
Attach 4
1
REPORT TO WANDSWORTH CLINICAL COMMISSIONING GROUP
11th July 2012
Agenda No. 6.4
Title of Document: Report to CCG on Sickle Cell Disease Service Improvement Update
Report Authors: Josephine Ruwende Consultant Public Health, Aslam Begg PH Strategist, Dr Soleman Begg Clinical lead Haemoglobinopathies, Laurence Gibson AD Health Intelligence Lead Director/ Clinical Lead: Houda Al Sharifi / Dr Soleman Begg
Contact details: [email protected] [email protected]
Summary: The purpose of this report is to update the Clinical Commissioning Group on the progress that has been made by the Haemoglobinopathy Working Group in improving the pathway and services for adolescents and adults with Sickle Cell Disease in Wandsworth.
The report focuses on the following areas:
Identification and development of a single site for the hospital and community
haemoglobinopathy teams
Primary care development
Development of sickle cell specialist pain management services
Development of primary care haemoglobinopathy disease registers
Patient engagement
Key sections for particular note (paragraph/page), areas of concern etc: Entire report
Recommendations: The CCG is requested to note the progress in improving the services and pathways for Sickle Cell Disease in Wandsworth and to support the general direction of travel identified in the model of care and the work streams of the Joint Haemoglobinopathy Working Group (Appendices 1 and 2)
Committees which have previously agreed the report Management Team 4 July 2012 A Sickle Cell Service Improvement Update report was provided to the Clinical Commissioning Group in April 2012.
Future Direction/Transition Arrangements: As described in report

Attach 4
2
Please state which of the assessments below does this document link to or provide evidence for: QIPP Plan: N/A Operating Plan: Sickle Cell has been identified as a priority in the Commissioning Strategy Plan and Operating Plan
Clinical Commissioning Group Comments where appropriate: April 2012- further CCG update requested for July 2012
Financial Implications:
Capital development-£242k (capital-200k, revenue -£42k) to be confirmed/approved
Development of Specialist Sickle Pain management Service £90k recurrent (approved 2012/13) Reviewed by: D. Marshman Other Implications including patient and public involvement/Legal/Governance/Diversity/ Staffing
Service users have been closely involved in this service redesign and in identifying priorities for development
Work is underway to integrate the community and acute haemoglobinopathy nursing teams
Equality Impact Assessment Has an EIA been carried out?
Yes
No issues of concern
Information Privacy Issues Has a consideration of privacy impacts been undertaken and controlled for?
Yes Key issues from assessment:
The development of a accurate disease registers requires access to patient data from SGH pathology departments. This has been discussed and approved by the appropriate information governance leads within the trust.
Other Issues
How will this support patient self-management (education)? This model of care explicitly supports patient self management and includes the development of a Pain Management Programme and a Sickle-Cell specific multi-component pain management programme
Have implications for Carers been considered? Yes Carers play an important role in the management of SCD in young adults. Carers play an increasingly important role in the transition of the paediatric patients into the adult services. Education and training of carers considered as part of the service delivery.
Has third sector contracting been considered? The Working Group has representatives from the Wandsworth Sickle Cell and Thalassaemia Support Group. This group works closely with clinical staff in delivering patient education The support group has received funding for patient education and awareness raising from Wandsworth Council

Attach 4
3
Wandsworth Sickle Cell Disease Service Improvement Update July 2012
1. Background
Sickle Cell Disease (SCD) has a significant impact on life expectancy, daily functioning and
the quality of life of patients. Pain crises result in frequent A&E attendances and emergency
admissions. There are significant inequalities associated with SCD- it is a condition that
predominantly affects people from Black ethnic groups and shortens life expectancy by
between 25 and 30 years (life expectancy in men is 53 and 58 in women). Over the years,
patients and clinicians have expressed dissatisfaction about local services and pathways
and several initiatives have been undertaken to address this.
The purpose of this paper is to update the Clinical Commissioning Group on the progress
that has been made by the joint Haemoglobinopathy Working Group in improving the
services and pathways for adolescents and adults with Sickle Cell Disease (SCD) in
Wandsworth.
2. Progress to date
An update was presented to the Clinical Commissioning Group in April 2012, describing the
four-tier model of care for Sickle Cell Disease in Wandsworth (Appendix 1) and the major
work streams and priorities of the Haemoglobinopathy Working Group for 2012/13 (Appendix
2). This paper further describes the work that has been undertaken to date in the following
areas:
Identification and development of a single site for the hospital and community
haemoglobinopathy teams
Primary care development
Development of a specialist pain management service for patients with Sickle Cell
Disease
Development of primary care haemoglobinopathy disease registers
Patient engagement

Attach 4
4
3. Site development:
3.1 Rationale
Plans are underway to identify and develop a single site for the acute and community
haemoglobinopathy teams. Co-location of the both teams will facilitate the development of
an integrated, clinically lead, community-orientated service and support patient self-
management. Integrating the hospital and community teams within a single location will
also:
Improve access to Multi-Disciplinary Team (MDT) support for patients. The MDT will
all be located together bringing efficiencies in working and a single point of access for
patients.
Provide an alternative setting for simple procedures – currently 80% of A&E
attendees are given advice only. The service will be able to provide monitoring and
management of early sickle crises symptoms and prevent A&E attendance and
emergency admissions.
Improve maintenance of patients’ Integrated Care Plans (ICP) with access to MDT on
site – currently multiple, single care plans and notes are in place across community
and acute settings.
Introduce one-stop clinics to reduce multiple appointments.
Improve facilities for providing education and training to both staff and patients.
Support service efficiencies by reducing duplication between the two teams and
maximise utilisation of staff time. This will potentially create capacity for staff to
expand or introduce community-based services such as home visits and outreach
clinics
3.2 Progress to date
Following discussions with the Working Group, the Strategic Asset Management (SAM)
team:
Undertook a detailed assessment of the space requirements for an integrated, co-
located service (clinical, counseling, training, waiting rooms, offices etc)
Devised the following criteria for site selection with the Working Group:
o Located south of borough/Wandle where 50% of patients are registered (see
Appendix 4- patient mapping)
o Good public transport links from all parts of the borough and Merton

Attach 4
5
o Disabled parking, ambulance access
o IT access and infrastructure
o Proximity to SGH etc
Identified several potential sites within the borough for consideration by the Working
Group.
3.3 Site identification
A preferred site has been identified in Wandle, south of borough. Discussions are currently
underway with Community Services Wandsworth (CSW) to explore the feasibility of
accommodating the single haemoglobinopathy team within this site.
Further discussions will be held with the CCG, CSW, SGH and the SAM team to progress
this development.
An updated business case will be submitted to the PCT by mid July. It is anticipated that
refurbishment will commence in September.
4. Primary Care Haemoglobinopathy Disease registers
4.1 Rationale
The Wandsworth Sickle Cell Needs Assessment and Service Review undertaken in May
2011 identified 162 patients with a diagnosis of Sickle Cell Disease from EMIS. Discussions
with service users and clinicians, suggested that these patients represented only 50% of the
patients with sickle cell disease in Wandsworth. In addition, EMIS searches identified 300
patients in Wandsworth with Thalassaemia major and 1200 with Thalassaemia trait.
Discussions with SGH clinicians revealed that this was a considerable overestimate as the
hospital had less than twenty patients with Thalassaemia major, and there are only
estimated 600-800 patients in the whole of the UK.
Work has been underway to develop validated, accurate and complete primary care
registers of patients with sickle cell and Thalassaemia (Haemoglobinopathies) in
Wandsworth. This will enable patient identification, call and recall for annual reviews and
immunizations etc and support the delivery of clinical care. In addition, correct identification
of carriers will enable preconception counseling and antenatal screening

Attach 4
6
4.2 Progress to date
There are 2,305 patients registered with a Wandsworth GP and read coded as D104, D105,
and D106 (Sickle cell and thalassemia). Using these codes this cohort of patient can be
followed on EMIS Web.
4.2.1 Reconciliation
In order to ensure all patients are identified in primary care, a reconciliation with St Georges
pathology department has been undertaken. The reconciliation has revealed patients
identified in primary care, but not at the St Georges pathology lab, and vice versa. The
reasons for records not reconciling include patients not been tested at St Georges, and St
Georges testing people that may have subsequently left the area.
Reconciliation results have been presented at the Haemoglobinopathy Working Group at St
Georges
4.3 Practice visits
Practice visits are planned in July 2012 to explain the process so far, to advise on the read
codes being used, and to query discrepancies between EMIS records and pathology
records.
4.4 Routine reporting
A series of indicators to monitor the quality of SCD care in general practice will be produced
routinely from EMIS web following consultation with GP practices, for example flu
immunization.
5. Primary Care Development
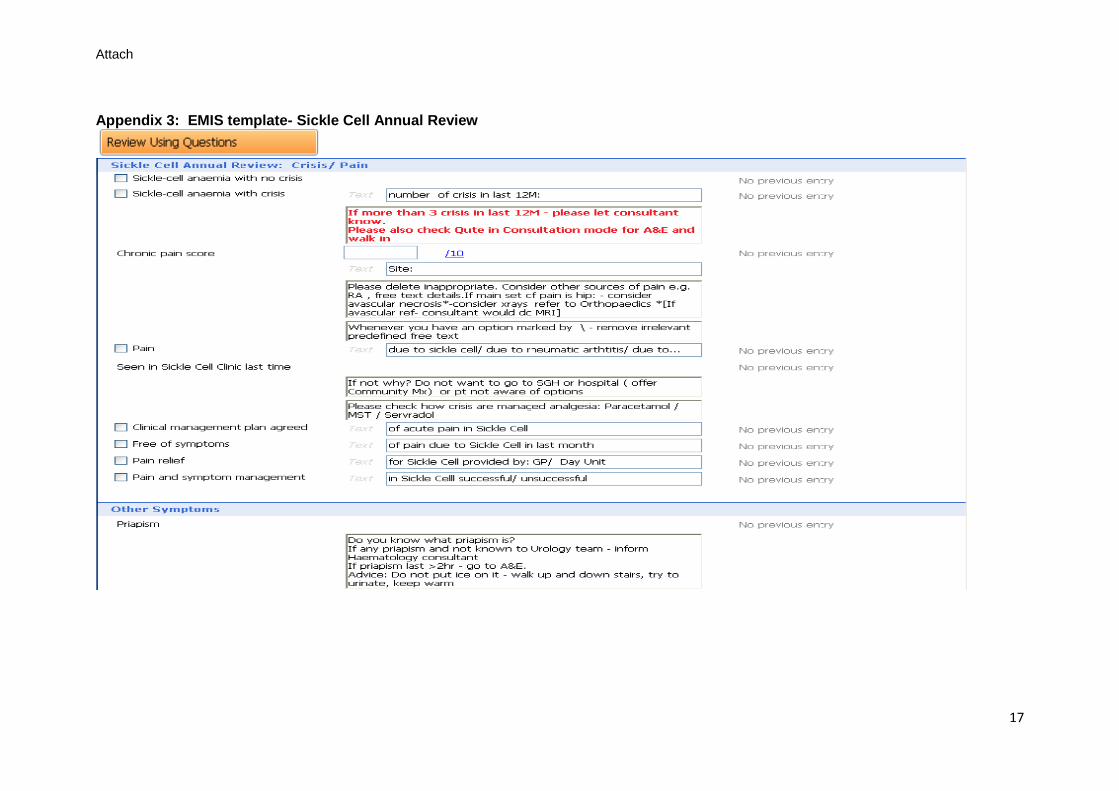
5.1 EMIS templates and roll out
A Primary Care Annual Review template has been created (Appendix 3) with conjunction
with Anna Trela (IM&T Facilitator NHS SWL).

Attach 4
7
5.1.1 Methodology
The NHS Brent sickle cell annual review template was reviewed
The Wandsworth annual review template was created in conjunction with
Working Group and Haemoglobinopathy Haematology Consultants at St
George’s and St Helier’s.
Focus is on key questions to enquire from the service user in an annual
review which include sickle cell issues as well as health promotion e.g.
immunisations and cervical screening uptake
Ensure red and yellow flags are clearly stated within the template, as well as
the method and indications for escalation to secondary care.
These templates will be piloted in GP surgeries after a number of practices
have switched to EMIS Web to allow use of template (this is expected to
occur by autumn 2012).
5.2 GP training
Teaching will be initiated at practices with higher number of service users and high
frequency attendees. Practice visits have been undertaken to Freeman, Chatfield and
Falcon Road practices.
Arrangements are in place to revisit these practices. Hence allow practices time to
implement the findings of the SCD data validation exercise (from the SGH pathology
database compared to EMIS data).
In addition to practice visits a webinar will be created and which will be accessible to all
Wandsworth practices regarding the SCD training. (There will be a separate webinar for GPs
and for nursing and health care staff).
6. Sickle Cell Specialist Pain management Service
6.1 Rationale
Pain is the predominant clinical feature of sickle cell disease; the pain can be unpredictable,
intermittent or constant and is often poorly managed over a lifetime. Most adults with the
condition have a combination of ongoing chronic pain and, in addition, will have acute pain
crises. Pain frequently is mixed as to type and mechanism due to confounding factors. Acute

Attach 4
8
pain can be superimposed on chronic pain, and frequent episodes of acute pain can
resemble chronic pain. Pain has a devastating impact on the patient’s quality of life and
unrelieved pain can have significant psychological, social and physiological effect.
Acute pain crises are the most common reason for A&E attendances and emergency
admissions. Frequent pain crises are associated with elevated mortality rates in adults with
SCD. Unrelieved chronic pain can be extremely disabling requiring significant health and
social care resources.
The causes and clinical presentation of pain are diverse and complex and multidisciplinary,
multi-component pain management services need to be available to patients.
6.2 Sickle Cell Pain Management Programme (PMP)
The specialist haematology and chronic pain psychologists have developed a multi-
component SCD pain management programme which will be available to patients in
2012/13.
Research has shown that patients who attend pain management programmes tend to use
hospital services less frequently, engage in more collaborative decision-making regarding
treatment, and benefit from an improved quality of life. This PMP, developed specifically for
sickle cell pain, will provide valuable skills and strategies to enable patients to:
Understand the mechanisms of and treatments for persistent pain
Provide highly relevant support and education in the context of a long-term, complex
condition
Improve quality of life
Maximise individual levels of daily functioning, whether at home, in the family, or at
work
Explore and manage the psychological aspects of pain, such as low mood and
anxiety
Access the latest evidence-based pain management strategies
Improve communication with clinical care teams
Increase opportunities for self-management
Benefit from a multi-disciplinary approach from clinicians whose expertise lies in the
treatment of sickle cell disease and persistent pain
Access specialist Haemoglobinopathies support if problems were to arise
Management strategies for acute crises
The programme will be comprised of
Specialist multidisciplinary assessment

Attach 4
9
Small group programmes run throughout each calendar year
Follow up and review clinics
Potential for life-stage specific programmes, eg young adults or older age group
programmes
Step-up and step-down model of treatment, for example to individual clinical
psychology interventions, nurse-led TENS, occupational therapy and physiotherapy
input
Ongoing evaluation and review
In addition to direct patient treatment and education, the Sickle Cell Pain Management
Service will provide staff training in pain management in sickle cell disease and pain
education workshops for patients and their friends and family members.
5.2 Joint Haemoglobinopathy and Pain Management Consultant Led Clinic
A consultant-led, joint specialist pain clinic for patients with sickle cell disease will be
introduced at SGH in Q2 2012/13. This will be a monthly joint clinic between the chronic
pain physicians and haematologists for the assessment, treatment and review of patients
with complex pain presentations. This clinic will also focus on the optimisation of medical
interventions for pain.
6. Tier 3: Community management
6.1 Tier 3 Supported discharge
Follow-up sickle cell patients discharged from the hospital following admission is one of the
CSW quality improvement goals/CQUINs* for 2012/13. It is also anticipated some of these
patients will be discharged into the Community Ward. Sickle Cell Disease protocols have
been developed for the Community Ward and training of the staff has taken place.
6.2 Tier 3 CNS-led community management- Integrated Care Plans
A CQUIN indicator has also been developed for CSW to ensure that all sickle cell patients
have an integrated care plan by Q4 2012/13. A sickle cell disease ICP was developed in
2011/12 and roll out commenced in Q3 2011.
* The Clinical Quality and Innovation (CQUIN) payment framework enables commissioners to reward excellence by linking a proportion of providers’ income to the achievement of local quality improvement goals
Attach 4
10
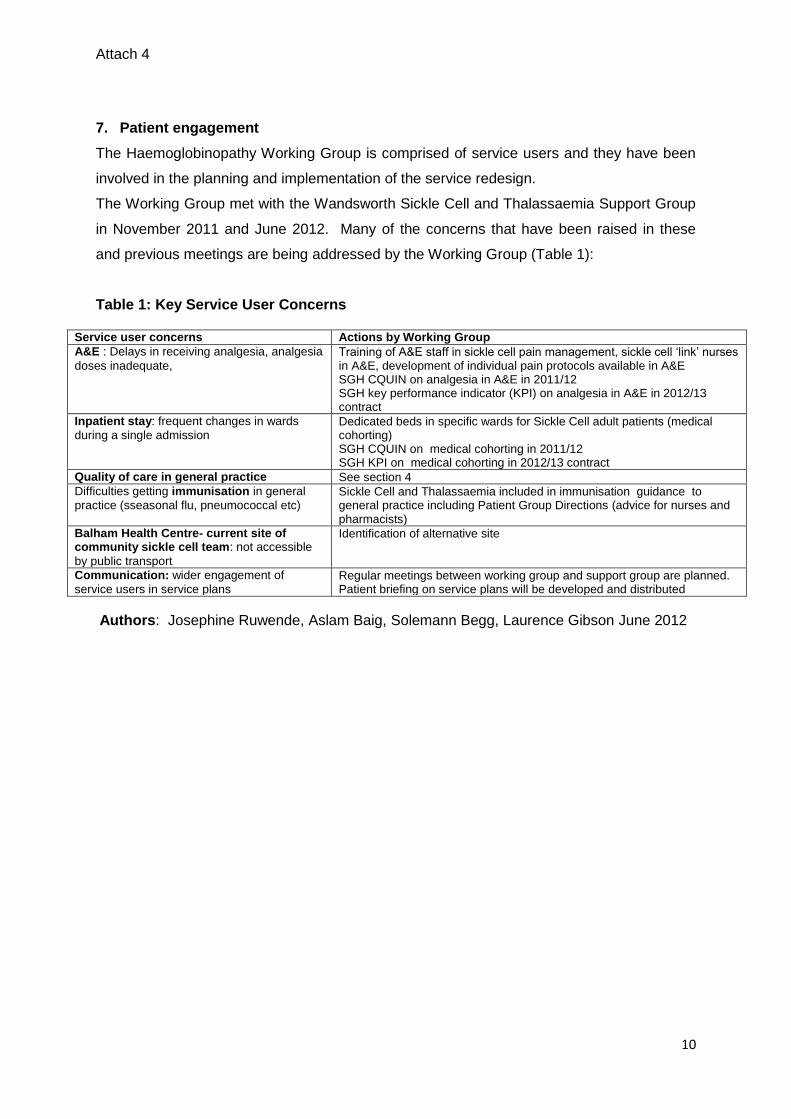
7. Patient engagement
The Haemoglobinopathy Working Group is comprised of service users and they have been
involved in the planning and implementation of the service redesign.
The Working Group met with the Wandsworth Sickle Cell and Thalassaemia Support Group
in November 2011 and June 2012. Many of the concerns that have been raised in these
and previous meetings are being addressed by the Working Group (Table 1):
Table 1: Key Service User Concerns
Service user concerns Actions by Working Group
A&E : Delays in receiving analgesia, analgesia
doses inadequate, Training of A&E staff in sickle cell pain management, sickle cell ‘link’ nurses in A&E, development of individual pain protocols available in A&E SGH CQUIN on analgesia in A&E in 2011/12 SGH key performance indicator (KPI) on analgesia in A&E in 2012/13 contract
Inpatient stay: frequent changes in wards
during a single admission Dedicated beds in specific wards for Sickle Cell adult patients (medical cohorting) SGH CQUIN on medical cohorting in 2011/12 SGH KPI on medical cohorting in 2012/13 contract
Quality of care in general practice See section 4
Difficulties getting immunisation in general
practice (sseasonal flu, pneumococcal etc) Sickle Cell and Thalassaemia included in immunisation guidance to general practice including Patient Group Directions (advice for nurses and pharmacists)
Balham Health Centre- current site of community sickle cell team: not accessible
by public transport
Identification of alternative site
Communication: wider engagement of
service users in service plans Regular meetings between working group and support group are planned. Patient briefing on service plans will be developed and distributed
Authors: Josephine Ruwende, Aslam Baig, Solemann Begg, Laurence Gibson June 2012

Attach
11
Appendix 1
Attach
12
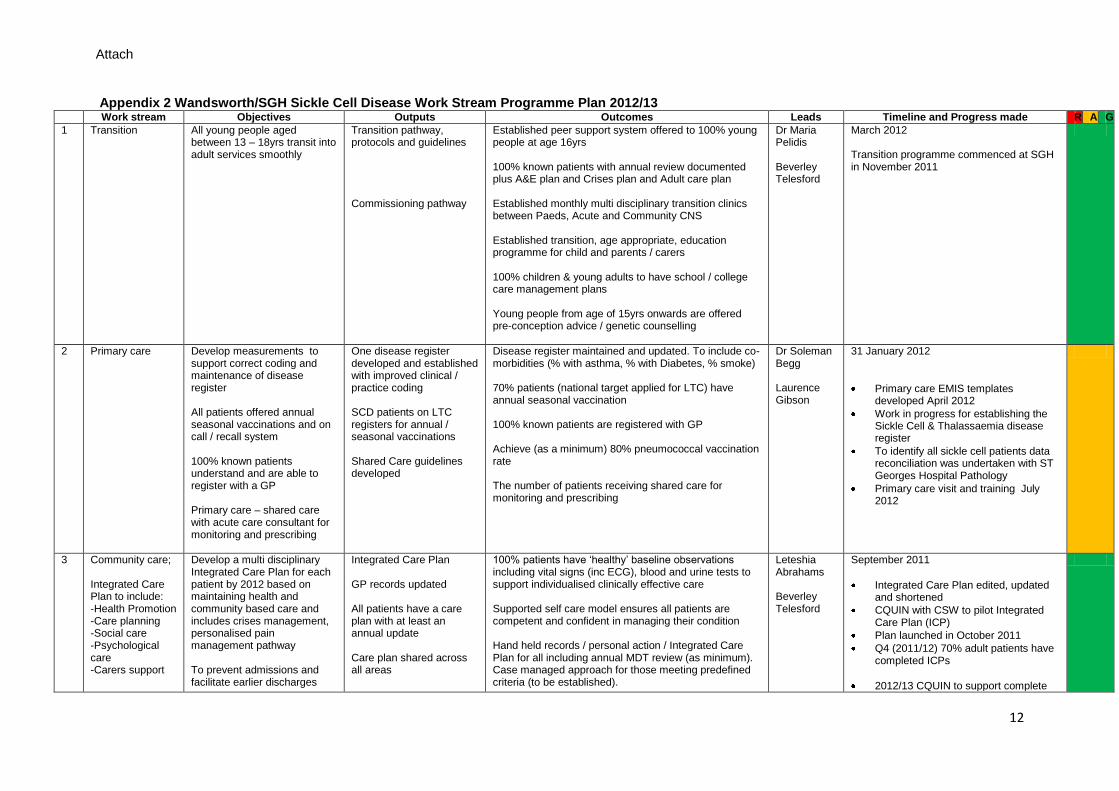
Appendix 2 Wandsworth/SGH Sickle Cell Disease Work Stream Programme Plan 2012/13 Work stream Objectives Outputs Outcomes Leads Timeline and Progress made R A G
1 Transition
All young people aged between 13 – 18yrs transit into adult services smoothly
Transition pathway, protocols and guidelines Commissioning pathway
Established peer support system offered to 100% young people at age 16yrs 100% known patients with annual review documented plus A&E plan and Crises plan and Adult care plan Established monthly multi disciplinary transition clinics between Paeds, Acute and Community CNS Established transition, age appropriate, education programme for child and parents / carers 100% children & young adults to have school / college care management plans Young people from age of 15yrs onwards are offered pre-conception advice / genetic counselling
Dr Maria Pelidis Beverley Telesford
March 2012 Transition programme commenced at SGH in November 2011
2 Primary care
Develop measurements to support correct coding and maintenance of disease register All patients offered annual seasonal vaccinations and on call / recall system 100% known patients understand and are able to register with a GP Primary care – shared care with acute care consultant for monitoring and prescribing
One disease register developed and established with improved clinical / practice coding SCD patients on LTC registers for annual / seasonal vaccinations Shared Care guidelines developed
Disease register maintained and updated. To include co-morbidities (% with asthma, % with Diabetes, % smoke) 70% patients (national target applied for LTC) have annual seasonal vaccination 100% known patients are registered with GP Achieve (as a minimum) 80% pneumococcal vaccination rate The number of patients receiving shared care for monitoring and prescribing
Dr Soleman Begg Laurence Gibson
31 January 2012
Primary care EMIS templates developed April 2012
Work in progress for establishing the Sickle Cell & Thalassaemia disease register
To identify all sickle cell patients data reconciliation was undertaken with ST Georges Hospital Pathology
Primary care visit and training July 2012
3 Community care; Integrated Care Plan to include: -Health Promotion -Care planning -Social care -Psychological care -Carers support
Develop a multi disciplinary Integrated Care Plan for each patient by 2012 based on maintaining health and community based care and includes crises management, personalised pain management pathway To prevent admissions and facilitate earlier discharges
Integrated Care Plan GP records updated All patients have a care plan with at least an annual update Care plan shared across all areas
100% patients have ‘healthy’ baseline observations including vital signs (inc ECG), blood and urine tests to support individualised clinically effective care Supported self care model ensures all patients are competent and confident in managing their condition Hand held records / personal action / Integrated Care Plan for all including annual MDT review (as minimum). Case managed approach for those meeting predefined criteria (to be established).
Leteshia Abrahams Beverley Telesford
September 2011
Integrated Care Plan edited, updated and shortened
CQUIN with CSW to pilot Integrated Care Plan (ICP)
Plan launched in October 2011
Q4 (2011/12) 70% adult patients have completed ICPs
2012/13 CQUIN to support complete

Attach
13
Work stream Objectives Outputs Outcomes Leads Timeline and Progress made R A G
To reduce A&E attendances
Annual audit calendar 100% carers signposted to and aware of carers assessments & support – including young carers Reduced A&E attendances and admissions including length of stay through increasing supported self care Identify criteria and patients with complex needs requiring active case management.
roll out with the following indicators: (1) (a) % of new adult sickle cell patients
on haemoglobinopathies team caseload are referred to appropriate self-management programmes if requested; (b) % of adult sickle cell patients who have been on the haemoglobinopathies team caseload for 12 month have a formal care plan review carried out and documented.
(2) % of adult sickle cell patients discharged from SGH are contacted or visited by the Haemoglobinopathies Team Clinical Nurse Specialist (CNS) within 48 hours of discharge summary being received (Mon - Fri excl. Bank Holidays)
Dedicated social services input to be developed
4 Secondary and tertiary care
To provide clinical leadership To provide health care services that meet national requirements To support network for specialist tertiary care
Service and pathway that meets peer review (national) standards
All patients receive clinically effective care reducing crises, preventing complications and improving quality of life
Dr Elizabeth Rhodes
October 2011
Designated haemoglobinopathy lead consultant appointed by SGH- commenced employment October 2011
Preparation for peer review to commenced
Peer Review to take place in October 2012
Key performance indicators included in 2012/13 SGH contract:
(1) Analagesia according to individual pain protocol in ED: Increasing number of adults with SCD who present to the ED in a pain crisis receive analgesia according to their individual pain protocol
(2) Analgesia administered within 30 minutes of presentation to ED: 80% of adults with SCD who present to the ED in a pain crisis receive analgesia within 30 minutes of presentation
(3) Designated beds: 80% of adults with SCD are admitted into haematology

Attach
14
Work stream Objectives Outputs Outcomes Leads Timeline and Progress made R A G
wards or medical beds specifically identified for cohorting of SCD admissions for the majority of that admission
5 Emergency admission and discharge planning
Develop early crisis intervention to prevent clinical escalation requiring A&E care and / or admission Reduce number of A&E attendances for advice, Emergency admissions and length of stay Increase number patients supported to manage at home
Commissioning pathway Integrated care plan Links established to community virtual ward
Joint patient visits / hand over’s between Acute and Community CNS All discharged patients notified to Balham within 24 hours of discharge (Monday – Friday exc. BH’s) All discharged patients contacted and visited within 48 hours of discharge 100% discharge patients have crises management plan Reductions in admissions, length of stay and A&E attendances
Carol Rose Letisha Abrahams
October 2011
Joint protocols for A&E attendance, emergency admission, clinic attendance, discharge developed
Work in progress to establish process to ensure CSW receive the discharge information from SGH as soon as the patients are discharged
6 Community ward Patients have access to enhanced supportive care in the community
All patients are registered with community ward Guidelines and protocols for management developed
Local sickle cell protocols and policies are embedded into community ward Specialist nurses supported in delivering and enhancing community care provision Reduce hospital admissions, A&E attendances and facilitate early discharge
Dr Elizabeth Rhodes
April 2012
SCD patients have access to community ward on discharge effective from 1 April 2012
Joint protocols and pathways drafted
Training of staff done in June 2012
7 Specialist nurse and admin support review
Review roles and responsibilities of specialist nurses and administration processes
Key recommendations identified for service delivery Suggested KPI - Self assessment annually with service improvement / implementation plan
KPI Annual review confirmed and copy received Effective and efficient service delivered through integrated care and case managed approach to patient group which deliver national standards Collaborative working with local support groups
Heather Anderson Julie Nicholson Laura Badley
Review completed October 2011
Further discussions ongoing between CSW and SGH to implement recommendations around integration of acute and community nursing services
8 Staff professional development
Develop an education programme for primary, community and acute care staff (?include social services ??LAC)
Training sessions delivered through a rolling education programme Funding for CPD
Competent and knowledgeable workforce Dr Elizabeth Rhodes Dr S Begg
Initial Primary Care visits undertaken to practices with largest cohorts of patients
GP Practice visit and training of primary care staff planned July 2012
9 Patient education and self management
Develop a supportive self care approach to Integrated Care Plan
Integrated Care Plan pathway Increased number of
Patients are confident in the supportive self care model and have a Integrated Care Plan pathway, pain management and crises management plan
Penelope Cream
March 2012
Dedicated haemoglobinopathy clinical Psychologist employed by SGH with
Attach
15
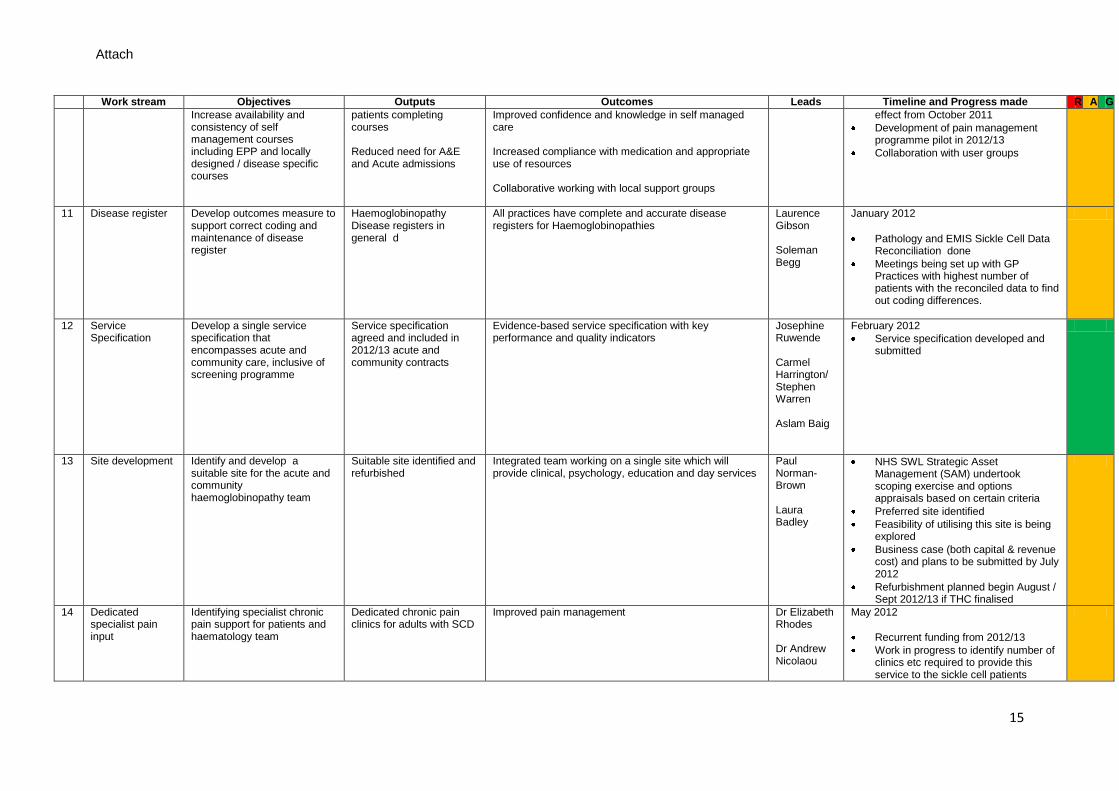
Work stream Objectives Outputs Outcomes Leads Timeline and Progress made R A G
Increase availability and consistency of self management courses including EPP and locally designed / disease specific courses
patients completing courses Reduced need for A&E and Acute admissions
Improved confidence and knowledge in self managed care Increased compliance with medication and appropriate use of resources Collaborative working with local support groups
effect from October 2011
Development of pain management programme pilot in 2012/13
Collaboration with user groups
11 Disease register Develop outcomes measure to support correct coding and maintenance of disease register
Haemoglobinopathy Disease registers in general d
All practices have complete and accurate disease registers for Haemoglobinopathies
Laurence Gibson Soleman Begg
January 2012
Pathology and EMIS Sickle Cell Data Reconciliation done
Meetings being set up with GP Practices with highest number of patients with the reconciled data to find out coding differences.
12 Service Specification
Develop a single service specification that encompasses acute and community care, inclusive of screening programme
Service specification agreed and included in 2012/13 acute and community contracts
Evidence-based service specification with key performance and quality indicators
Josephine Ruwende Carmel Harrington/ Stephen Warren Aslam Baig
February 2012
Service specification developed and submitted
13 Site development Identify and develop a suitable site for the acute and community haemoglobinopathy team
Suitable site identified and refurbished
Integrated team working on a single site which will provide clinical, psychology, education and day services
Paul Norman-Brown Laura Badley
NHS SWL Strategic Asset Management (SAM) undertook scoping exercise and options appraisals based on certain criteria
Preferred site identified
Feasibility of utilising this site is being explored
Business case (both capital & revenue cost) and plans to be submitted by July 2012
Refurbishment planned begin August / Sept 2012/13 if THC finalised
14 Dedicated specialist pain input
Identifying specialist chronic pain support for patients and haematology team
Dedicated chronic pain clinics for adults with SCD
Improved pain management Dr Elizabeth Rhodes Dr Andrew Nicolaou
May 2012
Recurrent funding from 2012/13
Work in progress to identify number of clinics etc required to provide this service to the sickle cell patients

Attach
16
Leads Leteshia Abrahams, CNS, Adults, CSW Heather Anderson, Manager, CSW Laura Badley, (Acting) General Manager, SGH Dr Aslam Baig, PH Strategist, NHS Wandsworth Dr Solemann Begg, GP lead Penelope Cream, Clinical Psychologist, SGH Laurence Gibson, AD Health Intelligence, NHSW Carmel Harrington, AD Acute Commissioning, SWLACU Julie Nicholson, Matron, SGH Dr Andrew Nicolau Consultant Pain Physician SGH Paul Norman-Brown, Head of Technical Services and Strategic Estates Dr Maria Pelidis, Consultant Paediatric Haematologist, SGH Dr Elizabeth Rhodes, Consultant Haematologist, SGH Carol Rose, CNS Adults, SGH Dr Josephine Ruwende, Consultant Public Health Medicine, NHSW Beverley Telesford, CNS, Paediatrics, CSW
Attach
17
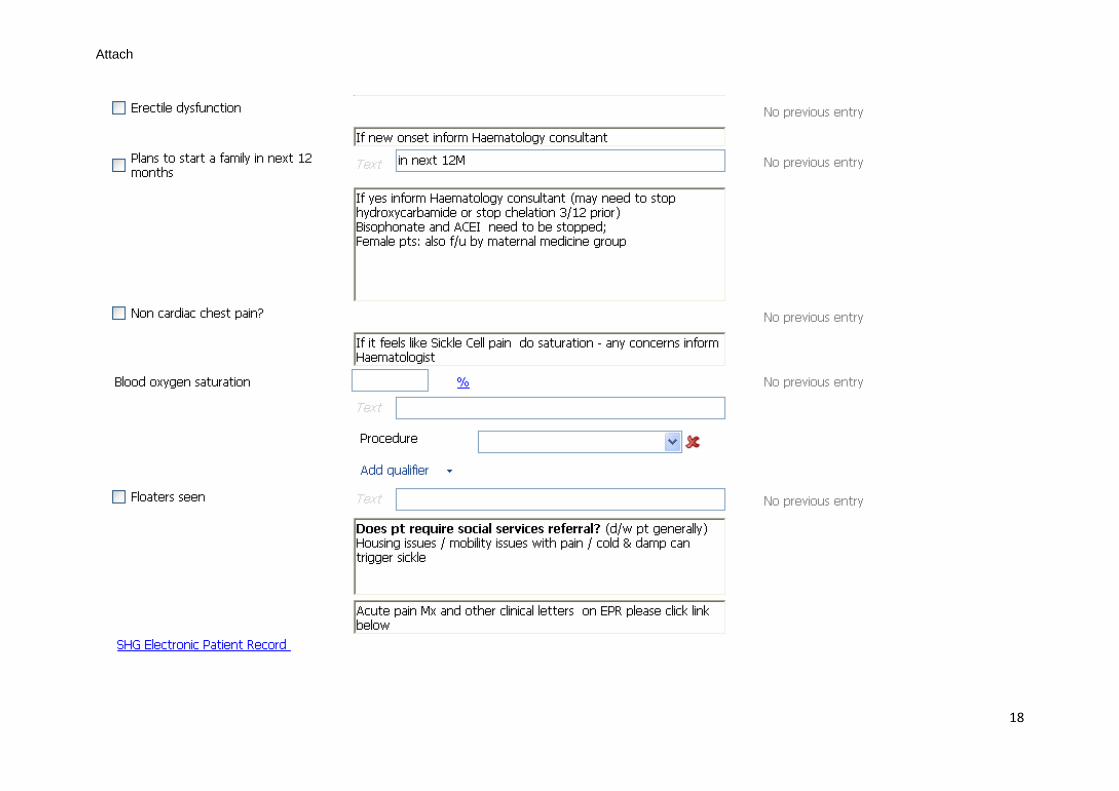
Appendix 3: EMIS template- Sickle Cell Annual Review
Attach
18

Attach
19

Attach
20
Attach
21
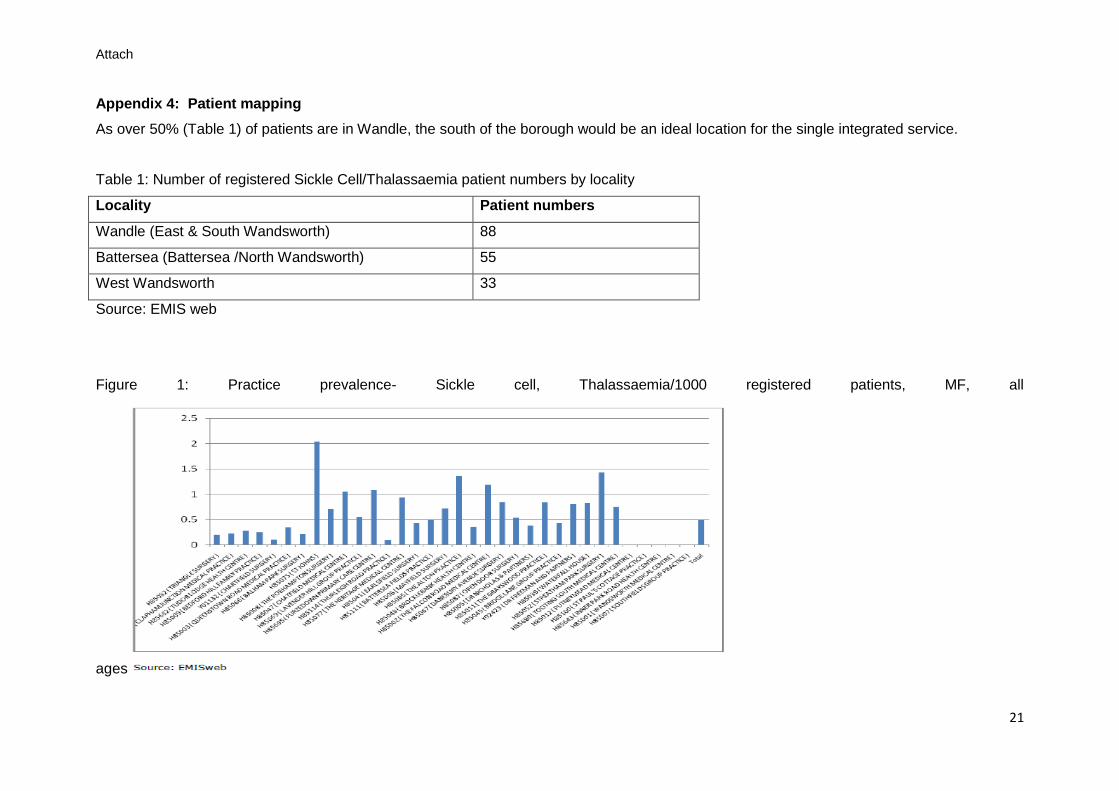
Appendix 4: Patient mapping
As over 50% (Table 1) of patients are in Wandle, the south of the borough would be an ideal location for the single integrated service.
Table 1: Number of registered Sickle Cell/Thalassaemia patient numbers by locality
Locality Patient numbers
Wandle (East & South Wandsworth) 88
Battersea (Battersea /North Wandsworth) 55
West Wandsworth 33
Source: EMIS web
Figure 1: Practice prevalence- Sickle cell, Thalassaemia/1000 registered patients, MF, all
ages
Recommended

















