Albrecht v. Graefes Arch. klin. exp. Ophthal. Graefes Archiv far klinische und experimentelle
211,307-311 (1979) Ophthalmologie �9 by Springer-Verlag 1979
Report of a Case Resembling the 'Fleck Retina of Kandori' with Ectodermal Peculiarities and Macula Degeneration
Melvin Fried and Gerd Meyer-Schwickerath Essen University Eye Hospital (Directors: Prof. Dr. Dr. h. c. G. Meyer-Schwickerath, Prof. Dr. Th. Waubke, and Prof. Dr. A. Wessing), Hufelandstrasse 55, D-4300 Essen, Federal Republic of Germany
Abstract. This report involves the case of a 36-year-old woman followed-up for nine years. The symptoms include unique, sharply-defined, irregular, yellow, large flecks of the retina combined with bilateral macula degener- ation. The patient's rusty-red hair, enamel dysplasia, and ashen-gray skin color were also noted. It is argued that this case is very likely identical with the ' fleck retina of Kandor i ' and as such, the first case reported outside Japan. The literature is reviewed.
Zusammenfassung. Es wird fiber eine 36-jfihrige Frau berichtet, die einzigar- tige, scharf begrenzte, unregelmfiBige, grol3e, gelbe Flecken der Retina sowie eine beidseitige Maculadegeneration aufweist, welche wir tiber 9 Jahre nach- untersucht haben. Es fanden sich auBerdem rostrote Haare, Zahnschmelz- defekte und eine aschgraue Hautfarbe. Sehr wahrscheinlich ist dieser Fall identisch mit der ,,fleck retina von Kandor i" und w/ire somit der erste beschriebene Fall dieser Art auBerhalb Japans.
Introduction
The fleck retina, first described by Kandori in 1959, is a rare condition of which four cases have been reported to date (Kandori, 1959, Kandori et al., 1966 and 1972). The characteristic features of this condition, as pointed out by Kandori, are: (a) sharply defined, dirty yellow, large, and irregular flecks of the retina distributed in between the equatorial and macular region with no macular involvement; (b) normal retinal vessels and normal optic nerve; (c) absence of pigment flecks as seen in pigmentary degeneration of the retina; (d) normal electroretinogram and normal electro-oculogram; (e) normal or mini- mal delay of dark adaptation; (f) onset at 3 0 4 0 years of age in both males and females; (g) lack of progression.
Our intention is to report a case with a striking similarity which has some ectodermal peculiarities (hair, skin, teeth) and macula degeneration not asso-
0065-6100/79/0211/0307/$1.00

308 M. Fried and G. Meyer-Schwickerath
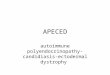
Fig. 1. Right eye. Typical, large, irregular, but sharply defln6d, yellow flecks along the upper temporai vein and artery. Vessels course over these flecks and are normal. The same changes were seen circumpapillary and in the midperiphery. Photo shows appearance at the beginning of follow-up
Fig. 2. Right eye. Same site as in Fig. 1. Note fading of the typical yellow fleck during nine years observation. The sharp demarcation is less distinct and no progression is seen
c i a t e d b e f o r e w i t h t h e f l eck r e t i n a o f K a n d o r i . T o o u r k n o w l e d g e it is t h e
f i r s t Case - l ike ly i d e n t i c a l w i t h t h e f l eck r e t i n a o f K a n d o r i - r e p o r t e d o u t s i d e
J a p a n .
Case Report
The patient was referred to us in 1971, age 36 years, and we. followed her for nine years. She complained of having had decreased vision for the past year. The referring ophthalmologist had noted extensive retinal changes.
The visual acuity at the initial visit was: right eye (RE) 0.05 no correction (n.c.), left eye (LE) 0.6 (with - 1.0 diopters spherical (D.sph.). The present visual acuity is RE: 0.05 (n.e.), LE: 0.3 (with -1.0 D.sph.). Intraocular tension was within normal limits. Both eyes revealed normal anterior segments and transparent media.
The fundi showed normally colored disks with sharply-defined margins and physiologic excava- tions. The retinal vessels were normal in size and course. Numerous, relatively large, irregular but sharply-defined, dirty yellow flecks were noted circumpapillary, in the midperiphery, and at the posterior pole. The flecks were irregular in size, the largest being 2-3 disk diameters, and irregular in configuration. Some were scattered dots, but most were impressive, large, confluent, yellow flecks. These flecks were located deeper than the retinal vessels which run over them. No pigmentary changes as in pigmentary degeneration were noted.
Both maculae revealed an abnormal, round-oval, yellow deposit surrounded by a cystlike halo. ERG and EOG examinations revealed no abnormalities. Color vision was normal. No red-green color disturbance was noted. Dark adaptation was
normal. No constriction of visual field was recorded. Fluorescein angiography of both maculae showed a concentric hyperfluorescence characteristic
at the site of the macula lesion with diffuse staining in the late stage (Figs. 5 and 6).

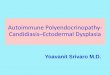
Fig. 3. Left eye. Typical, large, irregular, but sharply defined, yellow flecks along the upper temporal vein and artery. Vessels course over these flecks and are normal. The same changes were seen circumpapillary and in the midperiphery. Photo shows appearance at the beginning of follow-up
Fig. 4. Left eye. Same site as in Fig. 3. Note fading of the typical yellow flecks during nine years observation. The sharp demarcation is less distinct and no progression is seen
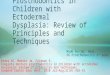
Fig. 5. Right eye. Round atrophic macular scar as seen in the eighth year of observation. The macular lesions in both eyes had revealed abnormal, round-oval yellow deposits which tended to scar formation at the beginning of follow-up
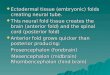
Fig. 6. Right eye. Fluorescein angiography of the macuIa shows a distinct concentric hyperfluorescent ring corresponding to pigment epithelium alterations. Similarity with the bull's eye macula will be noted. In the late stage diffuse staining appeared

310 M. Fried and G. Meyer-Schwickerath
Follow-up Result
A trial with prednisone 40 mg/die for two weeks did not influence this condition. After nine years of observation visual acuity has remained the same in the RE and has further decreased in the LE. The characteristic yellow retinal flecks have a slight tendency to disappear and to lose their sharp demarcation. No progression was noted. Deposits in both maculae have become less distinct and atrophic scars have formed (Fundusphotograph Figs. 1 4).
Family History and General Examination
There is no known history of intermarriage in her ancestry. Night blindness was detected in her mother many years ago. No other visual disturbance or eye disease has been reported in the family. The following peculiarities in this patient were striking: (a) rusty-red hair (one sister of her mother and one brother of her grandmother are known to have rusty-red hair as well); (b) enamel dysplasia (which was reported in her grandmother as well); (c) ashen skin color. General examination disclosed anorexia nervosa with secondary amenorrhea and reversible selective hypotha- lamic suppression of TRH and LH-RH secretion, serum potassium depletion, abuse of laxatives and barbiturates.
The patient's ashen skin color was suggestive of a suicide attempt, involving heavy metals such as silver (argyrosis) and gold (Chrysiasis); arsenic, mercury, and others were suspected, in fact, the patient refused further studies and analysis of skin and hair biopsies as well as urine analysis for porphyrins. Ochronosis and hemochromatosis were ruled out.
Discussion
The general examination gives no clue about the eye condition. Poisoning with heavy metals and abuse of laxatives or barbiturates have not been reported with such characteristic fundus changes as were present in our case (Duke-Elder, 1954). No interrelationship seems to exist between the diagnosis of anorexia nervosa, secondary amenorrhea, reversible selective hypothalamic suppression, and the eye disease in this case.
The association of rusty-red hair, enamel dysplasia and ashen skin color with these peculiar fundus changes seems to be more than accidental. Moreover, hair color and enamel dysptasia are reported in the family. But hair color, skin color, and enamel dysplasia are nonspecific features. They are found in connection with a few dozen eye diseases and syndromes. The striking and specific features in this case are the characteristic yellow fecks of the retina and macula degeneration.
The yellow flecks seem to be deposits and suggest a metabolic disorder or storage disease. But such fundus changes, especially without involvement of the conjunctiva, cornea, and uvea have not been reported in metabolic disor- ders or storage disease (Duke-Elder, 1967; Krill and Archer, 1977).
Krill and Archer (1977) have grouped four conditions - fundus albipunctatus, fundus flavimaculatus, familial drusen, and fleck retina of Kandori - in the chapter, 'Flecked retina diseases'. Besides the similarities among these four conditions there are striking differences and it is not yet known if the basic defect is the same in all four conditions.
The case reported here is clearly distinguished from fundus albipunctatus, fundus flavimaculatus, and familial drusen by its appearance and/or functional examinations such as ERG, EOG, color vision, and darkness adaptation. The

Case Resembling Fleck Retina of Kandori 311
differentiation from retinitis pigmentosa, pigmentary degenerations, and tape- toretinal degenerations presents no problem.
A striking similarity exists between the 'fleck retina of Kandori' and the case reported here. Both have the following in common: (a) the unique and characteristically large, irregular, sharply-defined yellow flecks; (b) normal reti- nal vessels and optic nerve; (c) absence of pigment flecks; (d) no constriction of visual field; (e) normal ERG and EOG; (f) normal or minimal delay of dark adaptation; (g) onset or discovery at 3 0 4 0 years of age; (h) lack of progression.
Some differences, which do not alter the principal similarity but may be considered as an individual variation, should be noted: (a) the ectodermal pecu- liarities of hair, skin, and teeth; (b) the slight tendency of the yellow flecks to disappear and to lose their sharp demarcation; (c) the association of macular degeneration, probably of a hereditary nature, but not identical with vitelli- ruptive macular degeneration (red-green disturbance, abnormal EOG, egg yolk- like vitelliform cyst), Stargardt's macula degeneration (protanomalia, abnor- mal dark adaptation, eventually normal ERG and EOG), and Stargardt flavi- maculatus (abnormal ERG and EOG) (Deutman, 1971; Gass, 1970; Francois, 1977; Jaeger et al., 1973; Krill and Archer, 1977).
All data indicate that the case of fleck retina changes reported here is a unique entity, most probably identical with the 'fleck retina of Kandori'. Since pathologic specimens have not yet been obtained, the histologic appearance and origin of the disease is still unknown. We would like to encourage the publication of similar cases to find a clue to this proposed entity.
Acknowledgements. We wish to thank Professor Jules Francois, Ghent, and Professor August F. Deutman, Nijmegen, for their support with advice and encouragement. We are grateful to Professor Deutman for providing the electrophysiologic examinations and color vision testing. Deutman (1978) has referred to this exceptional case fully described here.
References Duke-Elder, S. : Textbook of Ophthalmology. Voi. 6, Injuries, London: H. Kimpton, 1954 Duke-Eider, S.: Systems of Ophthalmology. Vol. 10, Retina, London: H. Kimpton, 1967 Deutman, A.F. : The hereditary dystrophies of the posterior pole of the eye. Assen: Van Gorcum,
1971 Deutman, A.F.: Retinal dystrophies with unusually large yellowish flecks. K. Shimizu (Ed.)
Int. Congress Series No. 450 XXIII Concilium Ophthalmologicum, Kyoto, 1978, pp. 758-763. Amsterdam-Oxford: Excerpta Medica
Franqois, J.: Juvenile macula degenerations. Jp. J. Ophthalmol. 21, 1-21 (1977) Gass, J.D. : Stereoscopic atlas of macular disease. St. Louis: C.V. Mosby, 1970 Jaeger, W., Alexandridis, E., Tenner, A., KS.fer, O. : Heredit/ire Maculadegenerationen. Ber. Dtsch.
Ophthalmol. Ges. 73, 695-735 (1973) Kandori, F. : Very rare cases of congenital nonprogressive night blindness with fleck retina. Jp.
J. Ophthalmol. 13, 384 (1959) Kandori, R., Setogawa, T., Tamai, A. : Electroretinograph]cal studies on 'fleck retina' with congeni-
tal nonprogressive night blindness. Yonago Acta Med. 10, 98 (1966) Kandori, F., Tamai, A., Kurimoto, S., Fukunaga, K. : Fleck Retina. Am. J. Ophthalmol. 73,
673-685 (1972) Krill, A.E., Archer, D.B. : Krill's hereditary and choroidal disease. Volume II. Clinical characteristics,
pp. : 739-824, 1137-1172. New York, San Francisco, London: Harper&Row, 1977
Received July 28, 1979
Recommended