Rafael Carrion, MDAssociate Professor of Urology
Program DirectorDirector of Research
Saving the Cavernous Spaces after Infection




Dilemma with Conservative Therapy Limited penetration of
oral or systemic antibiotics to area containing the prosthesis– Scar tissue surrounds the
prosthetic parts as a response to walling off a foreign body
– Bacterial Biofilm

Biofilm Biofilms occur when bacteria
and/or other microbes attach to surfaces and surround themselves with protective extracellular polymeric substances (EPS).
Cells communicating with each other, coordinate expression of certain genes, and organizing their activities.
Forming a 'resilient refugia'for bacteria; one that is able to resist natural stressors, and most antimicrobial agents.

Biofilm Bacteria in biofilms can
evolve as a result of starvation or other external pressures.
Significant problem in engineered systems (pipelines) and biomedical processes (e.g. hospital-acquired infections, persistent infections, biofouling of implant devices) (Kraigsleyand Finkley, 2009)

Overview
Modern penile implants provide a predictable/reliable treatment of erectile dysfunction (ED) despite the development of less-invasive therapies. – Patient and partner satisfaction is highest with a
penile implant among all of the treatments for ED
Procedure can be complicated by infection

Incidence Infection associated with penile implants is
– Thought to be due to bacterial colonization during surgery
Infection rates vary from 0.6% to 8.9% for primary procedures
Pre-Coated Implants: Incidence of up to 13.3% associated with revision surgery
Post-Coated Implants: 1.77% infection rate compared with 3.09% infection rate in a control group of non-coated implants
Coated + no-skin-touch group = 0.7%

Offenders Coagulase-negative Staphylococcus comprises 58%
of infections Staphylococcus Lugdunensis, Epidermitis Pseudomonas aeruginosa Serratia marcescens Enterococcus Proteus mirabilis MRSA Candida albicans Bacteroides fragilis

Removal– Then when or if to place implant in the future
Salvage Prosthesis– Malleable– Inflatable
Stimulan
Gross, M; Levine, L; Carrion, R; Eid, J, Martinez, D; Perito, P; Munariz, R. ISSM Abstract #045, Improved Infection outcomes after mulcahy salvageProcedure and replacement of infected IPP with malleable prosthesis.
Choices with a Clinical Penile Prosthetic Infection:

Risk Factors: Comorbidities, Surgical History
3X infection rate in diabetic population
Immunosuppression
Revision surgery
Does this affect your decision for salvage choice?

Consequences
Removal– Negative changes to Morphology– Raises difficulty for future implantation
Salvage Prosthesis– Preserves morphology and erectile function
Stimulan– Preserves morphology– Preserves ease of future implantation

Bio-inert Cast CaSO4
Widely used – Dentistry
– Orthopedics (Osteo-induction)
– Infection Osteomyelitis
Biocompatible material
Completely resorbed following implantation
Does not evoke a significant host response

Cast Content
Addition of Anti-microbial to mixture for local infection treatment
Release of pharmacologic agent from a carrier isdirectly proportional to dissolution of the CaSO4 ( Based on experimental calculations approximately -16.7% volume/week)

Limitations
Variation in inflammatory period based on risk factors and severity of infection
Addition of Abx increases diffusion coefficient
Gradual loss of volume still allows for some volume contracture

Not candidates for immediate salvage– Failed immediate
salvage – Septicaemia
THE CARRION CAST: AN UPDATE ON THE USAGE OF THE INTRACORPORAL ANTIMICROBIAL DOPED SPACER FOR THE TREATMENT OF PENILE IMPLANT INFECTION
Daniel R. Martinez, Eihab Alhammali, Justin Emtage, Justin Parker and Rafael E. CarrionDepartment of Urology, University of South Florida, Tampa, Florida
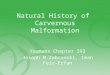
Updated series “Carrion Cast”– Antimicrobial spacer – Maintains size– Treating infection– Bridging gap between
explant and reimplant





5/2012 - 2/2014 9 cases
– 5 Coloplast Genesis SemirigidPenile Prosthesis (SRPP)
– 2 Coloplast Titan Inflatable Penile Prosthesis (IPP)
– 2 narrow SRPP’s• Size range 17cm to 23cm
CaSO4 cast size – 20-30cc, split between corpora
Serum calcium, vancomycinand tobramycin levels stable
THE CARRION CAST: AN UPDATE ON THE USAGE OF THE INTRACORPORAL ANTIMICROBIAL DOPED SPACER FOR THE TREATMENT OF PENILE IMPLANT INFECTION
Daniel R. Martinez, Eihab Alhammali, Justin Emtage, Justin Parker and Rafael E. CarrionDepartment of Urology, University of South Florida, Tampa, Florida

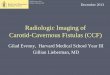
Time to reimplantation– 6-18 weeks
• 6 weeks cast dissolves All had prosthesis
replaced – 1 SRPP– 3 IPP’s– 2 narrow SRPP’s– 1 narrow IPP
• Size range 17cm -20cm
Mean loss prosthesis length 1.1cm
Average penile length maintained 95%
THE CARRION CAST: AN UPDATE ON THE USAGE OF THE INTRACORPORAL ANTIMICROBIAL DOPED SPACER FOR THE TREATMENT OF PENILE IMPLANT INFECTION
Daniel R. Martinez, Eihab Alhammali, Justin Emtage, Justin Parker and Rafael E. CarrionDepartment of Urology, University of South Florida, Tampa, Florida

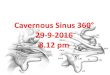
Initial Slurry injections

Active Research
8 50cc cylindrical casts were placed in 100cc of saline
Maintained at 78° F
Weighed weekly for 7 weeks
Ongoing0,00
10,00
20,00
30,00
40,00
50,00
60,00
1 2 3 4 5 6 7 8
100% CaSO4
80/20 SO4/PO4
60/40 SO4/PO4
50/50 SO4/PO4
40/60 SO4/PO4
20/80 SO4/PO4
100 CaPO4
weeks
cc

Infections still pose a risk for penile prosthetic surgery Management choices can be challenging
and have negative outcomes Development of a “Spacer” can provide a
safe option to manage the acute pathology and preserve optimal eventual prosthetic outcome.
Conclusion

References Kraigsley, A. M. and Finkel, S. E. (2009), Adaptive evolution in single species bacterial biofilms. FEMS
Microbiology Letters, 293: 135–140. doi: 10.1111/j.1574-6968.2009.01526.x
Burrows LL, Khoury AE. Infection of medical devices. In: Encyclopedia of biomaterials and biomedical engineering. New York: Marcel Dekker Inc; 2001. p. 839-848.
Costerton B, Cook G, Shirtliff M, Stoodley P, Pasmore M. Biofilms, biomaterials, and device-related infections. In: Ratner BD, Hoffman AS, Schoen FJ, Lemons JE, editors. Biomaterials science: An introducion to materials in medicine, 2nd edition. San Francisco, CA: Elsevier Academic Press; 2004. p. 345-354.
Donlan RM. Biofilms and device-associated infections. Emerging Infect Dis 2001; 7(2): 277-281.
Thomas MV, Puleo DA. Calcium sulfate: Properties and clinical applications. J Biomed Mater Res Part B ApplBiomater. 2009;88(2):597-610.
Harik NS, Smeltzer MS. Management of acute hematogenous osteomyelitis in children. Expert Rev Anti Infect Ther. 2010;8(2):175-81.
Thomas MV, Puleo DA, Al-sabbagh M. Calcium sulfate: a review. J Long Term Eff Med Implants. 2005;15(6):599-607.
Tay BK, Patel VV, Bradford DS. Calcium sulfate- and calcium phosphate-based bone substitutes. Mimicry of the mineral phase of bone. Orthop Clin North Am. 1999;30(4):615-23.
Guo H, Wei J, Liu CS. Development of a degradable cement of calcium phosphate and calcium sulfate composite for bone reconstruction. Biomed Mater. 2006;1(4):193-7.
Daniel M, Chessman R, Al-Zahid S, et al. Biofilm Eradication With Biodegradable Modified-Release Antibiotic Pellets: A Potential Treatment for Glue Ear. Arch Otolaryngol Head Neck Surg. 2012;138(10):942-949. doi:10.1001/archotol.2013.238.
Kostenko V, Lyczak J, Turner K, Martinuzzi RJ. Impact of silver-containing wound dressings on bacterial biofilm viability and susceptibility to antibiotics during prolonged treatment. Antimicrob Agents Chemother. 2010;54(12):5120-31.

References Fallon B., Ghanem H. (1990) Sexual performance and satisfaction with penile prostheses in impotence of
various etiologies. Int J Imp Res 2: 35–42.
Bandyk D.F., Bergamine T.M., Kinney E.V., Seabrook G.R., Towne J.B. (1991) In-situ replacement of vascular prostheses infected with bacterial biofilms. J Vasc Surg 13: 575–583.
Brant M.D., Ludlow J.K., Mulcahy J.J. (1996) The prosthesis salvage operation: immediate replacement of the infected penile prosthesis. J Urol 155: 155–157
Carson C.C., Robertson C.N. (1988) Late hematogenous infection of penile prostheses. J Urol 139: 50–52.
Dietzen C.J., Lloyd L.K. (1992) Complications of intracavernous injections and penile prostheses in spinal cord injured men. Arch Phys Med Rehab 73: 652–655.
Fishman I.J., Scott F.B., Selim A.M., Nguyen T.A. (1997) The rescue procedure: an alternative for managing an infected penile prosthesis. Contemp Urol 11: 77–80.
Knoll L.D. (1998) Penile prosthesis infection: management by delayed and immediate salvage technique. Urology 52: 287–290
Mulcahy J.J. (2000b) Surgical management of penile prosthesis complications. Int J Imp Res 12(Suppl 4): 108–111.
Dorozhkin SV. Biocomposites and hybrid biomaterials based on calcium orthophosphates. Biomatter. 2011;1(1):3-56.
Siegrist T.C., Kwon E.O., Fracchia J.A., Eid J.F. (2008) No touch technique: a novel technique for reducing postoperative infections in patients receiving multicomponent inflatable penile
Carson C.C. (2004) Efficacy of antibiotic impregnation of inflatable penile prostheses in decreasing infection in original implants. J Urol 171: 1611–1614.prostheses. J Urol 179(Suppl): 404–404.
Recommended