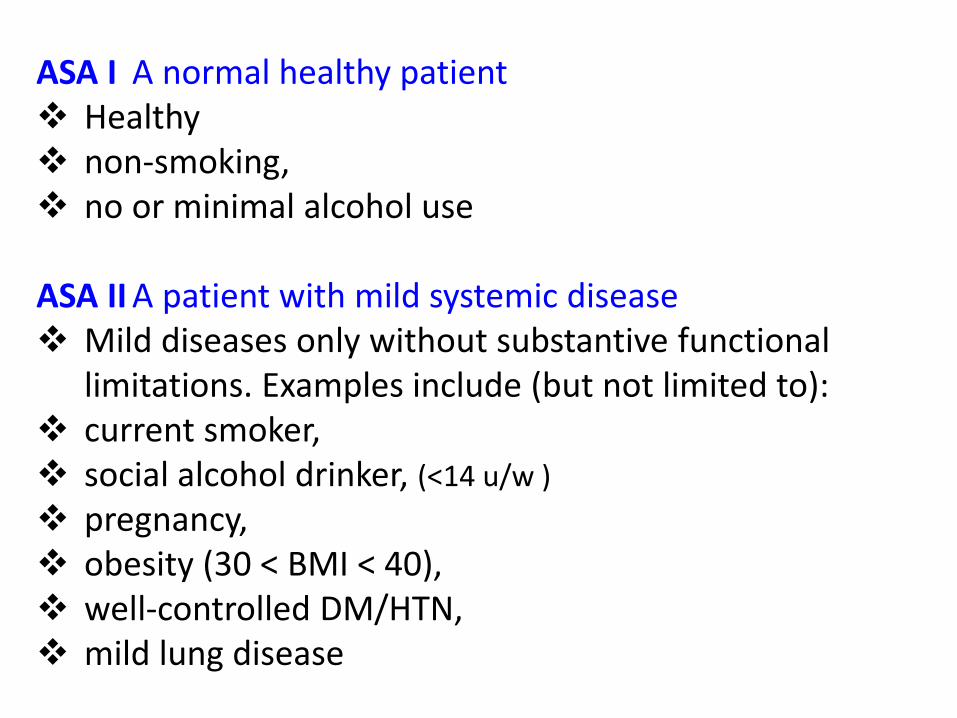
ASA I A normal healthy patient Healthy non-smoking, no or minimal alcohol use ASA II A patient with mild systemic disease Mild diseases only without substantive functional
limitations. Examples include (but not limited to): current smoker, social alcohol drinker, (<14 u/w )
pregnancy, obesity (30 < BMI < 40), well-controlled DM/HTN, mild lung disease
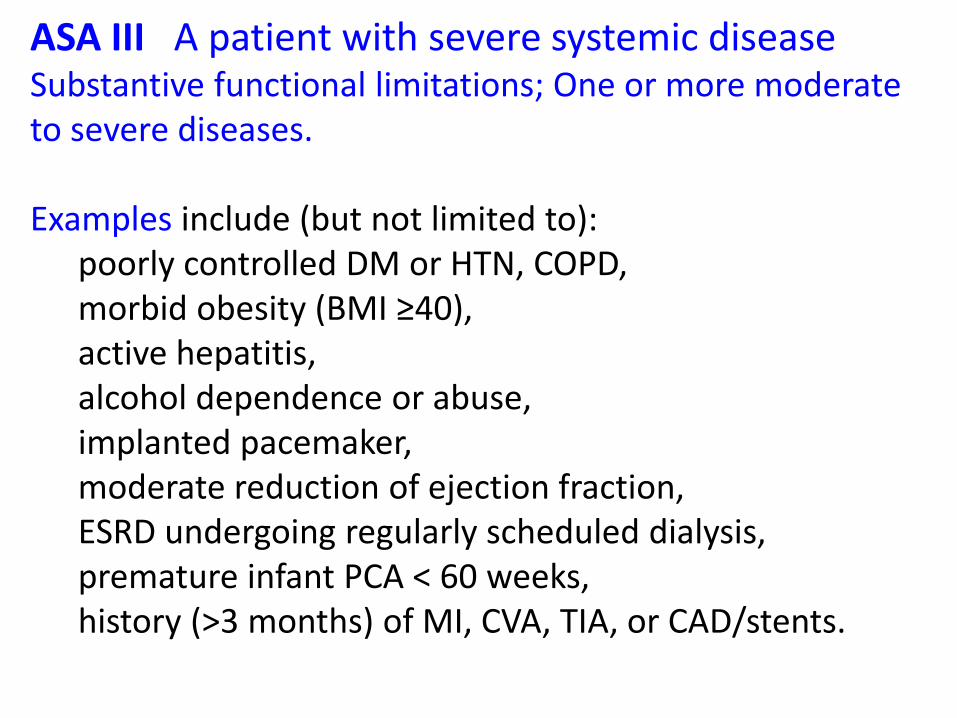
ASA III A patient with severe systemic disease Substantive functional limitations; One or more moderate to severe diseases. Examples include (but not limited to): poorly controlled DM or HTN, COPD, morbid obesity (BMI ≥40), active hepatitis, alcohol dependence or abuse, implanted pacemaker, moderate reduction of ejection fraction, ESRD undergoing regularly scheduled dialysis, premature infant PCA < 60 weeks, history (>3 months) of MI, CVA, TIA, or CAD/stents.
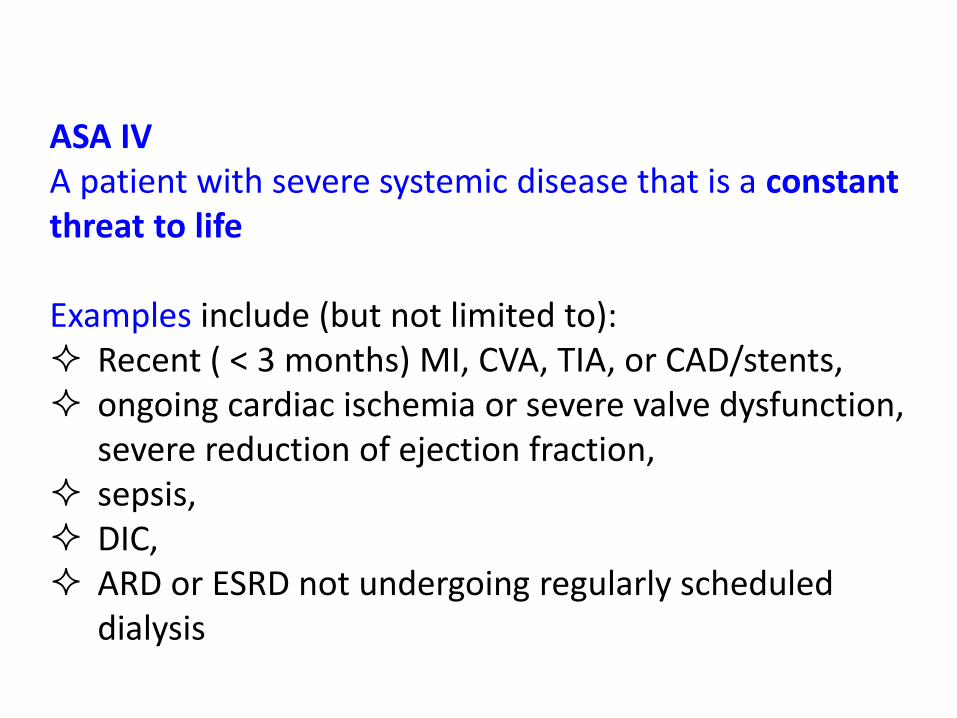
ASA IV A patient with severe systemic disease that is a constant threat to life Examples include (but not limited to): Recent ( < 3 months) MI, CVA, TIA, or CAD/stents, ongoing cardiac ischemia or severe valve dysfunction,
severe reduction of ejection fraction, sepsis, DIC, ARD or ESRD not undergoing regularly scheduled
dialysis
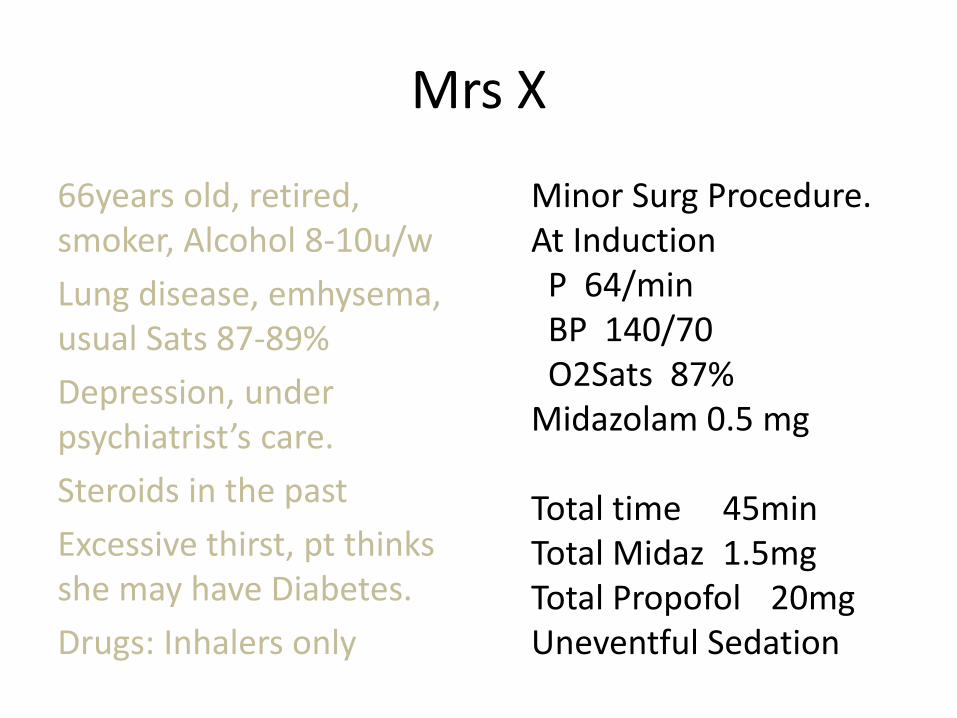
Mrs X
66years old, retired, smoker, Alcohol 8-10u/w
Lung disease, emhysema, usual Sats 87-89%
Depression, under psychiatrist’s care.
Steroids in the past
Excessive thirst, pt thinks she may have Diabetes.
Drugs: Inhalers only
Minor Surg Procedure. At Induction P 64/min BP 140/70 O2Sats 87% Midazolam 0.5 mg Total time 45min Total Midaz 1.5mg Total Propofol 20mg Uneventful Sedation
Mrs X
Escort took Mrs X back to Devon by car, no problems reported.
How many of you would be happy with that?
Mrs X was found dead the next morning.
Did the Sedation contribute towards her Demise
Post Mortem: No cause of death found.
RETIRE NOW
It is a severity-of-disease classification system (Knaus et al., 1985)
APACHE II Acute Physiology and Chronic Health Evaluation II
Is there an Alternative to ASA
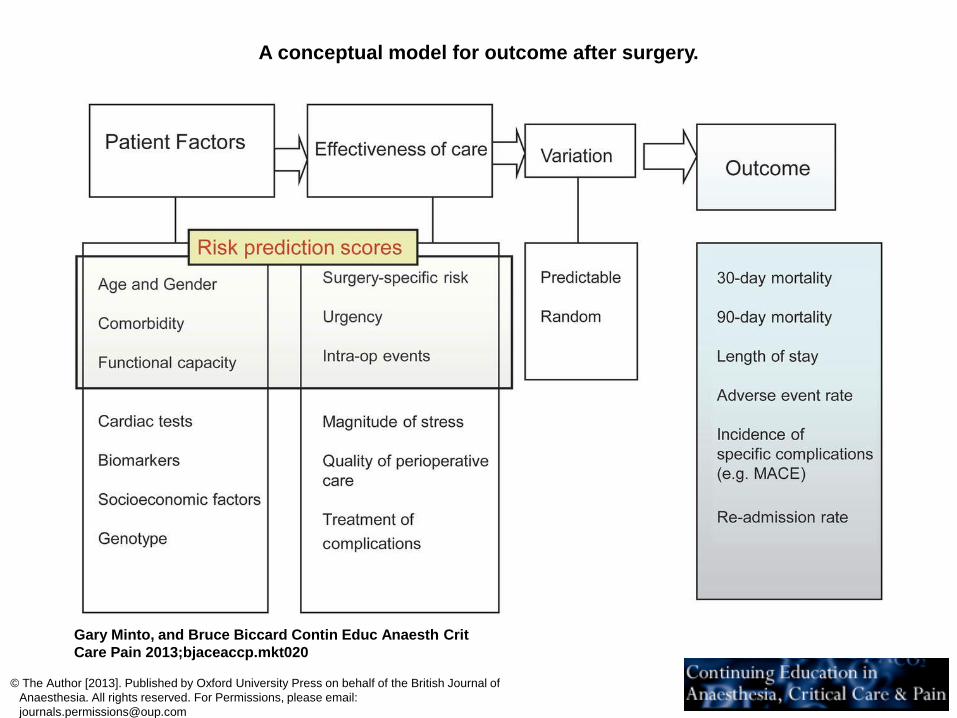
A conceptual model for outcome after surgery.
Gary Minto, and Bruce Biccard Contin Educ Anaesth Crit
Care Pain 2013;bjaceaccp.mkt020
© The Author [2013]. Published by Oxford University Press on behalf of the British Journal of
Anaesthesia. All rights reserved. For Permissions, please email:
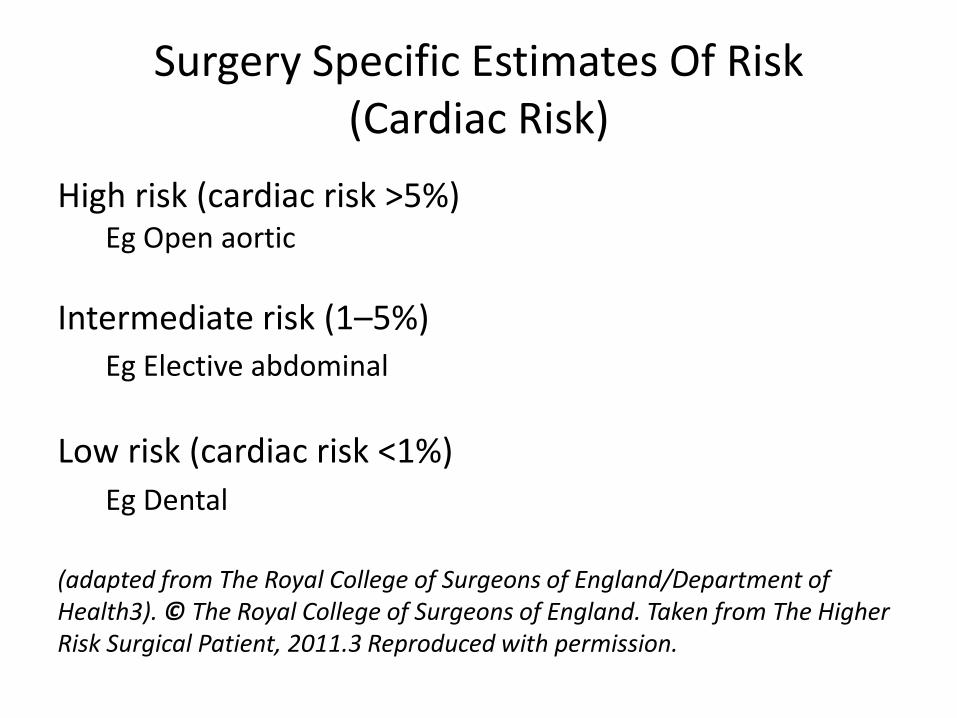
Surgery Specific Estimates Of Risk (Cardiac Risk)
High risk (cardiac risk >5%) Eg Open aortic
Intermediate risk (1–5%) Eg Elective abdominal
Low risk (cardiac risk <1%)
Eg Dental
(adapted from The Royal College of Surgeons of England/Department of Health3). © The Royal College of Surgeons of England. Taken from The Higher Risk Surgical Patient, 2011.3 Reproduced with permission.
Risk Factors in Dental Sedation
• Age
• Fitness
• Fear and anxiety of Pt
• Nature of procedure
• Duration of procedure
• Training of sedationist
• Experience of sedationist
• Gut Feeling
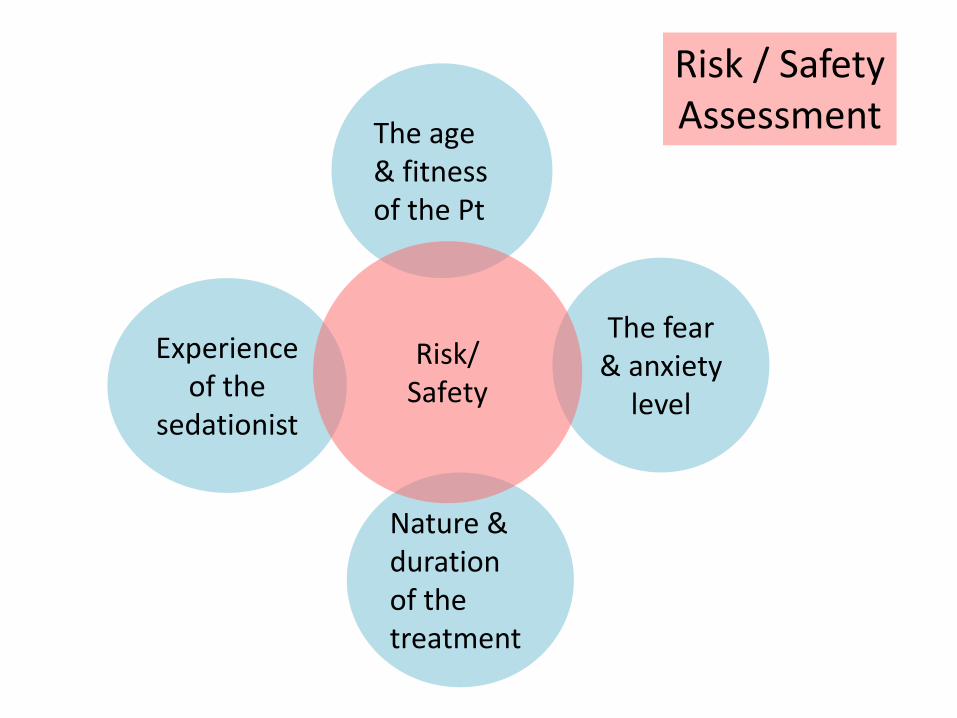
The age & fitness of the Pt
The fear & anxiety
level
Nature & duration of the treatment
Experience of the
sedationist
Risk/ Safety
Risk / Safety Assessment
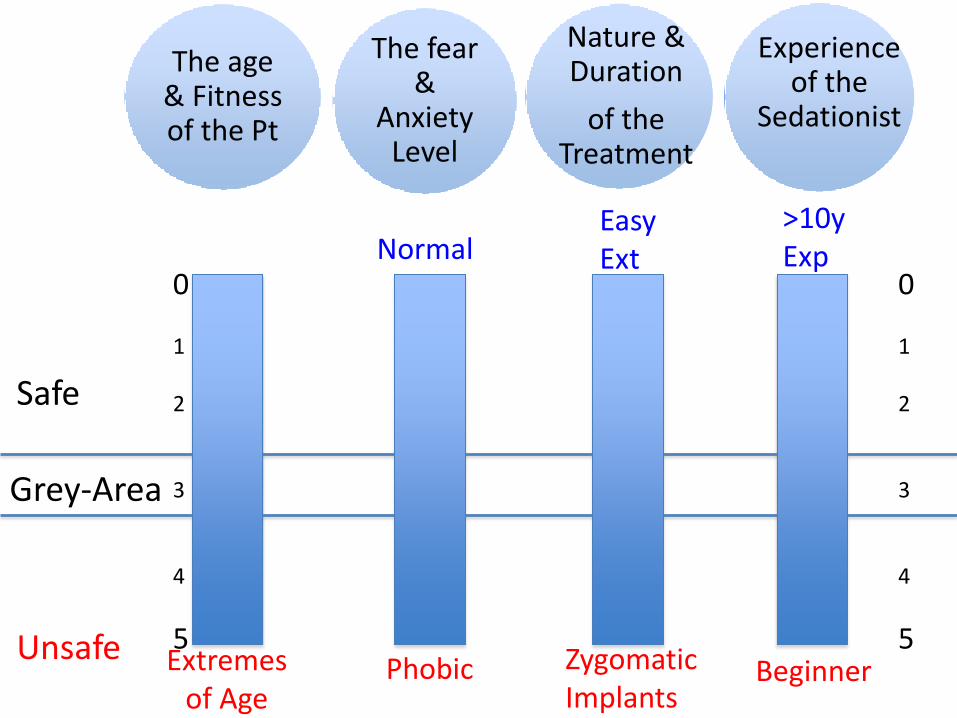
Safe
Unsafe Phobic
Normal
Grey-Area
Easy Ext
Zygomatic Implants
Beginner
>10y Exp
The age & Fitness of the Pt
The fear &
Anxiety Level
Nature & Duration
of the Treatment
Experience of the
Sedationist
0 1 2 3 4
5
0 1 2 3 4
5 Extremes
of Age
Safe
Unsafe Phobic
Normal
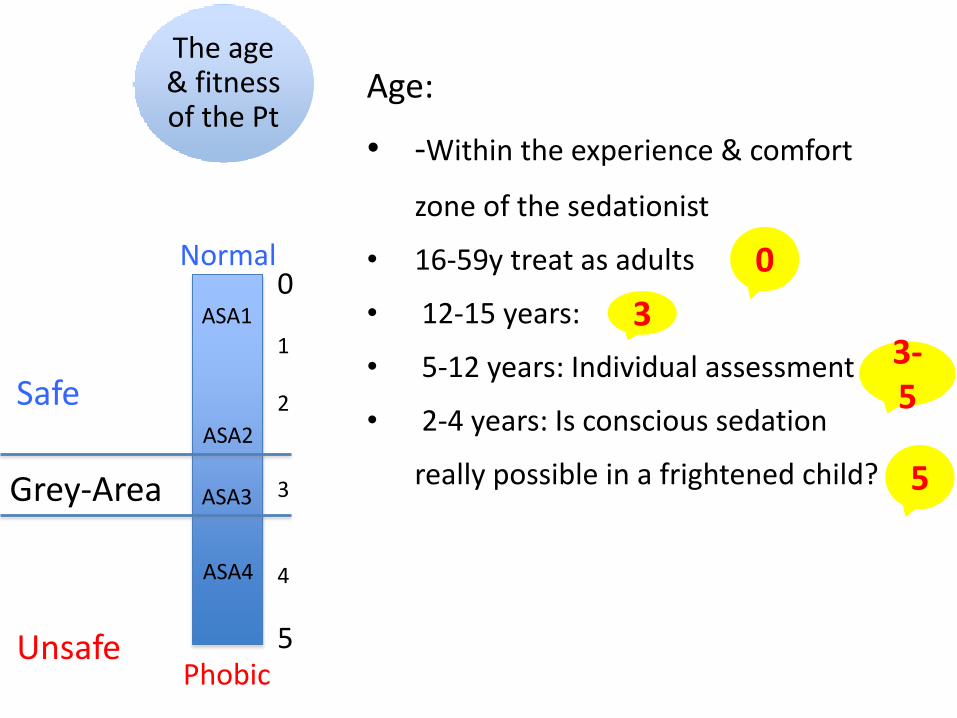
Age:
• -Within the experience & comfort
zone of the sedationist
• 16-59y treat as adults
• 12-15 years:
• 5-12 years: Individual assessment
• 2-4 years: Is conscious sedation
really possible in a frightened child? Grey-Area
The age & fitness of the Pt
0 1 2 3 4
5
ASA2
ASA3
ASA4
ASA1
5
3-5
3
0
Safe
Unsafe ASA 4
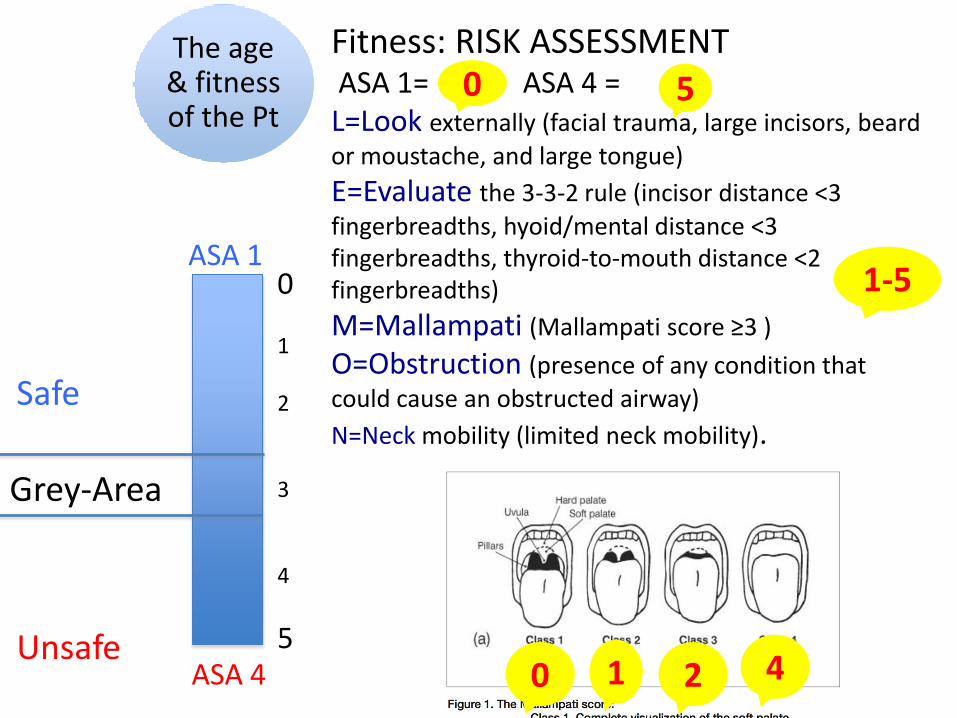
Fitness: RISK ASSESSMENT ASA 1= ASA 4 = L=Look externally (facial trauma, large incisors, beard
or moustache, and large tongue)
E=Evaluate the 3-3-2 rule (incisor distance <3
fingerbreadths, hyoid/mental distance <3 fingerbreadths, thyroid-to-mouth distance <2 fingerbreadths)
M=Mallampati (Mallampati score ≥3 )
O=Obstruction (presence of any condition that
could cause an obstructed airway)
N=Neck mobility (limited neck mobility).
Grey-Area
0 1 2 3 4
5
The age & fitness of the Pt
ASA 1
5
0 1 2 4
1-5
0
Safe
Unsafe
0 1 2 3 4
5
The fear &
anxiety level
Normal
Phobic
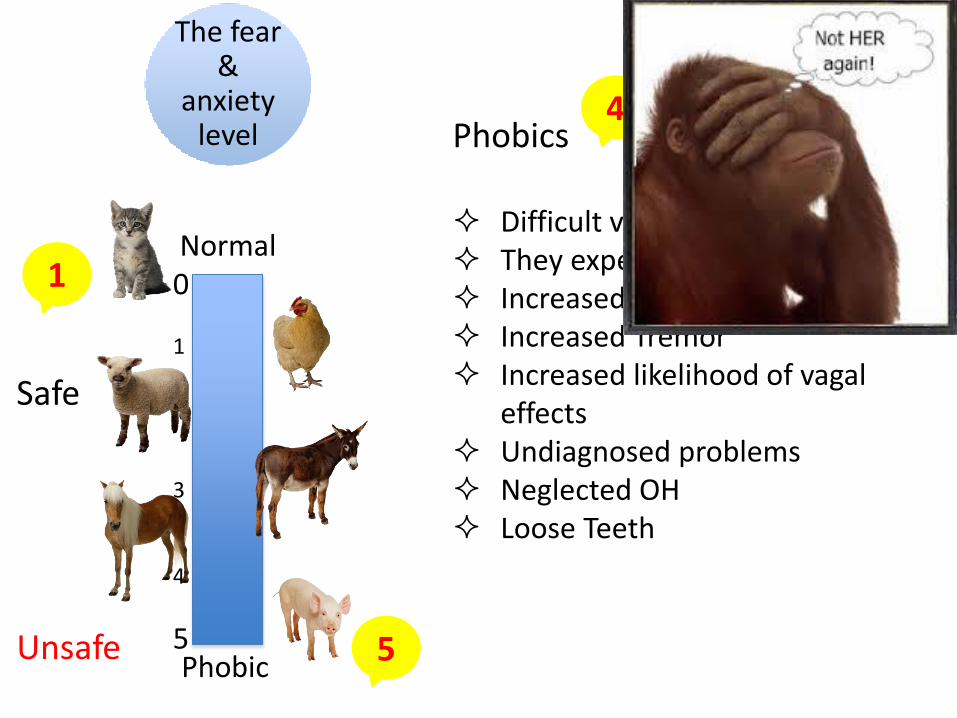
Phobics Difficult venipuncture They expect Oblivion Increased movements Increased Tremor Increased likelihood of vagal
effects Undiagnosed problems Neglected OH Loose Teeth
4
5
1
Safe
Unsafe
0 1 2 3 4
5
Grey-Area
Nature & duration
of the treatment
Easy Ext
Zygomatic Implants
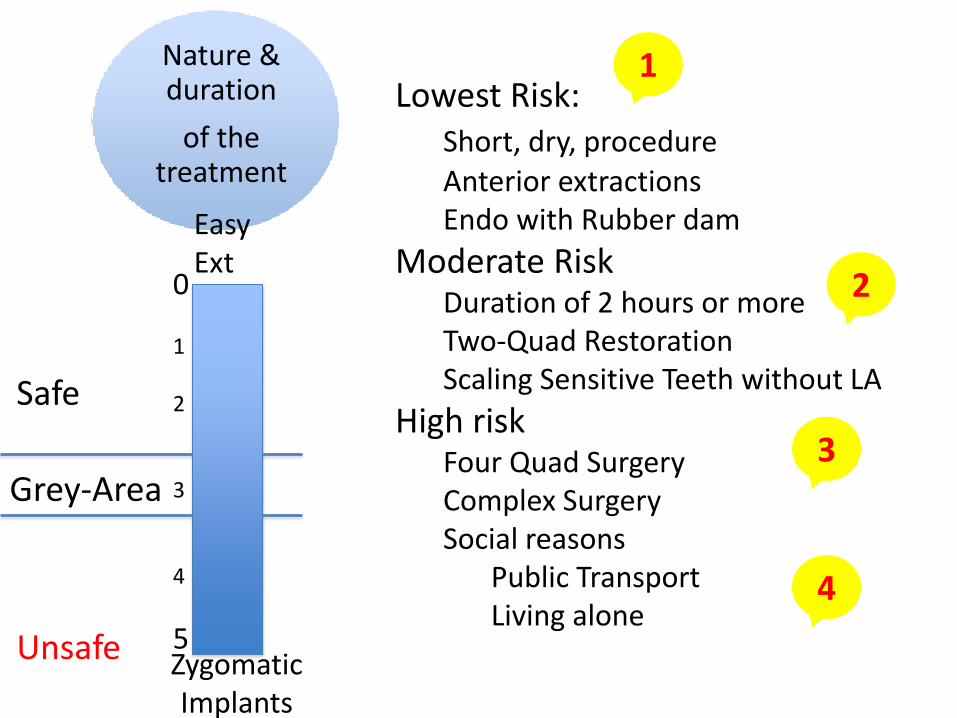
Lowest Risk: Short, dry, procedure Anterior extractions Endo with Rubber dam
Moderate Risk Duration of 2 hours or more Two-Quad Restoration Scaling Sensitive Teeth without LA
High risk Four Quad Surgery Complex Surgery Social reasons Public Transport Living alone
1
2
3
4
Safe
Unsafe
0 1 2 3 4
5
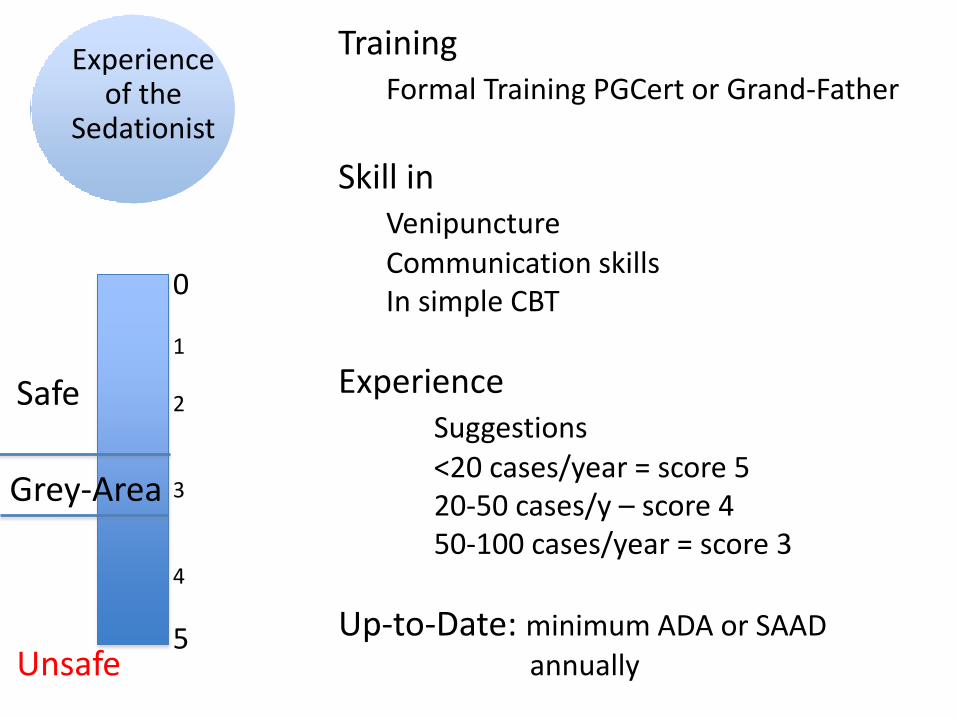
Grey-Area
Experience of the
Sedationist
Training Formal Training PGCert or Grand-Father
Skill in Venipuncture Communication skills In simple CBT
Experience Suggestions <20 cases/year = score 5 20-50 cases/y – score 4 50-100 cases/year = score 3
Up-to-Date: minimum ADA or SAAD annually
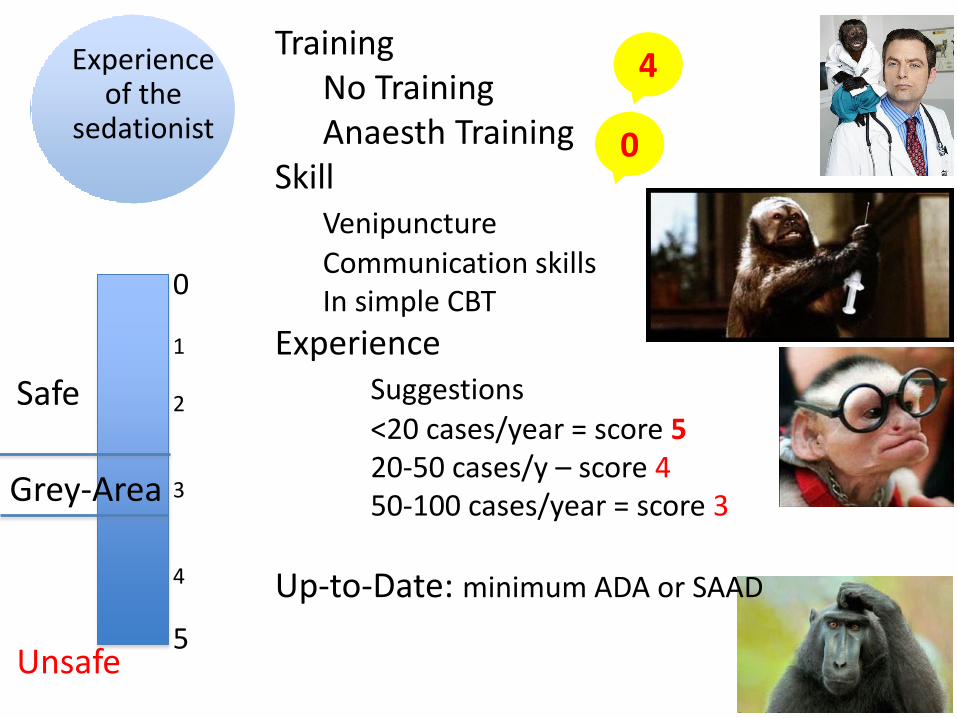
Training No Training Anaesth Training Skill Venipuncture Communication skills In simple CBT
Experience Suggestions <20 cases/year = score 5 20-50 cases/y – score 4 50-100 cases/year = score 3
Up-to-Date: minimum ADA or SAAD
Safe
Unsafe
0 1 2 3 4
5
Grey-Area
Experience of the
sedationist
4
0
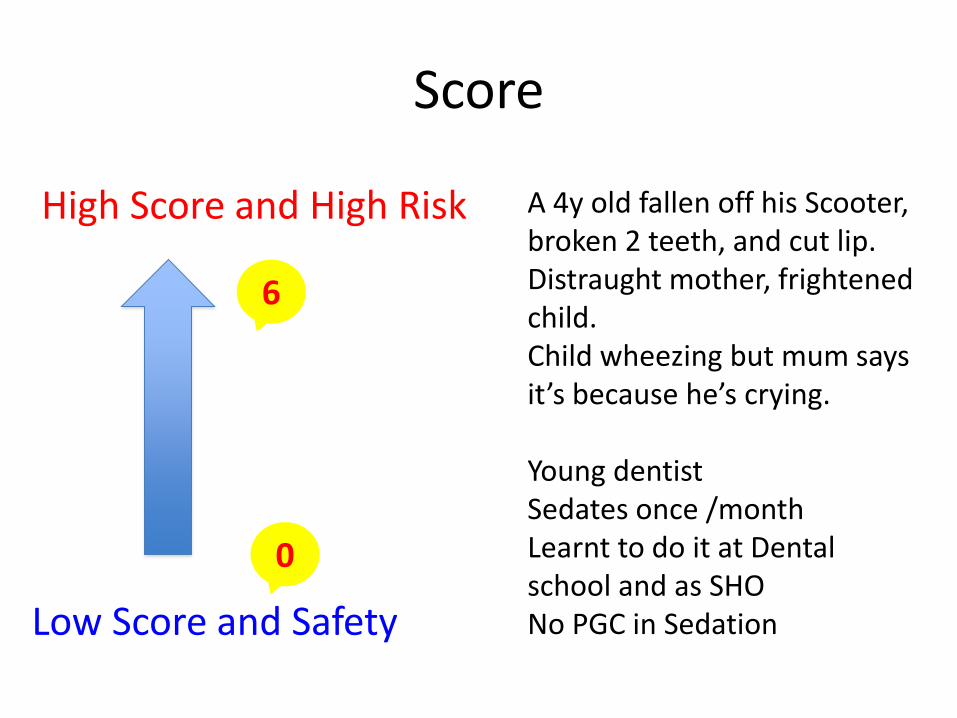
Score
Low Score and Safety
High Score and High Risk
6
0
A 4y old fallen off his Scooter, broken 2 teeth, and cut lip. Distraught mother, frightened child. Child wheezing but mum says it’s because he’s crying. Young dentist Sedates once /month Learnt to do it at Dental school and as SHO No PGC in Sedation
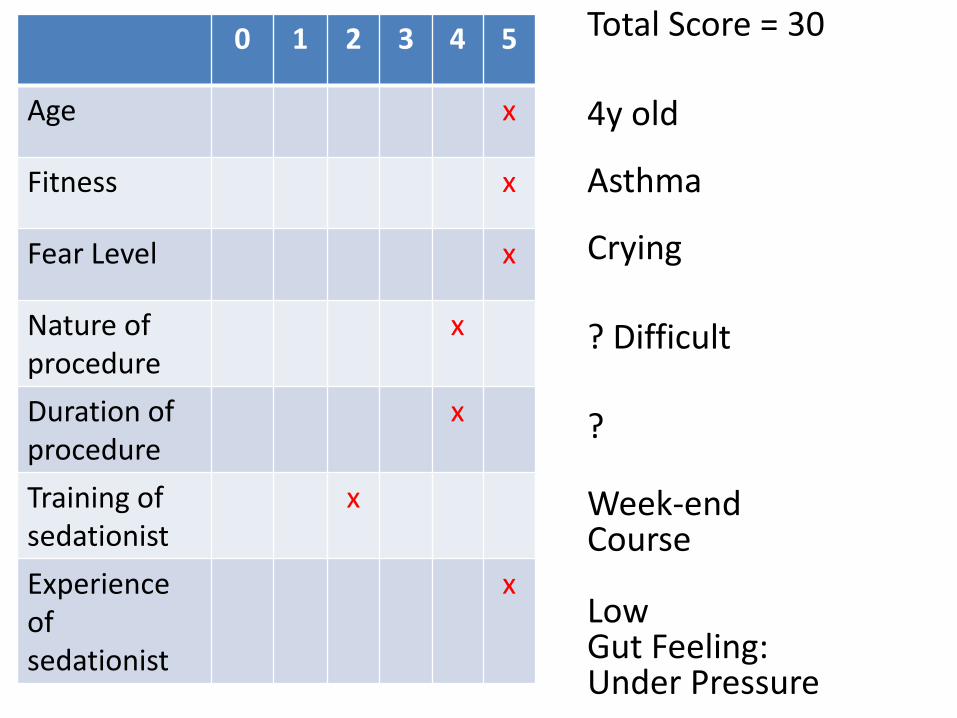
0 1 2 3 4 5
Age x
Fitness x
Fear Level x
Nature of procedure
x
Duration of procedure
x
Training of sedationist
x
Experience of sedationist
x
Total Score = 30 4y old Asthma Crying ? Difficult ? Week-end Course Low Gut Feeling: Under Pressure
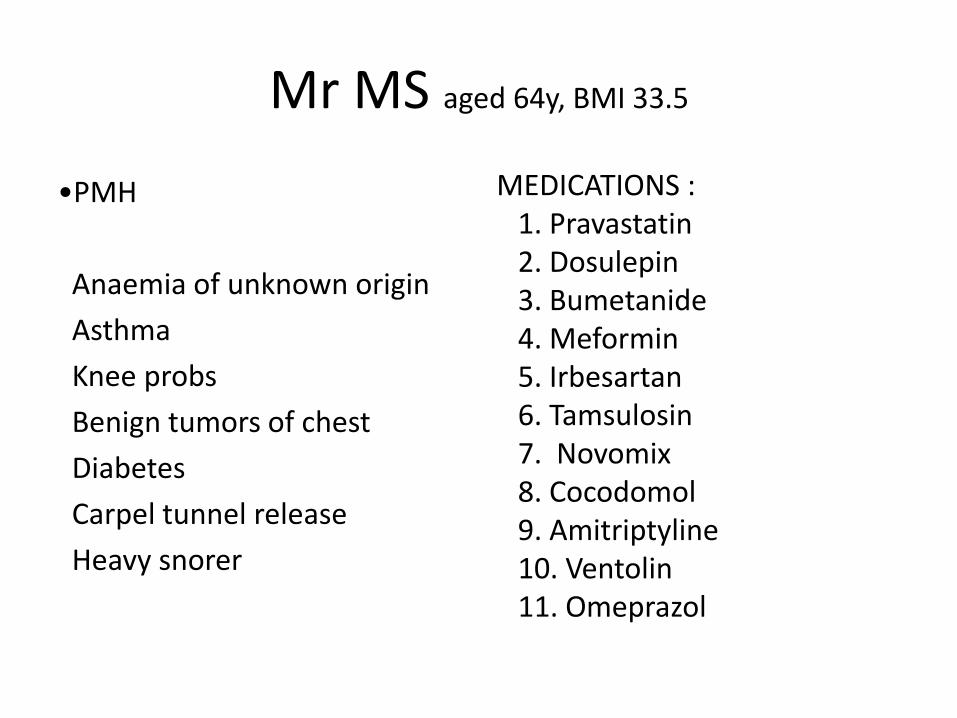
Mr MS aged 64y, BMI 33.5
•PMH
Anaemia of unknown origin
Asthma
Knee probs
Benign tumors of chest
Diabetes
Carpel tunnel release
Heavy snorer
MEDICATIONS : 1. Pravastatin 2. Dosulepin 3. Bumetanide 4. Meformin 5. Irbesartan 6. Tamsulosin 7. Novomix 8. Cocodomol 9. Amitriptyline 10. Ventolin 11. Omeprazol
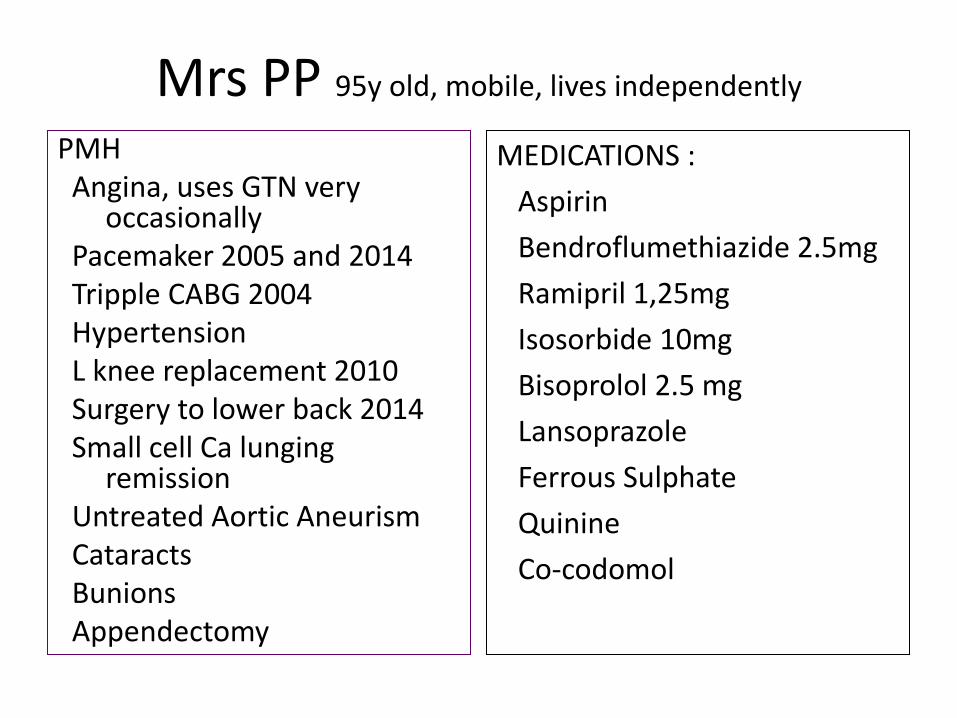
Mrs PP 95y old, mobile, lives independently
PMH Angina, uses GTN very occasionally Pacemaker 2005 and 2014 Tripple CABG 2004 Hypertension L knee replacement 2010 Surgery to lower back 2014 Small cell Ca lunging remission Untreated Aortic Aneurism Cataracts Bunions Appendectomy
MEDICATIONS :
Aspirin
Bendroflumethiazide 2.5mg
Ramipril 1,25mg
Isosorbide 10mg
Bisoprolol 2.5 mg
Lansoprazole
Ferrous Sulphate
Quinine
Co-codomol
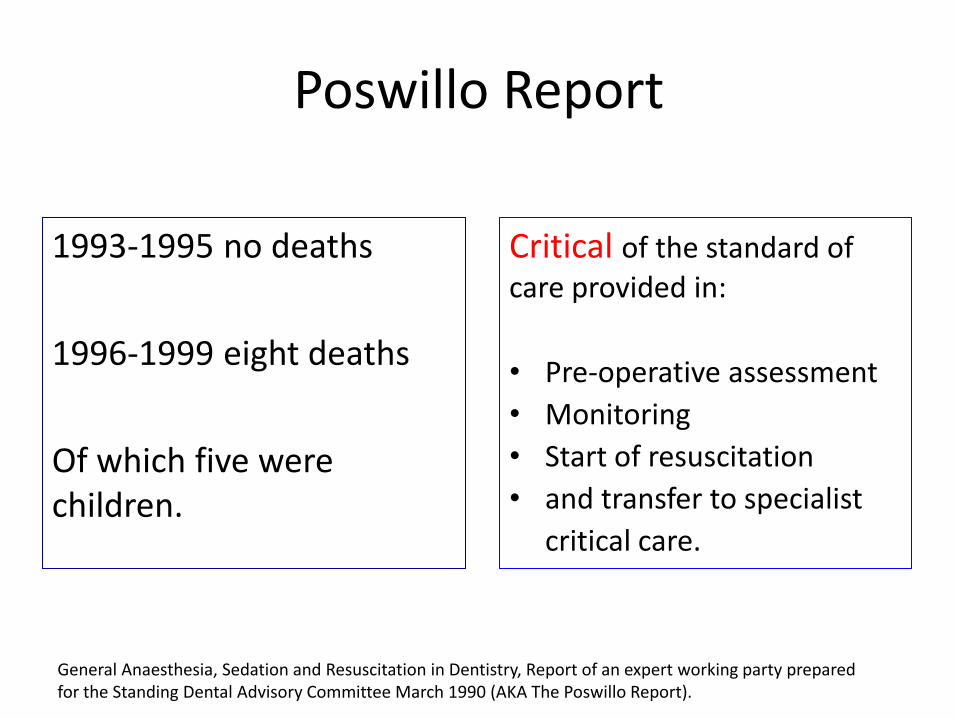
Poswillo Report
1993-1995 no deaths
1996-1999 eight deaths
Of which five were children.
Critical of the standard of care provided in:
• Pre-operative assessment
• Monitoring
• Start of resuscitation
• and transfer to specialist
critical care.
General Anaesthesia, Sedation and Resuscitation in Dentistry, Report of an expert working party prepared for the Standing Dental Advisory Committee March 1990 (AKA The Poswillo Report).
Thank you
THE ULTIMATE IGNORANCE IS THE
REJECTION OF SOMETHING YOU KNOW NOTHING
ABOUT
YET, REFUSE TO INVESTIGATE
Dr Wayne Dyer
Recommended