(Relates to Chapter 28 “Nursing Management:
Lower Respiratory Problems,” in the textbook)
Focus on Lung Cancer
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc.

Lung CancerLeading cause of cancer-related deaths
Leading cause of death in women
Survival rates are lower than for most other cancers.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 2

Etiology Most important risk factor in 80% to 90% of all lung cancers is smoking. Contains 60 carcinogens that interfere with cell development
Causes a change in bronchial epithelium
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 3

EtiologyLung cancer is related to total exposure to cigarette smoke measured by Total number of cigarettes smoked
Age of smoking onset Depth of inhalation Tar and nicotine content Use of unfiltered cigarettes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 4

EtiologyEnvironmental tobacco smoke (ETS) inhaled by nonsmokers poses 35% increased risk of developing lung cancer.
Children are more vulnerable to ETS than adults.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 5

EtiologyOther carcinogens pose risk for developing lung cancer. Asbestos Radon Nickel Iron/iron oxides Uranium
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 6

EtiologyOther carcinogens pose risk for developing lung cancer. Polycyclic aromatic hydrocarbons
Arsenic Chromates Air pollution
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 7

PathophysiologyMost cancers originate from epithelium of bronchus.
It takes 8 to 10 years for a tumor to reach 1 cm. Smallest lesion detectable on x-ray
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 8

PathophysiologyOccur primarily in segmental bronchi and upper lobes
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 9

Lung Cancer
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 10
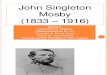
Fig. 28-2. Lung cancer (peripheral adenocarcinoma). The tumor shows prominent black pigmentation,suggestive of having evolved in an anthracotic scar.

Lung Carcinoma
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 11
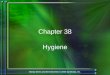
Fig. 28-3. Lung carcinoma. The gray-white tumor tissue is infiltrating the lung. Histologically this tumor wasidentified as a squamous cell carcinoma.

PathophysiologyPathologic changes in bronchial system Hypersecretion of mucus Desquamation of cells Reactive hyperplasia of basal cells
Metaplasia of normal respiratory epithelium to stratified squamous cells
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 12

PathophysiologyPrimary lung cancers categorized into two subtypes Non–small-cell lung cancer (NSCLC)80%
Small cell lung cancer (SCLC)20%
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 13

PathophysiologyLung cancers metastasize by Direct extension Blood circulation Lymph system
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 14

PathophysiologyCommon sites for metastatic growth Liver Brain Bones Scalene lymph nodes Adrenal glands
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 15

PathophysiologyParaneoplastic syndrome
Various systemic manifestations caused by factors produced by tumor cells
Commonly associated with SCLC
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 16

Clinical ManifestationsSymptoms appear late in disease.
Depend on type of primary lung cancer, location, and metastatic spread
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 17

Clinical ManifestationsPneumonitisPersistent cough with sputum (most common)
HemoptysisChest painDyspnea
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 18

Clinical ManifestationsLater manifestations
Anorexia Fatigue Nausea/vomiting Hoarse voice Unilateral paralysis of diaphragm
Dysphagia Superior vena cava obstruction
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 19

Diagnostic StudiesChest x-rayCT scanMagnetic resonance imaging (MRI)
Positron emission tomography (PET)
Diagnosis identified by malignant cells
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 20

Diagnostic StudiesSputum specimens obtained for cytologic studies Fiberoptic bronchoscope Mediastinoscopy Video-assisted thoracoscopy (VATS)
Pulmonary angiography
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 21

Diagnostic StudiesStaging
NSCLC staged according to TNM systemTT denotes tumor size, location, and degree of invasion.
NN indicates regional lymph node invasion.
MM represents presence/absence of distant metastases.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 22

Diagnostic StudiesStaging
SCLCHas not been useful because cancer has metastasized before diagnosis is made
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 23

Diagnostic StudiesScreening
No current recommendations exist.
No difference in deaths between those screened and those who were not
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 24

Collaborative CareSurgical therapy
Surgical resection is contraindicated for small cell carcinomas.
NSCLC is likely treated with surgery.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 25

Collaborative CareRadiation therapy
Used as curative therapy, palliative therapy, or adjuvant therapy
Primary therapy for those unable to tolerate surgery
Some cancer cells are more radiosensitive than others.
Stereotactic radiotherapy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 26

Collaborative CareChemotherapy
Primary treatment for SCLCTreatment of nonresectable tumors or adjuvant to surgery in NSCLC
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 27

Collaborative CareBiologic and targeted therapy
Erlotinib (Tarceva): Blocks growth stimulating signals in NSCLC cells
Bevacizumab (Avastin): Inhibits angiogenesis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 28

Collaborative CareOther therapies
Prophylactic cranial therapy Bronchoscopic laser therapy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 29

Collaborative CareOther therapies
Photodynamic therapy Airway stenting Cryotherapy
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 30

Nursing ManagementNursing Assessment
Assess patient’s and family’s understanding of diagnostic tests, diagnosis, treatment options, and prognosis.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 31

Nursing ManagementNursing Assessment
Assess level of anxiety.Obtain subjective and objective data.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 32

Nursing ManagementNursing Diagnoses
Ineffective airway clearance
AnxietyAcute pain
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 33

Nursing ManagementNursing Diagnoses
Imbalanced nutrition: Less than body requirements
Ineffective health maintenance
Ineffective breathing pattern
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 34

Nursing ManagementPlanning
Overall goals Effective breathing pattern Adequate airway clearance Adequate oxygenation of tissues
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 35

Nursing ManagementPlanning
Overall goals Minimal to no pain Realistic attitude toward treatment and prognosis
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 36

Nursing ManagementNursing ImplementationHealth promotion
Avoid smoking. Promote smoking cessation programs.
Support education and smoking policies.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 37

Nursing ManagementNursing ImplementationAcute intervention
Offer support during diagnostic evaluation.
Monitor for side effects. Provide comfort.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 38

Nursing ManagementNursing ImplementationAcute intervention
Teach methods to reduce pain.
Educate indications for hospitalization.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 39

Nursing ManagementNursing ImplementationAmbulatory and home care
Follow up carefully for manifestations of metastasis.
Educate patient on signs and symptoms of hemoptysis, dysphagia, chest pain, and hoarseness.
May need information about hospice
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 40

Case Study
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 41

Case Study62-year-old man is diagnosed with stage IIB small cell cancer of the lungs.
He has smoked 2 packs of cigarettes per day for past 40 years.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 42

Case StudyHe is the sole income provider for his wife and two grandchildren.
He has not agreed to chemotherapy and radiation.
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 43

1. How can you attempt to determine the patient’s goals and understanding of the diagnosis?
2. What is the most important thing that can improve the patient’s outcome?
Discussion Questions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 44

3. What can you do to help him with anticipatory guidance if he elects to get treatment?
Discussion Questions
Copyright © 2011, 2007 by Mosby, Inc., an affiliate of Elsevier Inc. 45
Recommended