Transforming Primary Care
Unlocking the Potential
UK Context
Focus on Managing Long Term Conditions
Reducing demand on hospital care (urgent care)
Shift of care into community settings
Increased demand for primary care
Better value from GP contract
CQC pressure on ‘demonstrating quality’
Commissioning Intentions (PH;NHSE;CCG)
Current State of General Practice
01
23
45
6
Num
ber o
f con
sulta
tions
per
per
son-
year
19951996
19971998
19992000
20012002
20032004
20052006
20072008
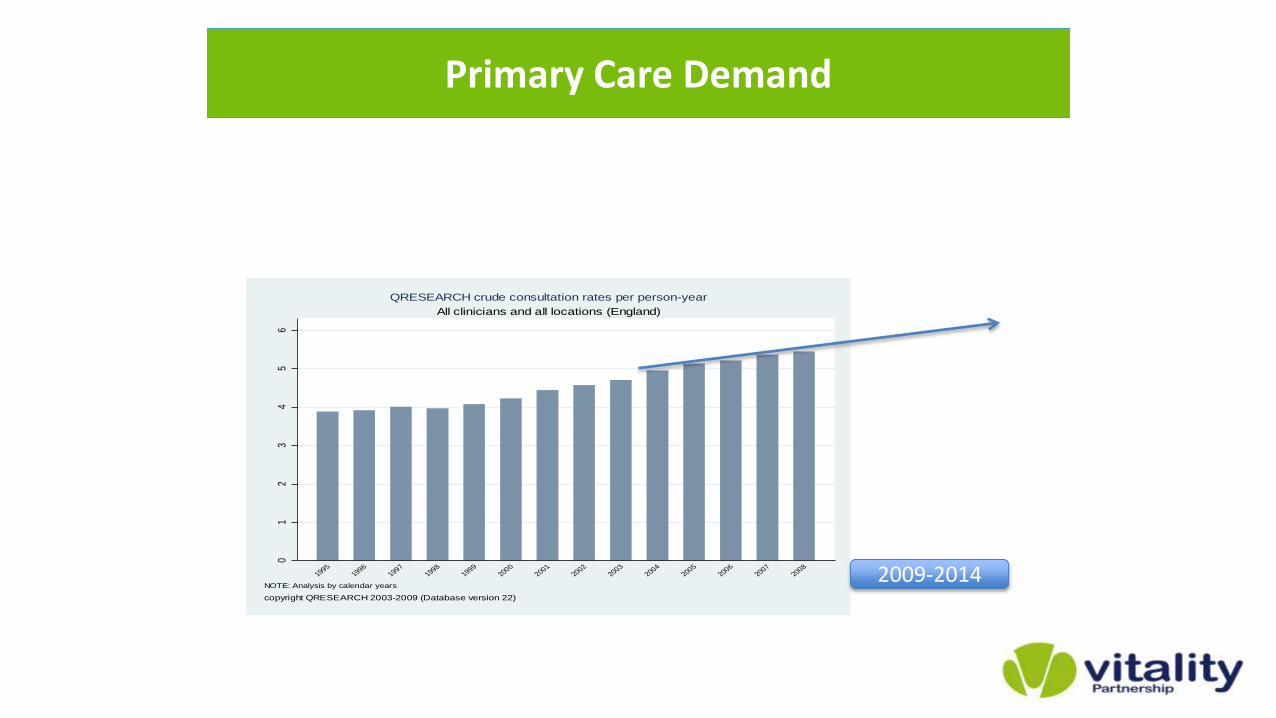
NOTE: Analysis by calendar years
copyright QRESEARCH 2003-2009 (Database version 22)
All clinicians and all locations (England)
QRESEARCH crude consultation rates per person-year
Primary Care Demand
2009-2014
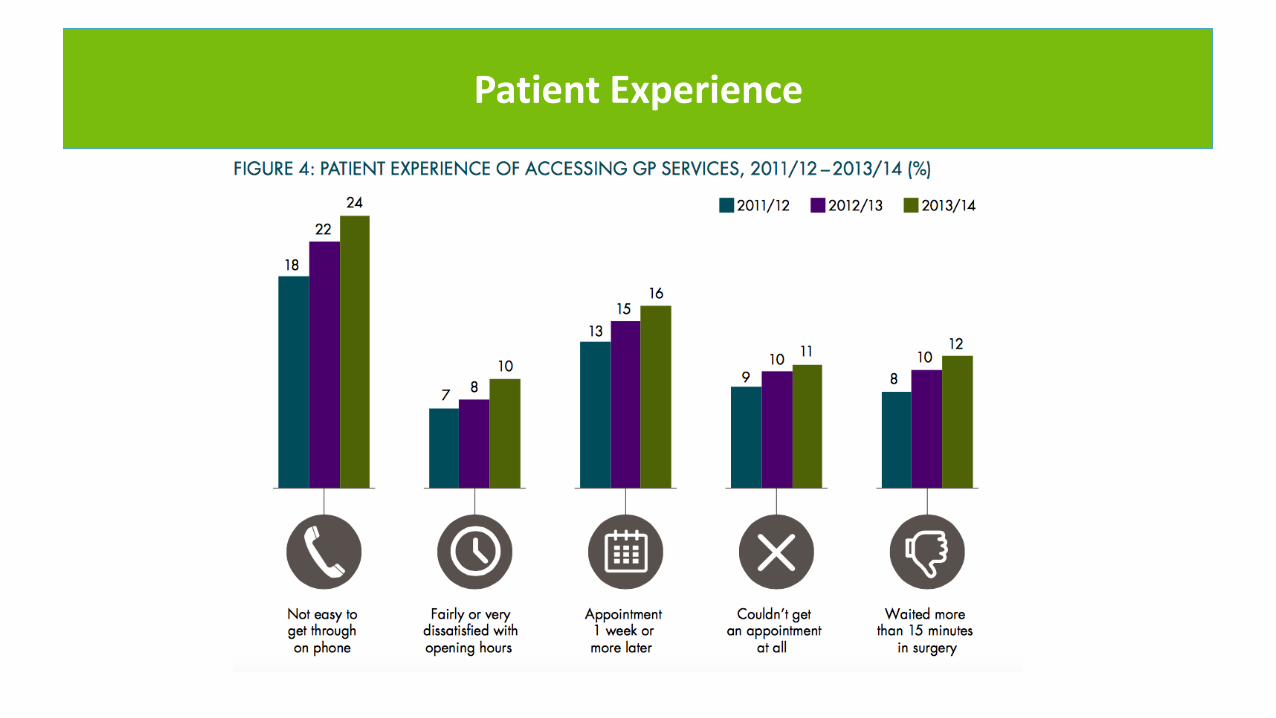
Patient Experience
Primary Care Demand (2)
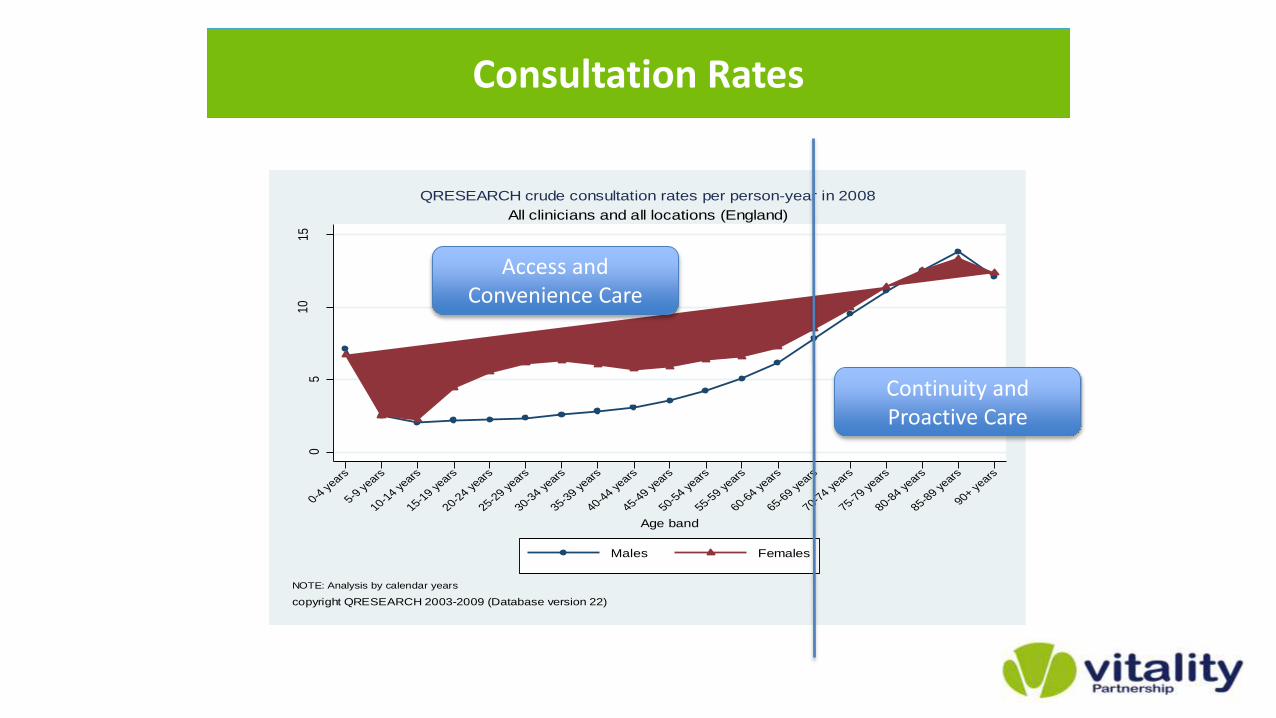
05
1015
Num
ber
of c
onsu
ltatio
ns p
er p
erso
n-ye
ar
0-4 y
ears
5-9 y
ears
10-14 y
ears
15-19 y
ears
20-24 y
ears
25-29 y
ears
30-34 y
ears
35-39 y
ears
40-44 y
ears
45-49 y
ears
50-54 y
ears
55-59 y
ears
60-64 y
ears
65-69 y
ears
70-74 y
ears
75-79 y
ears
80-84 y
ears
85-89 y
ears
90+ years
Age band
Males Females
NOTE: Analysis by calendar years
copyright QRESEARCH 2003-2009 (Database version 22)
All clinicians and all locations (England)
QRESEARCH crude consultation rates per person-year in 2008
Consultation Rates
Continuity and Proactive Care
Access and Convenience Care
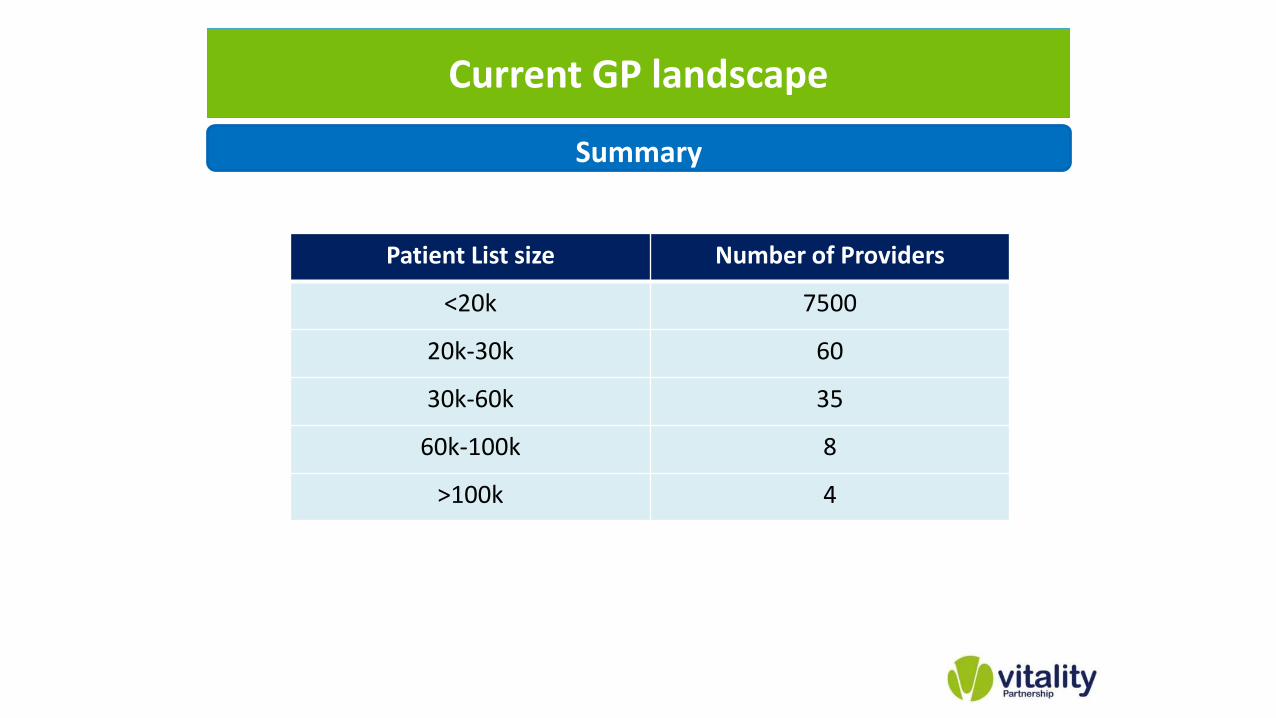
Patient List size Number of Providers
<20k 7500
20k-30k 60
30k-60k 35
60k-100k 8
>100k 4
Current GP landscape
Summary
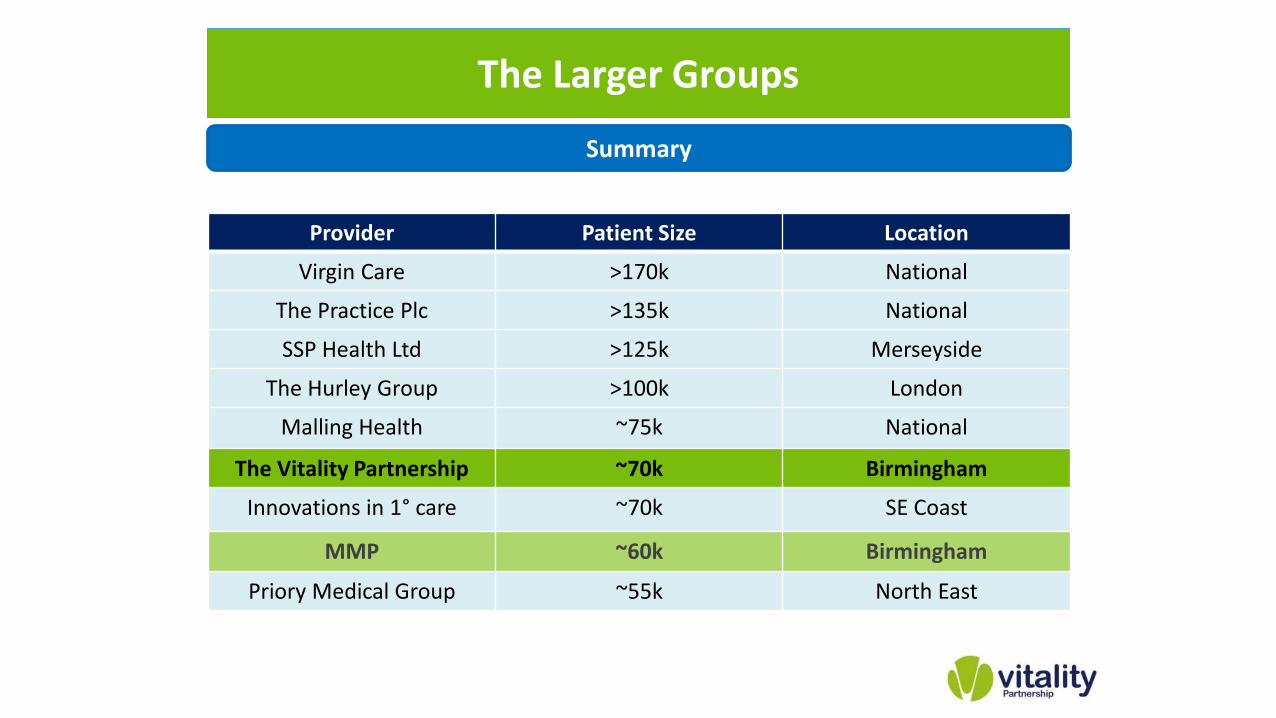
Provider Patient Size Location
Virgin Care >170k National
The Practice Plc >135k National
SSP Health Ltd >125k Merseyside
The Hurley Group >100k London
Malling Health ~75k National
The Vitality Partnership ~70k Birmingham
Innovations in 1° care ~70k SE Coast
MMP ~60k Birmingham
Priory Medical Group ~55k North East
The Larger Groups
Summary
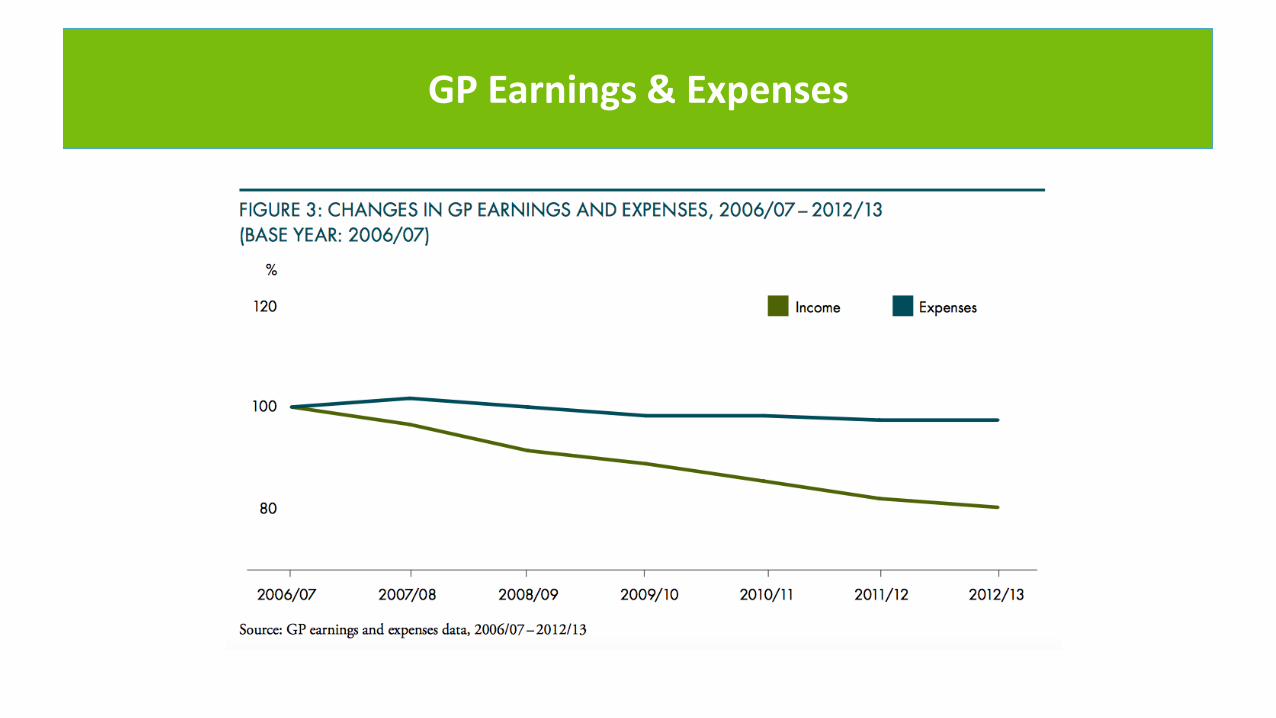
GP Earnings & Expenses
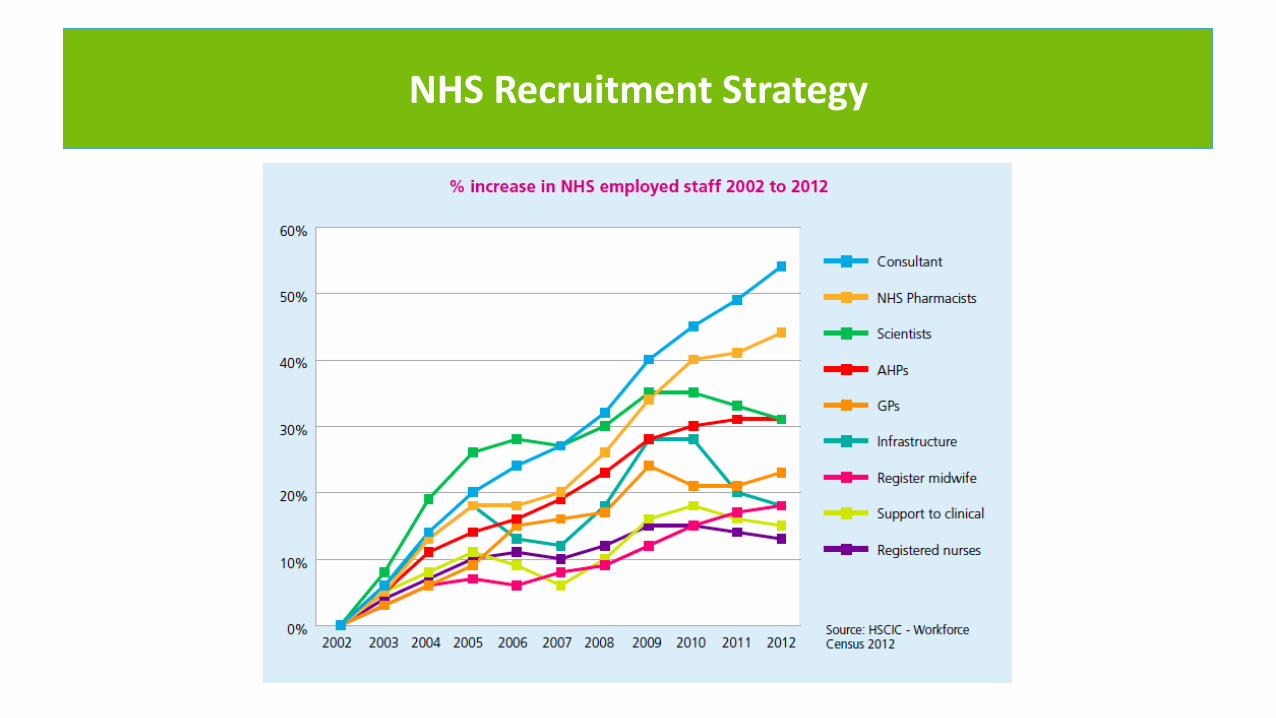
NHS Recruitment Strategy
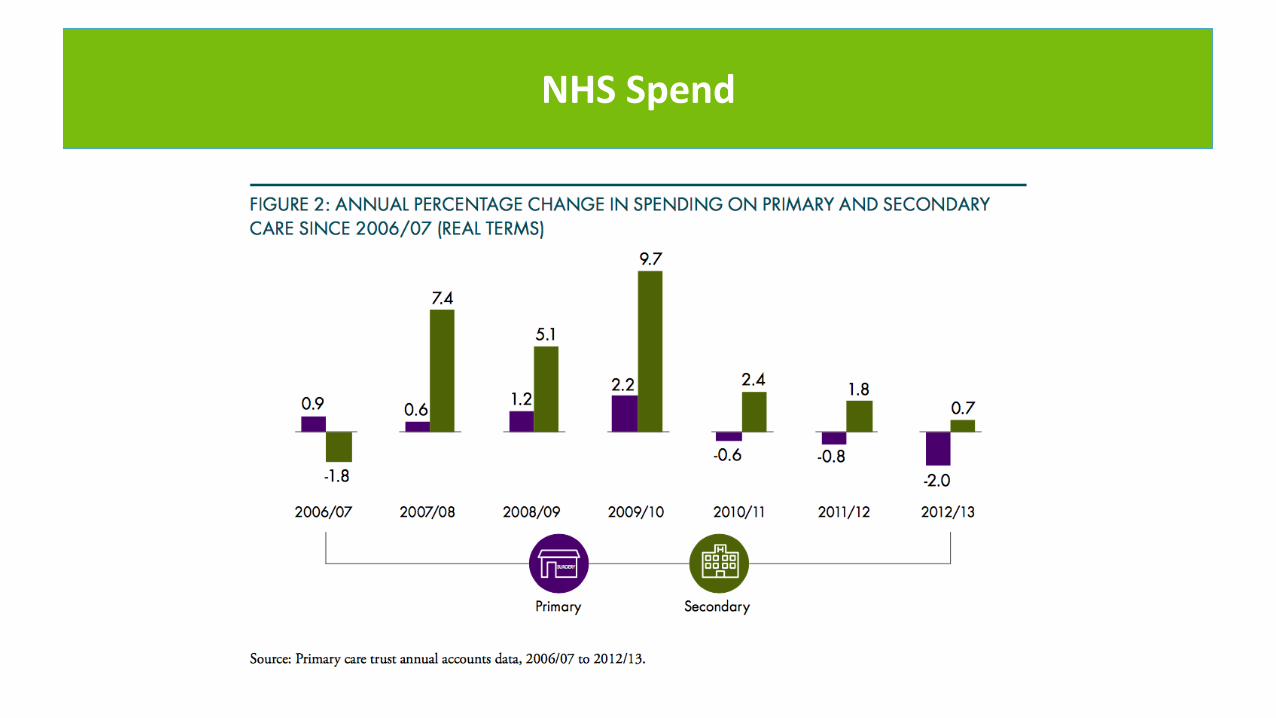
NHS Spend
UK Context
Major challenges to the sustainability of our current model….
Patient access to general practice
Future demand and implications
Unsustainable workloads
Workforce recruitment problems
Patient expectation/experience
Quality and Safety inconsistency
Financial constraints
Drivers for Change
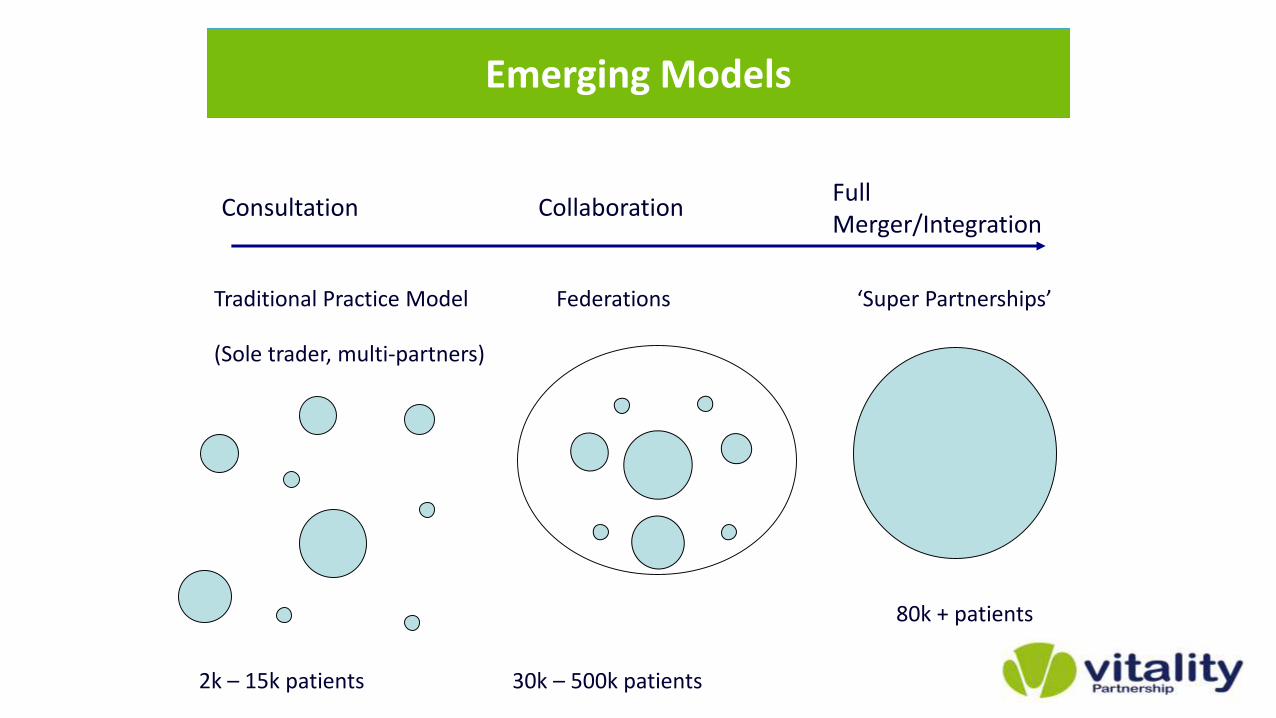
Traditional Practice Model Federations ‘Super Partnerships’
(Sole trader, multi-partners)
FullMerger/Integration
CollaborationConsultation
2k – 15k patients 30k – 500k patients
Emerging Models
80k + patients
UK ContextFederation vs Corporate-Partnership
• Collaboration between multiple practices.
• May be informal or a legal entity, e.g. LLP, CIC, Ltd Co
• Informally or formally established organisational structures with management teams funded by member practices.
• GMS provided by member practices.
• Enhanced services / specialist services provided by federation.
• May share back-office functions.
• Using organisational scale to achieve economies.
• Individual practices retain own identity.
• Potential for conflicts when bidding for services.
• Midlands Health Network, New Zealand
• Tower Hamlets, UK
• Full legal merger between practices
• Corporate style legal entity is the partnership
• Single Management team
• Core services, enhanced services, specialist services, community services, private services
• Share back office functions
• Single scaled organisational infrastructure to expand scope of primary care provision.
• Single legal entity to hold all contracts or legal sub-divisions
• Potential loss of individual practice autonomy
• Quality Improvement through peer review process
• Vitality Partnership, Birmingham
• Whitstable Medical Practice, Kent
• The patient voice at the heart of all provision
• General practice should be the ‘locus of community based
integrated services’
• Specialist expertise is an essential component
of effective integration
• Integrated services to incorporate social care
• Technology is an enabler to manage demand
Vitality Vision for Primary Care
Rationale for Partnership model
• GPs understand partnership model
• Potential for single IT system – shared records
• Innovation at speed
• Single employment structure for staff
• Population management to support business planning
• Foundation for succession planning
• Full alignment of interests
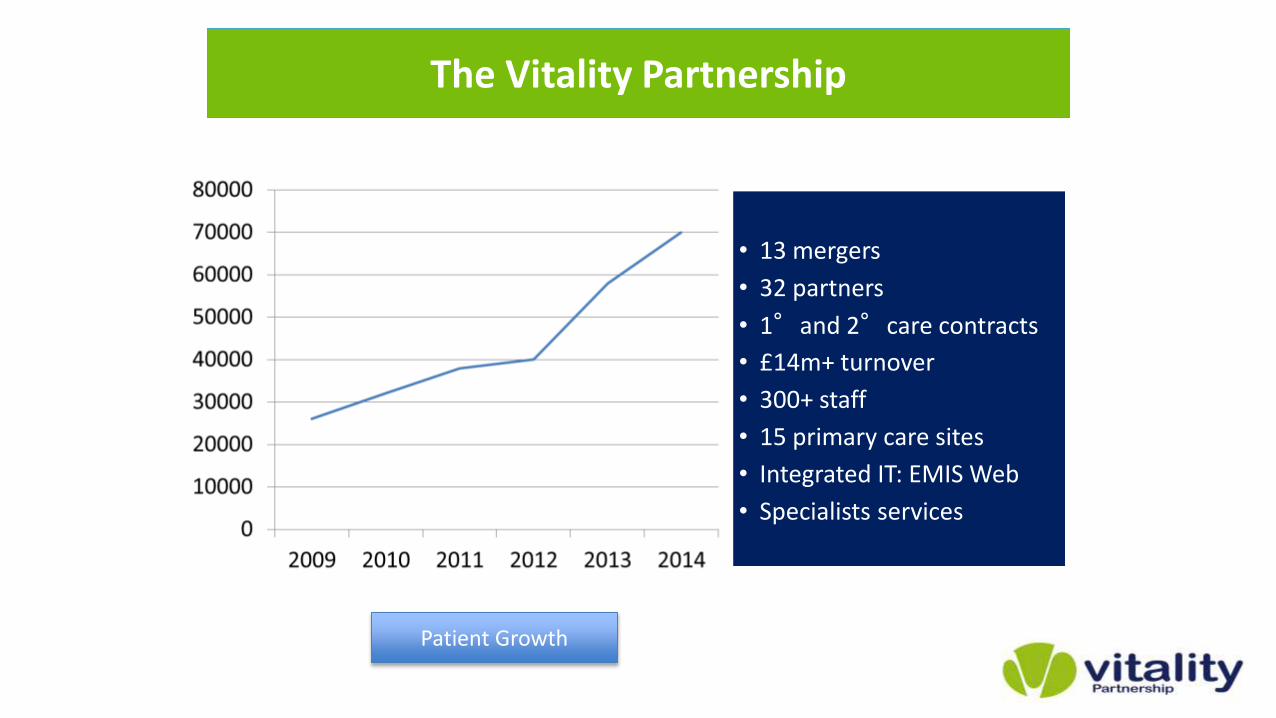
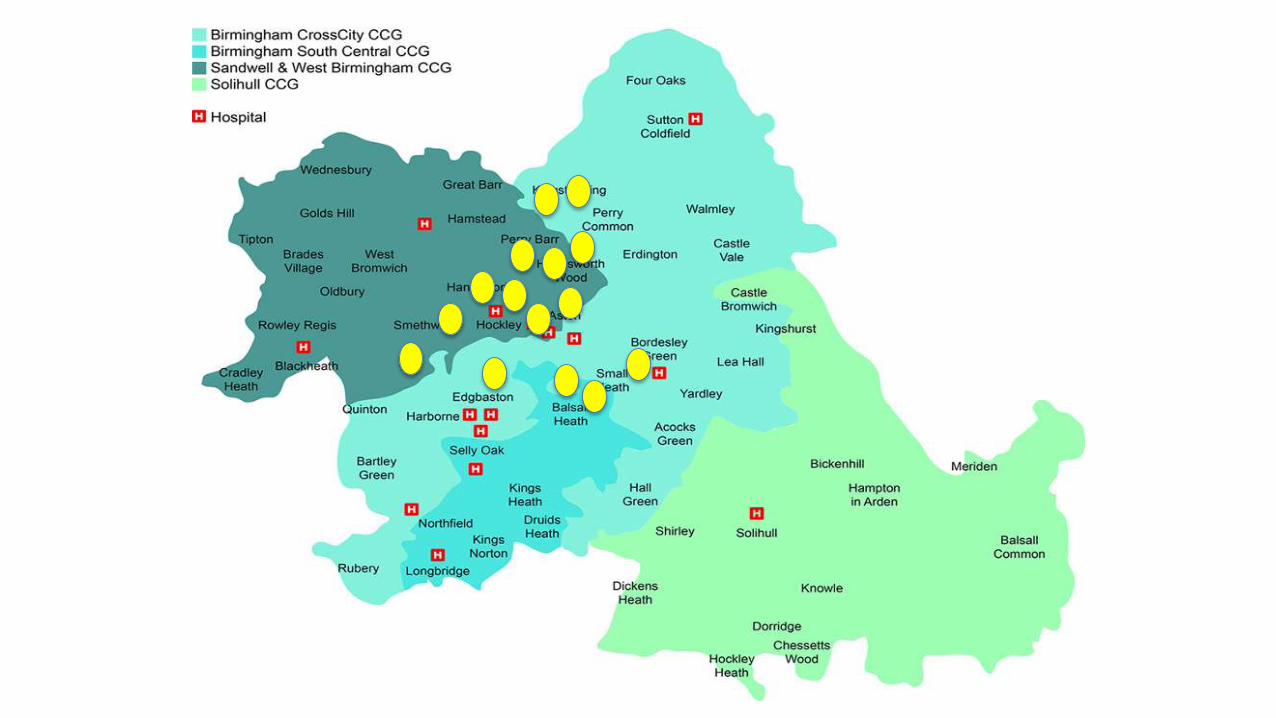
• 13 mergers
• 32 partners
• 1°and 2°care contracts
• £14m+ turnover
• 300+ staff
• 15 primary care sites
• Integrated IT: EMIS Web
• Specialists services
The Vitality Partnership
Patient Growth
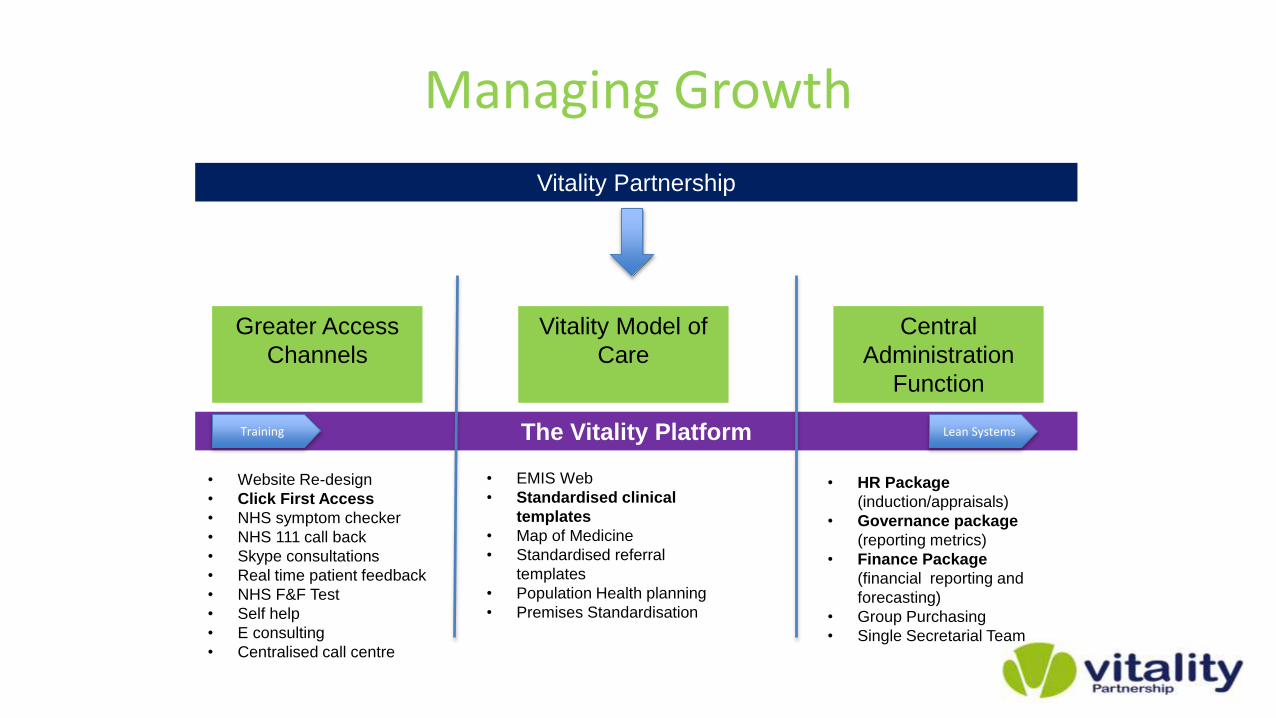
Managing Growth
Vitality Partnership
The Vitality Platform
Greater Access
Channels
Vitality Model of
Care
Central
Administration
Function
• Website Re-design
• Click First Access
• NHS symptom checker
• NHS 111 call back
• Skype consultations
• Real time patient feedback
• NHS F&F Test
• Self help
• E consulting
• Centralised call centre
Training
• EMIS Web
• Standardised clinical
templates
• Map of Medicine
• Standardised referral
templates
• Population Health planning
• Premises Standardisation
• HR Package
(induction/appraisals)
• Governance package
(reporting metrics)
• Finance Package
(financial reporting and
forecasting)
• Group Purchasing
• Single Secretarial Team
Lean Systems

Digital Vitality – Our Consumers
• 82% of UK population using broadband to transact…
• <1% of patients using the internet to interact with clinicians!
• Birmingham has highest penetration of smartphone use in the U.K….nearly 30% more than London..
We have the population
and capability to shift the
balanace of provision to
the web!
The HuB model
Digitally enabled transformation of healthcare is not about systems, data, technology, analytics….or any of the usual NHS IT/Informatics stuff….
Delivering real change is about changing the business model, through the power of the internet, to create new provider models….engaging consumers in new, highly efficient and scalable ways of actually receiving a service.
IT/Informatics operates at the margins of healthcare….Digital is the future of healthcare delivery!
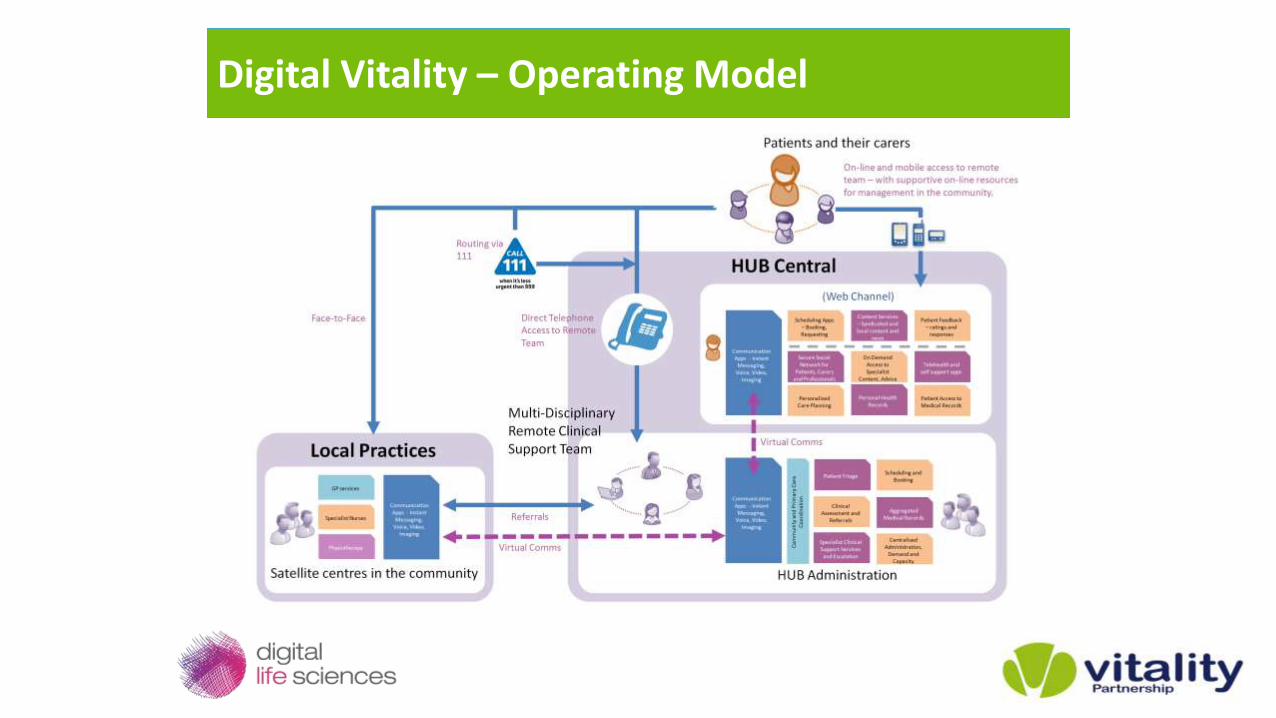
Digital Vitality – Operating Model
Making it Happen – So far… www.vitalitypartnership.nhs.uk
• New digital and telephone access channels launched and rolling out…
• New clinical contact centre launched and rolling out alongside clinical transformation at sites….
• New ‘Vitality Guides’ launched…
• Extended physical access model on-line..
• Scaling services to all patients within the consortium (Circa 70,000)…
• Launched initial long term conditions management programmes and unified care planning…
• Re-engineered clinical resource into the HuBmodel on an extended basis…
• Drive the ‘Vitality Healthy Community’
• Expand…
Making it Happen – So far… www.vitalitypartnership.nhs.uk
Reengineered in-day services
• 72% reduction in DNAs....equates to an annualised cost saving of approximately £210k
across the whole business
• 10% increase in within day activity – meeting unmet demand within the resources already
available
• 65% of patients are consistently being dealt with remotely without having to come in to
practice
• Average consultation time reduced to under 5 mins (for the remote consultations)
• 70% of patients say that the new access system is better than before
• Reduction in A&E of between 10-15%
Extended Access
• Now doing extended access 8-til-8 Monday to Friday and Saturdays, with both remote and
physical consultations
Headline Results
Challenges
• Managing short term contracts vs. GMS & PMS
• Managing costs as you grow
• Property infrastructure solutions
• Clinical Time into mergers
• Communication – staff/patients
• Accurate data to plan
• What is optimum size and footprint
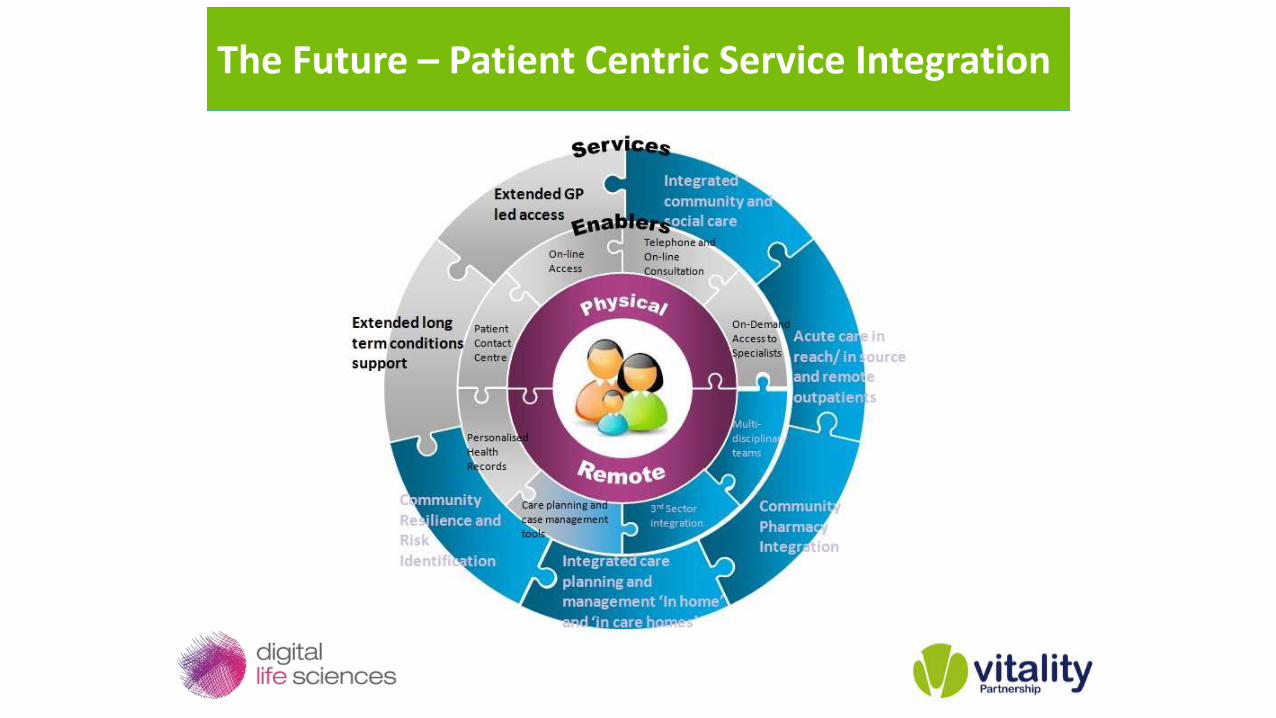
The Future – Patient Centric Service Integration

Questions…?
Robin Vickers
Exec Director at Digital Life Sciences
Sarb Basi
Managing Director at Vitality Partnership
Recommended

















