Respiratory System Disorders 4
Lecture 26
Pathology and Clinical
Science 1 (BIOC211)
Department of BioscienceText Reference:
Porth’s Pathophysiology: Concepts of Altered Health States
Sheila C. Grossman & Carol Mattson Porth.
Ninth Edition.
Copyright © 2014 Lippincott, Williams & Wilkins Publishers, Inc.
© endeavour.edu.au
© Endeavour College of Natural Health endeavour.edu.au 2
SESSION LEARNING
OUTCOMES o This session explains the aetiology, pathophysiology,
clinical features, investigations and management of
diseases of the respiratory system.
o It aims to understand the following respiratory infections
• Lung cancers
• Interstitial pulmonary disease
• Sarcoidosis
• Lung diseases caused by organic and inorganic dusts
• Alveolitis
• Vascular diseases
© Endeavour College of Natural Health endeavour.edu.au 3
TUMOURS OF THE BRONCHUS
AND LUNG
Introduction
• Lung cancer is the most common cancer
worldwide (1.2 million new cases in 2000 & 18%
of cancer death)
• Tobacco use is the major preventable cause
• Majority of tumours in the lung are primary
bronchial carcinoma
• The lung is also a common site of secondary
metastatic carcinoma
© Endeavour College of Natural Health endeavour.edu.au 4
PRIMARY TUMOURS
OF THE LUNGAetiology
• Cigarette smoking most common and though to be responsible for 90% of lung carcinomas
• Risk proportional to amount smoked and tar content
• Passive smoking though to be a factor in 5% of lung cancers though difficult to quantify
• Other risk factors – exposure to naturally occurring radon, atmospheric pollution and occupation dealing with some industrial products e.g. asbestos, cadmium
© Endeavour College of Natural Health endeavour.edu.au 5
BRONCHIAL CARCINOMA
Pathophysiology
o Arise from either bronchial epithelium or mucous gland
o Common cell types are squamous 35%,
adenocarcinoma 30%, small cell and large cell
o Onset of symptoms is dependent on cell types &
position
within the bronchus
o Can directly involve the pleura or by lymphatic spread
o Blood-borne metastasis occur mainly to liver, bone,
brain, adrenals and skin
© Endeavour College of Natural Health endeavour.edu.au 6
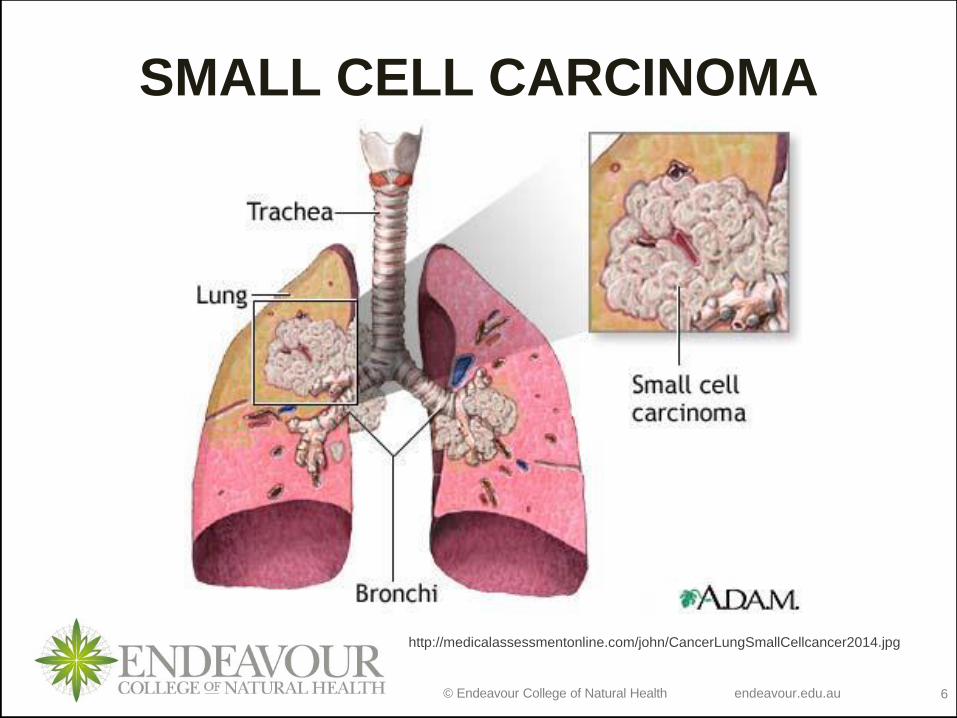
SMALL CELL CARCINOMA
http://medicalassessmentonline.com/john/CancerLungSmallCellcancer2014.jpg
© Endeavour College of Natural Health endeavour.edu.au 7
BRONCHIAL CARCINOMA
Clinical features
• Cough (dry or with sputum)
• Haemoptysis
• Bronchial obstruction
– complete or partial
– with or without infection
• Breathlessness
• Pleural pain
• Symptoms due to blood-borne metastasis
• Non-metastatic extrapulmonary manifestations
© Endeavour College of Natural Health endeavour.edu.au 8
BRONCHIAL CARCINOMA
Investigations
• Chest X ray
• CT
• Bronchoscopy and biopsy
Management
• Surgical resection
• Radiotherapy
• Chemotherapy
• Palliative
Prognosis
• Very poor (5 year survival less than 6%)
© Endeavour College of Natural Health endeavour.edu.au 9
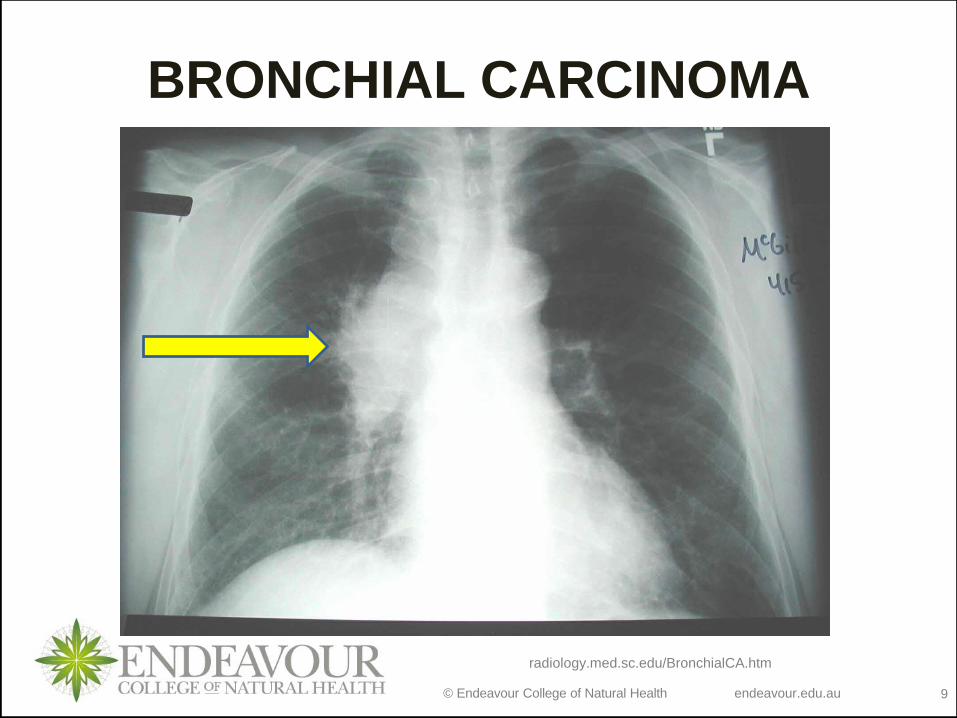
BRONCHIAL CARCINOMA
radiology.med.sc.edu/BronchialCA.htm
© Endeavour College of Natural Health endeavour.edu.au 10
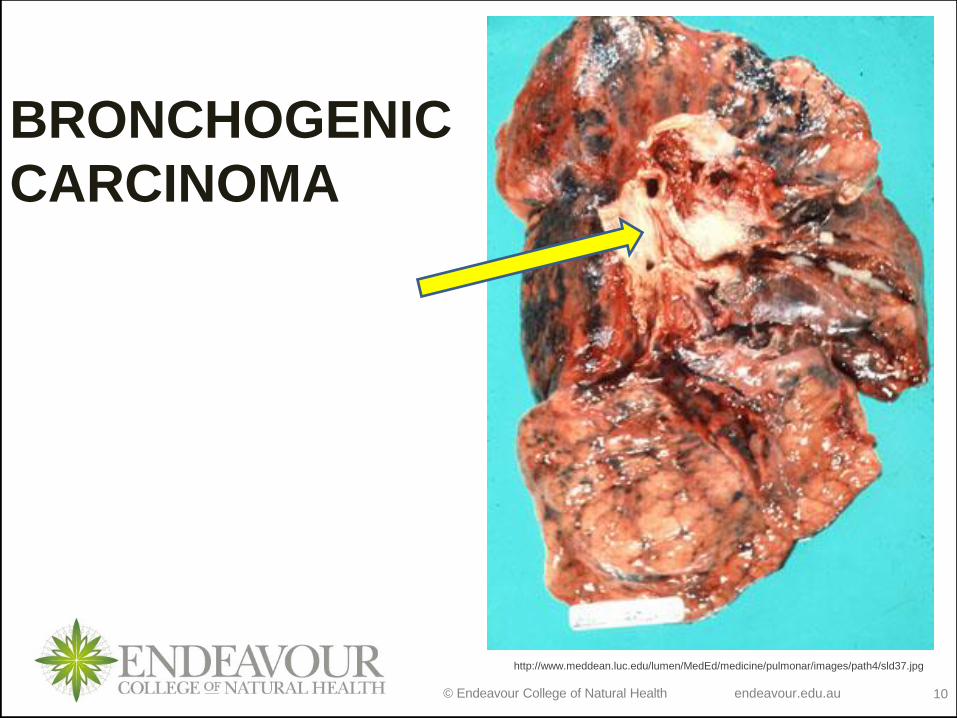
BRONCHOGENIC
CARCINOMA
http://www.meddean.luc.edu/lumen/MedEd/medicine/pulmonar/images/path4/sld37.jpg
© Endeavour College of Natural Health endeavour.edu.au 11
SECONDARY TUMOURS
OF THE LUNGo Blood-borne metastatic pulmonary
deposits from breast, kidney, uterus, ovary,
testes and thyroid
o Deposits are usually multiple and bilateral
o There are respiratory symptoms e. g.
breathlessness
o Diagnosis is made by radiological
examination
© Endeavour College of Natural Health endeavour.edu.au 12
INTERSTITIAL & INFILTRATIVE
PULMONARY DISEASESDiffuse parenchymal lung disease (DPLDs)
• Heterogeneous group of conditions associated with diffused thickening of the alveolar walls with inflammatory cells and exudates
• Include
–Acute respiratory distress syndrome
–Granulomas ( e.g. sarcoidosis )
–Alveolar haemorrhage and fibrosis
• Lung disease alone or part of systemic connective tissue disorder
© Endeavour College of Natural Health endeavour.edu.au 13
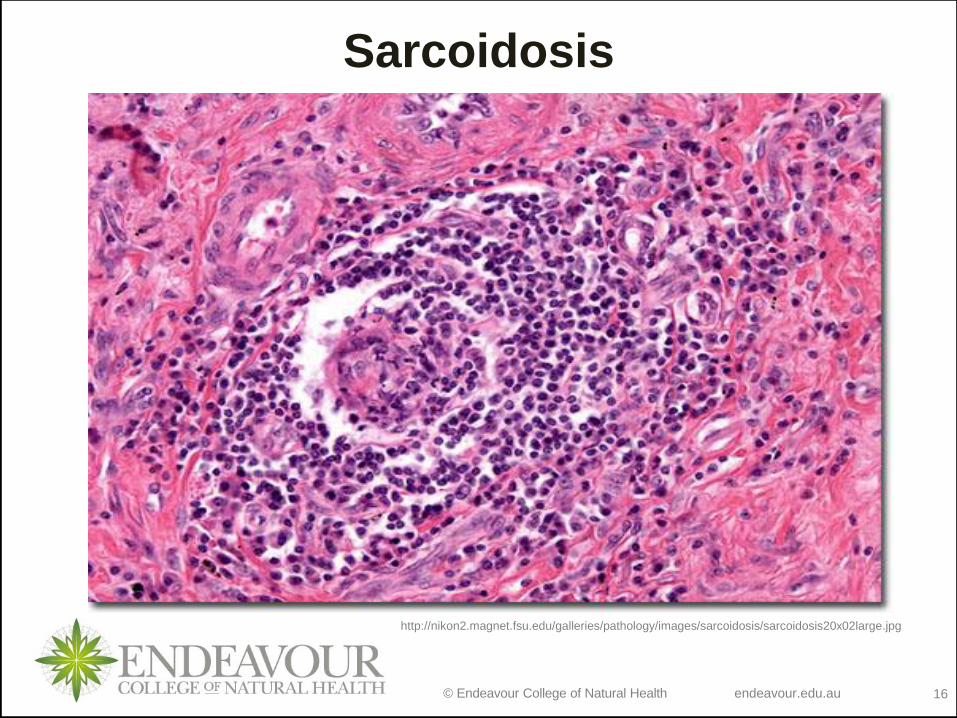
SARCOIDOSIS o Multisystem granulomatous disorder
o More commonly seen in colder parts of Northern Europe
Aetiology – uncertain
Pathology
• Granulomas mostly in mediastinal and superficial lymph nodes, lungs, liver, spleen, skin, eyes, parotid glands and phalangeal bones
Clinical features
• Asymptomatic
• Lofgren’s syndrome in young women
• Respiratory symptoms
• Skin lesions
• Lymphadenopathy
© Endeavour College of Natural Health endeavour.edu.au 14
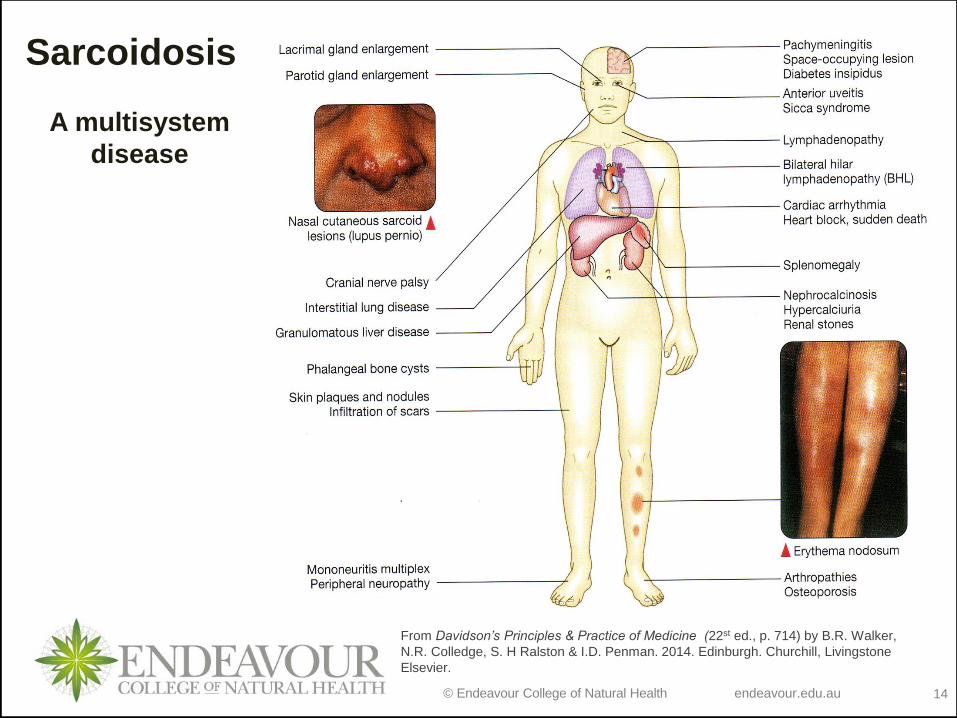
From Davidson’s Principles & Practice of Medicine (22st ed., p. 714) by B.R. Walker,
N.R. Colledge, S. H Ralston & I.D. Penman. 2014. Edinburgh. Churchill, Livingstone
Elsevier.
Sarcoidosis
A multisystem
disease
© Endeavour College of Natural Health endeavour.edu.au 15
SARCOIDOSIS
Investigation
• Blood tests, liver function tests
• Chest X ray
• Bronchoscopy and biopsy
Management
• Majority – spontaneous remission
• NSAIDs and corticosteroids
Prognosis
• Overall mortality low 1-5%
© Endeavour College of Natural Health endeavour.edu.au 16
Sarcoidosis
http://nikon2.magnet.fsu.edu/galleries/pathology/images/sarcoidosis/sarcoidosis20x02large.jpg
© Endeavour College of Natural Health endeavour.edu.au 17
LUNG DISEASES DUE TO
ORGANIC DUSTS
o Disease results from a local immune response to animal proteins or fungal antigens in mouldyvegetable matter
o Some examples
• Farmer’s lung (mouldy hay, straw, grain)
• Bird fancier’s lung (avian excreta, feathers)
• Malt worker’s lung
• Cheese worker’s lung (mouldy cheese)
o Most commonly presented as hypersensitivity pneumonitis
© Endeavour College of Natural Health endeavour.edu.au 18
HYPERSENSITIVITY PNEUMONITIS
(EXTRINSIC ALLERGIC ALVEOLITIS)
Pathogenesis
• Inhalation of certain types of organic dusts → diffuse immune complex reactions (Type III & type IV) in the walls of alveoli and bronchioles
• Chronic forms may lead to fibrosis
Clinical features
• History of exposure
• Flu-like symptoms – headache, myalgia, malaise, fever, dry cough, breathlessness
© Endeavour College of Natural Health endeavour.edu.au 19
HYPERSENSITIVITY PNEUMONITIS
(EXTRINSIC ALLERGIC ALVEOLITIS)
Investigations
• Chest X ray
• HRCT
• Pulmonary function tests
• Blood test – presence of antibodies to offending antigen
Management
• Removal of antigen or dust masks with appropriate filters
• Steroids
• Oxygen therapy in severely hypoxic patients
© Endeavour College of Natural Health endeavour.edu.au 20
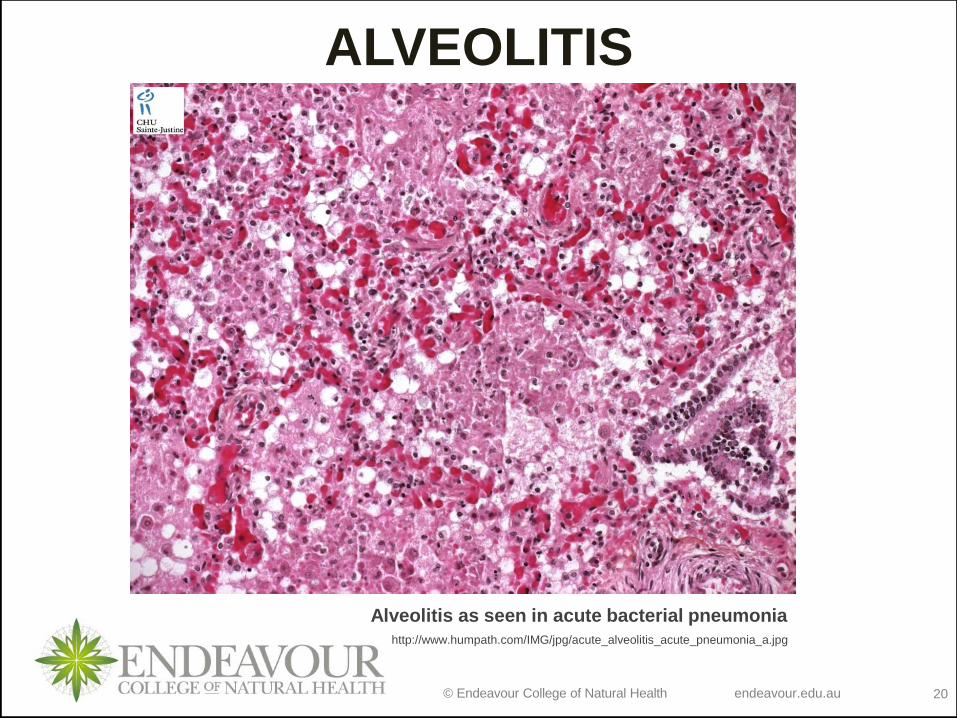
ALVEOLITIS
http://www.humpath.com/IMG/jpg/acute_alveolitis_acute_pneumonia_a.jpg
Alveolitis as seen in acute bacterial pneumonia
© Endeavour College of Natural Health endeavour.edu.au 21
LUNG DISEASES DUE TO
INORGANIC DUSTSo Specific pathological changes in the lungs due to
exposure to dusts, fumes or noxious substances
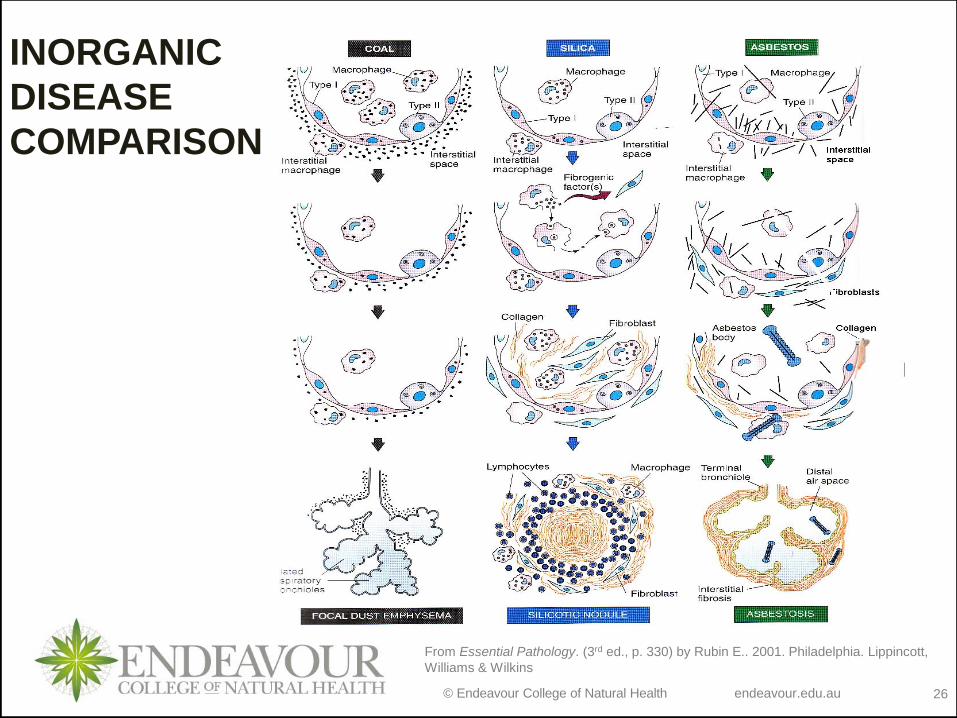
o Generally prolonged exposure to inorganic dusts leads to diffuse pulmonary fibrosis (pneumoconiosis)
o Damage is from the inflammatory and fibrotic response to the dust
o Generally a long period of exposure is required
o Exposure can lead to other lung diseases
o Need a detailed occupational case history
o Diagnose by history, radiological and pulmonary function abnormalities
o No specific treatment is available for this group of diseases
© Endeavour College of Natural Health endeavour.edu.au 22
LUNG DISEASES DUE TO
INORGANIC DUSTSCoal Workers Pneumoconiosis - Inhalation of coal dust
o Simple - does not progress after exposure is stopped
o Progressive - massive Fibrosis
• Disease is disabling, can shorten life expectancy and can progress even after exposure is stopped
• Associated with chronic bronchitis, cough and sputum
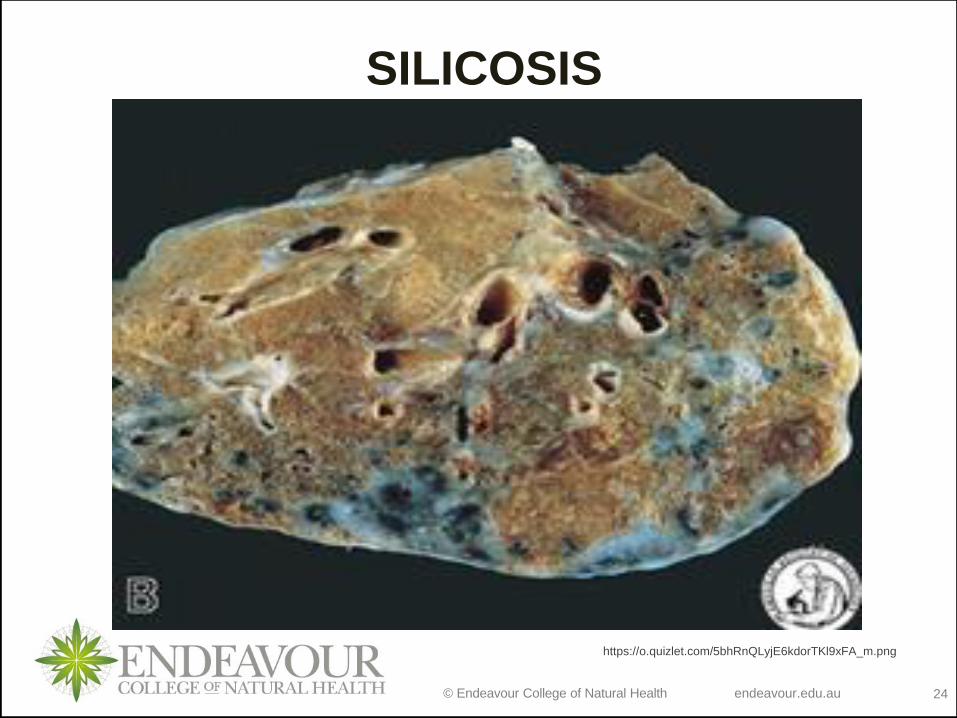
Silicosis - Inhalation of silica dust
o Clinical features similar to coal workers pneumoconiosis
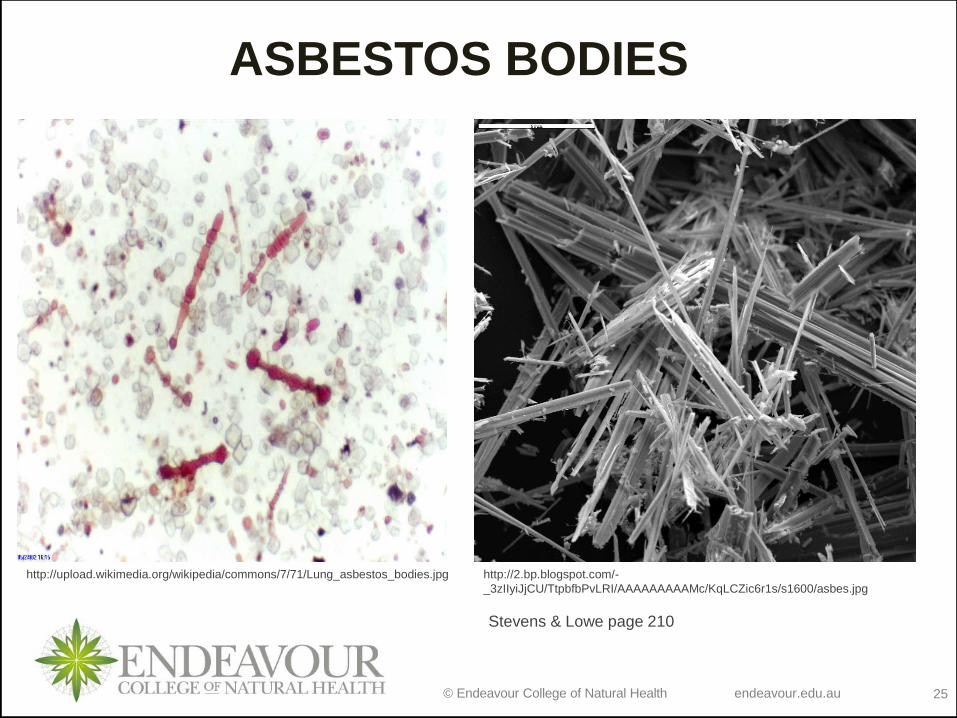
Asbestosis - Inhalation & exposure to asbestos dust
o Cause laryngeal carcinoma plus pleural and lung pathologies
o Decreases lung volumes and restricts ventilation of the lungs
o Usually progresses very slowly
© Endeavour College of Natural Health endeavour.edu.au 23
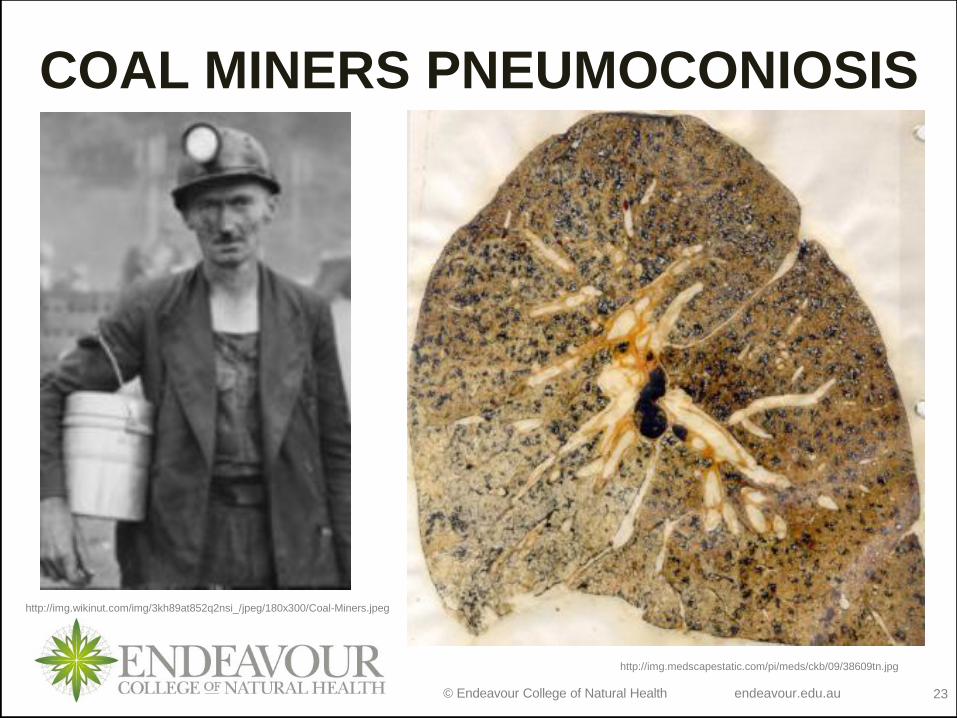
COAL MINERS PNEUMOCONIOSIS
Stevens & Lowe page 209
http://img.medscapestatic.com/pi/meds/ckb/09/38609tn.jpg
http://img.wikinut.com/img/3kh89at852q2nsi_/jpeg/180x300/Coal-Miners.jpeg
© Endeavour College of Natural Health endeavour.edu.au 24
SILICOSIS
https://o.quizlet.com/5bhRnQLyjE6kdorTKl9xFA_m.png
© Endeavour College of Natural Health endeavour.edu.au 25
ASBESTOS BODIES
Stevens & Lowe page 210
http://2.bp.blogspot.com/-
_3zIIyiJjCU/TtpbfbPvLRI/AAAAAAAAAMc/KqLCZic6r1s/s1600/asbes.jpg
http://upload.wikimedia.org/wikipedia/commons/7/71/Lung_asbestos_bodies.jpg
© Endeavour College of Natural Health endeavour.edu.au 26
From Essential Pathology. (3rd ed., p. 330) by Rubin E.. 2001. Philadelphia. Lippincott,
Williams & Wilkins
INORGANIC
DISEASE
COMPARISON
© Endeavour College of Natural Health endeavour.edu.au 27
PULMONARY VASCULAR
DISEASE
Venous thromboembolism (VTE)
• Majority ( 75% )of pulmonary emboli arise from lower limb DVT
• Risk factors – surgery, pregnancy, cardiopulmonary disease, lower limb problem, malignant disease
• Pathophysiology
– Based on size of the embolus
– Acute massive, acute small or medium, chronic multiple micro emboli
– Causes blockage or blood vessels in the lungs preventing the effective exchange of gases
– Leads to hypoxia and hypercapnia
© Endeavour College of Natural Health endeavour.edu.au 28
VENOUS THROMBOEMBOLISM
(VTE)
Clinical features
• Depend on size of embolism and underlying
disease
• Range from small emboli with few or no
haemodynamic consequences to
cardiovascular collapse
• Usually chest pain, dyspnoea, haemoptysis,
fainting
© Endeavour College of Natural Health endeavour.edu.au 29
VENOUS THROMBOEMBOLISMInvestigations
• Chest X-ray
• ECG
• Arterial blood gas analysis
• Ventilation perfusion scanning
• Echocardiography
• Pulmonary angiograph
Management
• General measure – pain relief, oxygen, resuscitation
• Anticoagulants
• Thrombolytic therapy
© Endeavour College of Natural Health endeavour.edu.au 30
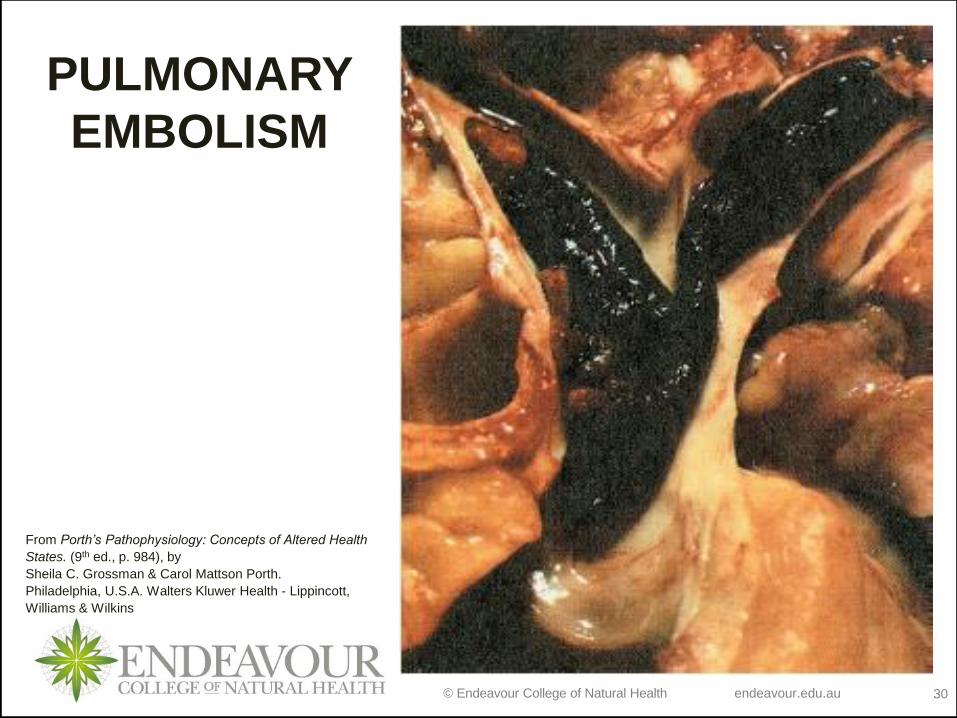
PULMONARY
EMBOLISM
From Porth’s Pathophysiology: Concepts of Altered Health
States. (9th ed., p. 984), by
Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott,
Williams & Wilkins
© Endeavour College of Natural Health endeavour.edu.au 31
DISEASES OF THE PLEURA
Pleurisy
o Term for any disease that involves the
pleura and leads to pleural pain or friction
• Common in pulmonary infarction, TB or
Tumour
• Clinical features are dependent on the
nature of the disease causing the pain
© Endeavour College of Natural Health endeavour.edu.au 32
EMPYEMA
o The presence of pus in the pleural space (Thin like serous fluid or Incredibly thick)
o Generally unilateral – involving the whole or part of a lung
o Always secondary - generally to infection of the lung
o Bacterial pneumonia and TB
Pathophysiology
o The pleura becomes covered with a thick shaggy inflammatory exudate
o The pus is generally under pressure and can erupt into a bronchus if not treated
© Endeavour College of Natural Health endeavour.edu.au 33
EMPYEMA
Clinical Features
o Persistent recurrent pyrexia in a patient already diagnosed with lung infection particularly if antibiotic treatment is being given
Treatment and Management
o Dependent of the underlying cause
© Endeavour College of Natural Health endeavour.edu.au 34
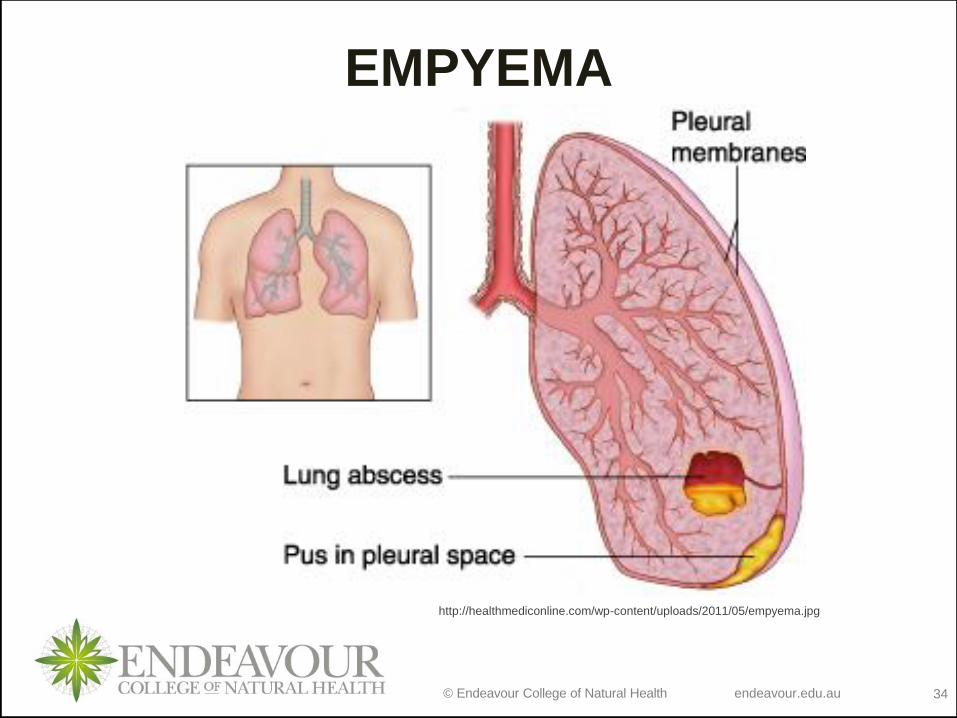
EMPYEMA
http://healthmediconline.com/wp-content/uploads/2011/05/empyema.jpg
© Endeavour College of Natural Health endeavour.edu.au 35
SPONTANEOUS PNEUMOTHORAXPresence of air in the pleural space
Causes
o Rupture of a sub pleural emphysematous bulla or pleural bleb
o Rupture of a sub pleural tuberculoses focu
Pathophysiology
o Closed - No communication between the pleura and lungs with deflation
o Open - Communication between the lungs and the pleural space generally through a bronchus
o Tension / Valvular
• Communication present but small and only allows movement of air in one direction
© Endeavour College of Natural Health endeavour.edu.au 36
SPONTANEOUS PNEUMOTHORAX
Clinical Features
o Onset generally rapid, may present with infection
o Pain or tightness on the affected side of the chest
aggravated by deep breathing and dependent on the size of the pneumothorax and the type
o Breathlessness and cyanosis
o Hyper-resonance on percussion and increased vocal resonance
Treatment and Management
o Bed rest
o Infection must be countered in open pneumothorax
o Valvular pneumothorax can be extreme resulting in death within minutes though generally time for medical intervention
© Endeavour College of Natural Health endeavour.edu.au 37
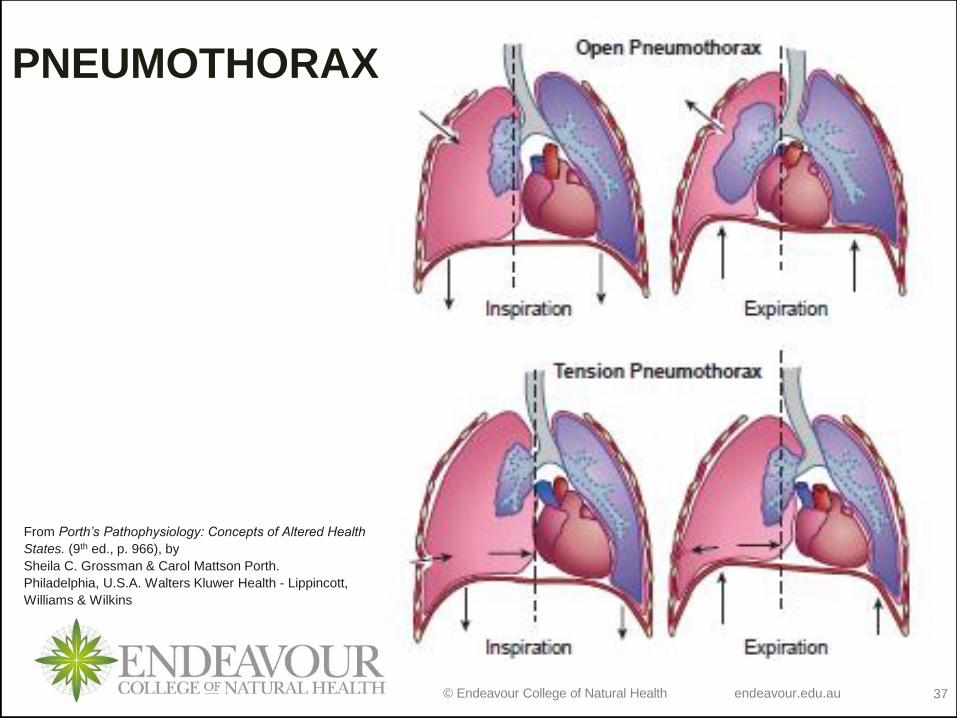
PNEUMOTHORAX
From Porth’s Pathophysiology: Concepts of Altered Health
States. (9th ed., p. 966), by
Sheila C. Grossman & Carol Mattson Porth.
Philadelphia, U.S.A. Walters Kluwer Health - Lippincott,
Williams & Wilkins
© Endeavour College of Natural Health endeavour.edu.au 38
CONGENITAL DISORDERS OF
THE DIAPHRAGM
Diaphragmatic Hernias
o Defects of the diaphragm allowing herniation of the abdominal viscera. More commonly found towards the posterior aspect
Eventration of the diaphragm
o Abnormal elevation or bulging of one hemidiaphragm
o Usually asymptomatic
© Endeavour College of Natural Health endeavour.edu.au 39
ACQUIRED DISORDERS
OF THE DIAPHRAGMDiaphragmatic Paralysis
• Generally through phrenic nerve damage to one hemi-
diaphragm
Clinical Features
• Loss of ventilatory capacity (20%)
• Generally asymptomatic in a healthy individual
Causes
• Bronchial carcinoma
• Injury or disease of the cervical vertebrae including birth
injuries, surgery and aneurysms

© Endeavour College of Natural Health endeavour.edu.au 40
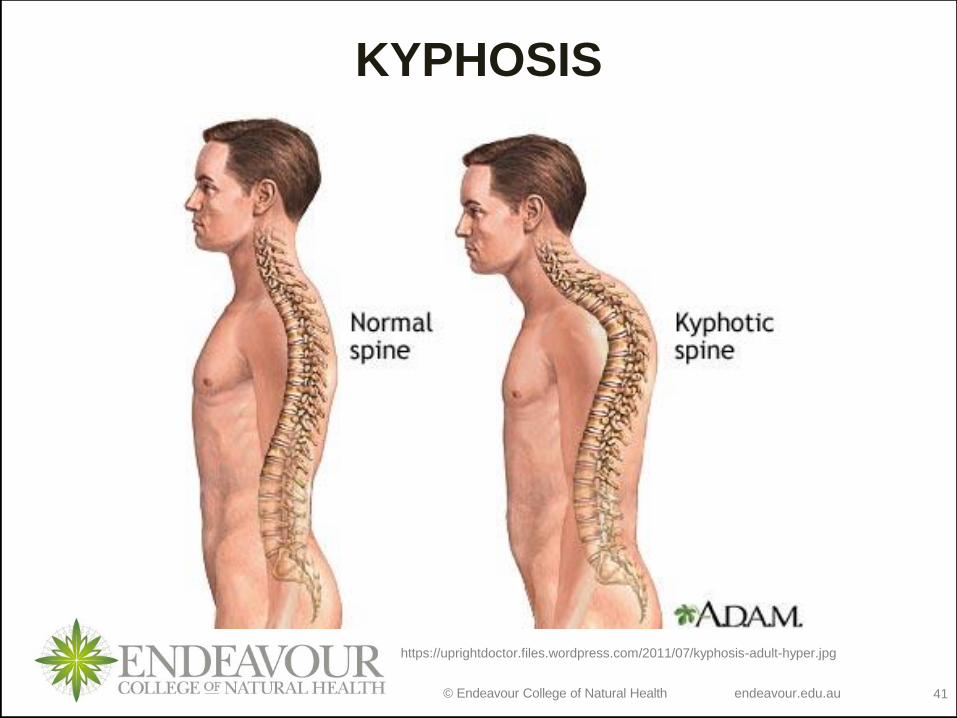
DEFORMITIES OF
THE CHEST WALL
Thoracic Kyphoscoliosis
Abnormalities of alignment of the dorsal spine
Causes
• Congenital abnormality
• Vertebral Disease - TB, osteoporosis, ankylosing spondylitis
• Trauma
• Neuromuscular disease - Poliomyelitis
© Endeavour College of Natural Health endeavour.edu.au 41
KYPHOSIS
https://uprightdoctor.files.wordpress.com/2011/07/kyphosis-adult-hyper.jpg
© Endeavour College of Natural Health endeavour.edu.au 42
DEFORMITIES OF
THE CHEST WALL
Clinical Manifestations (if severe)
• Restriction and distortion of the chest wall
• Misdistribution of the ventilation and blood flow to the lungs
• Can develop
– Type II respiratory failure - Pulmonary hypertension
– Right ventricular Failure - Survival beyond middle age uncommon
© Endeavour College of Natural Health endeavour.edu.au 43
Readings and ResourcesResources:
o Set Textbooks:
Colledge, N.R., Walker, B.R. & Ralston S.H. (2014). Davidson’s Principles and Practice of Medicine, (22nd ed.). Edinburgh.
Churchill Livingstone.
Grossman, S.C. & Porth, C.M. (2014). Porth’s Pathophysiology: concepts of altered health states, (9th ed.). Philadelphia,
U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins.
o Additional textbooks:
Davies, A. & Moores, C. (2010). The respiratory system: basic science and clinical conditions, (2nd ed.). Edinburgh. Churchill,
Livingstone, Elsevier.
Field, M., Pollock, C., Harris, D. (2010). Systems of the Body: The Renal System; Basic Science and Clinical Conditions. (2nd
ed.). United Kingdom: Churchill Livingstone.
Jamison, J.R. (2006) Differential Diagnosis for Primary Care: a handbook for health care practitioners. (2nd ed.). Edinburgh.
Churchill Livingstone.
Lee, G. & Bishop, P. (2013). Microbiology and Infection Control for Health Professionals, (5th ed.). Frenchs Forest, NSW.
Pearson Education.
McCance, K.L. & Huether, S.E. (2014). Pathophysiology: the biological basis for disease in adults and children, (7th ed.). St.
Louis, MO. Elsevier.
Murphy, K. (2011). Janeway’s immunobiology, (8th ed.). New York. Garland Science.
Noble, A., Johnson, R. & Bass, P. (2010). The cardiovascular system: basic science and clinical conditions, (2nd ed.).
Edinburgh. Churchill, Livingstone, Elsevier.
Pagana, K.D. & Pagana, T.J. (2013). Mosby’s diagnostic and laboratory test reference, (11th ed.). St. Louis, MO. Elsevier.
Smith, M.E. & Morton, D.G. (2010). The digestive system: basic science and clinical conditions, (2nd ed.). Edinburgh.
Churchill, Livingstone, Elsevier.
VanMeter, K.C. & Hubert, R. (2014). Gould’s pathophysiology for health professions, (5th ed.). St. Louis, MO. Elsevier.
© Endeavour College of Natural Health endeavour.edu.au 44
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and
communicated to you by or on behalf of
the Endeavour College of Natural Health pursuant to
Part VB of the Copyright Act 1968 (the Act).
The material in this communication may
be subject to copyright under the Act.
Any further reproduction or
communication of this material by you
may be the subject of copyright
protection under the Act.
Do not remove this notice.
Recommended