Reirradiation and Primary Treatment Spine Cases
IAEA Singapore SBRT Symposium
Yoshiya (Josh) Yamada MD FRCPCDepartment of Radiation Onology
Memorial Sloan Kettering Cancer Center
Mechanisms of CNS Damage• Direct injury to normal cells
– Endothelial apoptosis– Oligodendroglial cells most vulnerable
• 10-20Gy x 1 causes apoptosis within hours– Schwann cells most resistant– Poor DS repair of mature neurons and precursors– Inflammation from activated glial cells and monocyte infiltration
• Vascular injury– Endothelial apoptosis within hours and BBB disruption– P53 dependent phenomenon– Increased VEGF
• Immune hypersensitivity response– Antigens released by injured glial cells induce hypersensitivity
response.
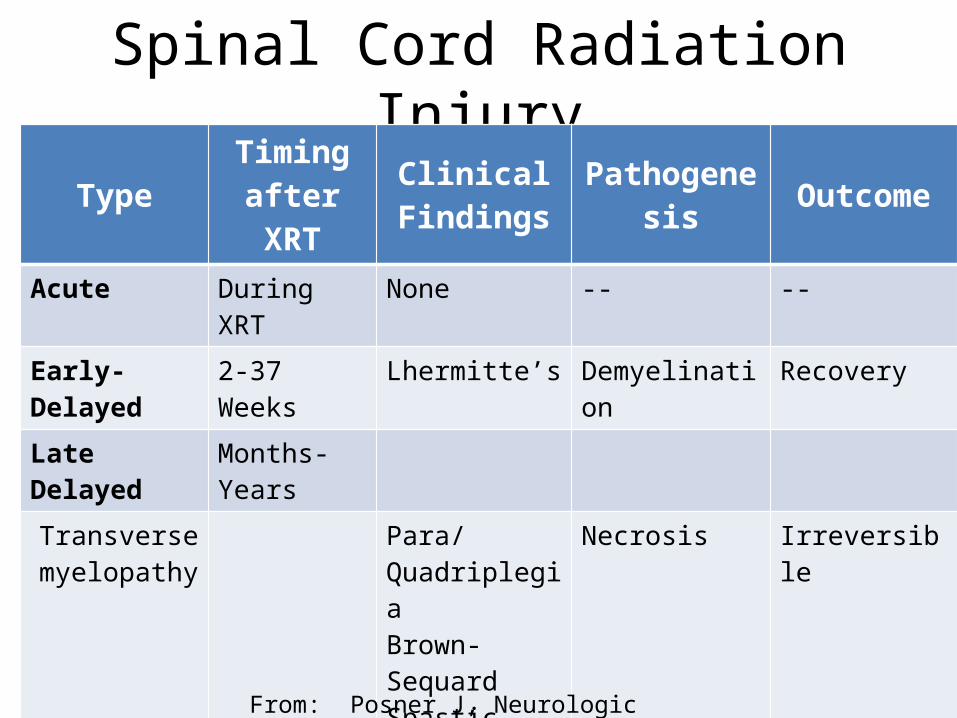
Spinal Cord Radiation InjuryType Timing
after XRTClinical
Findings Pathogenesis Outcome
Acute During XRT None -- --
Early-Delayed 2-37 Weeks Lhermitte’s Demyelination Recovery
Late Delayed Months-Years
Transverse myelopathy
Para/QuadriplegiaBrown-SequardSpastic paraparesis
Necrosis Irreversible
Motor Neuron Dysfunction
Leg Weakness Ventral roots Irreversible
Hemorrhagic myelopathy
8-30 years Acute paraparesis
Telangectasia Reversible
From: Posner J, Neurologic Complications of Cancer, p 525
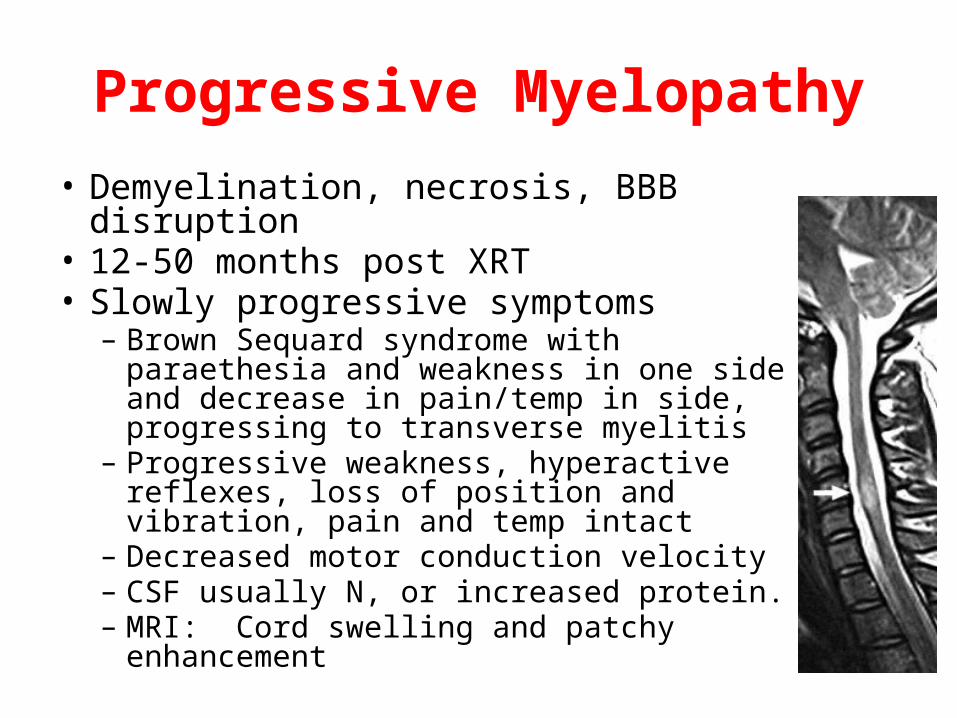
Progressive Myelopathy• Demyelination, necrosis, BBB disruption• 12-50 months post XRT• Slowly progressive symptoms– Brown Sequard syndrome with paraethesia
and weakness in one side and decrease in pain/temp in side, progressing to transverse myelitis
– Progressive weakness, hyperactive reflexes, loss of position and vibration, pain and temp intact
– Decreased motor conduction velocity– CSF usually N, or increased protein.– MRI: Cord swelling and patchy enhancement
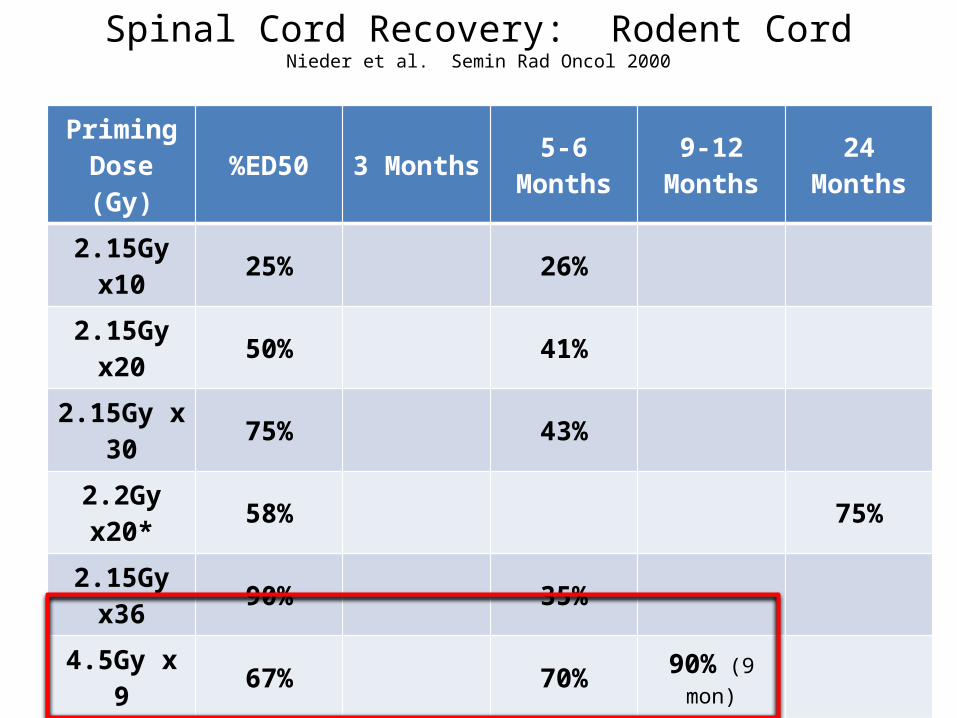
Spinal Cord Recovery: Rodent CordNieder et al. Semin Rad Oncol 2000
Priming Dose (Gy) %ED50 3 Months 5-6 Months 9-12
Months 24 Months
2.15Gy x10 25% 26%2.15Gy x20 50% 41%
2.15Gy x 30 75% 43%
2.2Gy x20* 58% 75%2.15Gy x36 90% 35%4.5Gy x 9 67% 70% 90% (9 mon)
4.5Gy x 12 87% N/A9Gy x 2 47% 20% 35%9Gy x3 71% 16% 33%
10.25Gy x 3 89% 11% 23% 40%
10Gy x1 48% 100%12Gy x1 50% 83%15Gy x1 53% 45%
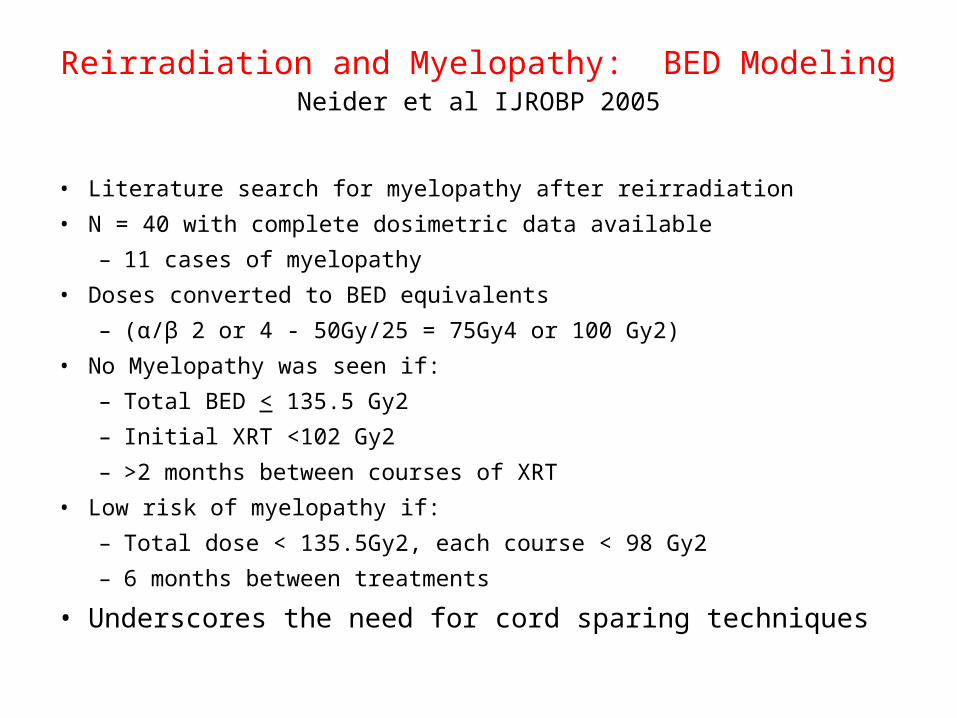
Reirradiation and Myelopathy: BED ModelingNeider et al IJROBP 2005
• Literature search for myelopathy after reirradiation• N = 40 with complete dosimetric data available
– 11 cases of myelopathy• Doses converted to BED equivalents
– (α/β 2 or 4 - 50Gy/25 = 75Gy4 or 100 Gy2)• No Myelopathy was seen if:
– Total BED < 135.5 Gy2– Initial XRT <102 Gy2– >2 months between courses of XRT
• Low risk of myelopathy if:– Total dose < 135.5Gy2, each course < 98 Gy2– 6 months between treatments
• Underscores the need for cord sparing techniques
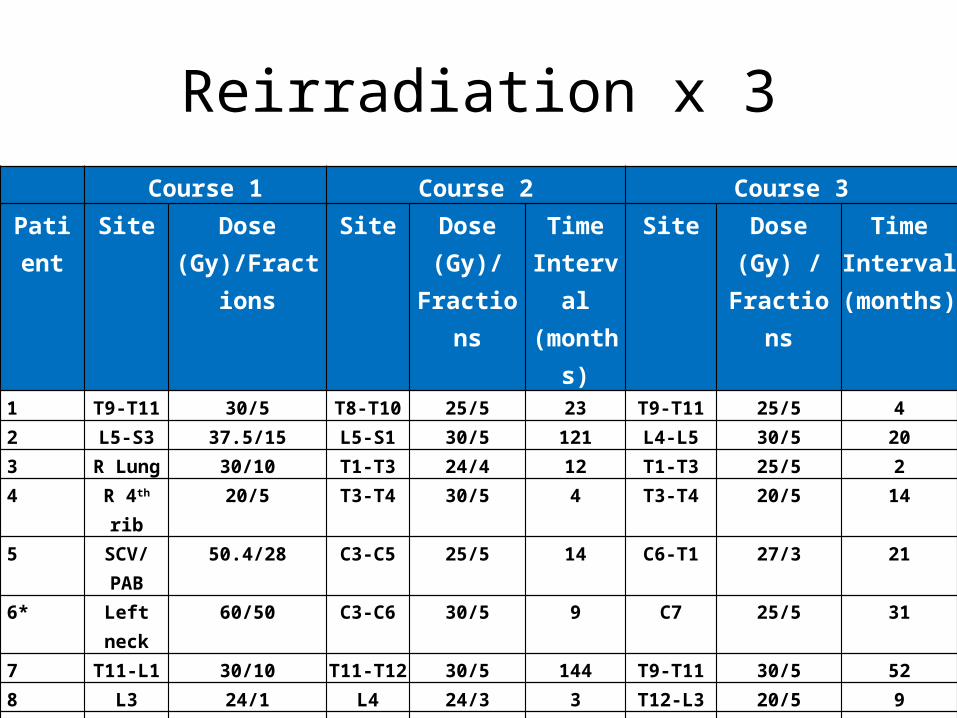
Reirradiation x 3Course 1 Course 2 Course 3
Patient Site Dose (Gy)/Fractions
Site Dose (Gy)/
Fractions
Time Interval
(months)
Site Dose (Gy) /
Fractions
Time Interval
(months)1 T9-T11 30/5 T8-T10 25/5 23 T9-T11 25/5 42 L5-S3 37.5/15 L5-S1 30/5 121 L4-L5 30/5 203 R Lung 30/10 T1-T3 24/4 12 T1-T3 25/5 24 R 4th rib 20/5 T3-T4 30/5 4 T3-T4 20/5 145 SCV/
PAB50.4/28 C3-C5 25/5 14 C6-T1 27/3 21
6* Left neck 60/50 C3-C6 30/5 9 C7 25/5 31
7 T11-L1 30/10 T11-T12 30/5 144 T9-T11 30/5 528 L3 24/1 L4 24/3 3 T12-L3 20/5 99 Lt neck 55.8/31 C7 30/5 8 C6-7 30/5 810 H&N 70/35 C2/BOS 30/3 23 C2 30/5 5
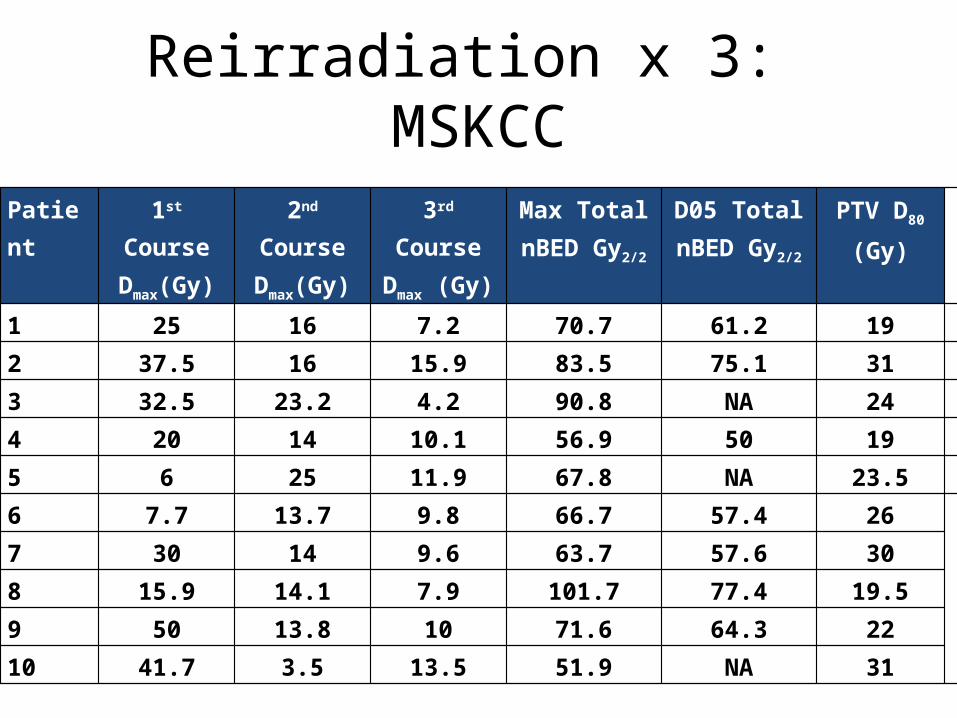
Reirradiation x 3: MSKCC
Patient 1st Course Dmax(Gy)
2nd Course Dmax(Gy)
3rd CourseDmax (Gy)
Max Total nBED Gy2/2
D05 TotalnBED Gy2/2
PTV D80
(Gy)
1 25 16 7.2 70.7 61.2 19
2 37.5 16 15.9 83.5 75.1 31
3 32.5 23.2 4.2 90.8 NA 24
4 20 14 10.1 56.9 50 19
5 6 25 11.9 67.8 NA 23.5
6 7.7 13.7 9.8 66.7 57.4 26
7 30 14 9.6 63.7 57.6 30
8 15.9 14.1 7.9 101.7 77.4 19.5
9 50 13.8 10 71.6 64.3 22
10 41.7 3.5 13.5 51.9 NA 31
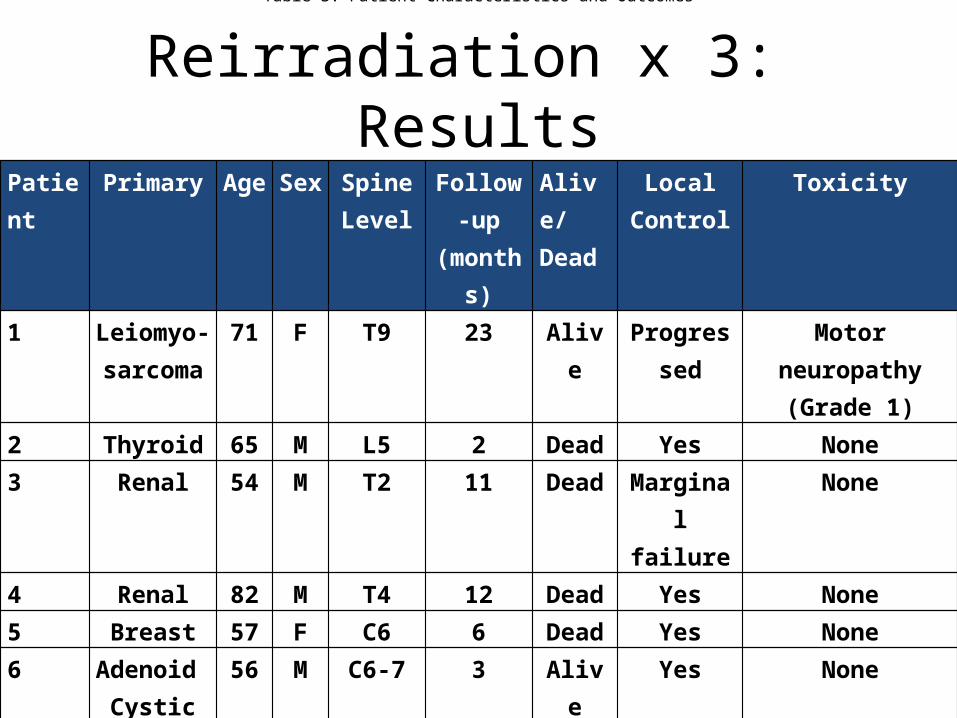
Reirradiation x 3: ResultsPatient Primary Age Sex Spine
LevelFollow-
up (months)
Alive/Dead
Local Control
Toxicity
1 Leiomyo-sarcoma
71 F T9 23 Alive Progressed Motor neuropathy(Grade 1)
2 Thyroid 65 M L5 2 Dead Yes None3 Renal 54 M T2 11 Dead Marginal
failureNone
4 Renal 82 M T4 12 Dead Yes None5 Breast 57 F C6 6 Dead Yes None6 Adenoid
Cystic56 M C6-7 3 Alive Yes None
7 Renal 69 M T11 3 Alive Yes None8 Leiomyo-
sarcoma45 F L3 23 Alive Yes Foot drop
(Grade 2)9 Ewings 16 M C6-7 8 Alive Yes None10 Spindle Cell 65 F C2 2 Alive Yes None
Table 3: Patient Characteristics and Outcomes
Quantec: Spinal Cord ReirradiationKirkpatrick et al IJROBP 2010
• Most data on reirradiation with a minimum interval of at least 6 months
• Volume effects:– At 2 Gy equivalents, full circumference cord dose, at least
25% recovery at 6 months– With SBRT (partial cord) 13Gy/1 or 20Gy/3 < 1% risk of
myelopathy
• Impact of systemic therapy unknown
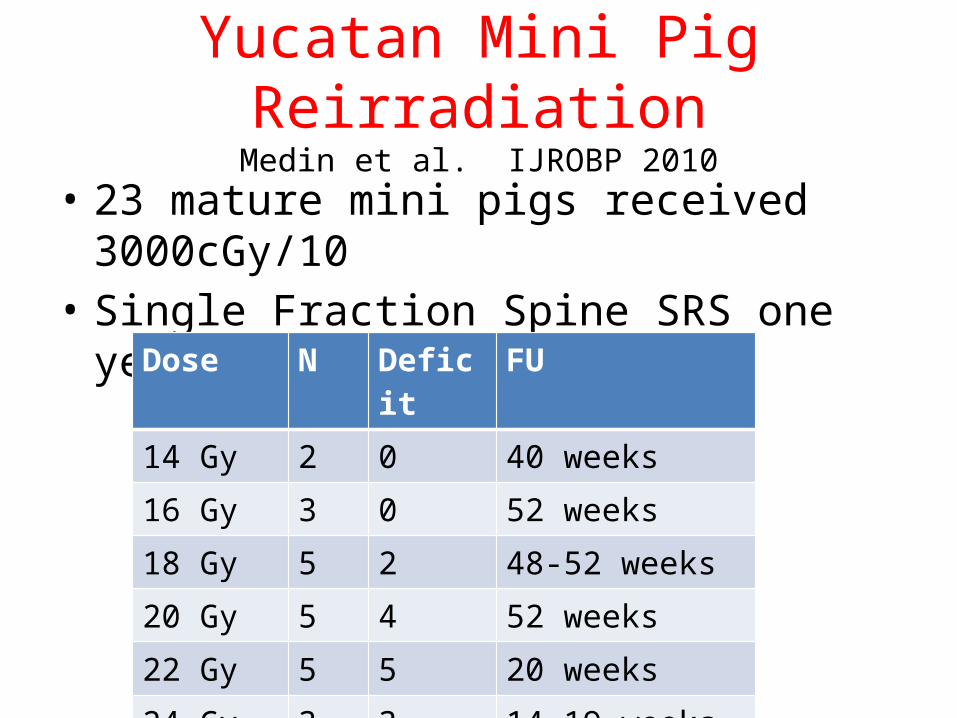
Yucatan Mini Pig ReirradiationMedin et al. IJROBP 2010
• 23 mature mini pigs received 3000cGy/10• Single Fraction Spine SRS one year later
Dose N Deficit FU
14 Gy 2 0 40 weeks
16 Gy 3 0 52 weeks
18 Gy 5 2 48-52 weeks
20 Gy 5 4 52 weeks
22 Gy 5 5 20 weeks
24 Gy 3 3 14-19 weeks
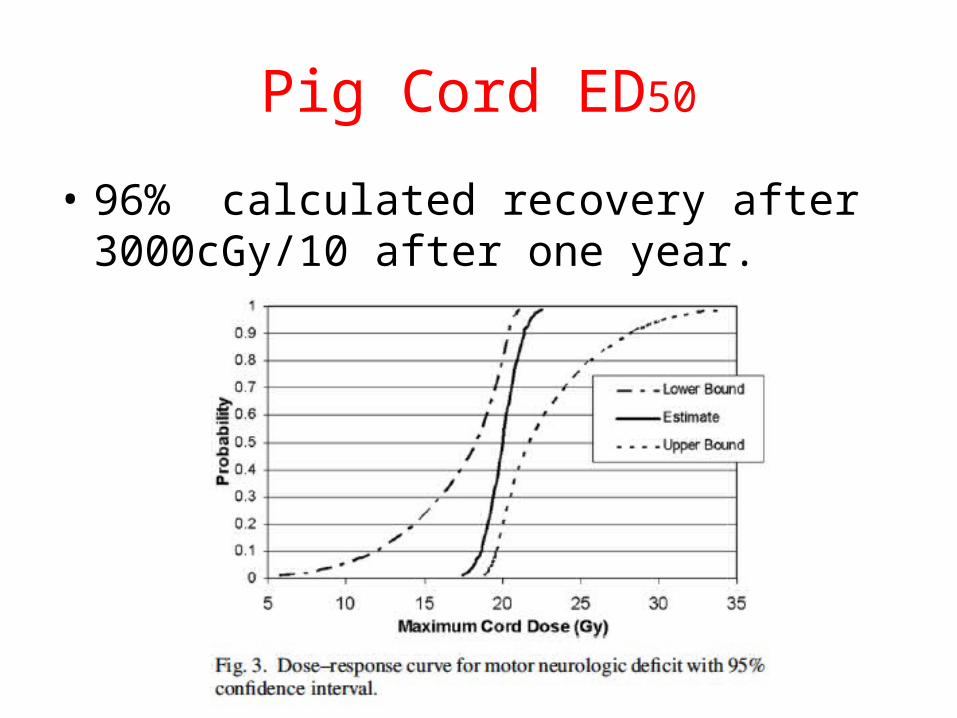
Pig Cord ED50
• 96% calculated recovery after 3000cGy/10 after one year.
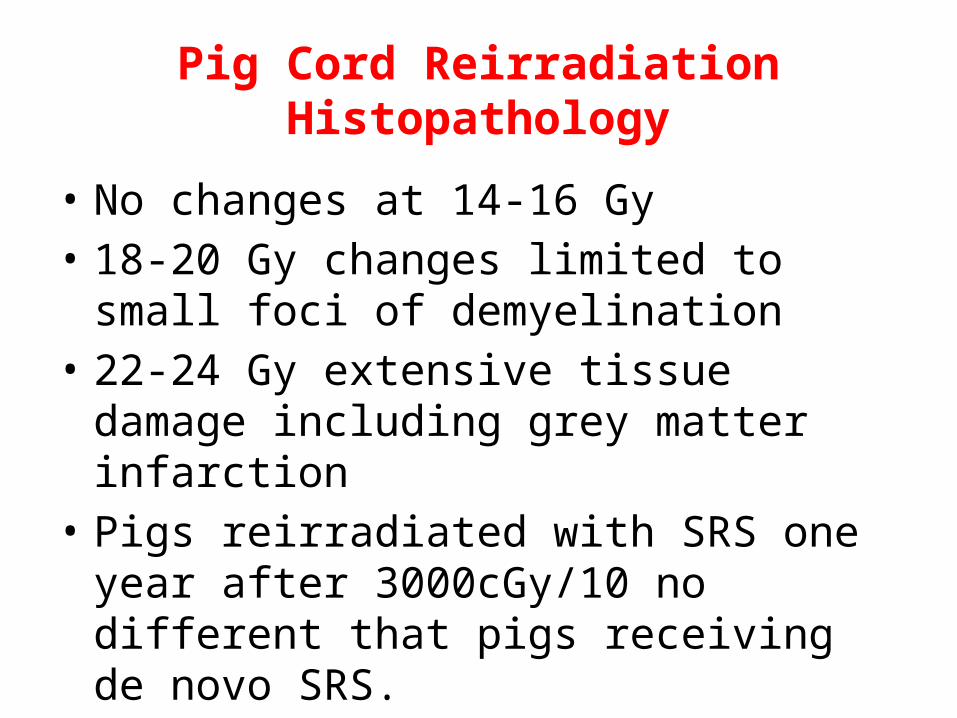
Pig Cord Reirradiation Histopathology
• No changes at 14-16 Gy• 18-20 Gy changes limited to small foci of
demyelination• 22-24 Gy extensive tissue damage including
grey matter infarction• Pigs reirradiated with SRS one year after
3000cGy/10 no different that pigs receiving de novo SRS.
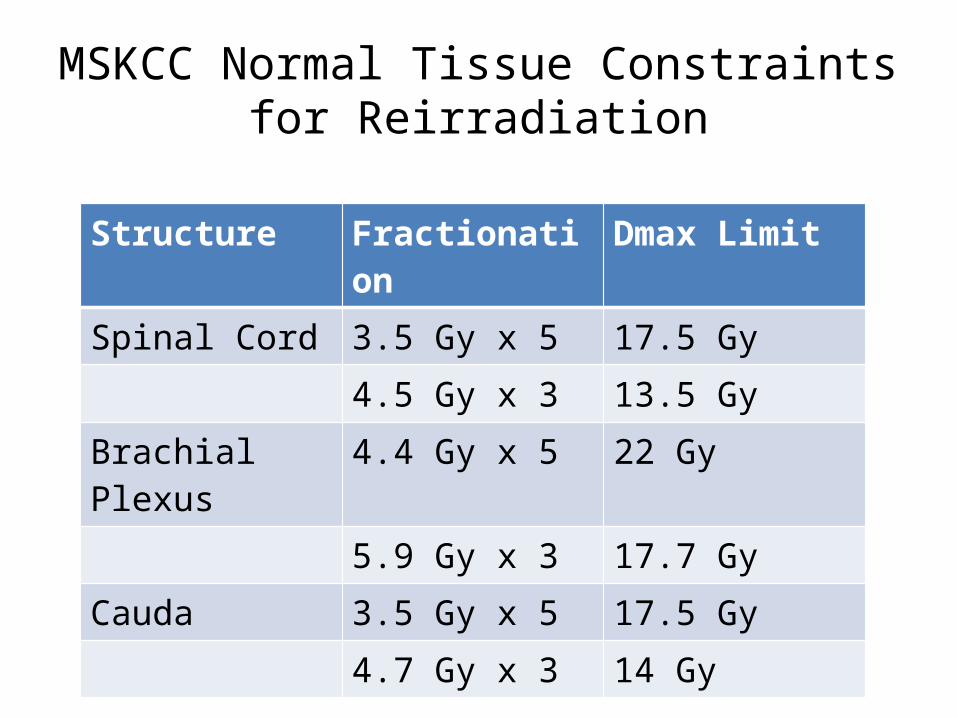
MSKCC Normal Tissue Constraints for Reirradiation
Structure Fractionation Dmax Limit
Spinal Cord 3.5 Gy x 5 17.5 Gy
4.5 Gy x 3 13.5 Gy
Brachial Plexus 4.4 Gy x 5 22 Gy
5.9 Gy x 3 17.7 Gy
Cauda 3.5 Gy x 5 17.5 Gy
4.7 Gy x 3 14 Gy
Salvage Spine Radiation
• Local control of spine metastases after conventional radiation is 20-60%
• Durability of symptom control for conventionally fractionated spine XRT is low (median 2.5 – 3 months-Patchell and Maranzano)
• Systemic therapy is often less effective in treating spine metastases
• Recurrence is often highly symptomatic• Surgical salvage can be morbid and recurrence rates
are high without adjuvant therapy
Rationale for Hypofractionation
• By definition, recurrent tumors are resistant to conventional XRT
• Hypofractionation represents a different radiobiologic approach to treatment
• IGRT is the best vehicle to deliver high dose radiation near the spinal cord/esophagus
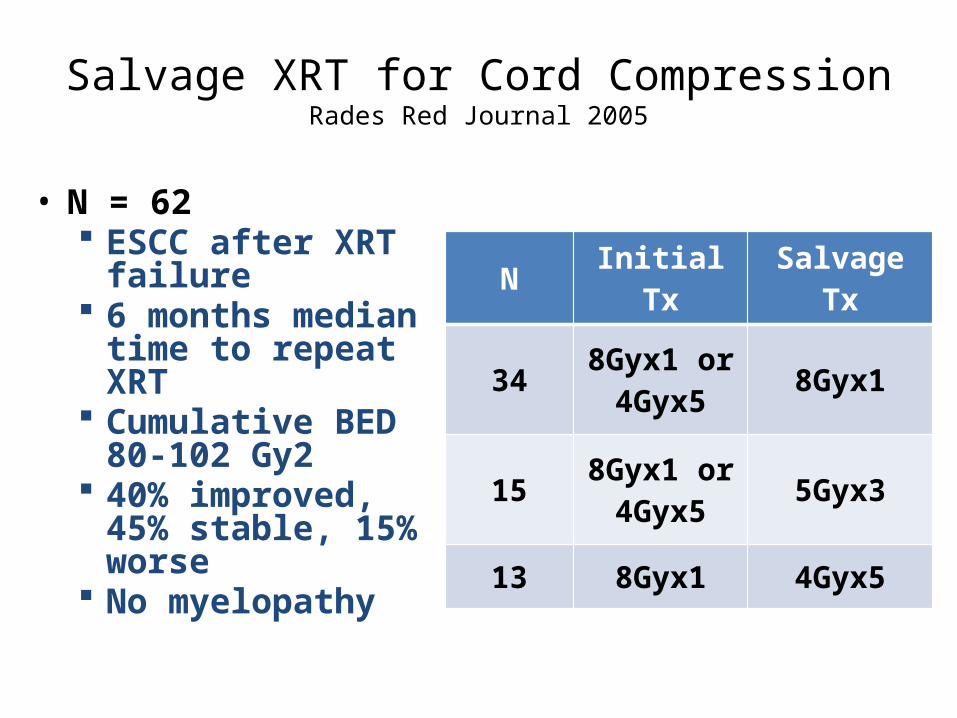
Salvage XRT for Cord CompressionRades Red Journal 2005
• N = 62 ESCC after XRT
failure 6 months median
time to repeat XRT Cumulative BED 80-
102 Gy2 40% improved, 45%
stable, 15% worse No myelopathy
N Initial Tx Salvage Tx
34 8Gyx1 or 4Gyx5 8Gyx1
15 8Gyx1 or 4Gyx5 5Gyx3
13 8Gyx1 4Gyx5
SRS vs Conventional XRT
• Differences in volumes• Steep dose fall off• Single fraction or hypofractionation vs.
conventional fraction sizes
Radiation Myelopathy After Spine SRS
• N=6/1075• Mean of 6.3 months (2-9 months)• 2 patients had prior RT (39.6Gy/22, 50.4Gy/28
70 and 80 months prior)• 20-21 Gy/2 fractions, 20Gy/2-14Gy/2 cord
Dmax– Both had prior chemotx– Progression to paraplegia, walker dependent.
Gibbs et al, Neursurgery, 2009
Salvage SRS After Spine XRT FailureGerzsten et al. Spine 2007
• N = 393• Prior XRT = 3Gy x10 or 2.5Gy x14• 20Gy x1 (12.5-25Gy) mean dose to 80%• Median FU = 21 months (3-53)• 88% local control, 86% dural pain palliation• No cases of myelitis
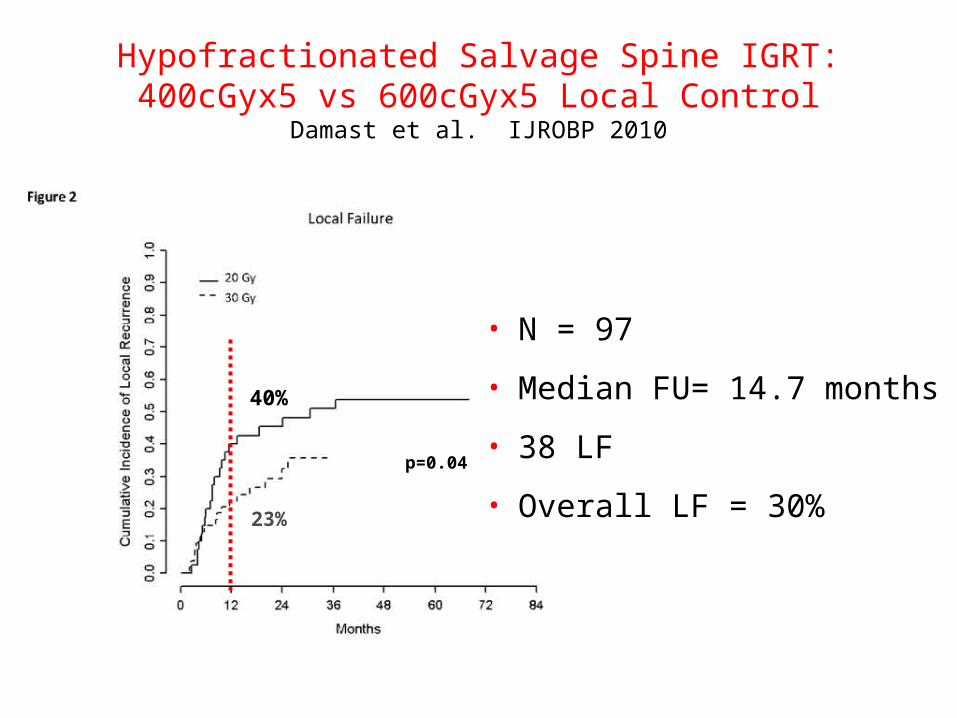
Hypofractionated Salvage Spine IGRT: 400cGyx5 vs 600cGyx5 Local Control
Damast et al. IJROBP 2010
p=0.04
23%
40%
• N = 97
• Median FU= 14.7 months
• 38 LF
• Overall LF = 30%
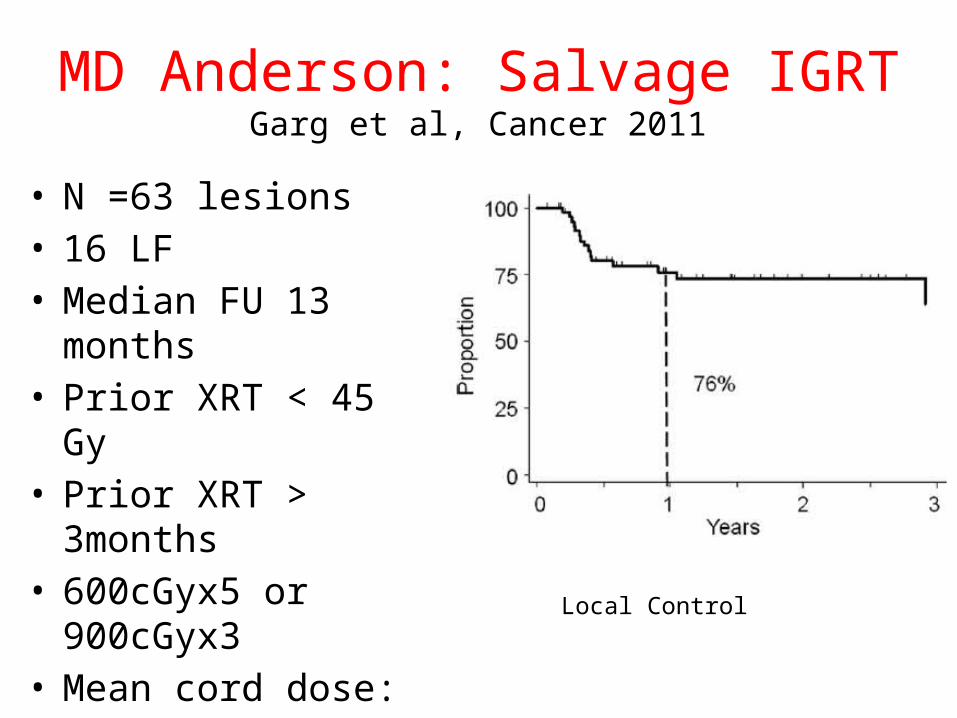
MD Anderson: Salvage IGRTGarg et al, Cancer 2011
• N =63 lesions• 16 LF• Median FU 13 months• Prior XRT < 45 Gy• Prior XRT > 3months• 600cGyx5 or 900cGyx3• Mean cord dose: 10 Gy
Local Control
Reirradiation Spinal Cord Summary
• Animal data suggests that reirradiation of the spinal cord is feasible– Significant repair of radiation does occur• Dose dependent• Volume dependent• Time dependent
• Clinical data is of poor quality• Repeat radiotherapy is effective palliation• Risk of myelitis is low• SRS is safe after conventional radiation failure
Spine Reirradiation Summary
• There is mounting evidence that:• Spinal cord is likely capable of radiation repair over
time– Cord recovery occurs after prior XRT – 6-12 months– Pig data: Steep complication curve slope!
• Spine reirradiation is safe and an effective salvage treatment.– Both single fraction or hypofractionated– 75% durable successful salvage rates
Recommendations
• Careful and meticulous treatment planning and delivery is crucial– Accurate cord deliniation (ie myelogram)
• Minimum of 6 months between initial and salvage XRT for spinal cord recovery
• Maximum cord doses should be less than 17.5 Gy/3 fractions
• Detailed and well documented discussion with patients about potential complications
Compression/Burst FractureAxial Load Pain
•64 year old male with stage IV thyroid cancer•Prior I 131 treatment•T6 burst fracture•Systemic disease otherwise well controlled•Increased pain with sitting to standing•No myelopathy
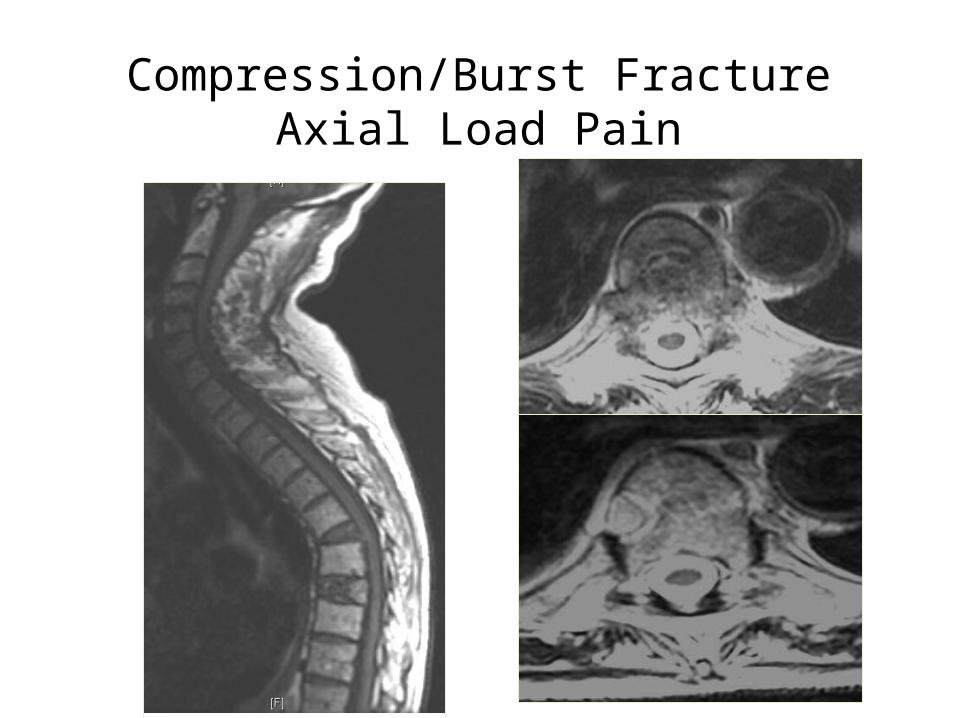
Compression/Burst FractureAxial Load Pain
Compression/Burst FractureAxial Load Pain
• Axial Load Pain: No gross instabilityPercutaneous cement augmentationVertebroplastyKyphoplasty
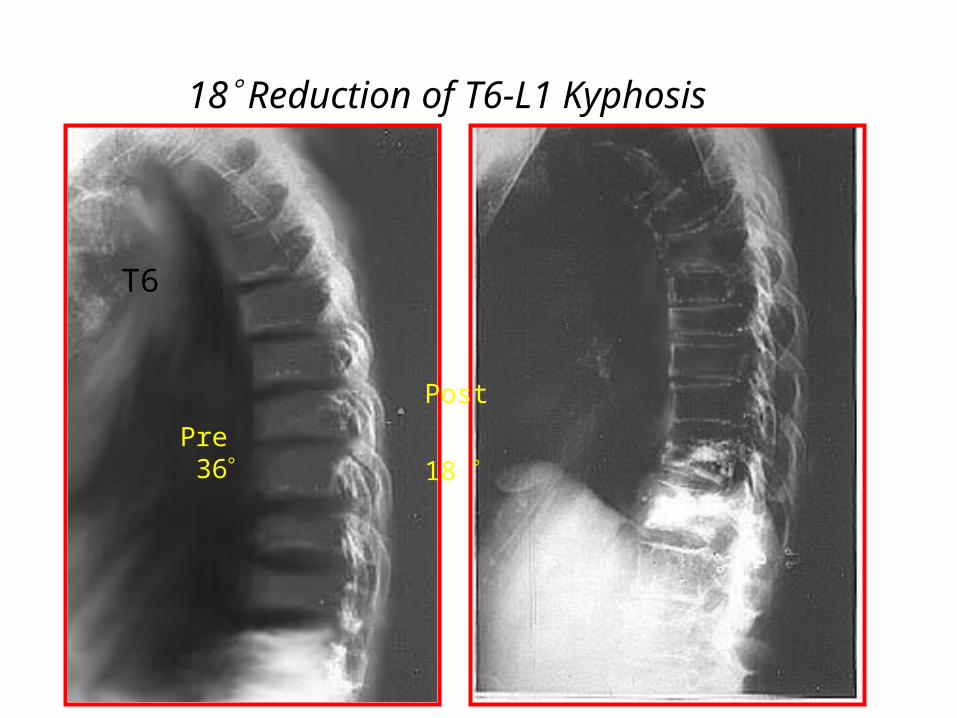
18 Reduction of T6-L1 Kyphosis
T6
L1
T6
Post
18 Pre 36
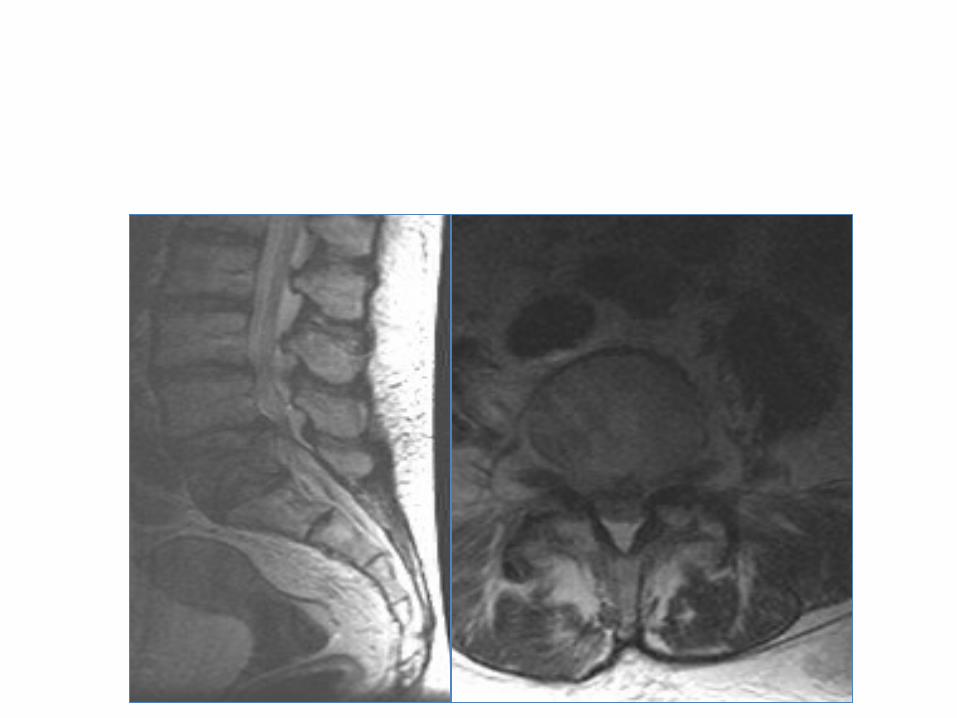
Melanoma L5 with mechanical radiculopathy
•54 year old male with long standing melanoma•4 month history of progressive lower back pain, 3 week history of pain radiating down the right leg, laterally below the knee to ankle in L5 distribution•Motor intact•Pain worse with weight bearing, 8/10•Visceral metastases to liver and lung, “stable”•KPS 80, able to tolerate any treatment•No prior RT
Treatment options?
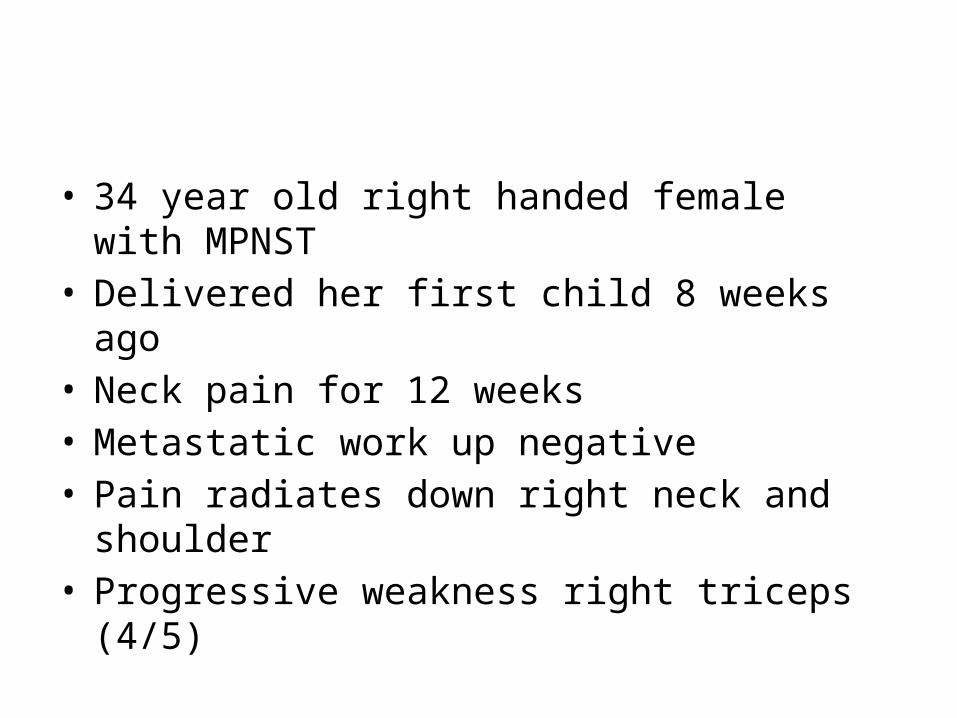
• 34 year old right handed female with MPNST• Delivered her first child 8 weeks ago• Neck pain for 12 weeks• Metastatic work up negative• Pain radiates down right neck and shoulder• Progressive weakness right triceps (4/5)
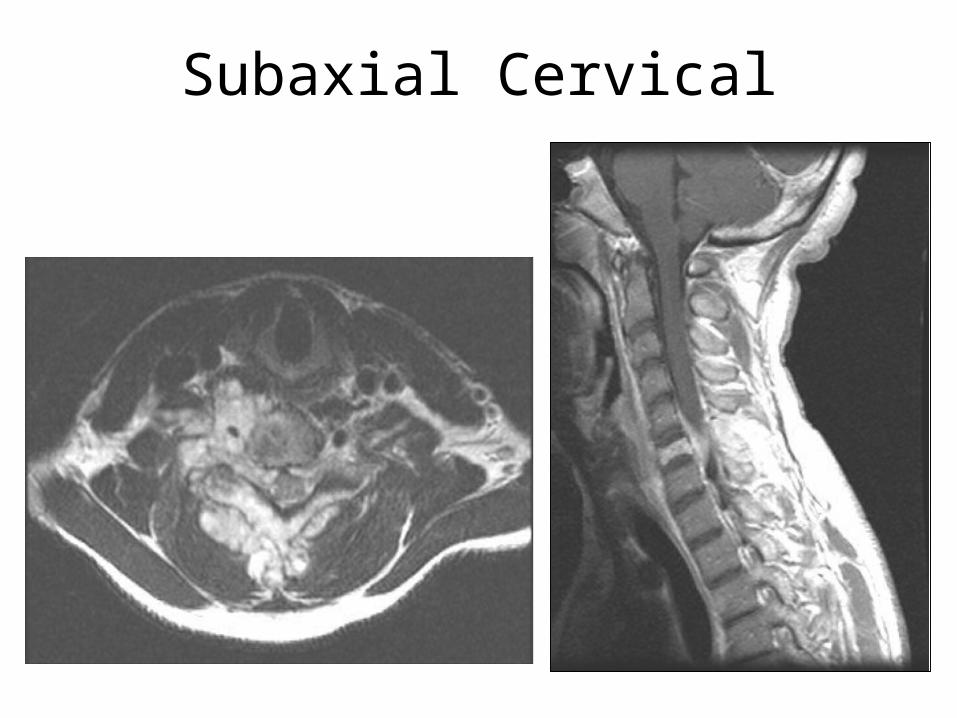
Subaxial Cervical
Treatment Options?
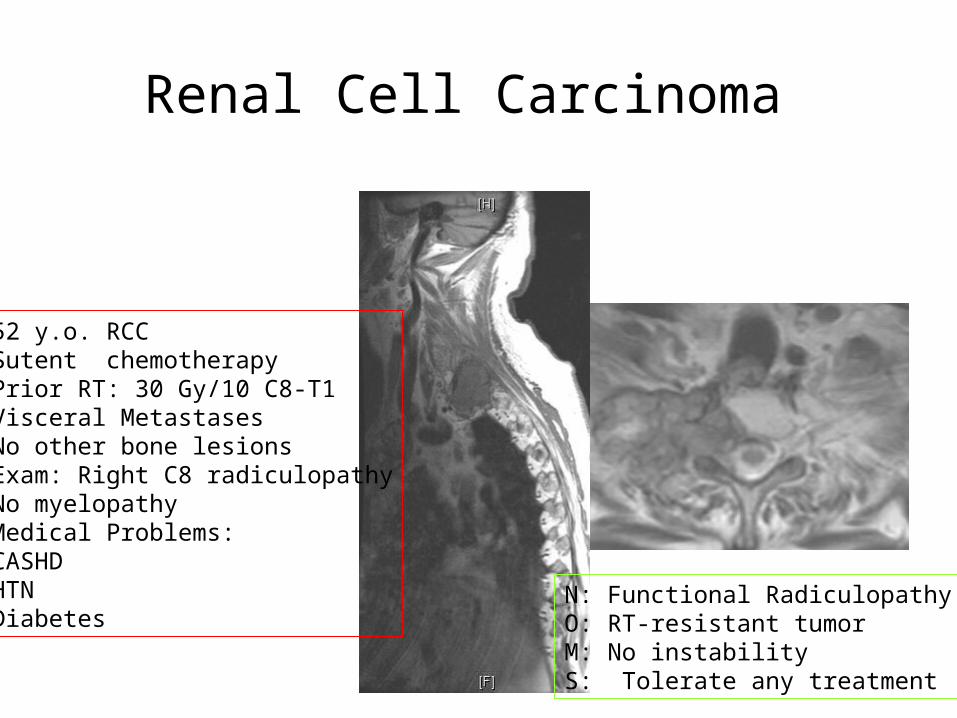
Renal Cell Carcinoma
52 y.o. RCCSutent chemotherapyPrior RT: 30 Gy/10 C8-T1Visceral MetastasesNo other bone lesionsExam: Right C8 radiculopathyNo myelopathyMedical Problems:CASHDHTN Diabetes
N: Functional RadiculopathyO: RT-resistant tumorM: No instabilityS: Tolerate any treatment
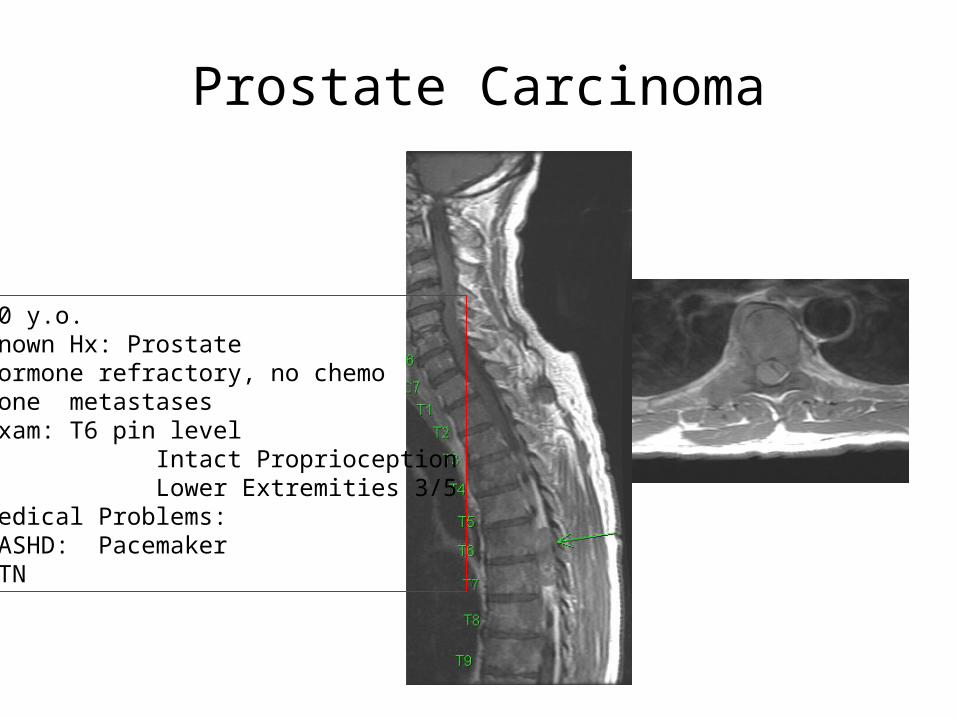
Prostate Carcinoma
60 y.o.Known Hx: ProstateHormone refractory, no chemoBone metastasesExam: T6 pin level Intact Proprioception Lower Extremities 3/5Medical Problems: CASHD: PacemakerHTN
Subaxial Cervical
56 year old with stage IV breast ca 3 month history of neck pain, able to flex
rotate and extend the neck Pain radiates to the right shoulder Hand function intact No myelopathy
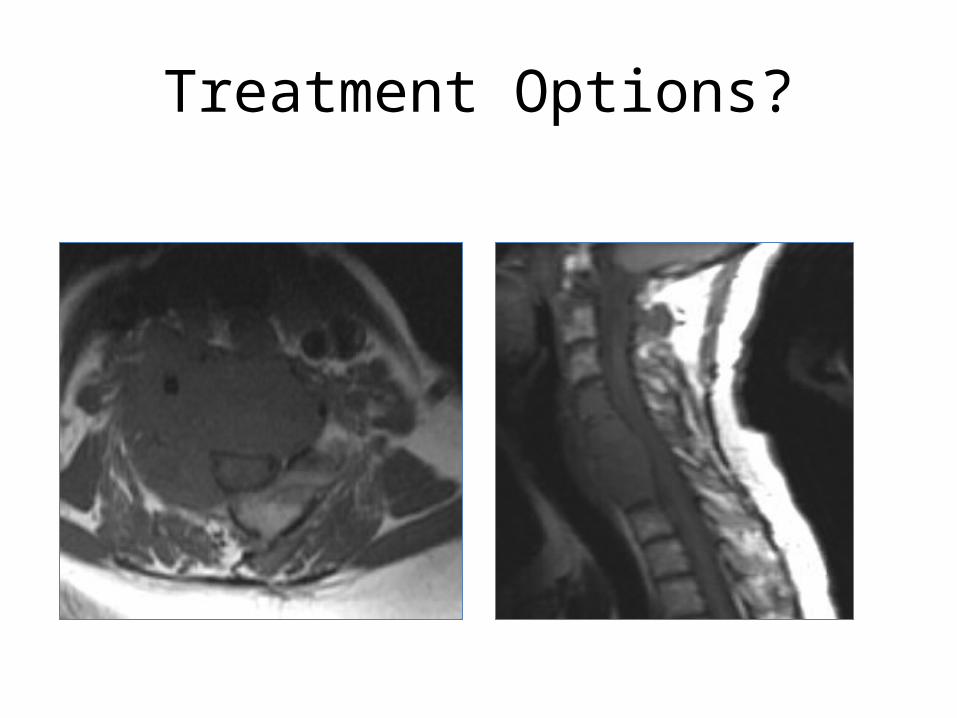
Treatment Options?
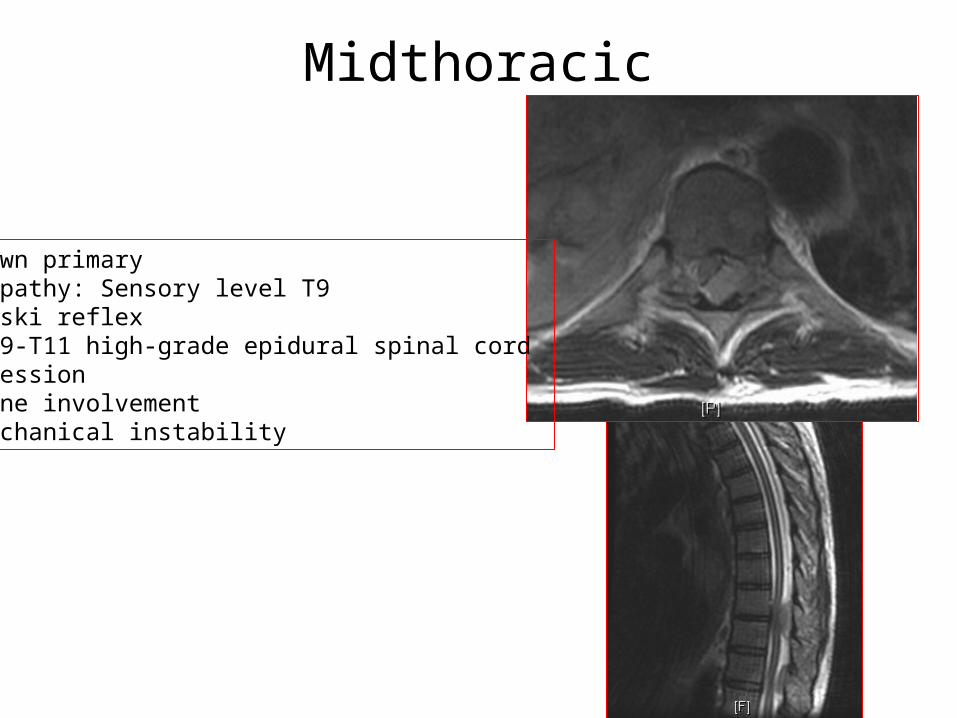
Midthoracic
Unknown primaryMyelopathy: Sensory level T9Babinski reflexMRI T9-T11 high-grade epidural spinal cord CompressionNo bone involvementNo mechanical instability
Recommended











![Current status and recent advances in reirradiation of ......2-year survival rate of 26.5%, respectively [1]. However, almost all GBMs relapse within or in close proximity to the initial](https://img.pdfslide.us/doc/110x75/613bd738f8f21c0c826939cf/current-status-and-recent-advances-in-reirradiation-of-2-year-survival-rate.jpg)





