
Research Priorities of NIDA’s Medications Development Program
Iván D. Montoya, M.D., M.P.H.
Deputy Director, Division of Therapeutics and Medical Consequences
NIDA
No Disclosures

NIDA Medications Development Program
• In 1989, the U.S. Congress mandated that a Medications Development Program (MDP) be established within NIDA
• In 1990, NIDA created the Medications Development Division (MDD), now the Division of Therapeutics and Medical Consequences.
Mission
To use science as a vehicle for improving the pharmacological treatment of Substance Use Disorders with an emphasis on the identification, evaluation, and development of safe and effective medications and biologics to treat them.

NIDA MDP
Division of
Therapeutics &
Medical Consequences
of Drug Abuse
Kurt Rasmussen
Ivan Montoya
Chemistry &
Pharmaceutics
Rik Kline
Med Discovery &
Toxicology
Jane Acri
Clinical Research
Grants
Kevin Walton
Clinical Medical
Shwe Gyaw
Regulatory
Affairs
Robert Walsh

Medication Development Program
Modeled after a typical pharmaceutical company
Supports all phases of medications development
Grants
Contracts
Interagency Agreement
Marketed medications with good
rationale to test in addicted subjects
Basic science, discovery driven process based
on the emerging Neurobiology of Addiction
Medications Development

MDP Emphasis
• Opioids
• Marijuana
• Cocaine
• Amphetamines
• Nicotine
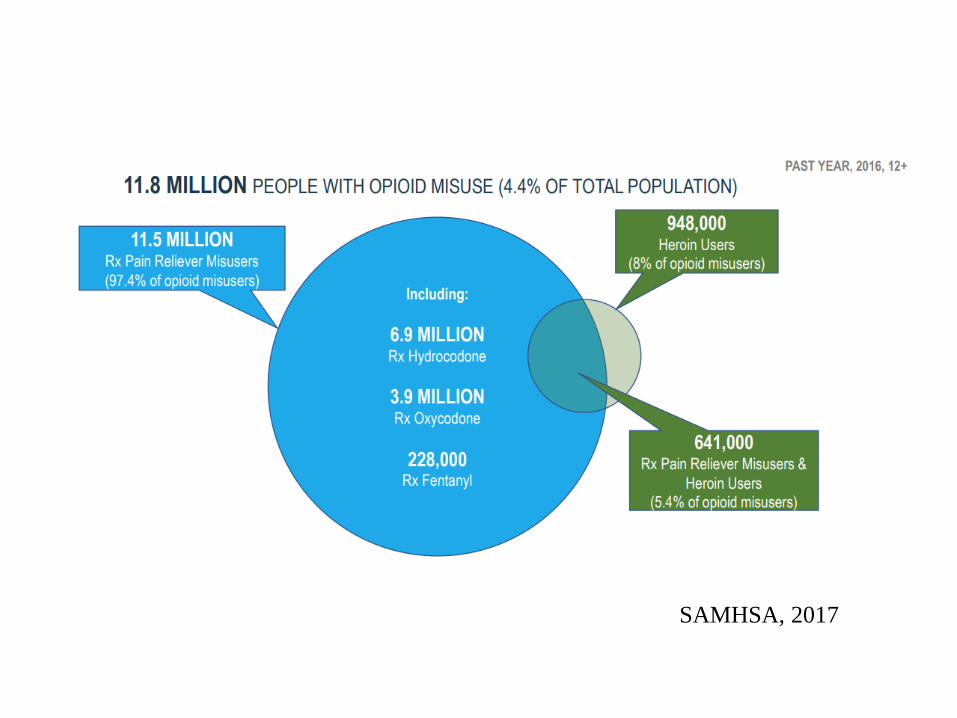
SAMHSA, 2017

Based on CDC MMWR Report 2017
Any opioid 49,900
Challenges of the Opioid Crisis
• Has claimed about 200,000 lives
• Overdose deaths continue to rise. There is no end in sight.
• Efficacious treatments are available to treat opioid use disorders and to prevent/reverse overdose; however:
– Few FDA approved medications
– Efficacy needs improvement
– Side-effects
– Limited access
– Underutilized
– Minimal industry investment

• Prevent initiation and progression of OUD
• Improve OUD treatment outcomes
• Facilitate opioid agonist discontinuation
• Improve tx opioid withdrawal (including neonatal)
• Reduce lethality of opioid overdose
• Reduce overdose relapses
• Reduce need/dose of opioids analgesics
• Reduce risk of opioid respiratory depression
Clinical Priorities

Lofexidine
• Selective alpha2 adrenergic agonist
• Pre-synaptic inhibitor of NE release
• Reduces NE release during opioid withdrawal
• FDA indication: “for the mitigation of withdrawal symptoms to facilitate abrupt discontinuation of opioids in adults” for tx for up to 14 days in > 18 years old.

Lofexidine
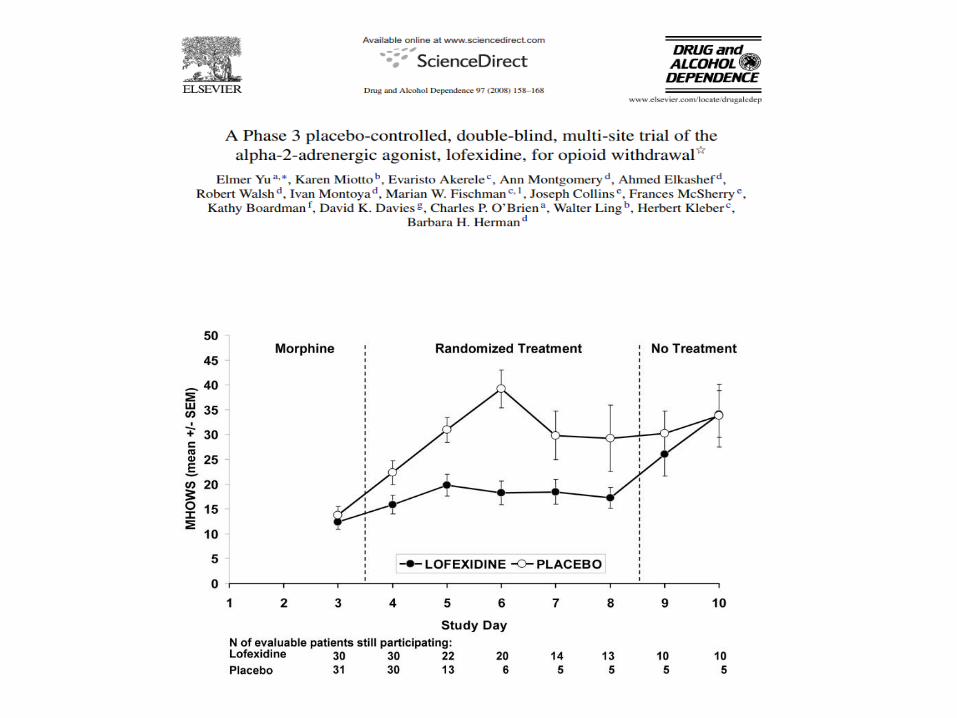

N=264
Lofexidine: 3.2 mg/day

Lofexidine - Dosing
• Dosage is three 0.18 mg tablets taken orally 4 times daily at 5- to 6-hour intervals
• The total daily dosage of should not exceed 2.88 mg (16 tablets) and no single dose should exceed 0.72 mg (4 tablets)
• Dosing guided by symptoms
• Discontinue with a gradual dose reduction over 2 to 4 days
• Hepatic or Renal Impairment: Dose adjustments

Lofexidine - Risks
• Hypotension, bradycardia , somnolence, dizziness, dry month, few cases of syncope
• Rebound hypertension
• Change in opioid tolerance may lead to overdose
• QT prolongation (methadone)
• May potentiate CNS depressants
• CYP2D6 inhibitors (e.g., paroxetine) may increase plasma levels

• Naloxone Nasal Spray Development
Needle-free, unit-dose, ready-to-use opioid overdose antidote.
Image courtesy of ADAPT Pharma,
Inc.

Rosenthal et al., Addiction 2013;105.
PROBUPHINE®

Meds for OUD - Clinical
• Gabapentin
• Pregabalin
• CB1 agonists
• CBD
• VLY-686 Tradipitant (NK1 antagonist)

Meds for OUDs - Preclinical
Mechanisms to reduce cue-induced drug
seeking
• D3 Receptor Antagonists
• OX-1 Receptor Antagonists
• 5-HT2C Receptor Agonists
• 5-HT2A Receptor Inverse Agonists
• mGluR2 Positive Allosteric Modulators
• 5-HT6 Receptor Inhibitors
• PDE7 Inhibitors
Mechanisms to reduce stress-induced
drug seeking
• Kappa Opioid Receptor Antagonists
• OX-1 Receptor Antagonists
• NOP Receptor Agonists
• α2-Adrenergic Receptor Agonists
• PDE7 Inhibitors
Promising Targets
Almitrine (Duxil® by Servier)
• Agonist of peripheral chemoreceptors located on the carotid bodies.
• Increase arterial oxygen tension while decreasing arterial carbon dioxide tension in patients with chronic obstructive pulmonary disease
• Indicated for COPD• Oral activity, prolonged duration of effect, and an
improved adverse effect profile. • Well tolerated (headache and minor GI disturbances)
Respiratory Stimulants

Heroin Vaccine
Raleigh, Pentel LeSage, 2014
• Morphine-conjugate vaccine (M-KLH)
• Vaccinated rats compared to controls:
• Heroin and its active metabolites, 6-
acetylmorphine (6-AM) and morphine,
were retained in plasma
• Metabolite concentrations were reduced in
brain
• Consistent with the changes in heroin self-
administration rates

Fentanyl Vaccine
IgG titers determined by ELISA against a fentanyl-BSA conjugate
i= vaccine injection
Bremer, 2017

Question
• To NIDA: Could you give us a breakdown of the funds provided to NIH for the opioid epidemic? How much to NIDA/year for how long? Could you provide some insight into how funds be used by NIDA and other NIH institutes (that is, basic v clinical; genomics?, drug development, etc.)


HEAL: Helping to End Addiction Long-term
NIH Initiative to Address the Opioid Crisis
• $500M just added by Congress
• Adds to $600M current funds = $1.1B for FY18
• Will propel HEAL
• Collaborative, cross-cutting research
• From basic to behavioral – and everything between
• Innovative partnerships – across agencies, sectors, organizations –
will ensure rapid progress
• Advances national priorities for pain and OUD research.


Based on CDC MMWR Report 2017
Any opioid 49,900

CANNABIS LAWS IN THE U.S.
States with MML vary on:• Allowable conditions and routes of administration.• Dispensaries/home growth and registries.• Testing, regulatory requirements.
States with Recreational Laws vary on: • Marketing, product labeling, distribution
(home growth).• Taxation.
29 states have legalized medical marijuanaalong with D.C., Guam and Puerto Rico
As of Jan. 22, 2018, theVermont legislature passedadult-use legalization legislationand the governor signed the bill.The measure does NOT set up aregulatory system for sales or production.
Recommended





![Les Laboratoires Servier and anr (Appellants) v …...Michaelmas Term [2014] UKSC 55 On appeal from: [2012] ECWA Civ 593 JUDGMENT Les Laboratoires Servier and another (Appellants)](https://img.pdfslide.us/doc/110x75/5f4b5569e2cf9541492af3c9/les-laboratoires-servier-and-anr-appellants-v-michaelmas-term-2014-uksc.jpg)




![Les Laboratoires Servier and anr (Appellants) v … Term [2014] UKSC 55 On appeal from: [2012] ECWA Civ 593 JUDGMENT Les Laboratoires Servier and another (Appellants) v Apotex Inc](https://img.pdfslide.us/doc/110x75/5ab7dcfe7f8b9a684c8c0c3f/les-laboratoires-servier-and-anr-appellants-v-term-2014-uksc-55-on-appeal.jpg)






