Robotic Telepathology: Practical Applications
Bruce E. Dunn, M.D.
Chief Pathologist, Veterans Integrated Service Network (VISN) 12
Professor and Vice-Chair, Dept of Pathology, Medical College of Wisconsin

Conflict-of-interest statement
Bruce E. Dunn, MD has no financial interest in any commercially-available telepathology system

21 Veterans Integrated Service Networks (VISNs)

Hospitals and CBOCs in VISN 12

Robotic Telepathology (TP) at Iron Mtn
• Iron Mountain is an active, rural DVA hospital with a general surgery program– 1000 - 1500 surgical pathology cases per year– Occasional frozen sections requested
• 1996: part-time Iron Mountain pathologist retired• Full implementation of commercial hybrid
dynamic store/forward system operated by two senior pathologists in Milwaukee
• Feasibility study performed - published in 1997

Three Phases of Robotic TP at Iron Mtn
• Phase I: mid-1996 – early 1999– Two senior surgical pathologists exclusively read cases with
extensive documentation– 2,200 cases available for TP– Summary published in 1999
• Phase II: early 1999 – end of 2004– One senior pathologist retired; three junior pathologists hired– Consolidation in VISN resulted in increased AP workload– 5,841 cases available for TP
• Phase III: 2005 – present (through July 2006)– One original senior pathologist and two new pathologists– ASAP ImagingTM implemented– 2,015 cases available for TP through July 2006

Objectives
• Compare rates of case deferral and major TP discordance with light microscopy (LM) among seven pathologists during three phases of robotic telepathology
• Compare rates of major discordance before and after implementing the ASAP ImagingTM system

Summary of Cases (1999)
Organ/system Percent of totalGastrointestinal 42.9Skin 27.5Prostate 10.2Hernia sac 3.8Urinary bladder 2.6Bone/synovium/tendon 2.1Penis/testis/spermatic cord 1.9Gallbladder 1.3Extremity amputation 1.1Appendix 0.5Gynecologic 0.5Breast 0.3Miscellaneous 5.2

Technical Aspects of Workflow
• Tissue grossed in Iron Mtn by experienced PA (tele-gross imaging available)
• Slides processed by Iron Mtn histotechnician
• Telepathology systems “linked up”
• PA places slides onto stage in Iron Mtn
• Pathologist controls robotic microscope remotely from Milwaukee

Current and Future




Robotic Microscopy• Commercial hybrid dynamic store/forward system• Olympus microscope with motorized stage, objectives,
lighting control• CODEC used for gross & microscopic imaging and
videoconferencing• 4x,10x, 20x 40x 100 (oil free) objectives• Dynamic imaging: 350 x 288 x 24-bit color• Static imaging: 1520 x 1144 x 24-bit color• Images transmitted at 768 kbps over WAN• 2005: ASAP ImagingTM enables remote access with live
streaming imaging

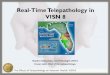
VISN 12 Telepathology Network
Hines
Madison
Tomah
NorthChicago
Westside
Milw
IronMtn
VHA WANInternet
VHA WANInternet
DR
DR
GS
RM
DR
GS
NRM
NRM
NRM
GS
NRM
NRM
KEYPOP – point of presenceVistA – VA computerized patient record system
WAN
POP
POP
POP
POP
POP
POP
POP
Multi-siteconferencing
DR
DR
POP
DedicatedServer
Current and Future
Tomah
Madison
Hines
Hines Micro
Iron Mtn
Milwaukee
N. Chicago
Chicago
Interface to HIS

Current and Future

Methods• Each of 7 pathologists read cases by TP, completed
reports where appropriate, then read same cases by LM• Over 50% of cases read by second pathologist by LM• Revised reports generated based on LM diagnosis, if
necessary, and clinician notified • Reasons for case deferral to LM documented• Pathologist-specific rates of deferral and discordance
determined • Notes:
– TURP and bone marrow cases deferred automatically– Gastric biopsies reviewed for H. pylori-like organisms by PA
in Iron Mtn by LM

Current and Future
Non-Robotic Telepathology System

Deferral to Light Microscopy
• Reasons for deferral: case difficulty, need for consultation, special or immuno stains, “short staffing”
• If case referred to Milwaukee due to computer unavailability (malfunction or upgrade), or the assigned pathologist was not yet competent to use telepathology, then case not counted as a deferral

Discordance Rates by Pathologist
• Deferred cases not included
• Major discordance– Benign versus malignant– Different patient outcome or therapy
• Report modified and clinician called

Phase I Individual SummariesPathologist A B Total
Total opportunities 1121 1079 2200
No. deferred 34 22 56
Deferral rate (%) 3.0 2.0 2.5
TP cases 1087 1057 2144
Maj discord 5 2 7
Discordance (%) 0.46 0.19 0.33

Phase II Individual SummariesPathologist B C D E Total
Total opportunities 2231 1582 1031 997 5841
No. deferred 319 290 270 326 1205
Defer rate (%) 14.3 18.3 26.2 32.7 20.6
TP cases 1912 1292 761 671 4636
Maj discord 7 5 8 1 21
Discordance (%) 0.37 0.39 1.05 0.15 0.45

Phase III Individual Summaries (ASAP) (July 2006)
Pathologist B D E F G Total
Total opportunities 795 17 185 683 335 2015
No. deferred 40 0 12 78 65 195
Deferral rate (%) 5.0 0 6.5 11.4 19.4 9.7
TP cases 755 17 173 605 270 1820
Maj discord 1 0 0 2 1 4
Discordance (%) 0.13 0 0 0.33 0.37 0.22

Comparison by Phase (July 2006)
Phase I II III Total
Total opportunities 2,200 5,841 2,015 10,056
No. deferred 56 1,205 195 1,456
Deferral rate (%) 2.5 20.6 9.7 14.5
TP cases 2,144 4,636 1,820 8,600
Maj discord 7 21 4 32
Discordance (%) 0.33 0.45 0.22 0.37

Pathologist B: Major concordance rate (N=3,724)(July 2006)
95
96
97
98
99
100
0-10
0
201-
300
401-
500
601-
700
801-
900
1001
-110
0
1201
-130
0
1401
-150
0
1601
-170
0
1801
-190
0
2001
-210
0
2201
-230
0
2401
-250
0
2601
-270
0
2801
-290
0
3001
-310
0
3201
-330
0
3401
-350
0
3601
-370
0
% c
onco
rdan
ce

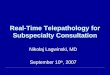
Pathologist-Specific Discordance Rates
0.12
0.270.33 0.37 0.39
0.46
1.03
0
0.2
0.4
0.6
0.8
1
1.2
E B F G C A D
Pathologist
Dis
cord
ance
Rat
e (%
)

Major Discordance Rate by Technology (July 2006)
Pathologist
Technology B E All
Pre-ASAP 0.30 0.15 0.41*
ASAP 0.13 0 0.22
*0.33 excluding pathologist D

Summary
• Pathologist-specific discordance rates ranged from 0.12% to 1.03%, with median of 0.37% and overall rate of 0.37%
• Despite extensive experience of one senior pathologist, occasional discordances continue to occur
• The rates of discordance using ASAP ImagingTM are lower that those observed previously
• All TP cases continue to be reviewed by LM

References
• Dunn, B.E., U.A. Almagro, H. Choi, N.K. Sheth, J.S. Arnold, D.L.Recla, E.A. Krupinski, A.R. Graham and R.S. Weinstein. 1997. Dynamic-robotic telepathology: Department of Veterans Affairs feasibility study. Human Pathol. 28:8-1.
• Dunn, B.E., H. Choi, U.A. Almagro, D.L. Recla, and R.S. Weinstein. 1999. Routine surgical telepathology in the Department of Veterans Affairs: Experience-related improvements in pathologist performance in 2200 cases. Telemed J. 5:323-337.
Recommended