Robotic Surgery for
Upper Tract Urothelial Carcinoma
Li-Ming Su, MD David A. Cofrin Professor of Urology, Associate Chairman of Clinical Affairs, Chief, Division of Robotic and Minimally Invasive Urologic
Surgery, University of Florida College of Medicine; Gainesville, Florida
Objectives: • Describe the indications and contraindications for robotic surgery
for upper tract urothelial carcinoma • Outline operative setup and surgical steps for robotic
nephroureterectomy with regional lymphadenectomy • Discuss the operative setup and surgical steps Psoas hitch and
ureteral reimplantation • Review the published literature on robotic surgery for upper tract
urothelial carcinoma as compared to conventional laparoscopic surgery
Robotic Surgery for Upper Tract Urothelial Carcinoma
Li-Ming Su, M.D.David A. Cofrin Professor of Urology
Chief, Division of Robotic and Minimally Invasive Urologic SurgeryDepartment of Urology
University of Florida College of Medicine
U N I V E R S I T Y of
FLORIDA UFThe Foundation for The Gator Nation
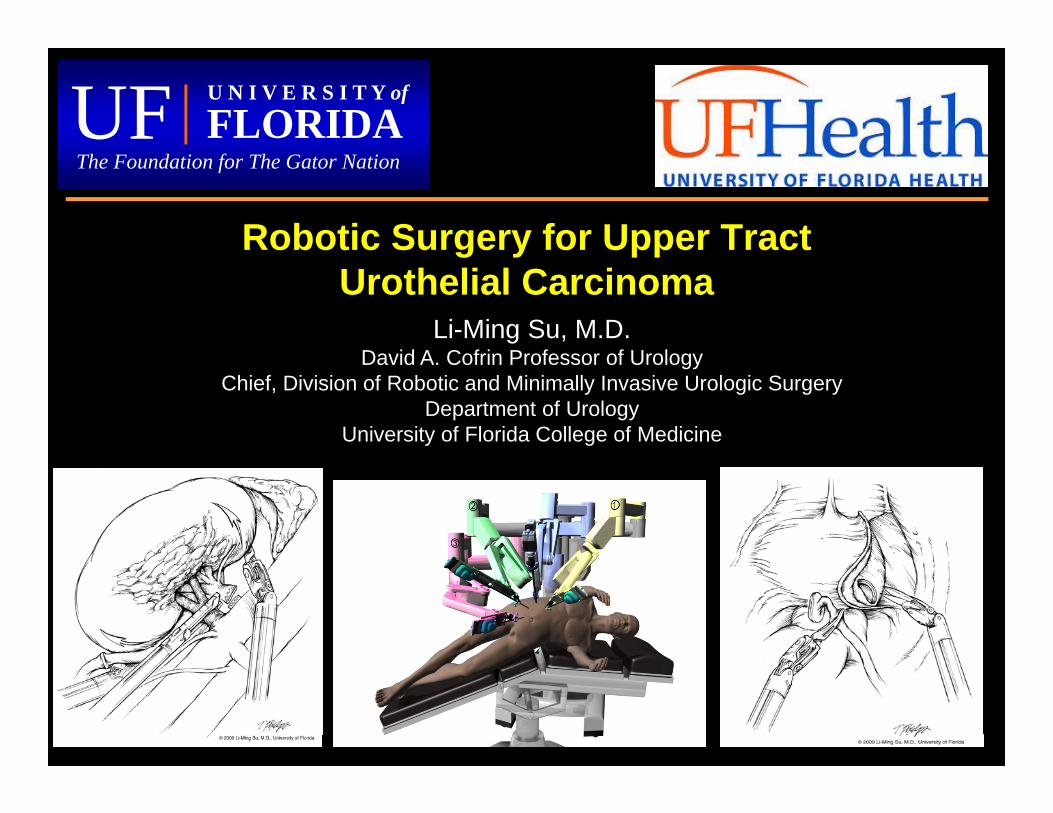
Is The Robot Necessary?
vs.
Laparoscopy Robotic Surgery
• Not necessary for experienced laparoscopists• Surgeons with limited laparoscopic experience• Expansion of robotic practice and offerings• Stepping stone towards robotic partial NTx
Indications and ContraindicationsIndications:• Same as open or laparoscopic
surgery
• Endoscopic or biopsy proven upper tract TCCa
• Normal contralateral kidney and renal function
Contraindications:• Contraindication to laparoscopy
• ?Evidence of regional spread (e.g. N+ disease) consider chemo
Robotic NUx: General Principles
• 3-armed robotic technique• Single patient positioning• Single trocar configuration (4 trocars)• For NUx:
– Two robot docking setup• nephrectomy • distal ureterectomy and bladder cuff
– Extravesical approach to bladder cuff– Single cystotomy
Operative Steps: RANUx
• Step 1: Dock robot 45o angle from the head of OR table
• Step 2: Mobilize of ipsilateral colon
• Step 3: Clip ureter beneath lesion
• Step 4: Dissect renal hilum
• Step 5: Transect renal artery and vein
• Step 6: Complete mobilization of kidney
• Step 7: Perihilar lymphadenectomy
• Step 8: Dissect ureter as far distally as possible
Operative Steps: RANUx (cont.)
• Step 9: Instill intravesical mitomycin C
• Step 10: Re-dock robot at 45o angle from the foot of OR table
• Step 11: Mobilize ipsilateral bladder
• Step 12: Dissect out ureterovesical junction; drain bladder
• Step 13: Excise bladder cuff and close cystotomy
• Step 14: Pelvic lymphadenectomy
• Step 15: Entrap specimens and place drain
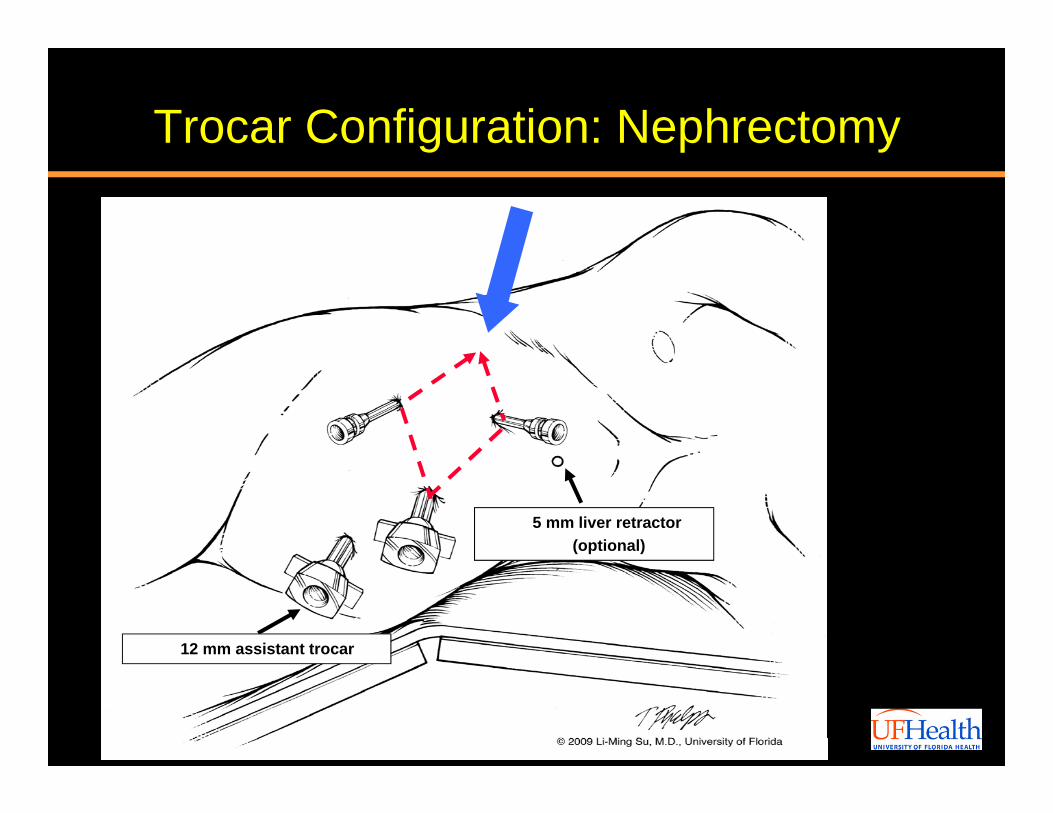
Trocar Configuration: Nephrectomy
5 mm liver retractor (optional)
12 mm assistant trocar
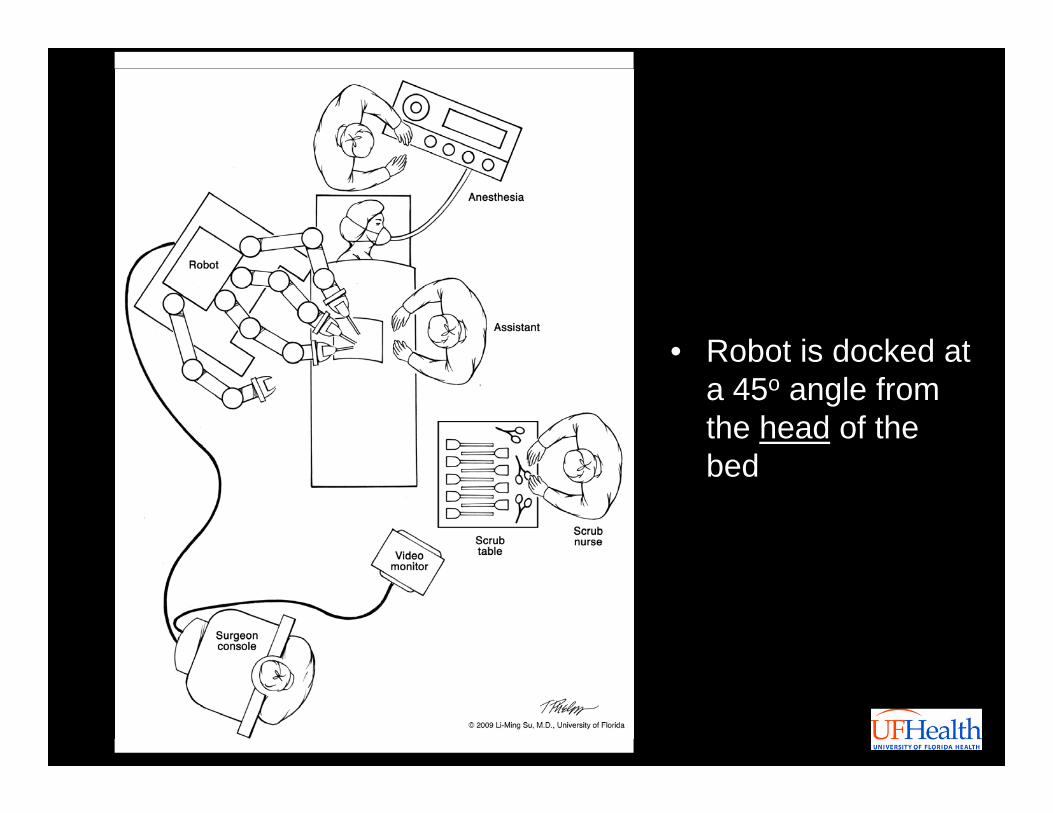
• Robot is docked at a 45o angle from the head of the bed
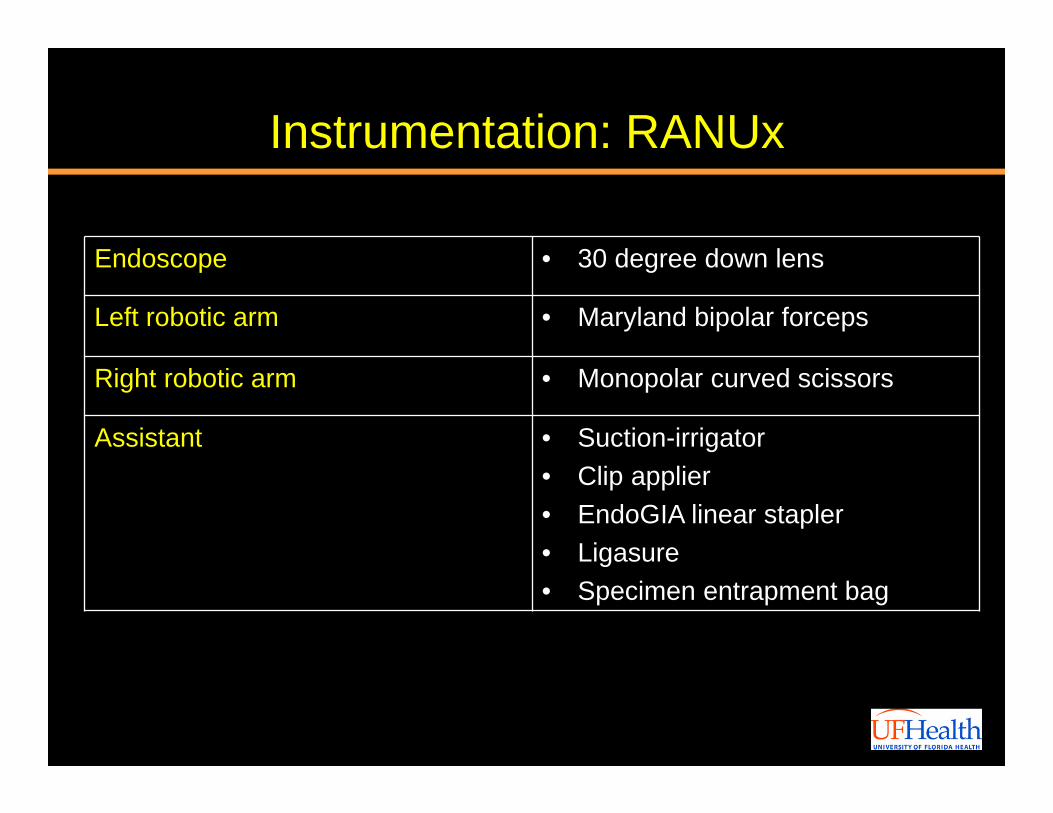
Instrumentation: RANUx
Endoscope • 30 degree down lens
Left robotic arm • Maryland bipolar forceps
Right robotic arm • Monopolar curved scissors
Assistant • Suction-irrigator• Clip applier• EndoGIA linear stapler• Ligasure• Specimen entrapment bag
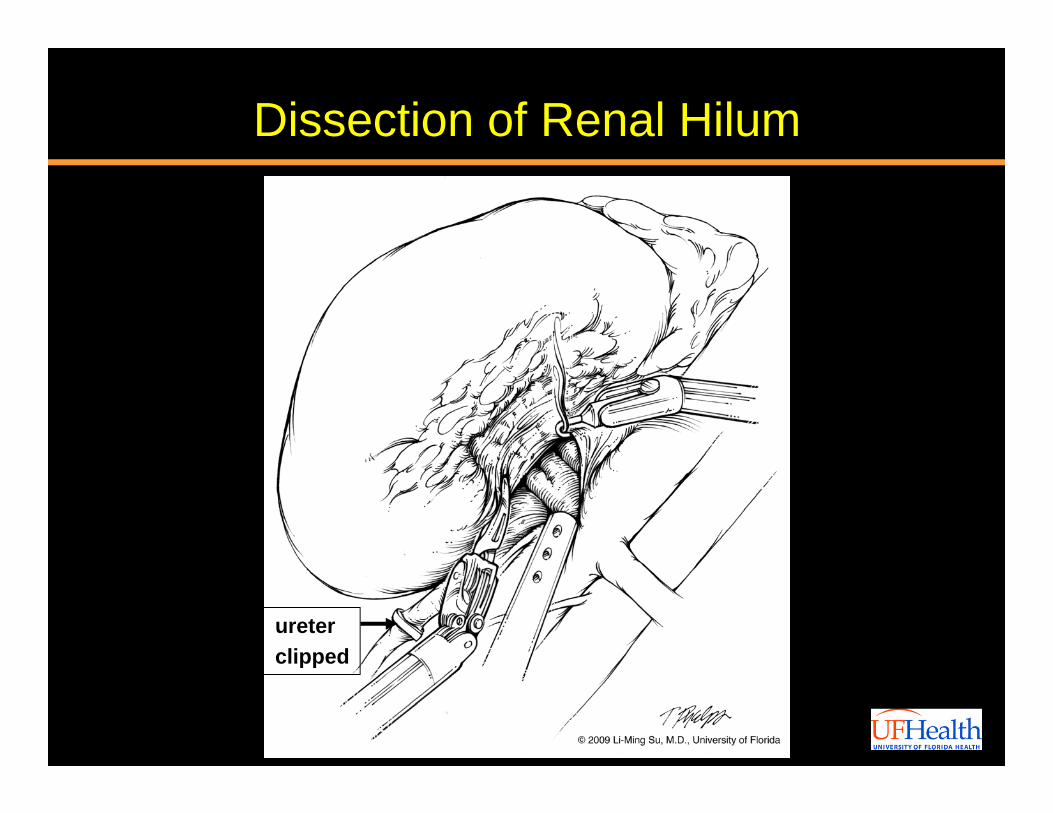
Dissection of Renal Hilum
ureterclipped
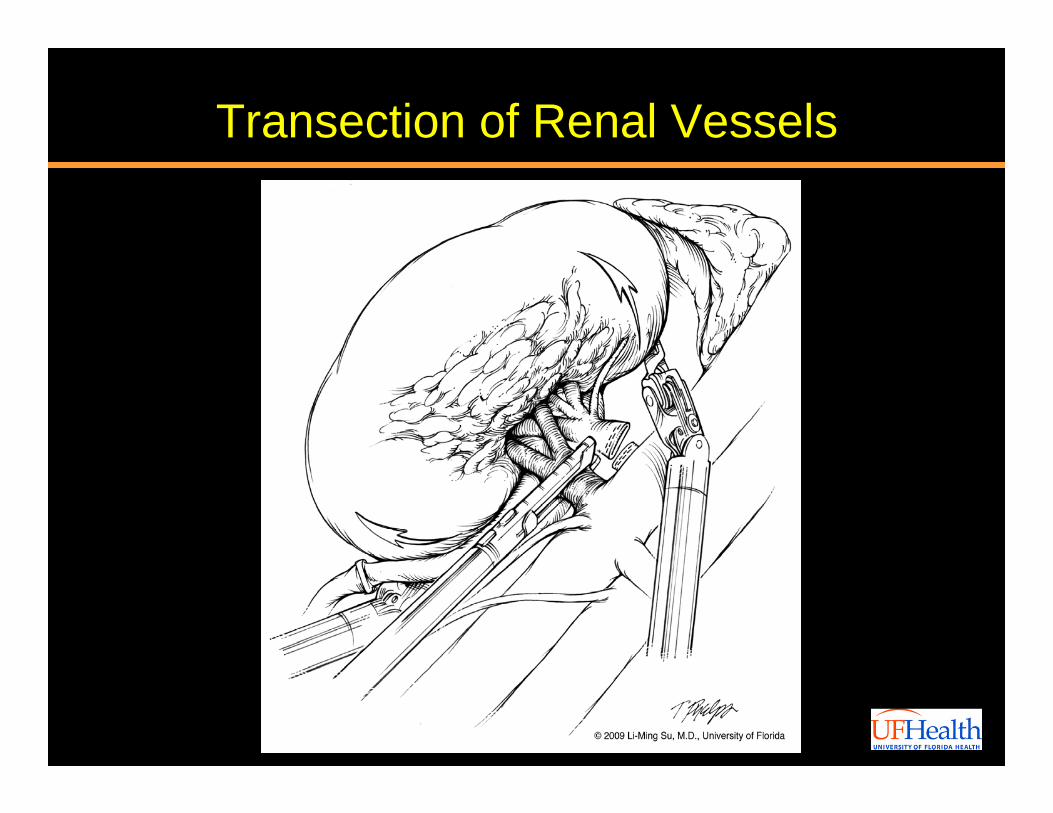
Transection of Renal Vessels
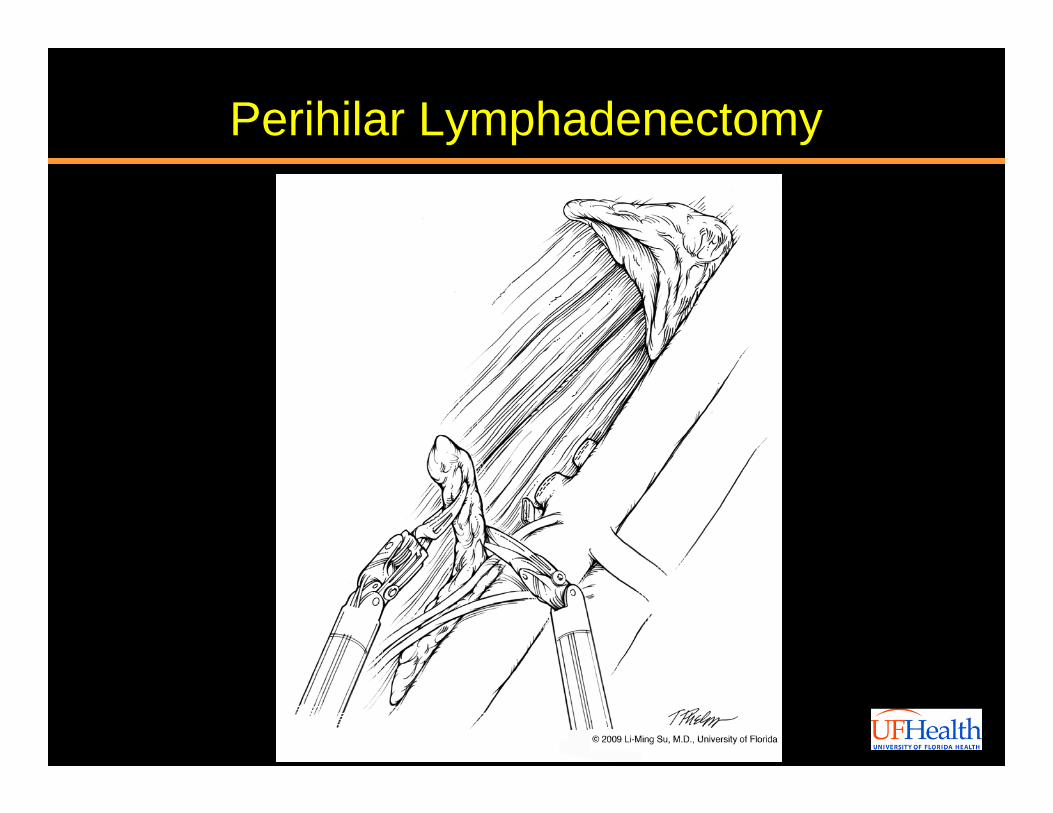
Perihilar Lymphadenectomy
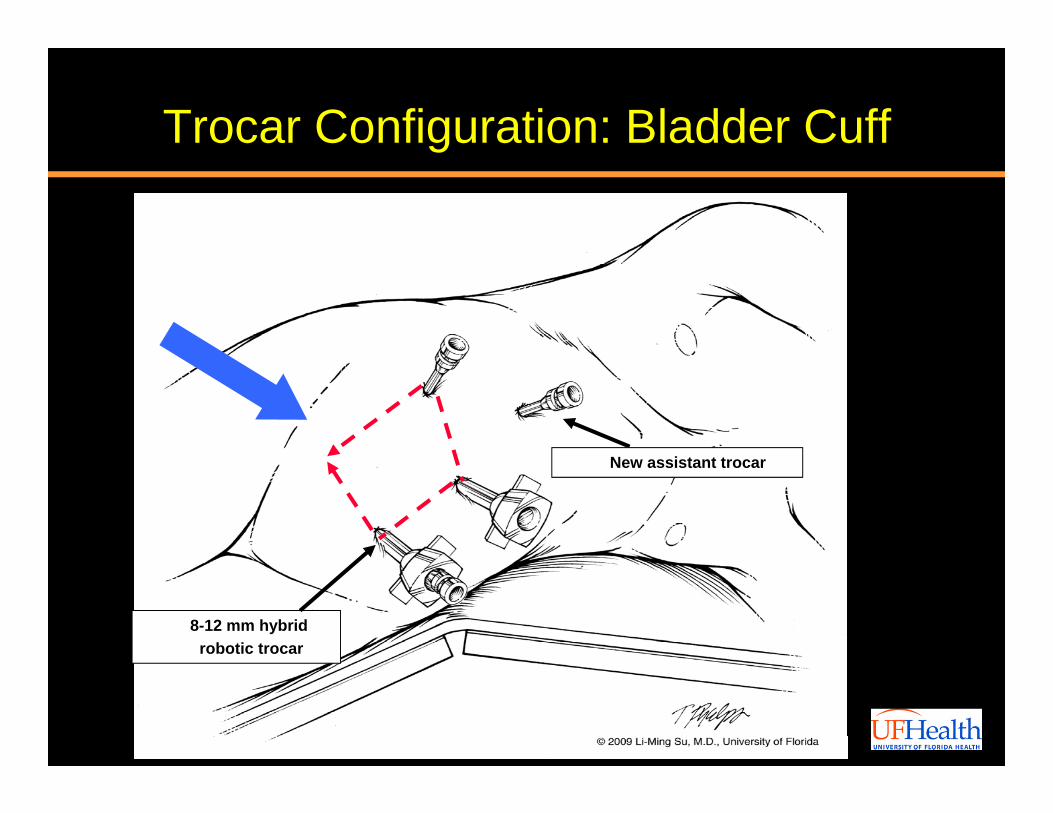
Trocar Configuration: Bladder Cuff
New assistant trocar
8-12 mm hybrid robotic trocar
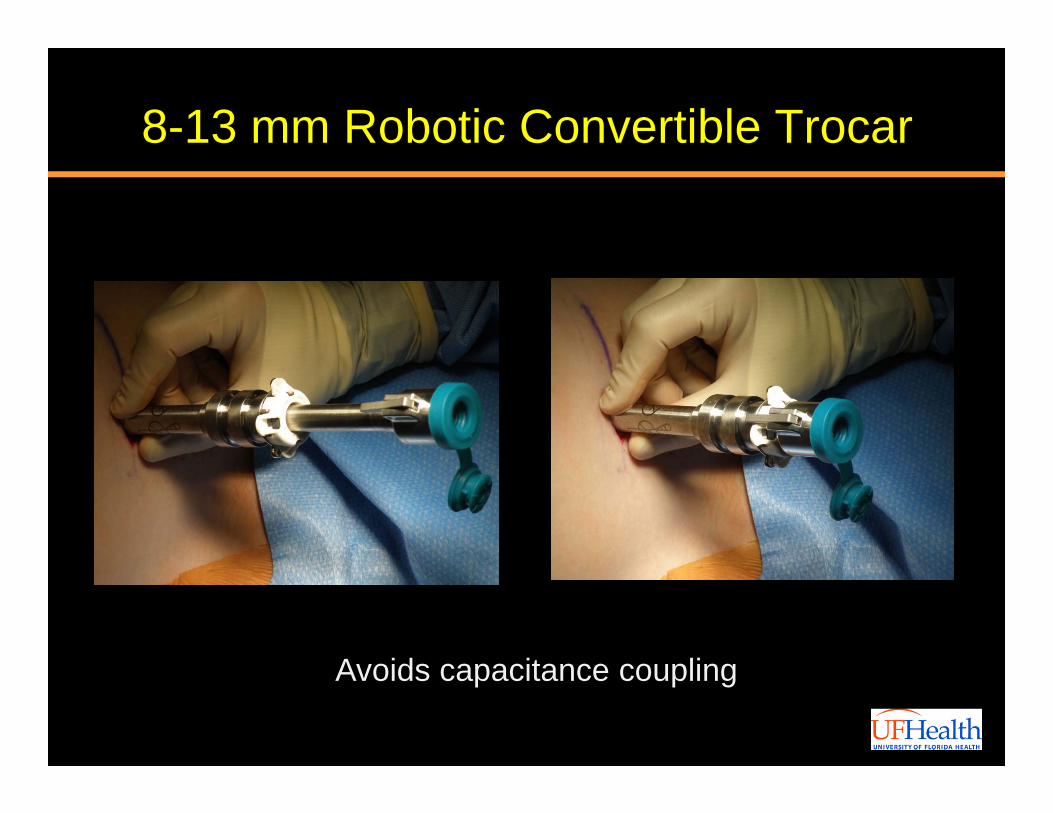
8-13 mm Robotic Convertible Trocar
Avoids capacitance coupling
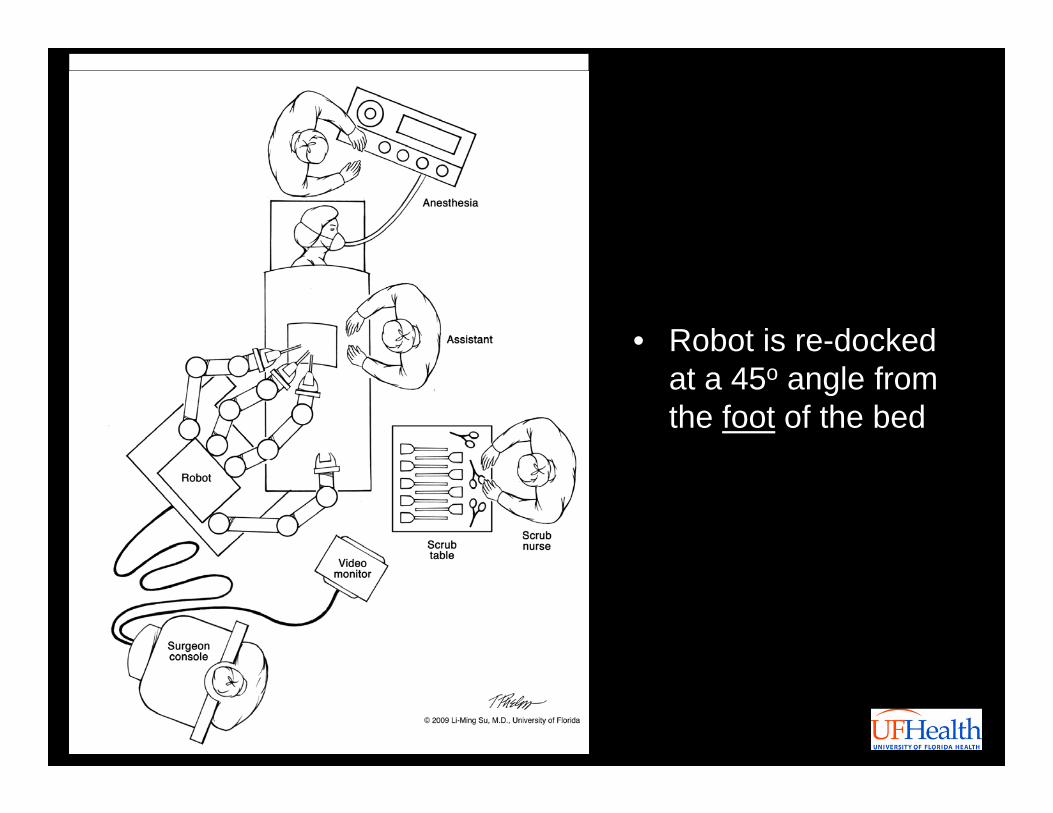
• Robot is re-docked at a 45o angle from the foot of the bed
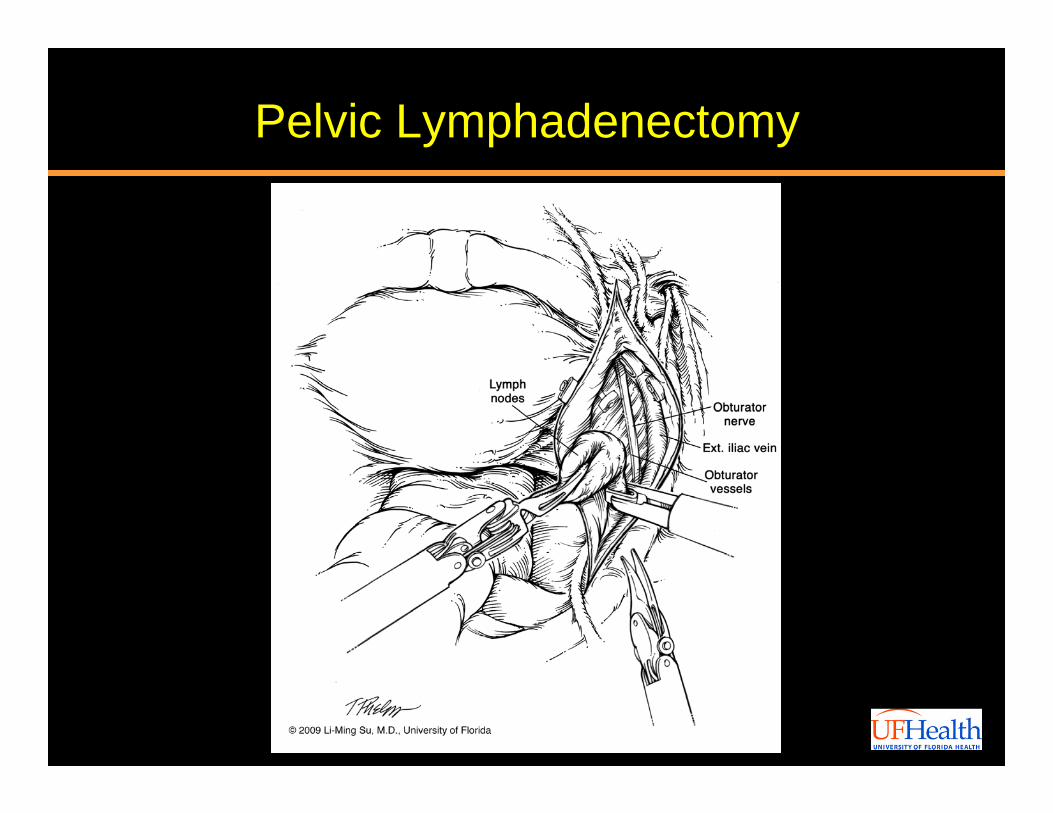
Pelvic Lymphadenectomy
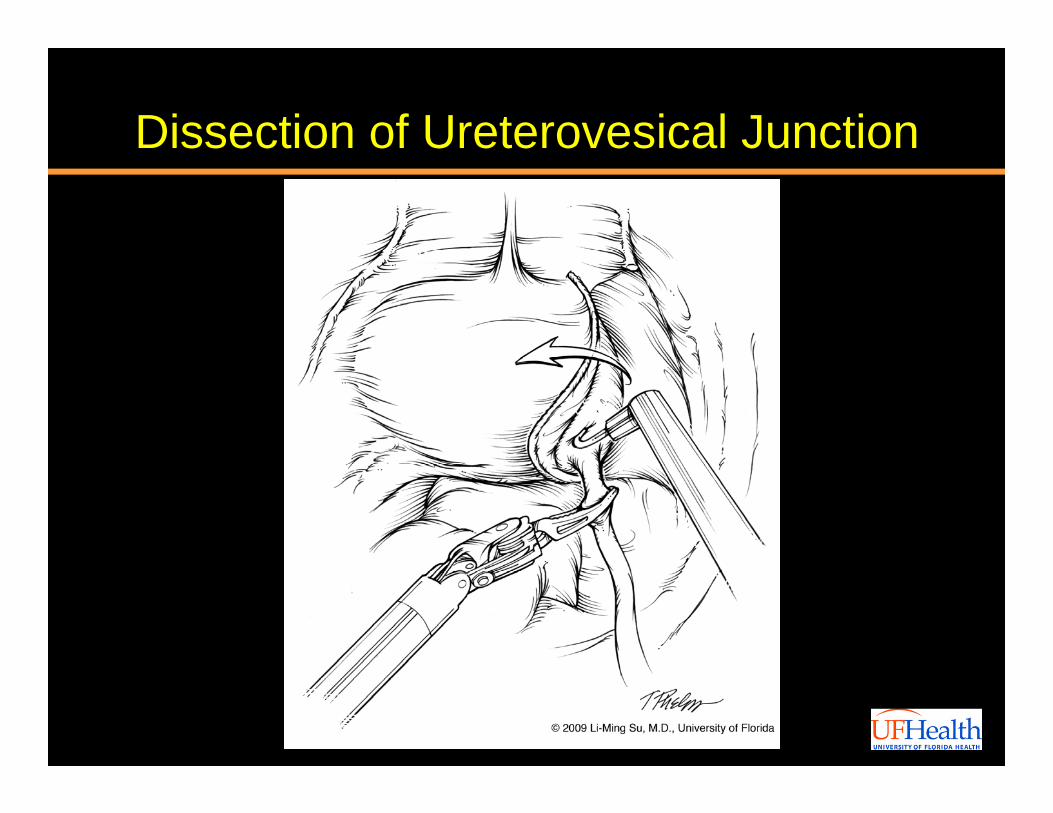
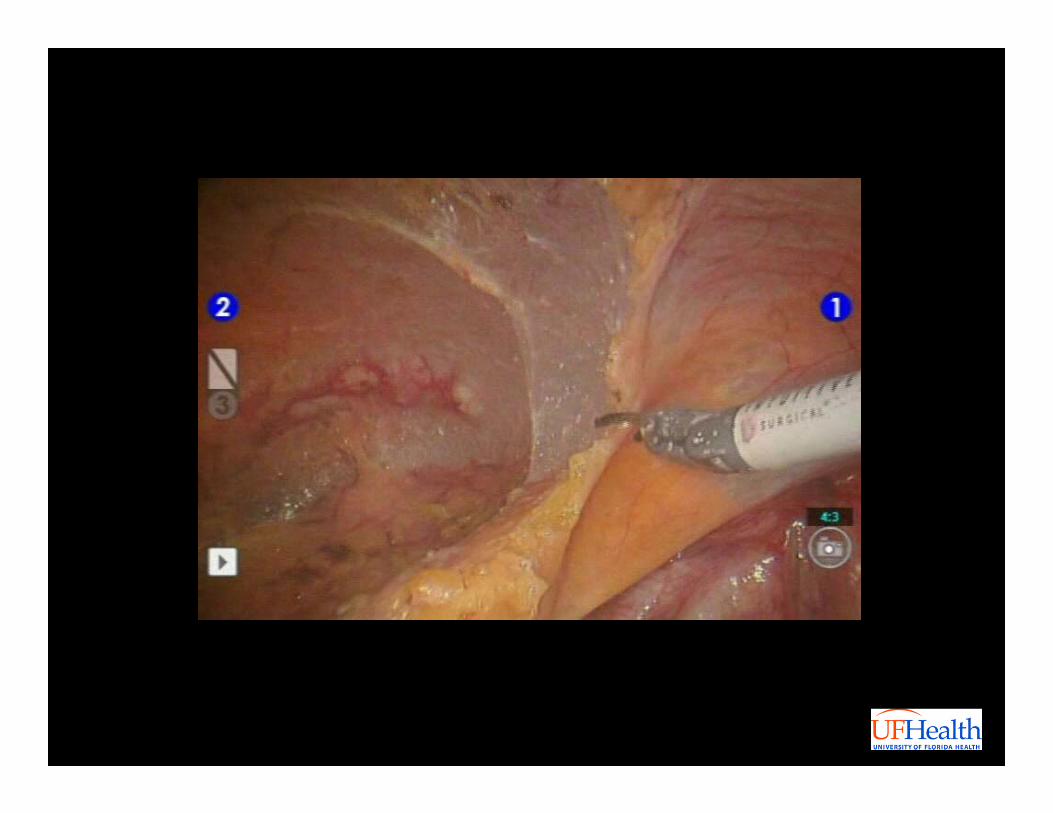
Dissection of Ureterovesical Junction
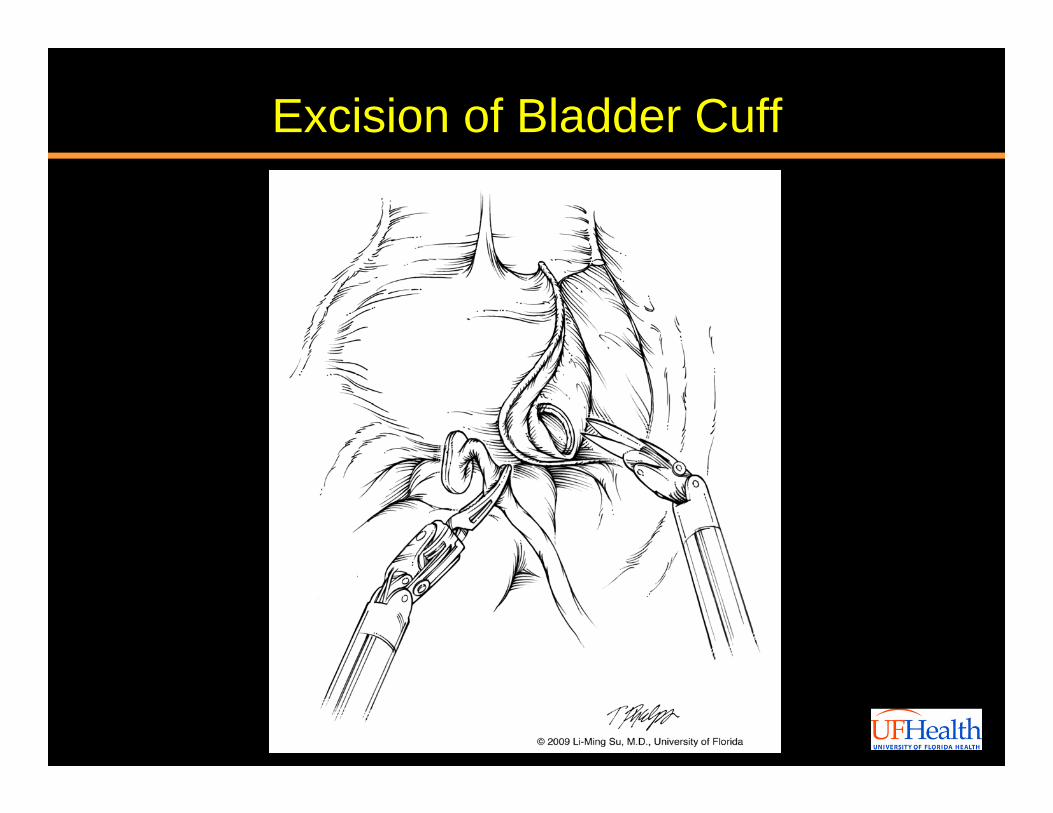
Excision of Bladder Cuff
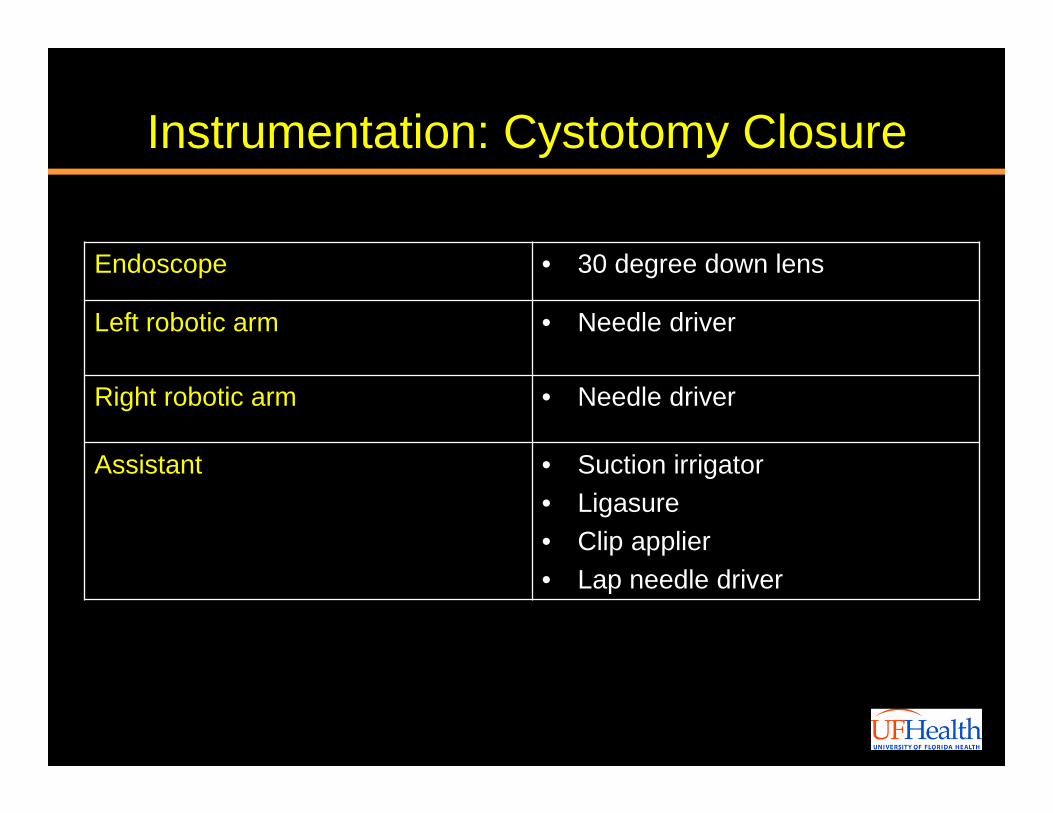
Instrumentation: Cystotomy Closure
Endoscope • 30 degree down lens
Left robotic arm • Needle driver
Right robotic arm • Needle driver
Assistant • Suction irrigator• Ligasure• Clip applier• Lap needle driver
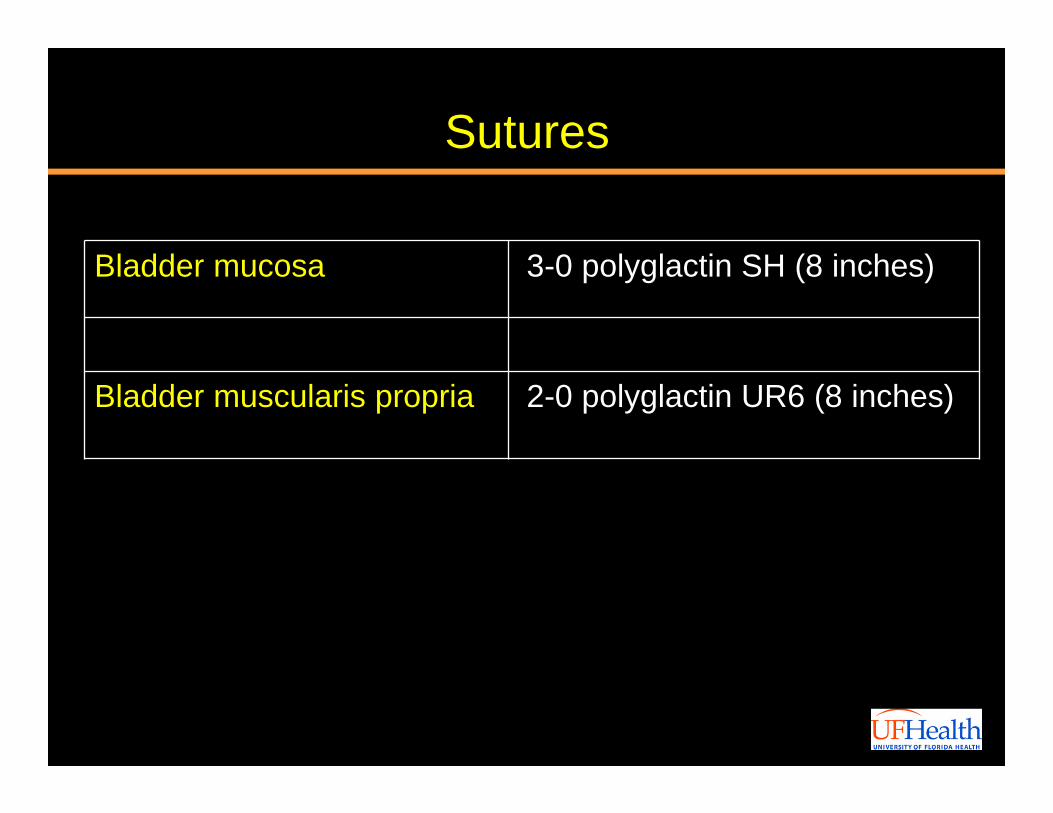
Sutures
Bladder mucosa 3-0 polyglactin SH (8 inches)
Bladder muscularis propria 2-0 polyglactin UR6 (8 inches)
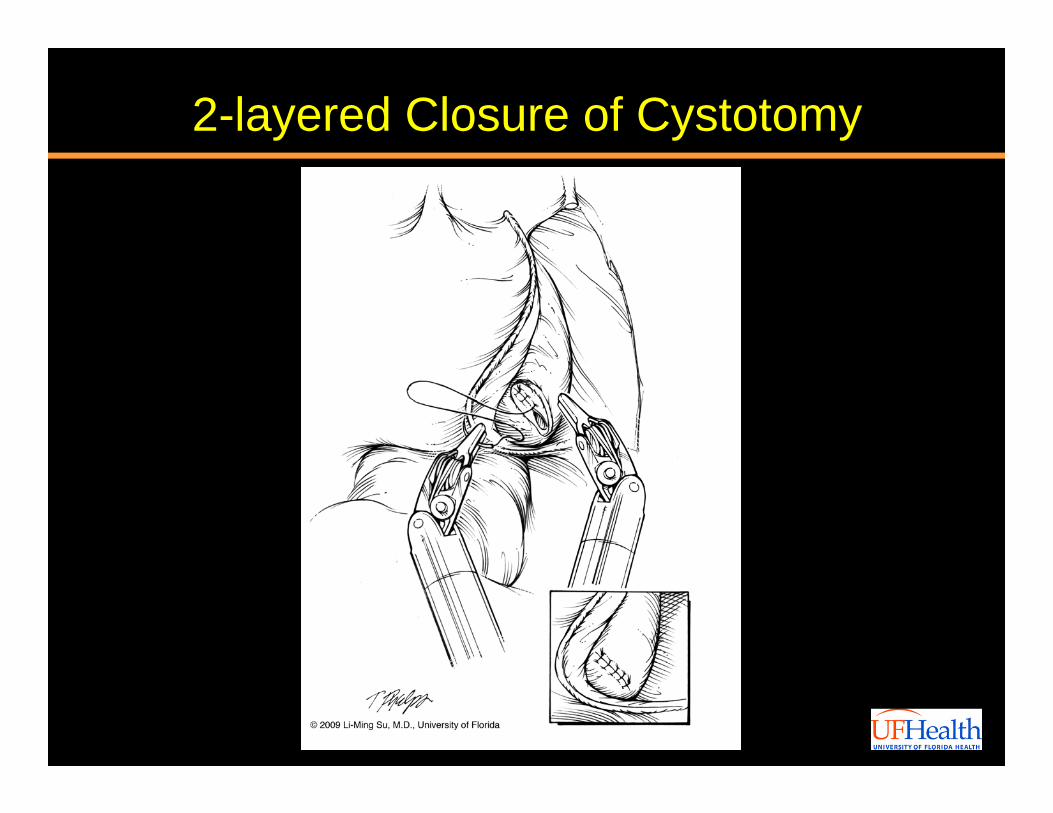
2-layered Closure of Cystotomy
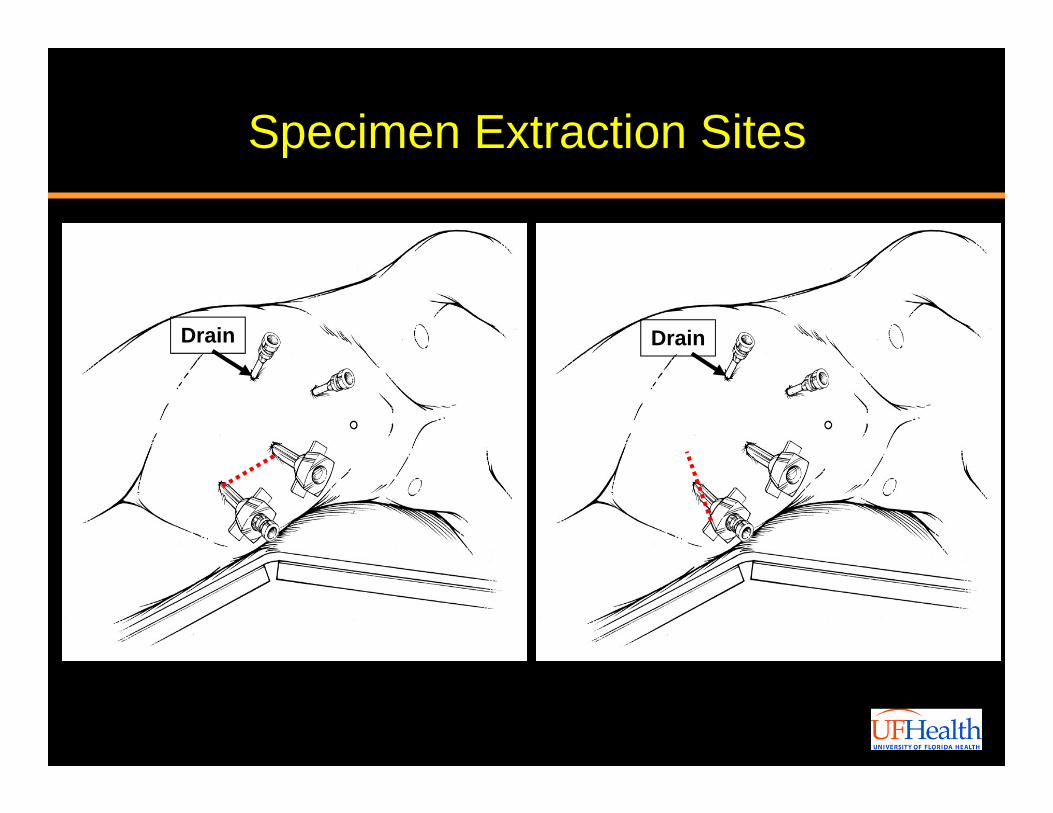
Specimen Extraction Sites
Drain Drain
Case Presentation
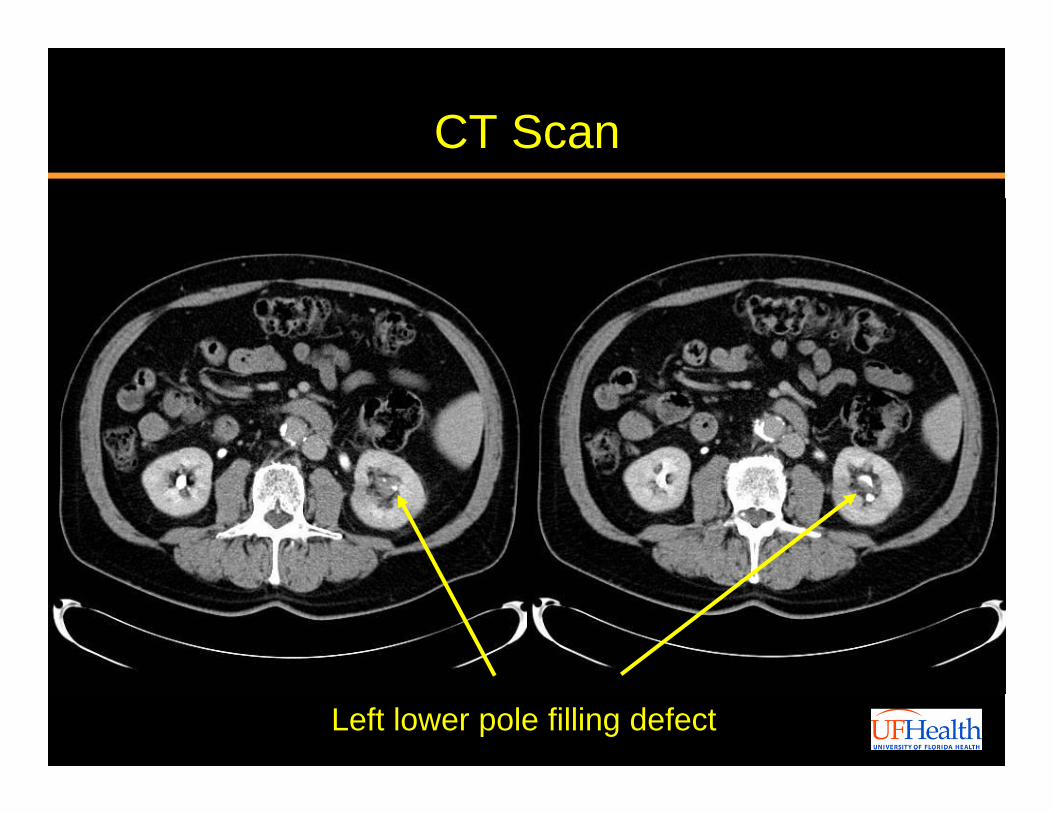
CT Scan
Left lower pole filling defect
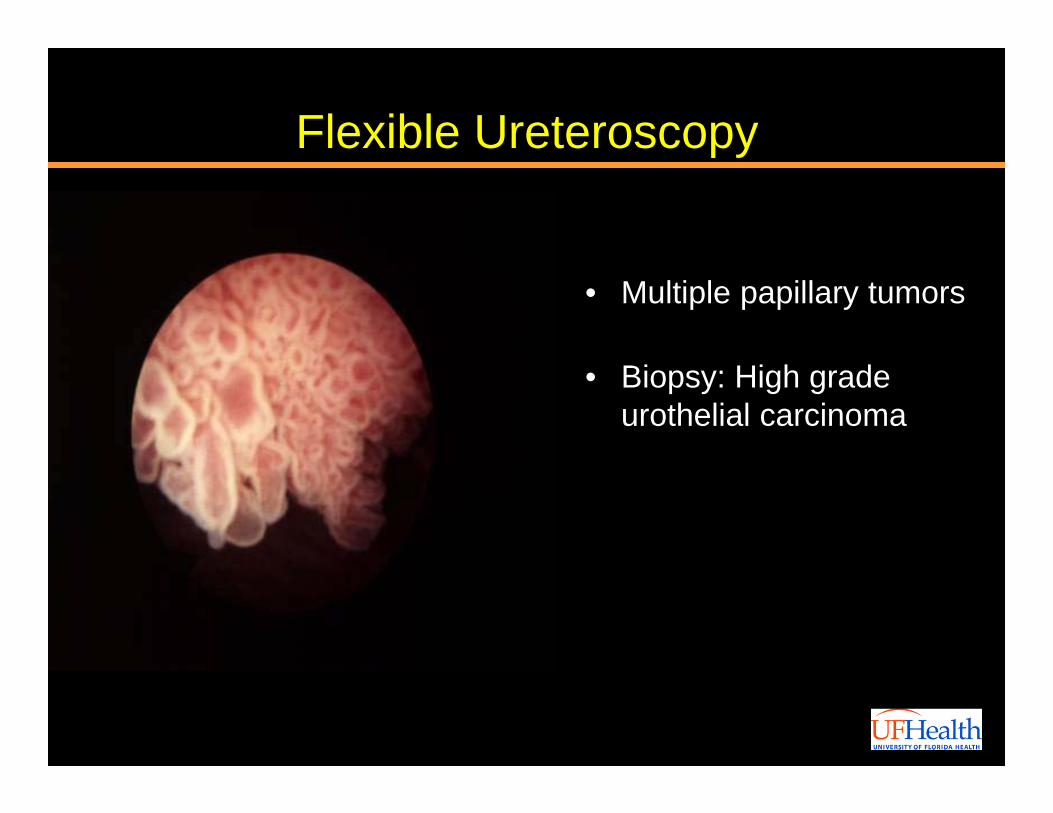
Flexible Ureteroscopy
• Multiple papillary tumors
• Biopsy: High grade urothelial carcinoma
Video: Robotic Nephrectomy

Video: Robotic Distal Ureterectomy and Bladder Cuff
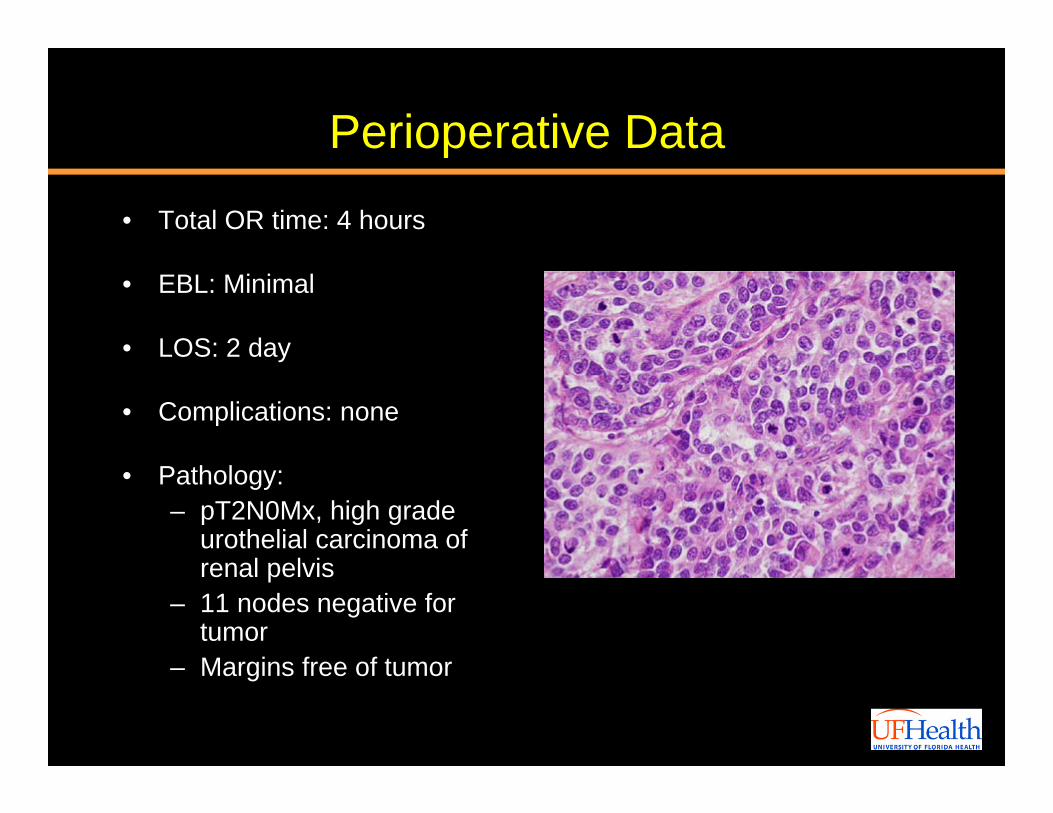
Perioperative Data
• Total OR time: 4 hours
• EBL: Minimal
• LOS: 2 day
• Complications: none
• Pathology: – pT2N0Mx, high grade
urothelial carcinoma of renal pelvis
– 11 nodes negative for tumor
– Margins free of tumor
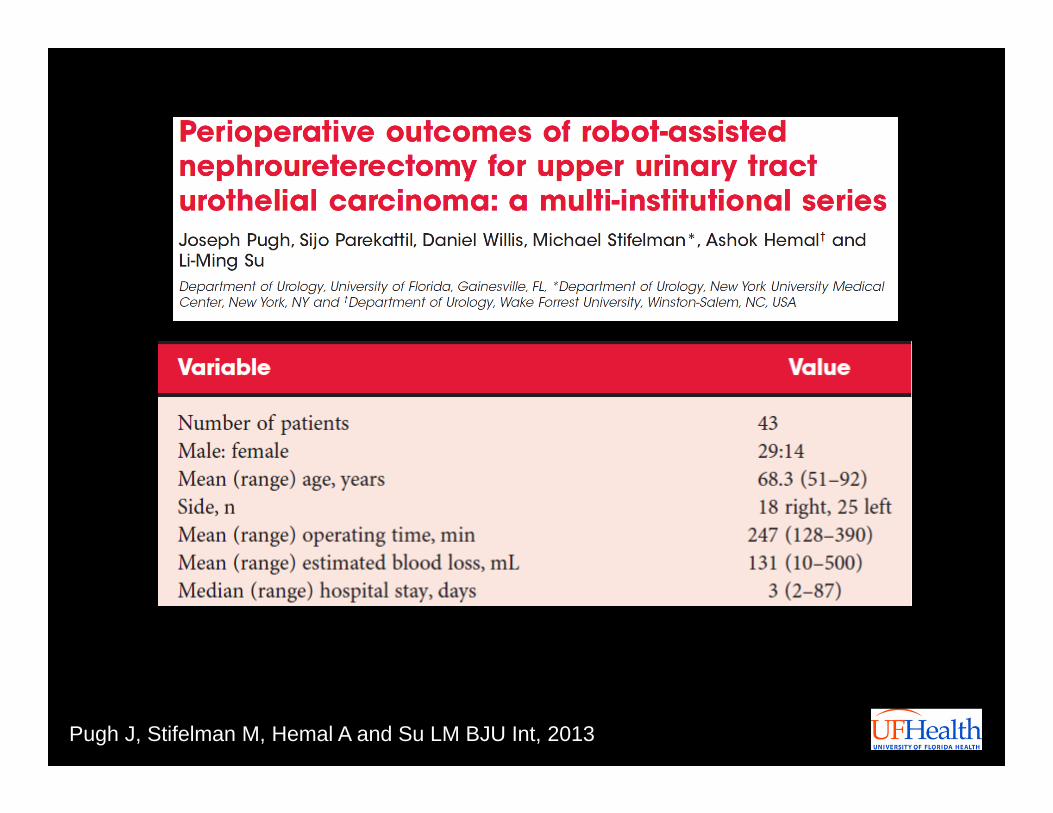
Pugh J, Stifelman M, Hemal A and Su LM BJU Int, 2013
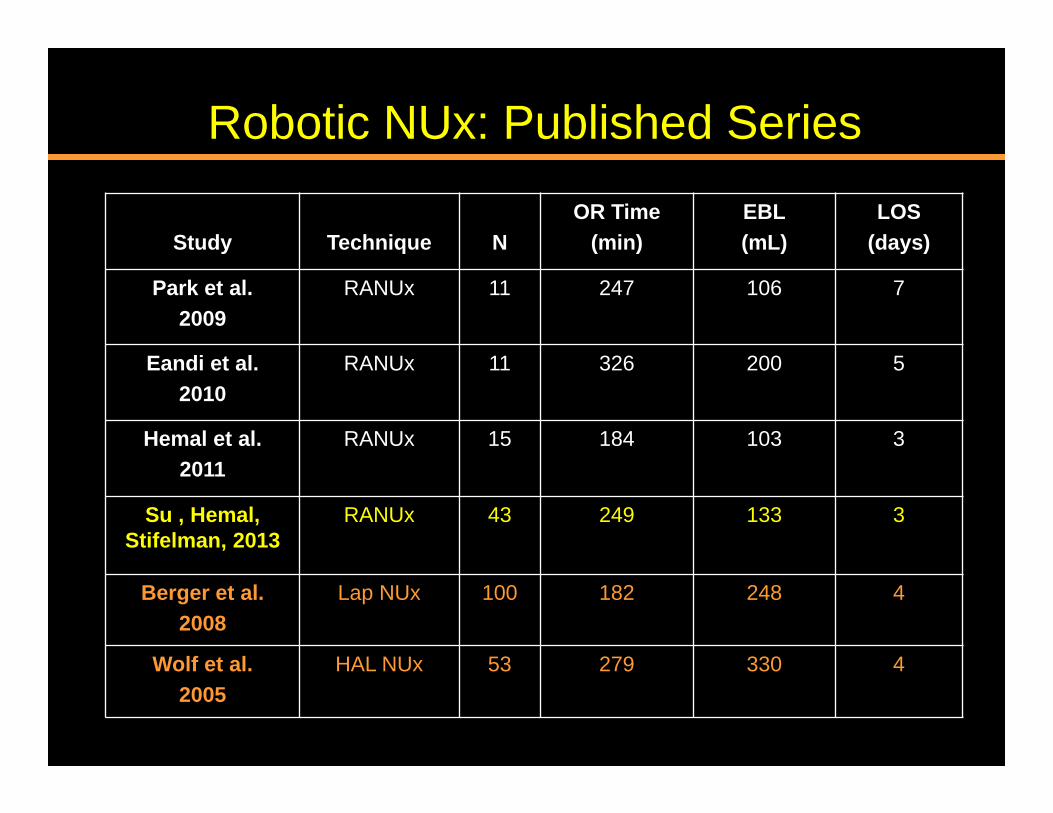
Robotic NUx: Published Series
Study Technique NOR Time
(min)EBL(mL)
LOS(days)
Park et al.2009
RANUx 11 247 106 7
Eandi et al.2010
RANUx 11 326 200 5
Hemal et al.2011
RANUx 15 184 103 3
Su , Hemal, Stifelman, 2013
RANUx 43 249 133 3
Berger et al.2008
Lap NUx 100 182 248 4
Wolf et al.2005
HAL NUx 53 279 330 4
Pugh J, Stifelman M, Hemal A and Su LM BJU Int, 2013
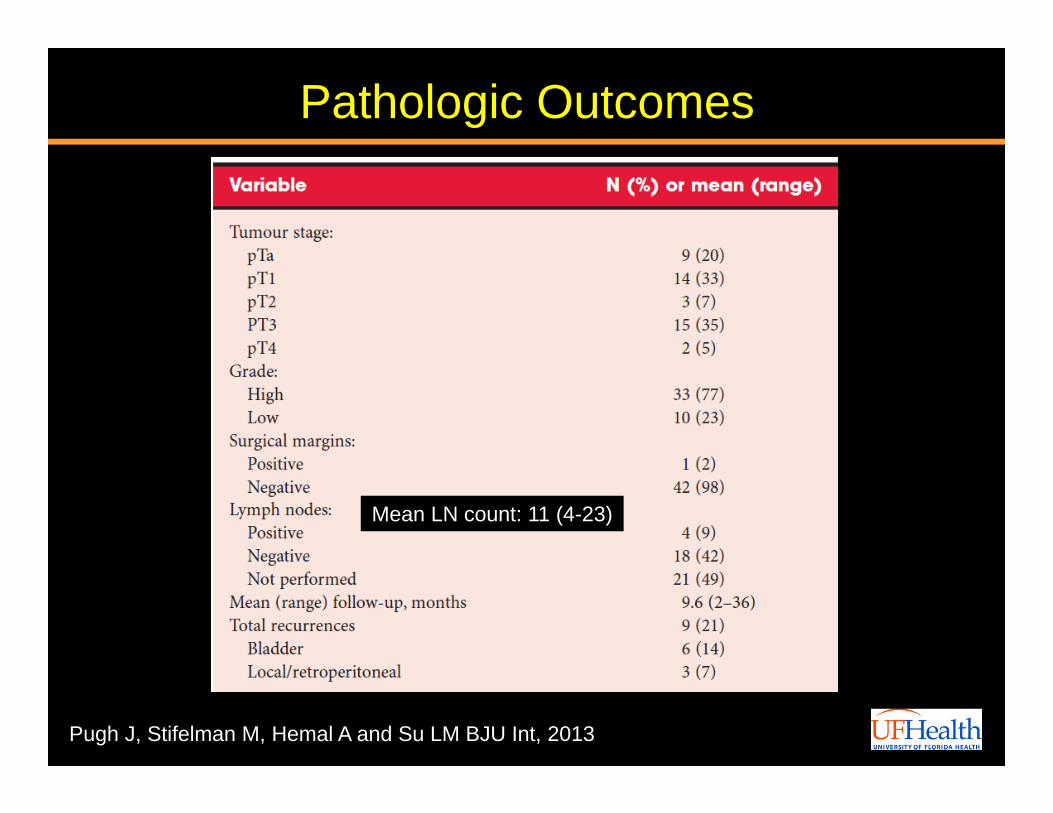
Mean LN count: 11 (4-23)
Pathologic Outcomes
Pugh J, Stifelman M, Hemal A and Su LM BJU Int, 2013
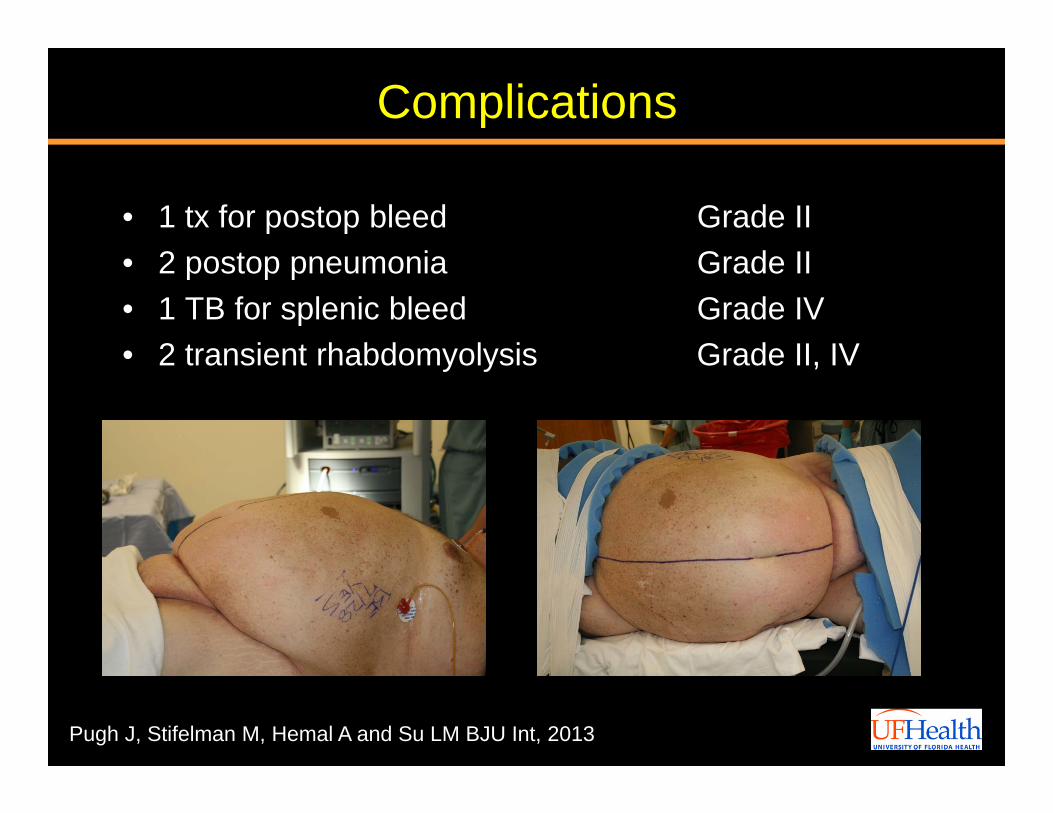
Complications
• 1 tx for postop bleed Grade II• 2 postop pneumonia Grade II• 1 TB for splenic bleed Grade IV• 2 transient rhabdomyolysis Grade II, IV
Video: Robotic Psoas Hitch
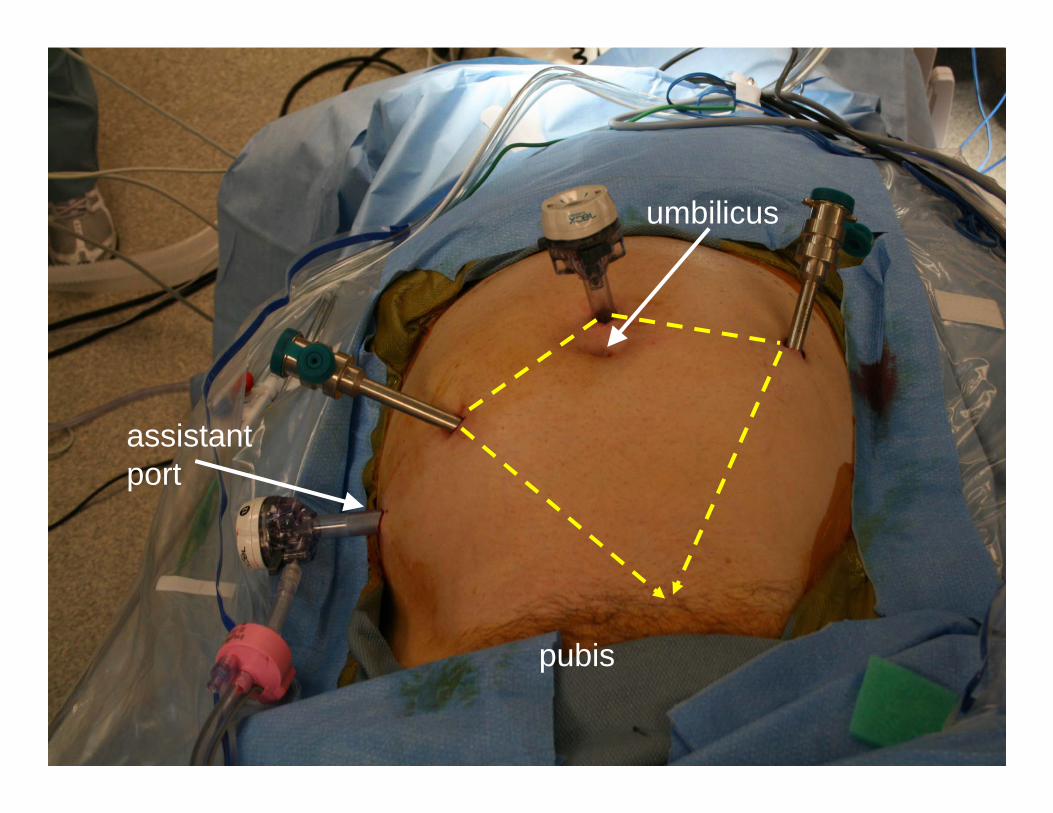
pubis
umbilicus
assistantport
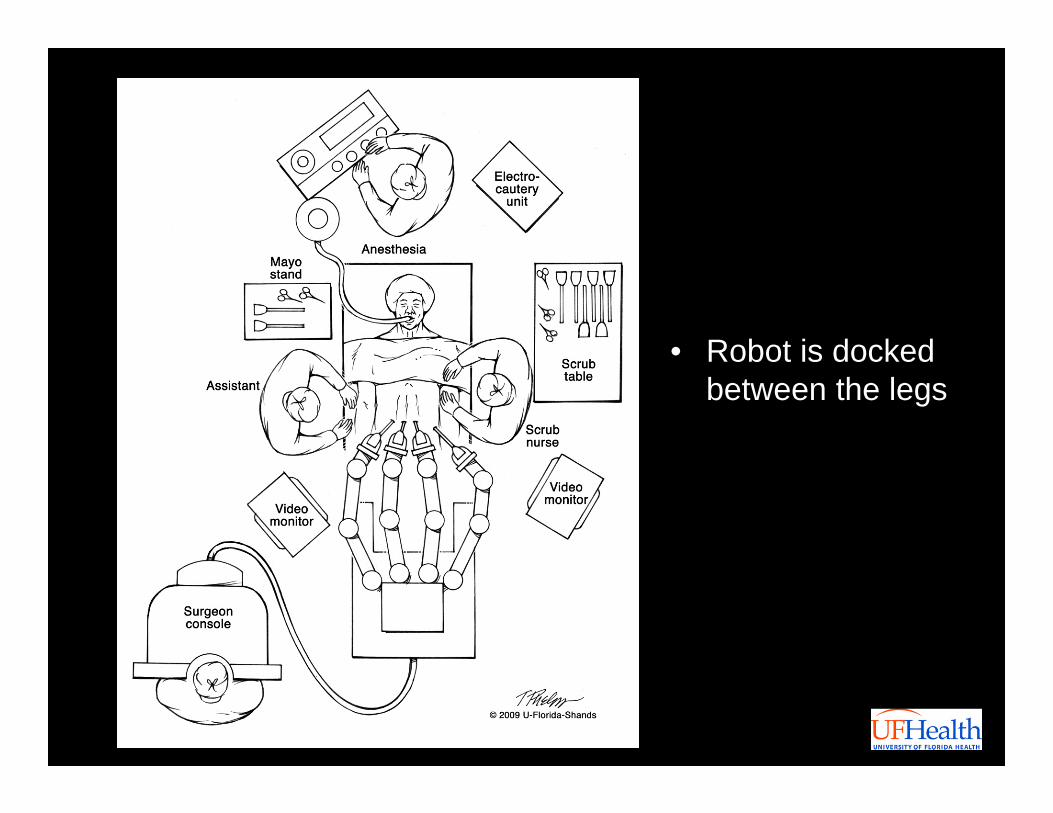
• Robot is docked between the legs
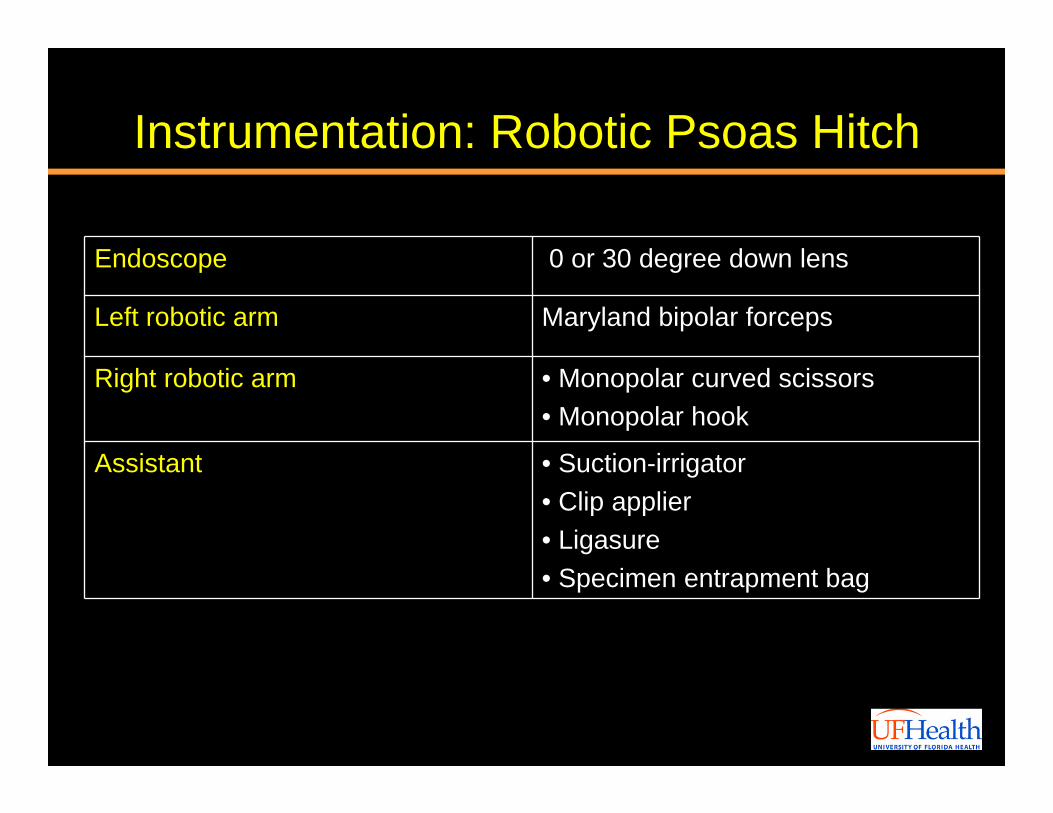
Instrumentation: Robotic Psoas Hitch
Endoscope 0 or 30 degree down lens
Left robotic arm Maryland bipolar forceps
Right robotic arm • Monopolar curved scissors• Monopolar hook
Assistant • Suction-irrigator• Clip applier• Ligasure• Specimen entrapment bag
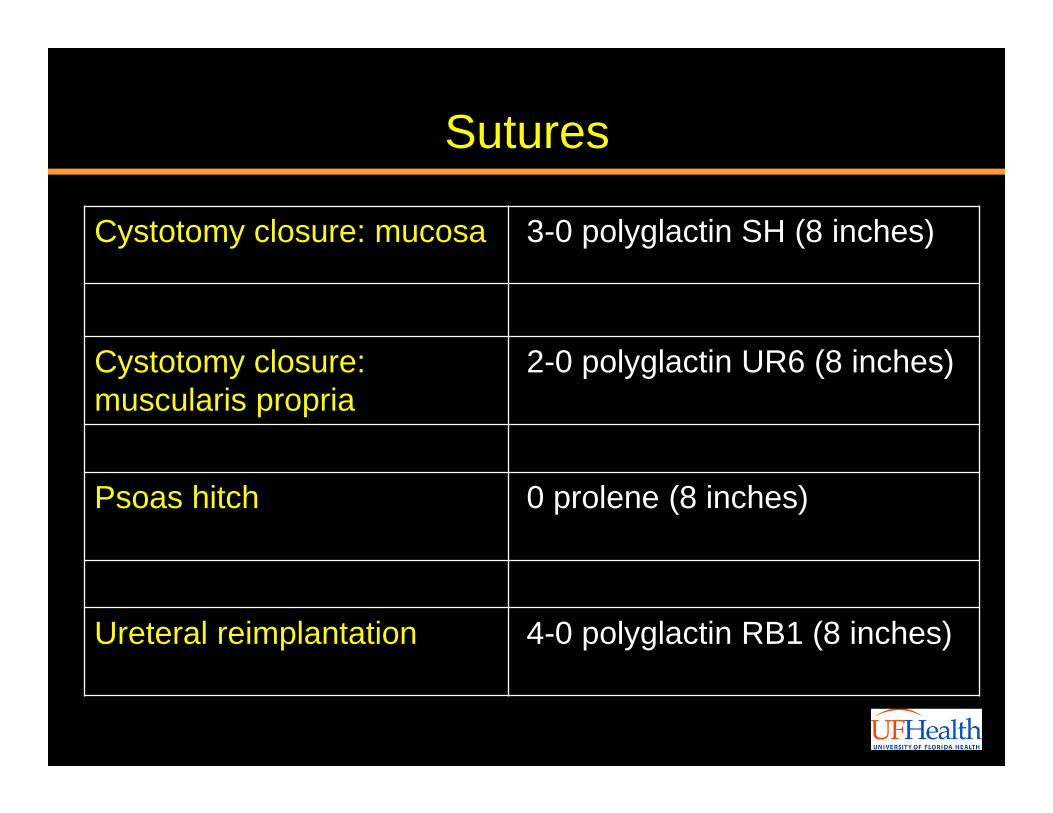
Sutures
Cystotomy closure: mucosa 3-0 polyglactin SH (8 inches)
Cystotomy closure: muscularis propria
2-0 polyglactin UR6 (8 inches)
Psoas hitch 0 prolene (8 inches)
Ureteral reimplantation 4-0 polyglactin RB1 (8 inches)
ConclusionsRobotic nephroureterectomy and distal ureterectomy
– Easy techniques to adopt esp. for experienced robotic teams
• Simplifies bladder cuff dissection
• Avoids a second cystotomy
• Favorable ergonomics esp. suturing as compared to laparoscopic
– May serve as a stepping stone towards performing robotic partial NTx
– Similar perioperative outcomes to conventional laparoscopic techniques
– Longer oncologic followup required
Thank You
Recommended







![Review Article - ICUrology · increase the detection rate of upper urinary tract urothelial malignancy [12]. Deflecting mechanisms have been greatly developed as well. Deflection](https://img.pdfslide.us/doc/110x75/5fab4c986a0cb04a8817ec9b/review-article-increase-the-detection-rate-of-upper-urinary-tract-urothelial-malignancy.jpg)