T he aim of this five part series is togive you a basic system for lookingat chest x ray films. They should
enable you to say something sensiblewhen presented with a film in your finalsand be confident that you are not missingserious disease when you view a film onyour own as a house officer.
Looking at chest x ray films—thesystemBy the time you do finals you will havelearnt a system for examining theabdomen; you also need to develop a sys-tem for looking at x ray films. This willreduce your chances of missing abnor-malities and it will provide a structuredpatter to come out with in exams whenyou are under pressure.
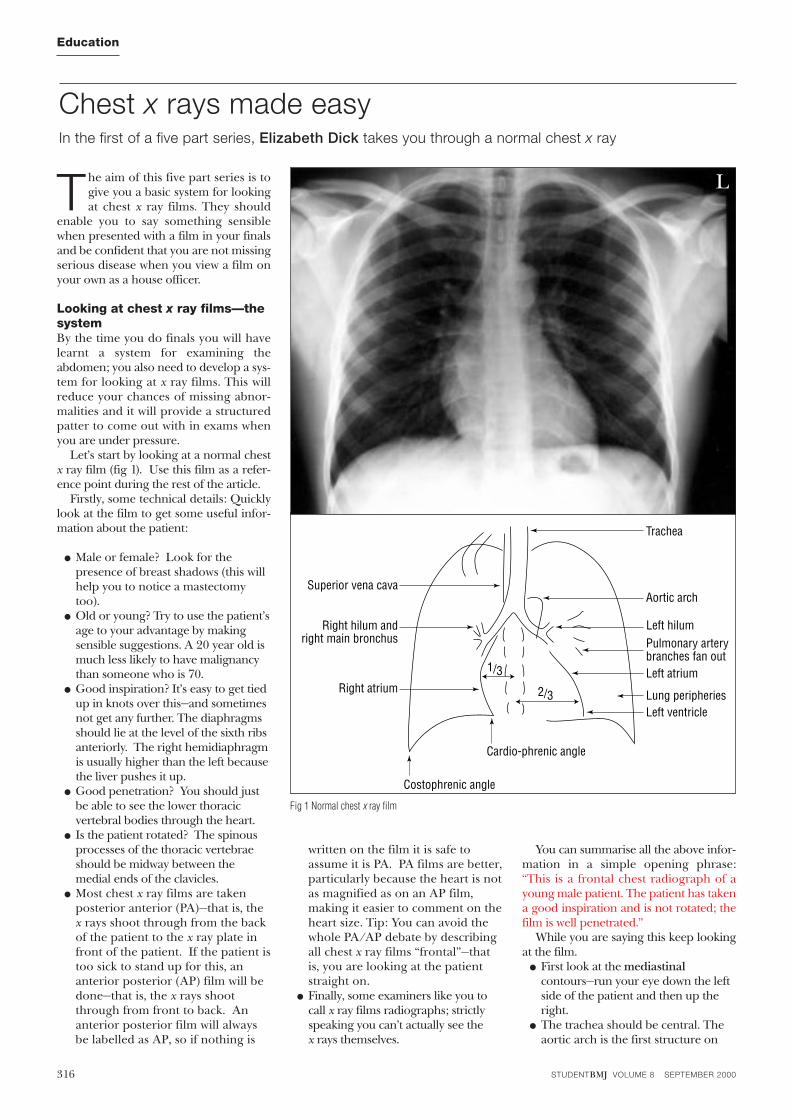
Let’s start by looking at a normal chestx ray film (fig 1). Use this film as a refer-ence point during the rest of the article.
Firstly, some technical details: Quicklylook at the film to get some useful infor-mation about the patient:
● Male or female? Look for thepresence of breast shadows (this willhelp you to notice a mastectomytoo).
● Old or young? Try to use the patient’sage to your advantage by makingsensible suggestions. A 20 year old ismuch less likely to have malignancythan someone who is 70.
● Good inspiration? It’s easy to get tiedup in knots over this—and sometimesnot get any further. The diaphragmsshould lie at the level of the sixth ribsanteriorly. The right hemidiaphragmis usually higher than the left becausethe liver pushes it up.
● Good penetration? You should justbe able to see the lower thoracicvertebral bodies through the heart.
● Is the patient rotated? The spinousprocesses of the thoracic vertebraeshould be midway between themedial ends of the clavicles.
● Most chest x ray films are takenposterior anterior (PA)—that is, thex rays shoot through from the backof the patient to the x ray plate infront of the patient. If the patient istoo sick to stand up for this, ananterior posterior (AP) film will bedone—that is, the x rays shootthrough from front to back. Ananterior posterior film will alwaysbe labelled as AP, so if nothing is
written on the film it is safe toassume it is PA. PA films are better,particularly because the heart is notas magnified as on an AP film,making it easier to comment on theheart size. Tip: You can avoid thewhole PA/AP debate by describingall chest x ray films “frontal”—thatis, you are looking at the patientstraight on.
● Finally, some examiners like you tocall x ray films radiographs; strictlyspeaking you can’t actually see the x rays themselves.
You can summarise all the above infor-mation in a simple opening phrase: “This is a frontal chest radiograph of ayoung male patient. The patient has takena good inspiration and is not rotated; thefilm is well penetrated.”
While you are saying this keep lookingat the film.● First look at the mediastinal
contours—run your eye down the leftside of the patient and then up theright.
● The trachea should be central. Theaortic arch is the first structure on
Chest x rays made easyIn the first of a five part series, Elizabeth Dick takes you through a normal chest x ray
316
Education
STUDENTBMJ VOLUME 8 SEPTEMBER 2000
Fig 1 Normal chest x ray film
Superior vena cava
Right hilum andright main bronchus
Right atrium
Cardio-phrenic angle
1/3
2/3
Trachea
Aortic arch
Left hilumPulmonary arterybranches fan outLeft atrium
Lung peripheriesLeft ventricle
Costophrenic angle
L

317
Education
STUDENTBMJ VOLUME 8 SEPTEMBER 2000
the left, followed by the leftpulmonary artery; notice how youcan trace the pulmonary arterybranches fanning out through thelung (see fig 1).
● Two thirds of the heart lies on the leftside of the chest, with one third onthe right. The heart should take upno more than half of the thoraciccavity. The left border of the heart ismade up by the left atrium and leftventricle.
● The right border is made up by theright atrium alone (the right ventriclesits anteriorly and therefore does nothave a border on the PA chest x rayfilm—a question that examiners loveto ask. Above the right heart borderlies the edge of the superior venacava.
● The pulmonary arteries and mainbronchi arise at the left and righthila. Enlarged lymph nodes canalso occur here, as can primarytumours. These make the hilumseem bulky—note the normal size ofthe hila on this film.
● Now look at the lungs. Apart fromthe pulmonary vessels (arteries andveins), they should be black(because they are full of air). Scanboth lungs, starting at the apicesand working down, comparing leftwith right at the same level, just asyou would when listening to thechest with your stethoscope. Thelungs extend behind the heart, solook here too. Force your eye tolook at the periphery of the lungs—you should not see many lungmarkings here; if you do then there
may be disease of the air spaces orinterstitium. Don’t forget to lookfor a pneumothorax—in which caseyou would see the sharp line of theedge of the lung.
● Make sure you can see the surface ofthe hemidiaphragms curvingdownwards, and that thecostophrenic and cardiophrenicangles are not blunted—suggesting aneffusion. Check there is no free airunder the hemidiaphragm.
● Finally look at the soft tissues andbones. Are both breast shadowspresent? Is there a rib fracture? Thiswould make you look even harderfor a pneumothorax. Are the bonesdestroyed or sclerotic? (see fig 2)
You can summarise your findings as youare looking: “The trachea is central, themediastinum is not displaced. The medi-astinal contours and hila seem normal.The lungs seem clear, with no pneumo-thorax. There is no free air under thediaphragm. The bones and soft tissuesseem normal.”
If you have not seen any abnormality bythis point, say so—“I have not yet identifiedan abnormality so I will now look throughmy review areas”—and then look at the“review areas”—places where you can easily miss disease. These are:
apices, periphery of the lungs, underand behind the hemidiaphragms(don’t forget the lungs will extendhere), and behind the heart.
By the time you have gone throughthe above, showing that you are lookingat the film in a logical fashion, the examiner should guide you towards theabnormality.
You may be shown a lateral chest x ray (see fig 3), usually to confirm adiagnosis you have made on the PAfilm. Therefore don’t panic when thelateral goes up because it means you’veprobably made the diagnosis. There areonly two spaces to look at on the later-al film.
The heart lies antero-inferiorly. Lookat the area anterior and superior to theheart. This should be black, because itcontains aerated lung. Similarly the areaposterior to the heart should be blackright down to the hemidiaphragms. Theblackness in these two areas should beequivalent; therefore you can compareone with the other. If the area anteriorand superior to the heart is opacified,suspect disease in the anterior medi-astinum or upper lobes. If the area pos-terior to the heart is opacified suspectcollapse or consolidation in the lowerlobes.
Elizabeth Dick specialist registrar in radiology NorthThames Deanery
Acknowledgements: I would like to thank Dr Anju Sahdev,Dr Brian Holloway, and Dr Robert Dick for contributingsome of the films shown. Many thanks to Dr DianaFairclough, Dr Robert Dick, and Dr Alex Leff for their help-ful comments reviewing these articles.
Fig 2 Sclerotic—white metastasis in the right seventh rib
Fig 3 Lateral chest x ray (normal)
L
A

STUDENTBMJ VOLUME 8 OCTOBER 2000 studentbmj.com358
Chest x rays made easyIn the second of a five part series, Elizabeth Dick begins to look at chest abnormalities, starting with themediastinum and heart
Education
Superior vena cava
Right hilum andright main bronchus
Right atrium
Cardio-phrenic angle
1/3
2/3
Trachea
Aortic arch
Left hilumPulmonary arterybranches fan outLeft atrium
Lung peripheriesLeft ventricle
Costophrenic angle
Fig 1 Normal chest x ray film
The basics of looking at a chest x ray (recap):
●First look at the mediastinal contours—runyour eye down the left side of the patientand then up the right.
●The trachea should be central. The aorticarch is the first structure on the left,followed by the left pulmonary artery;notice how you can trace the pulmonaryartery branches fanning out through thelung (see figure 1).
●Two thirds of the heart lies on the left sideof the chest, with one third on the right.The heart should take up no more thanhalf of the thoracic cavity. The left borderof the heart is made up by the left atriumand left ventricle.
●The right border is made up by the rightatrium alone. Above the right heart borderlies the edge of the superior vena cava.
●The pulmonary arteries and main bronchiarise at the left and right hila. Enlargedlymph nodes can also occur here, as canprimary tumours. These make the hilumseem bulky—note the normal size of thehila on this film.
●Now look at the lungs. Apart from thepulmonary vessels (arteries and veins),they should be black (because they are fullof air). Scan both lungs, starting at theapices and working down, comparing leftwith right at the same level, just as youwould when listening to the chest withyour stethoscope. The lungs extend behindthe heart, so look here too. Force your eyeto look at the periphery of the lungs—youshould not see many lung markings here;if you do then there may be disease of theair spaces or interstitium. Don’t forget tolook for a pneumothorax.
●Make sure you can see the surface of thehemidiaphragms curving downwards, andthat the costophrenic and cardiophrenicangles are not blunted—suggesting aneffusion. Check there is no free air underthe hemidiaphragm.
●Finally, look at the soft tissues and bones.Are both breast shadows present? Is therea rib fracture? This would make you lookeven harder for a pneumothorax. Are thebones destroyed or sclerotic?
Presenting the filmYou can summarise your findings in a few sentences: “The trachea is central, themediastinum is not displaced. The mediastinal contours and hila seem normal. The lungsseem clear, with no pneumothorax. There is no free air under the diaphragm. The bonesand soft tissues seem normal.”
STUDENTBMJ VOLUME 8 OCTOBER 2000 studentbmj.com 359
Education
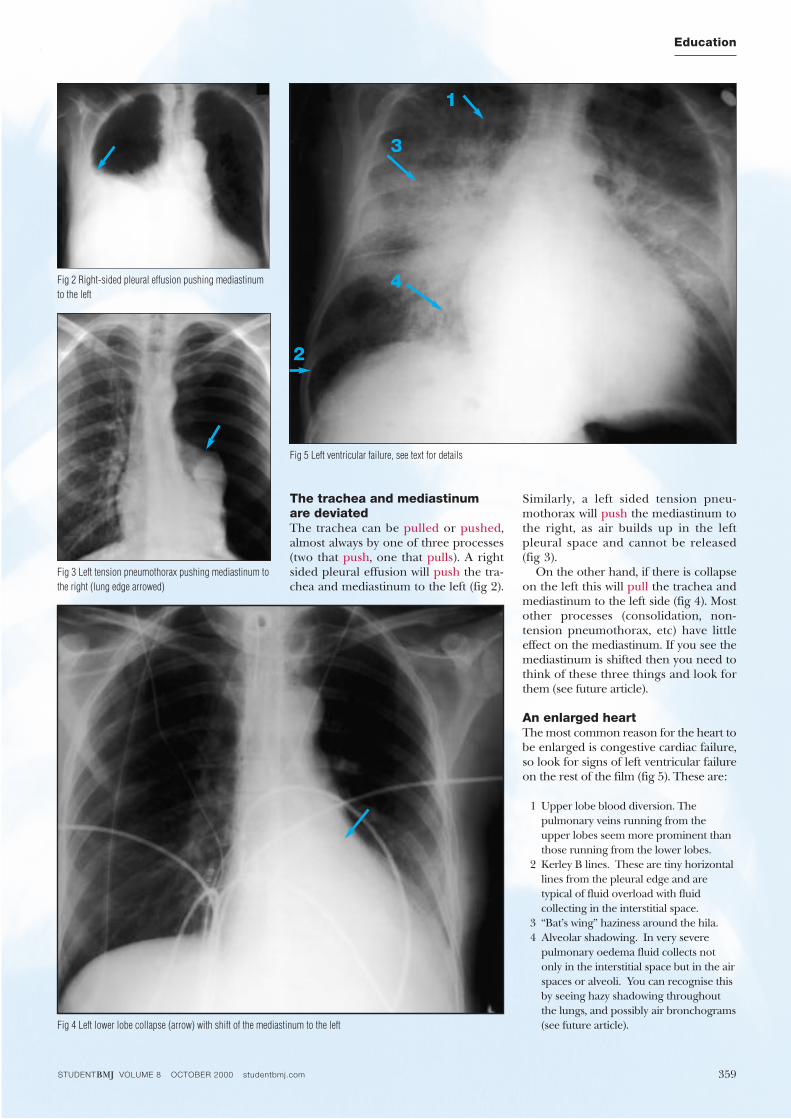
The trachea and mediastinum are deviatedThe trachea can be pulled or pushed,almost always by one of three processes(two that push, one that pulls). A rightsided pleural effusion will push the tra-chea and mediastinum to the left (fig 2).
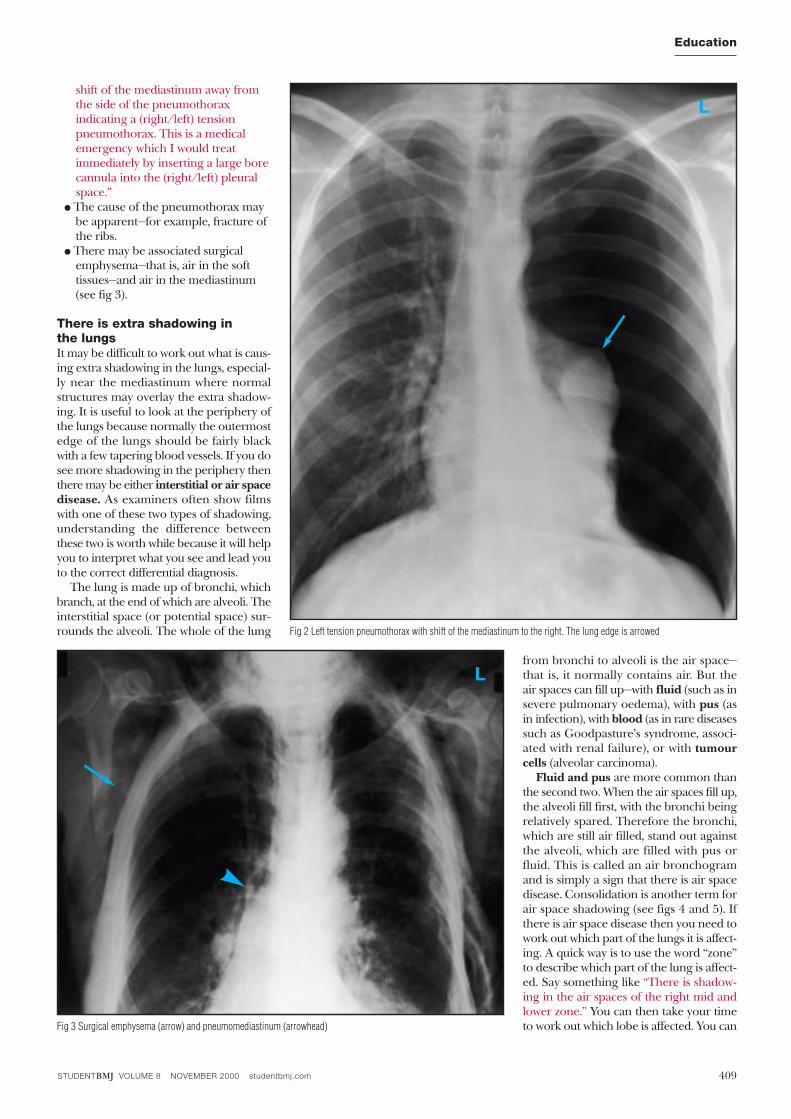
Similarly, a left sided tension pneu-mothorax will push the mediastinum tothe right, as air builds up in the leftpleural space and cannot be released(fig 3).
On the other hand, if there is collapseon the left this will pull the trachea andmediastinum to the left side (fig 4). Mostother processes (consolidation, non-tension pneumothorax, etc) have littleeffect on the mediastinum. If you see themediastinum is shifted then you need tothink of these three things and look forthem (see future article).
An enlarged heartThe most common reason for the heart tobe enlarged is congestive cardiac failure,so look for signs of left ventricular failureon the rest of the film (fig 5). These are:
1 Upper lobe blood diversion. Thepulmonary veins running from theupper lobes seem more prominent thanthose running from the lower lobes.
2 Kerley B lines. These are tiny horizontallines from the pleural edge and aretypical of fluid overload with fluidcollecting in the interstitial space.
3 “Bat’s wing” haziness around the hila.4 Alveolar shadowing. In very severe
pulmonary oedema fluid collects notonly in the interstitial space but in the airspaces or alveoli. You can recognise thisby seeing hazy shadowing throughoutthe lungs, and possibly air bronchograms(see future article).
Fig 5 Left ventricular failure, see text for details
1
3
4
2
Fig 2 Right-sided pleural effusion pushing mediastinumto the left
Fig 3 Left tension pneumothorax pushing mediastinum tothe right (lung edge arrowed)
Fig 4 Left lower lobe collapse (arrow) with shift of the mediastinum to the left
STUDENTBMJ VOLUME 8 OCTOBER 2000 studentbmj.com360
Education
There are only a few occasions whenthere may be the appearance of left ven-tricular failure (LVF) but a normal sizedheart—in an acute myocardial infarct (sud-den onset of LVF), or lymphangitis carci-nomatosa may mimic the appearances ofLVF and be accompanied by a normalsized heart.
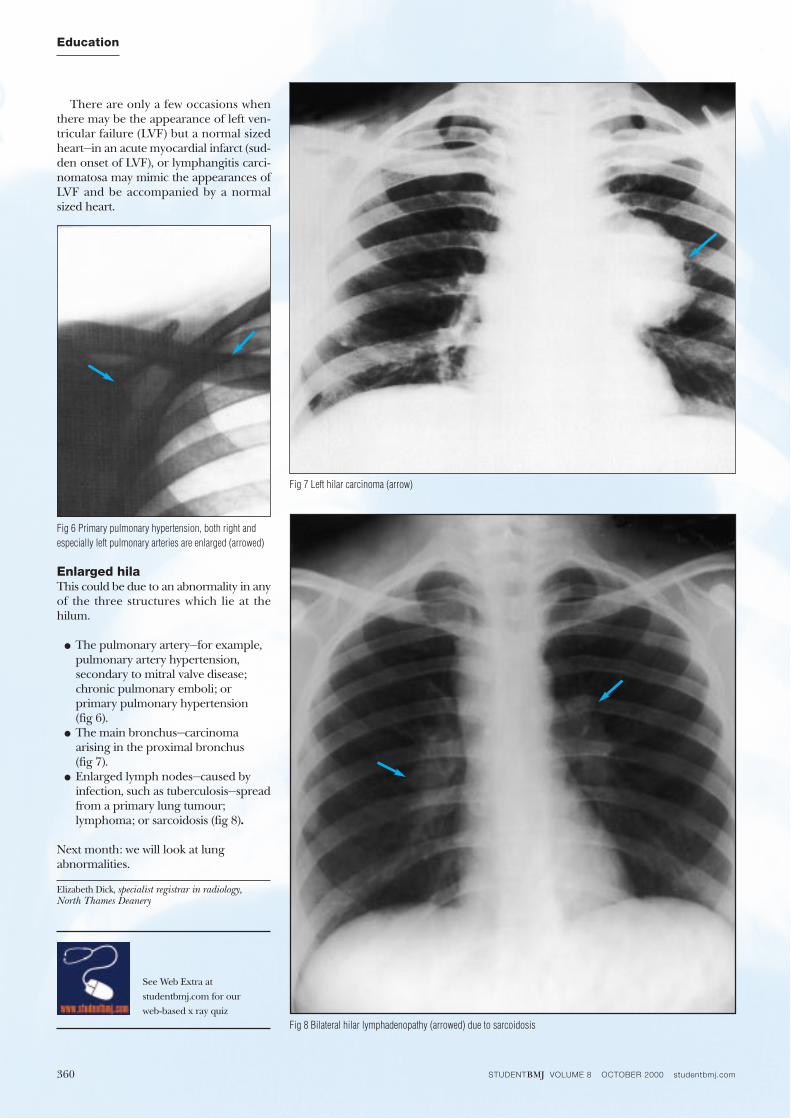
Enlarged hilaThis could be due to an abnormality in anyof the three structures which lie at thehilum.
● The pulmonary artery—for example,pulmonary artery hypertension,secondary to mitral valve disease;chronic pulmonary emboli; orprimary pulmonary hypertension (fig 6).
● The main bronchus—carcinomaarising in the proximal bronchus (fig 7).
● Enlarged lymph nodes—caused byinfection, such as tuberculosis—spreadfrom a primary lung tumour;lymphoma; or sarcoidosis (fig 8).
Next month: we will look at lung abnormalities.
Elizabeth Dick, specialist registrar in radiology, North Thames Deanery
Fig 8 Bilateral hilar lymphadenopathy (arrowed) due to sarcoidosis
Fig 6 Primary pulmonary hypertension, both right andespecially left pulmonary arteries are enlarged (arrowed)
Fig 7 Left hilar carcinoma (arrow)
See Web Extra at
studentbmj.com for our
web-based x ray quiz
STUDENTBMJ VOLUME 8 NOVEMBER 2000 studentbmj.com408
Education
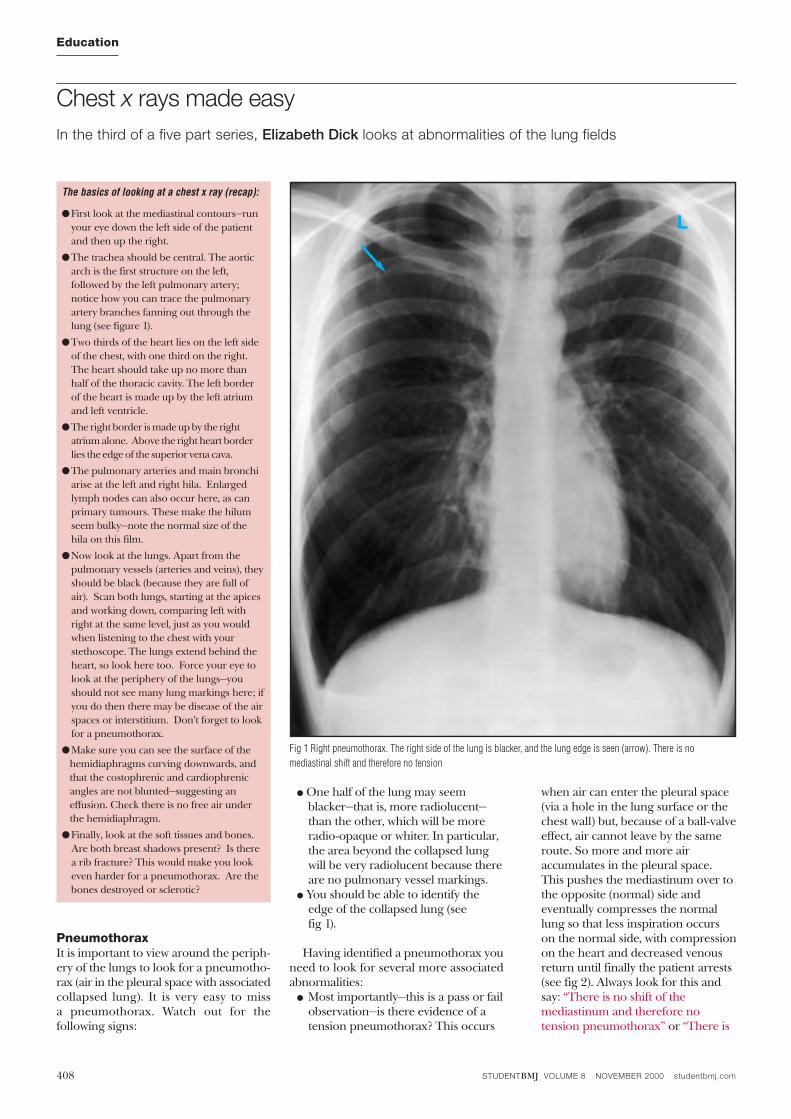
PneumothoraxIt is important to view around the periph-ery of the lungs to look for a pneumotho-rax (air in the pleural space with associatedcollapsed lung). It is very easy to miss a pneumothorax. Watch out for the following signs:
● One half of the lung may seemblacker—that is, more radiolucent—than the other, which will be moreradio-opaque or whiter. In particular,the area beyond the collapsed lungwill be very radiolucent because thereare no pulmonary vessel markings.
● You should be able to identify theedge of the collapsed lung (see fig 1).
Having identified a pneumothorax youneed to look for several more associatedabnormalities:● Most importantly—this is a pass or fail
observation—is there evidence of atension pneumothorax? This occurs
when air can enter the pleural space(via a hole in the lung surface or thechest wall) but, because of a ball-valveeffect, air cannot leave by the sameroute. So more and more airaccumulates in the pleural space.This pushes the mediastinum over tothe opposite (normal) side andeventually compresses the normallung so that less inspiration occurson the normal side, with compressionon the heart and decreased venousreturn until finally the patient arrests(see fig 2). Always look for this andsay: “There is no shift of themediastinum and therefore notension pneumothorax” or “There is
Chest x rays made easy In the third of a five part series, Elizabeth Dick looks at abnormalities of the lung fields
The basics of looking at a chest x ray (recap):
●First look at the mediastinal contours—runyour eye down the left side of the patientand then up the right.
●The trachea should be central. The aorticarch is the first structure on the left,followed by the left pulmonary artery;notice how you can trace the pulmonaryartery branches fanning out through thelung (see figure 1).
●Two thirds of the heart lies on the left sideof the chest, with one third on the right.The heart should take up no more thanhalf of the thoracic cavity. The left borderof the heart is made up by the left atriumand left ventricle.
●The right border is made up by the rightatrium alone. Above the right heart borderlies the edge of the superior vena cava.
●The pulmonary arteries and main bronchiarise at the left and right hila. Enlargedlymph nodes can also occur here, as canprimary tumours. These make the hilumseem bulky—note the normal size of thehila on this film.
●Now look at the lungs. Apart from thepulmonary vessels (arteries and veins), theyshould be black (because they are full ofair). Scan both lungs, starting at the apicesand working down, comparing left withright at the same level, just as you wouldwhen listening to the chest with yourstethoscope. The lungs extend behind theheart, so look here too. Force your eye tolook at the periphery of the lungs—youshould not see many lung markings here; ifyou do then there may be disease of the airspaces or interstitium. Don’t forget to lookfor a pneumothorax.
●Make sure you can see the surface of thehemidiaphragms curving downwards, andthat the costophrenic and cardiophrenicangles are not blunted—suggesting aneffusion. Check there is no free air underthe hemidiaphragm.
●Finally, look at the soft tissues and bones.Are both breast shadows present? Is therea rib fracture? This would make you lookeven harder for a pneumothorax. Are thebones destroyed or sclerotic?
Fig 1 Right pneumothorax. The right side of the lung is blacker, and the lung edge is seen (arrow). There is nomediastinal shift and therefore no tension
L
STUDENTBMJ VOLUME 8 NOVEMBER 2000 studentbmj.com 409
Education
shift of the mediastinum away fromthe side of the pneumothoraxindicating a (right/left) tensionpneumothorax. This is a medicalemergency which I would treatimmediately by inserting a large borecannula into the (right/left) pleuralspace.”
● The cause of the pneumothorax maybe apparent—for example, fracture ofthe ribs.
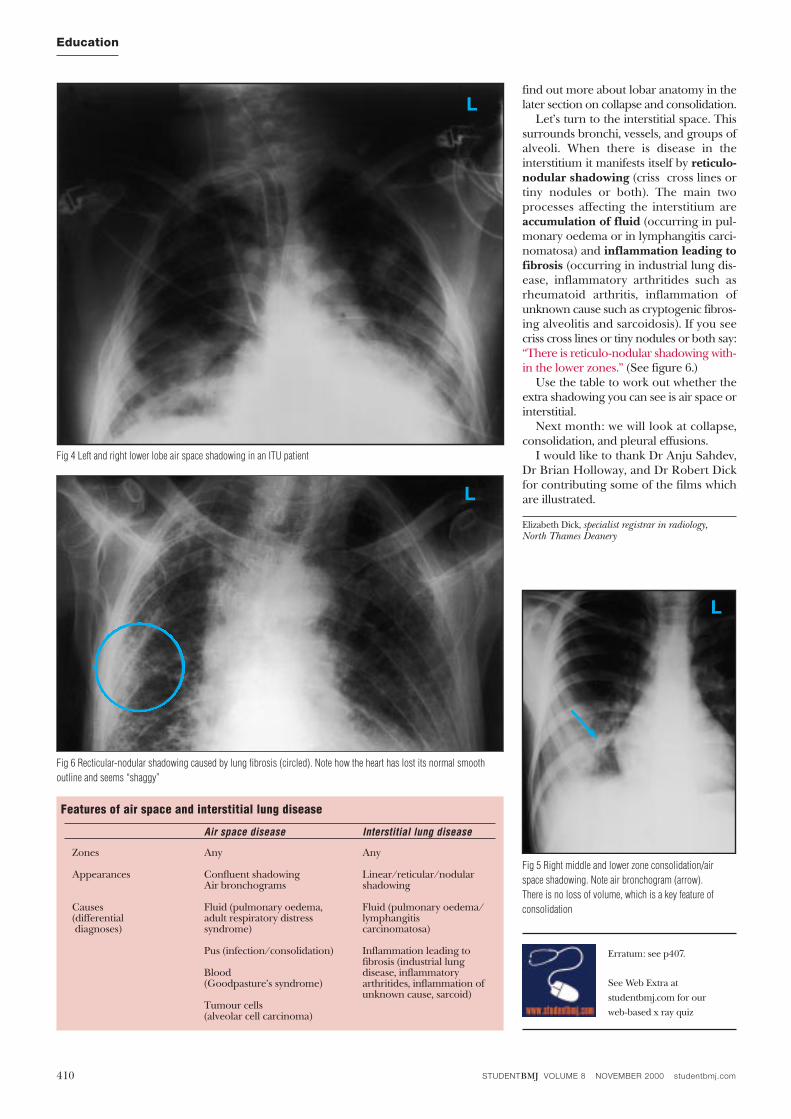
● There may be associated surgicalemphysema—that is, air in the softtissues—and air in the mediastinum(see fig 3).
There is extra shadowing in the lungsIt may be difficult to work out what is caus-ing extra shadowing in the lungs, especial-ly near the mediastinum where normalstructures may overlay the extra shadow-ing. It is useful to look at the periphery ofthe lungs because normally the outermostedge of the lungs should be fairly blackwith a few tapering blood vessels. If you dosee more shadowing in the periphery thenthere may be either interstitial or air spacedisease. As examiners often show filmswith one of these two types of shadowing,understanding the difference betweenthese two is worth while because it will helpyou to interpret what you see and lead youto the correct differential diagnosis.
The lung is made up of bronchi, whichbranch, at the end of which are alveoli. Theinterstitial space (or potential space) sur-rounds the alveoli. The whole of the lung
from bronchi to alveoli is the air space—that is, it normally contains air. But the air spaces can fill up—with fluid (such as insevere pulmonary oedema), with pus (asin infection), with blood (as in rare diseasessuch as Goodpasture’s syndrome, associ-ated with renal failure), or with tumourcells (alveolar carcinoma).
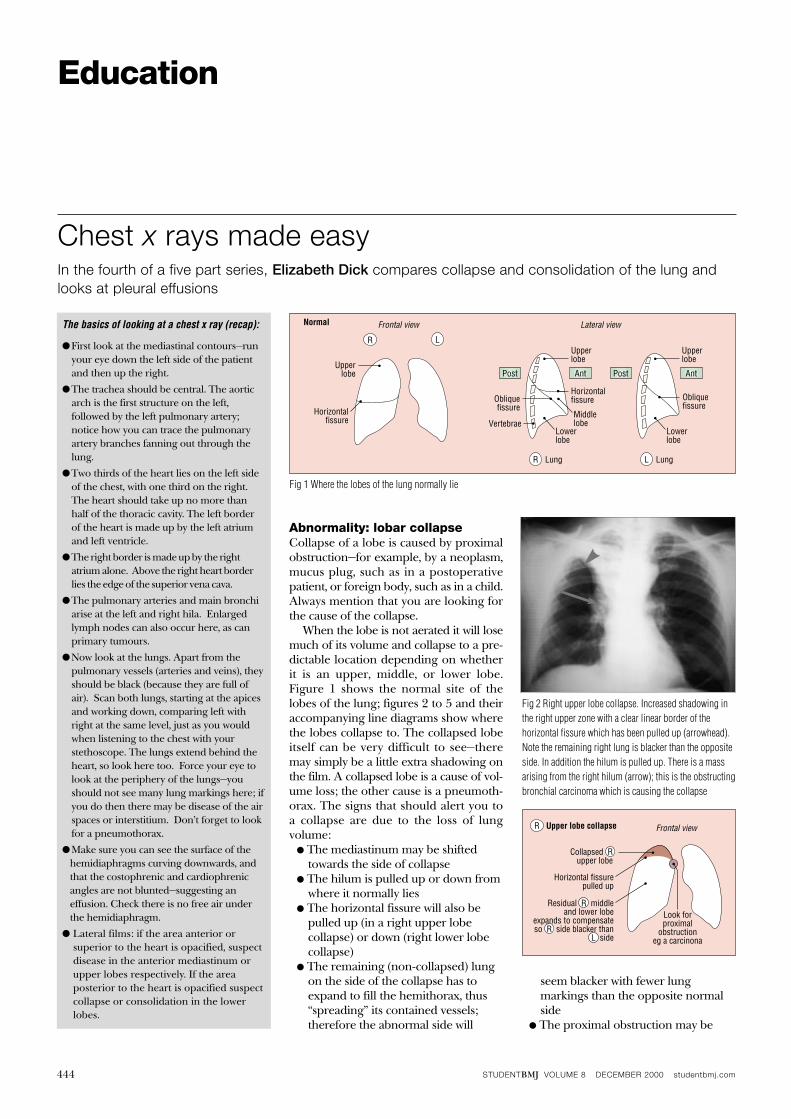
Fluid and pus are more common thanthe second two. When the air spaces fill up,the alveoli fill first, with the bronchi beingrelatively spared. Therefore the bronchi,which are still air filled, stand out againstthe alveoli, which are filled with pus orfluid. This is called an air bronchogramand is simply a sign that there is air spacedisease. Consolidation is another term forair space shadowing (see figs 4 and 5). Ifthere is air space disease then you need towork out which part of the lungs it is affect-ing. A quick way is to use the word “zone”to describe which part of the lung is affect-ed. Say something like “There is shadow-ing in the air spaces of the right mid andlower zone.” You can then take your timeto work out which lobe is affected. You can
Fig 2 Left tension pneumothorax with shift of the mediastinum to the right. The lung edge is arrowed
Fig 3 Surgical emphysema (arrow) and pneumomediastinum (arrowhead)
L
L
STUDENTBMJ VOLUME 8 NOVEMBER 2000 studentbmj.com410
Education
find out more about lobar anatomy in thelater section on collapse and consolidation.
Let’s turn to the interstitial space. Thissurrounds bronchi, vessels, and groups ofalveoli. When there is disease in the interstitium it manifests itself by reticulo-nodular shadowing (criss cross lines ortiny nodules or both). The main twoprocesses affecting the interstitium areaccumulation of fluid (occurring in pul-monary oedema or in lymphangitis carci-nomatosa) and inflammation leading tofibrosis (occurring in industrial lung dis-ease, inflammatory arthritides such asrheumatoid arthritis, inflammation ofunknown cause such as cryptogenic fibros-ing alveolitis and sarcoidosis). If you seecriss cross lines or tiny nodules or both say:“There is reticulo-nodular shadowing with-in the lower zones.” (See figure 6.)
Use the table to work out whether theextra shadowing you can see is air space orinterstitial.
Next month: we will look at collapse,consolidation, and pleural effusions.
I would like to thank Dr Anju Sahdev,Dr Brian Holloway, and Dr Robert Dickfor contributing some of the films whichare illustrated.
Elizabeth Dick, specialist registrar in radiology, North Thames Deanery
Fig 5 Right middle and lower zone consolidation/airspace shadowing. Note air bronchogram (arrow). There is no loss of volume, which is a key feature ofconsolidation
Fig 6 Recticular-nodular shadowing caused by lung fibrosis (circled). Note how the heart has lost its normal smoothoutline and seems “shaggy”
See Web Extra at
studentbmj.com for our
web-based x ray quiz
Erratum: see p407.
L
L
Fig 4 Left and right lower lobe air space shadowing in an ITU patient
L
Features of air space and interstitial lung disease
Air space disease Interstitial lung disease
Zones Any Any
Appearances Confluent shadowing Linear/reticular/nodular Air bronchograms shadowing
Causes Fluid (pulmonary oedema, Fluid (pulmonary oedema/(differential adult respiratory distress lymphangitisdiagnoses) syndrome) carcinomatosa)
Pus (infection/consolidation) Inflammation leading tofibrosis (industrial lung
Blood disease, inflammatory(Goodpasture’s syndrome) arthritides, inflammation of
unknown cause, sarcoid)Tumour cells(alveolar cell carcinoma)
STUDENTBMJ VOLUME 8 DECEMBER 2000 studentbmj.com444
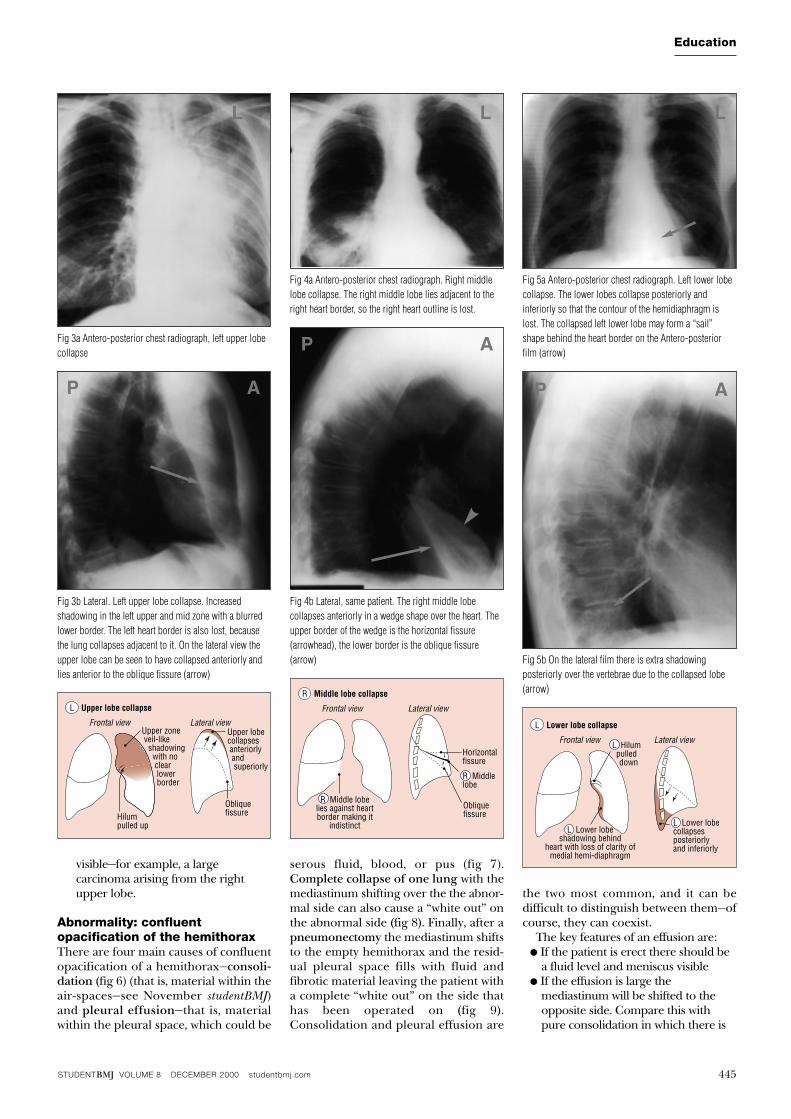
Abnormality: lobar collapseCollapse of a lobe is caused by proximalobstruction—for example, by a neoplasm,mucus plug, such as in a postoperativepatient, or foreign body, such as in a child.Always mention that you are looking forthe cause of the collapse.
When the lobe is not aerated it will losemuch of its volume and collapse to a pre-dictable location depending on whetherit is an upper, middle, or lower lobe.Figure 1 shows the normal site of thelobes of the lung; figures 2 to 5 and theiraccompanying line diagrams show wherethe lobes collapse to. The collapsed lobeitself can be very difficult to see—theremay simply be a little extra shadowing onthe film. A collapsed lobe is a cause of vol-ume loss; the other cause is a pneumoth-orax. The signs that should alert you toa collapse are due to the loss of lungvolume:
● The mediastinum may be shiftedtowards the side of collapse
● The hilum is pulled up or down fromwhere it normally lies
● The horizontal fissure will also bepulled up (in a right upper lobecollapse) or down (right lower lobecollapse)
● The remaining (non-collapsed) lungon the side of the collapse has toexpand to fill the hemithorax, thus“spreading” its contained vessels;therefore the abnormal side will
seem blacker with fewer lungmarkings than the opposite normalside
● The proximal obstruction may be
Chest x rays made easy In the fourth of a five part series, Elizabeth Dick compares collapse and consolidation of the lung andlooks at pleural effusions
Education
The basics of looking at a chest x ray (recap):
● First look at the mediastinal contours—runyour eye down the left side of the patientand then up the right.
● The trachea should be central. The aorticarch is the first structure on the left,followed by the left pulmonary artery;notice how you can trace the pulmonaryartery branches fanning out through thelung.
● Two thirds of the heart lies on the left sideof the chest, with one third on the right.The heart should take up no more thanhalf of the thoracic cavity. The left borderof the heart is made up by the left atriumand left ventricle.
● The right border is made up by the rightatrium alone. Above the right heart borderlies the edge of the superior vena cava.
● The pulmonary arteries and main bronchiarise at the left and right hila. Enlargedlymph nodes can also occur here, as canprimary tumours.
● Now look at the lungs. Apart from thepulmonary vessels (arteries and veins), theyshould be black (because they are full ofair). Scan both lungs, starting at the apicesand working down, comparing left withright at the same level, just as you wouldwhen listening to the chest with yourstethoscope. The lungs extend behind theheart, so look here too. Force your eye tolook at the periphery of the lungs—youshould not see many lung markings here; ifyou do then there may be disease of the airspaces or interstitium. Don’t forget to lookfor a pneumothorax.
● Make sure you can see the surface of thehemidiaphragms curving downwards, andthat the costophrenic and cardiophrenicangles are not blunted—suggesting aneffusion. Check there is no free air underthe hemidiaphragm.
● Lateral films: if the area anterior orsuperior to the heart is opacified, suspectdisease in the anterior mediastinum orupper lobes respectively. If the areaposterior to the heart is opacified suspectcollapse or consolidation in the lowerlobes.
Frontal view Lateral viewNormal
Upperlobe
Upperlobe
Horizontalfissure
R L
R Lung L Lung
Post Ant Post Ant
Upperlobe
Lowerlobe
Lowerlobe
Horizontalfissure Oblique
fissureObliquefissure
MiddlelobeVertebrae
Fig 1 Where the lobes of the lung normally lie
Frontal viewUpper lobe collapse
Collapsed Rupper lobe
Horizontal fissurepulled up
Look forproximal
obstructioneg a carcinona
R
Residual R middleand lower lobe
expands to compensateso R side blacker than
L side
Fig 2 Right upper lobe collapse. Increased shadowing inthe right upper zone with a clear linear border of thehorizontal fissure which has been pulled up (arrowhead).Note the remaining right lung is blacker than the oppositeside. In addition the hilum is pulled up. There is a massarising from the right hilum (arrow); this is the obstructingbronchial carcinoma which is causing the collapse
STUDENTBMJ VOLUME 8 DECEMBER 2000 studentbmj.com 445
Education
visible—for example, a largecarcinoma arising from the rightupper lobe.
Abnormality: confluentopacification of the hemithoraxThere are four main causes of confluentopacification of a hemithorax—consoli-dation (fig 6) (that is, material within theair-spaces—see November studentBMJ)and pleural effusion—that is, materialwithin the pleural space, which could be
serous fluid, blood, or pus (fig 7).Complete collapse of one lung with themediastinum shifting over the the abnor-mal side can also cause a “white out” onthe abnormal side (fig 8). Finally, after apneumonectomy the mediastinum shiftsto the empty hemithorax and the resid-ual pleural space fills with fluid andfibrotic material leaving the patient witha complete “white out” on the side thathas been operated on (fig 9).Consolidation and pleural effusion are
the two most common, and it can be difficult to distinguish between them—ofcourse, they can coexist.
The key features of an effusion are:● If the patient is erect there should be
a fluid level and meniscus visible● If the effusion is large the
mediastinum will be shifted to theopposite side. Compare this withpure consolidation in which there is
Fig 3a Antero-posterior chest radiograph, left upper lobecollapse
Fig 3b Lateral. Left upper lobe collapse. Increasedshadowing in the left upper and mid zone with a blurredlower border. The left heart border is also lost, becausethe lung collapses adjacent to it. On the lateral view theupper lobe can be seen to have collapsed anteriorly andlies anterior to the oblique fissure (arrow)
Fig 4a Antero-posterior chest radiograph. Right middlelobe collapse. The right middle lobe lies adjacent to theright heart border, so the right heart outline is lost.
Fig 4b Lateral, same patient. The right middle lobecollapses anteriorly in a wedge shape over the heart. Theupper border of the wedge is the horizontal fissure(arrowhead), the lower border is the oblique fissure(arrow)
Fig 5a Antero-posterior chest radiograph. Left lower lobecollapse. The lower lobes collapse posteriorly andinferiorly so that the contour of the hemidiaphragm islost. The collapsed left lower lobe may form a “sail”shape behind the heart border on the Antero-posteriorfilm (arrow)
Fig 5b On the lateral film there is extra shadowingposteriorly over the vertebrae due to the collapsed lobe(arrow)Middle lobe collapseR
Frontal view Lateral view
R Middle lobelies against heartborder making it
indistinct
Horizontalfissure
Obliquefissure
R Middlelobe
Lower lobe collapseL
Frontal view Lateral view
L Lower lobeshadowing behind
heart with loss of clarity ofmedial hemi-diaphragm
L Hilumpulled down
L Lower lobecollapsesposteriorlyand inferiorly
Upper lobe collapseL
Frontal view Lateral viewUpper lobecollapses anteriorly and superiorly
Upper zone veil-like shadowing with no clear lower border
ObliquefissureHilum
pulled up
L L L
P
P
A
A
AP
STUDENTBMJ VOLUME 8 DECEMBER 2000 studentbmj.com446
Education
no change in volume of thehemithorax and therefore nomediastinal shift. There is one caveatto bear in mind, which is that if
collapse of the lung is accompaniedby a pleural effusion the loss ofvolume (caused by the collapse) maybe balanced out by the increase involume of the hemithorax (caused bythe effusion) and therefore it mayseem as if the volume of thehemithorax overall is equivalent tothe opposite side.
As we discussed in November the keyfeature of consolidation is an air bron-chogram. In infective causes of consolida-tion the process may affect a lobe (lobarpneumonia in a distribution according thenormal anatomy shown in fig 1) or spreadin a more patchy distribution (broncho-pneumonia). Now test yourself with ourweb quiz at studentbmj.com.
Next month: we will look at lung nod-ules and masses.
I would like to thank Dr Anju Sahdev,Dr Brian Holloway, and Dr Robert Dickfor contributing some of the films whichare illustrated.
Elizabeth Dick, specialist registrar in radiology, NorthThames Deanery
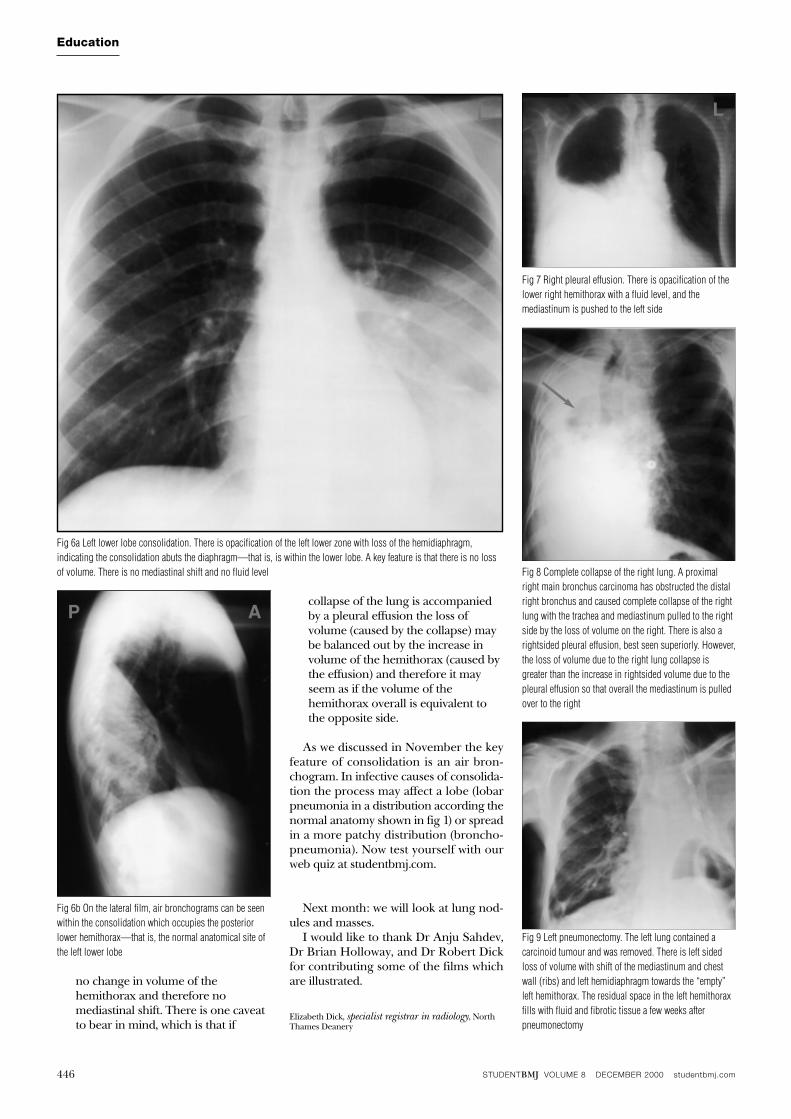
Fig 6a Left lower lobe consolidation. There is opacification of the left lower zone with loss of the hemidiaphragm,indicating the consolidation abuts the diaphragm—that is, is within the lower lobe. A key feature is that there is no lossof volume. There is no mediastinal shift and no fluid level
Fig 6b On the lateral film, air bronchograms can be seenwithin the consolidation which occupies the posteriorlower hemithorax—that is, the normal anatomical site ofthe left lower lobe
Fig 7 Right pleural effusion. There is opacification of thelower right hemithorax with a fluid level, and themediastinum is pushed to the left side
Fig 8 Complete collapse of the right lung. A proximalright main bronchus carcinoma has obstructed the distalright bronchus and caused complete collapse of the rightlung with the trachea and mediastinum pulled to the rightside by the loss of volume on the right. There is also arightsided pleural effusion, best seen superiorly. However,the loss of volume due to the right lung collapse isgreater than the increase in rightsided volume due to thepleural effusion so that overall the mediastinum is pulledover to the right
Fig 9 Left pneumonectomy. The left lung contained acarcinoid tumour and was removed. There is left sidedloss of volume with shift of the mediastinum and chestwall (ribs) and left hemidiaphragm towards the “empty”left hemithorax. The residual space in the left hemithoraxfills with fluid and fibrotic tissue a few weeks afterpneumonectomy
L L
L
P A
STUDENTBMJ VOLUME 9 FEBRUARY 2001 studentbmj.com10
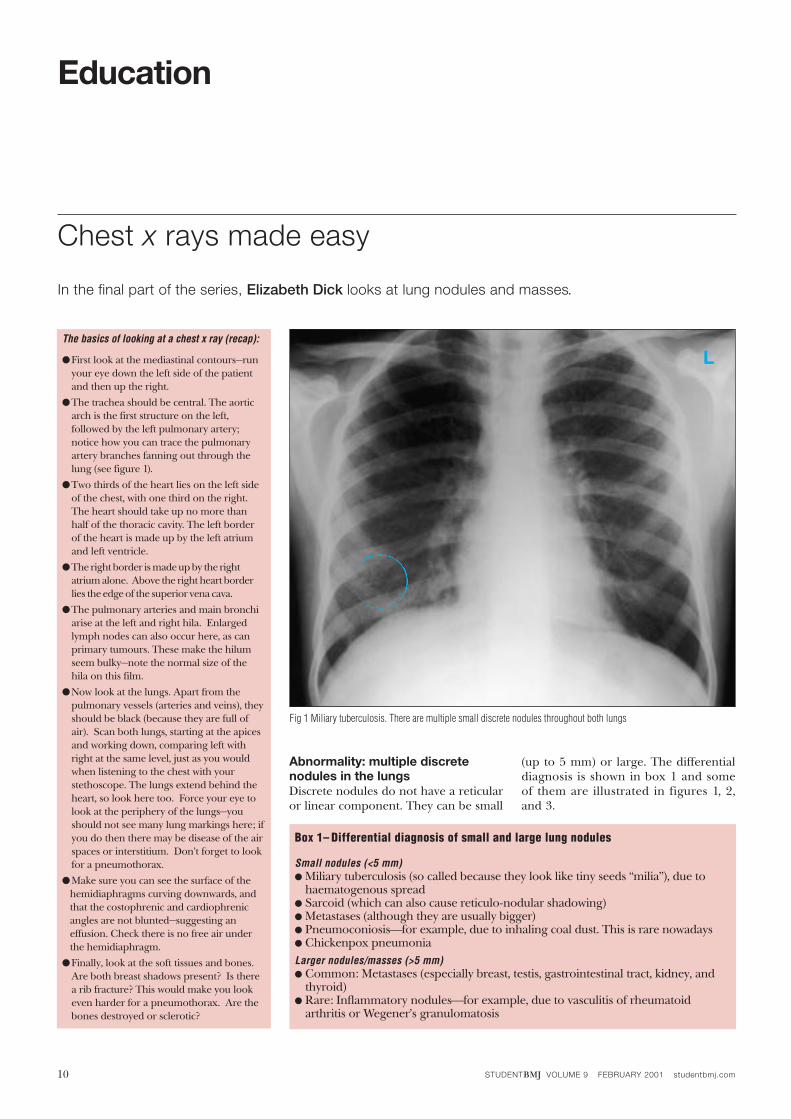
Abnormality: multiple discretenodules in the lungsDiscrete nodules do not have a reticularor linear component. They can be small
(up to 5 mm) or large. The differentialdiagnosis is shown in box 1 and someof them are illustrated in figures 1, 2,and 3.
Chest x rays made easy
In the final part of the series, Elizabeth Dick looks at lung nodules and masses.
Education
The basics of looking at a chest x ray (recap):
●First look at the mediastinal contours—runyour eye down the left side of the patientand then up the right.
●The trachea should be central. The aorticarch is the first structure on the left,followed by the left pulmonary artery;notice how you can trace the pulmonaryartery branches fanning out through thelung (see figure 1).
●Two thirds of the heart lies on the left sideof the chest, with one third on the right.The heart should take up no more thanhalf of the thoracic cavity. The left borderof the heart is made up by the left atriumand left ventricle.
●The right border is made up by the rightatrium alone. Above the right heart borderlies the edge of the superior vena cava.
●The pulmonary arteries and main bronchiarise at the left and right hila. Enlargedlymph nodes can also occur here, as canprimary tumours. These make the hilumseem bulky—note the normal size of thehila on this film.
●Now look at the lungs. Apart from thepulmonary vessels (arteries and veins), theyshould be black (because they are full ofair). Scan both lungs, starting at the apicesand working down, comparing left withright at the same level, just as you wouldwhen listening to the chest with yourstethoscope. The lungs extend behind theheart, so look here too. Force your eye tolook at the periphery of the lungs—youshould not see many lung markings here; ifyou do then there may be disease of the airspaces or interstitium. Don’t forget to lookfor a pneumothorax.
●Make sure you can see the surface of thehemidiaphragms curving downwards, andthat the costophrenic and cardiophrenicangles are not blunted—suggesting aneffusion. Check there is no free air underthe hemidiaphragm.
●Finally, look at the soft tissues and bones.Are both breast shadows present? Is therea rib fracture? This would make you lookeven harder for a pneumothorax. Are thebones destroyed or sclerotic?
Fig 1 Miliary tuberculosis. There are multiple small discrete nodules throughout both lungs
Box 1– Differential diagnosis of small and large lung nodules
Small nodules (<5 mm)● Miliary tuberculosis (so called because they look like tiny seeds “milia”), due to
haematogenous spread● Sarcoid (which can also cause reticulo-nodular shadowing)● Metastases (although they are usually bigger)● Pneumoconiosis⎯for example, due to inhaling coal dust. This is rare nowadays● Chickenpox pneumoniaLarger nodules/masses (>5 mm)● Common: Metastases (especially breast, testis, gastrointestinal tract, kidney, and
thyroid)● Rare: Inflammatory nodules⎯for example, due to vasculitis of rheumatoid
arthritis or Wegener’s granulomatosis
L
STUDENTBMJ VOLUME 9 FEBRUARY 2001 studentbmj.com 11
Education
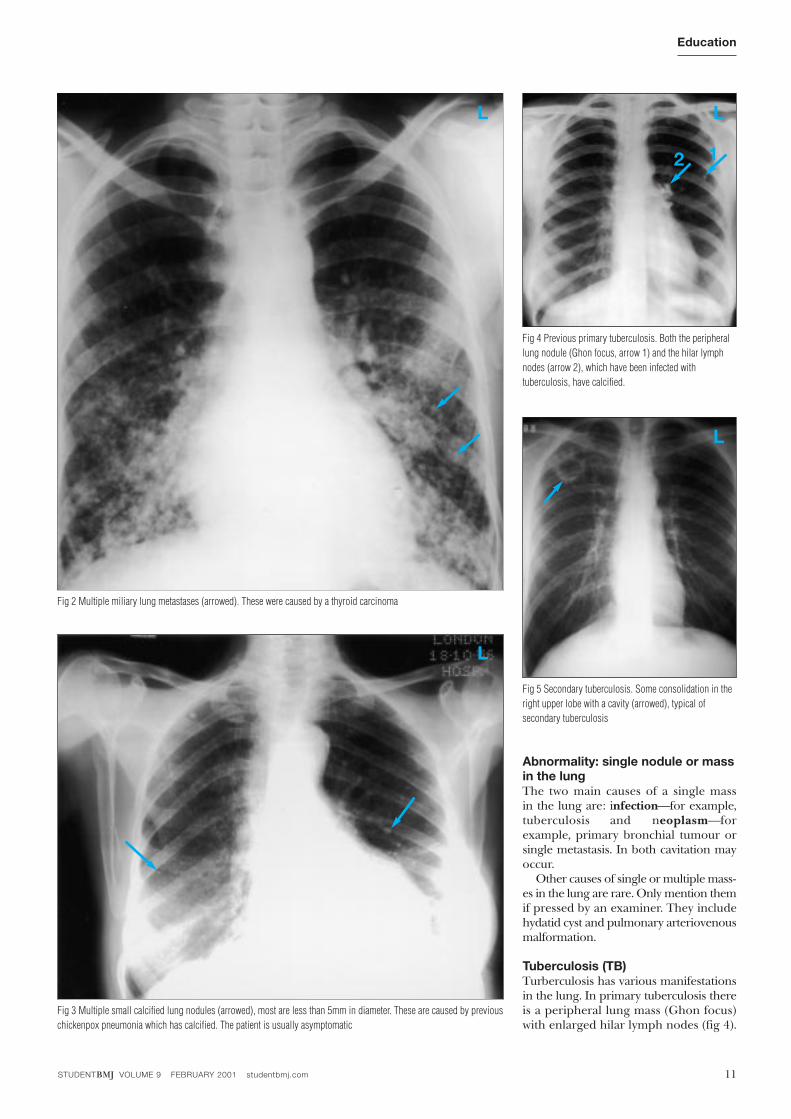
Abnormality: single nodule or massin the lungThe two main causes of a single massin the lung are: infection⎯for example,tuberculosis and neoplasm⎯forexample, primary bronchial tumour orsingle metastasis. In both cavitation mayoccur.
Other causes of single or multiple mass-es in the lung are rare. Only mention themif pressed by an examiner. They includehydatid cyst and pulmonary arteriovenousmalformation.
Tuberculosis (TB)Turberculosis has various manifestationsin the lung. In primary tuberculosis thereis a peripheral lung mass (Ghon focus)with enlarged hilar lymph nodes (fig 4).
Fig 4 Previous primary tuberculosis. Both the peripherallung nodule (Ghon focus, arrow 1) and the hilar lymphnodes (arrow 2), which have been infected withtuberculosis, have calcified.
Fig 5 Secondary tuberculosis. Some consolidation in theright upper lobe with a cavity (arrowed), typical ofsecondary tuberculosis
Fig 3 Multiple small calcified lung nodules (arrowed), most are less than 5mm in diameter. These are caused by previouschickenpox pneumonia which has calcified. The patient is usually asymptomatic
Fig 2 Multiple miliary lung metastases (arrowed). These were caused by a thyroid carcinoma
L L
12
L
L
STUDENTBMJ VOLUME 9 FEBRUARY 2001 studentbmj.com12
Education
Consolidation can also occur. In secondarytuberculosis there is patchy consolidationespecially in the upper lobes (fig 5). Thiscan cavitate. Other manifestations includepleural effusions and miliary tuberculosis.Mediastinal lymphadenopathy does notoccur in secondary TB.
Other infections can cavitate, includingpneumonias due to Staphylococcus, Klebsiel-la, and Cryptococcus. Pneumocystis carinii, asthe name suggests, can form cysts whichare airfilled and have a similar appearanceon an x ray film to cavities (fig 6).
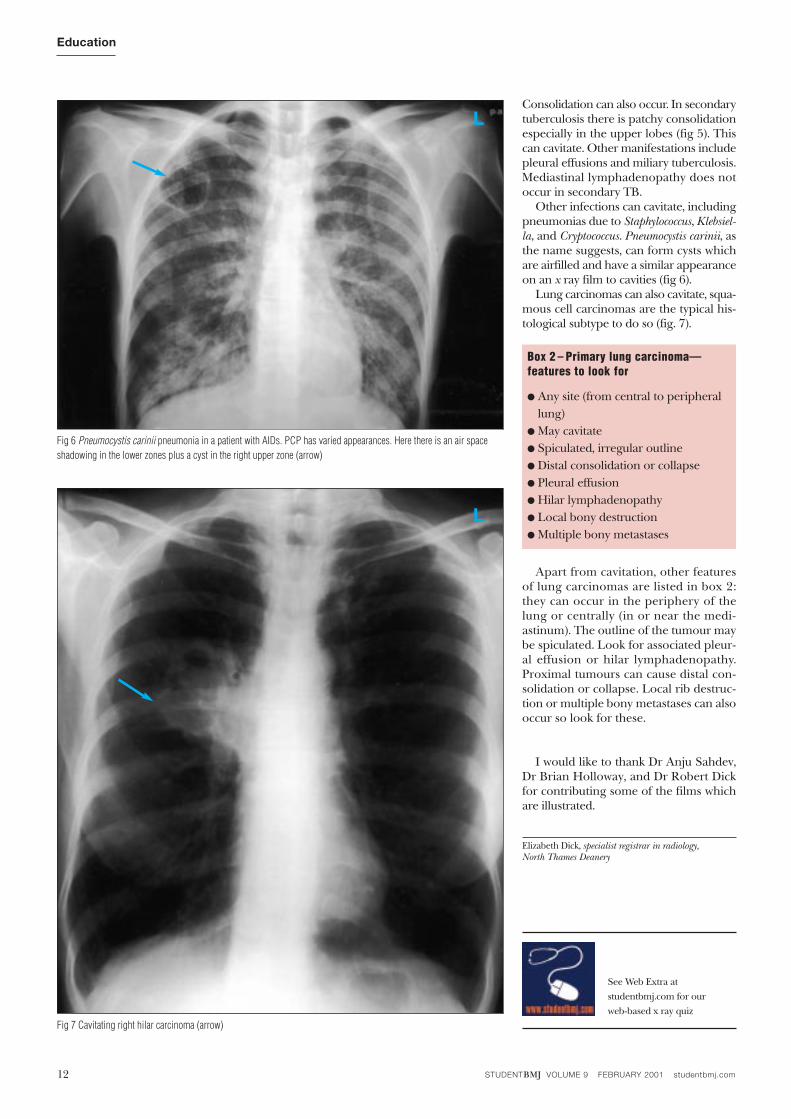
Lung carcinomas can also cavitate, squa-mous cell carcinomas are the typical his-tological subtype to do so (fig. 7).
Apart from cavitation, other featuresof lung carcinomas are listed in box 2:they can occur in the periphery of thelung or centrally (in or near the medi-astinum). The outline of the tumour maybe spiculated. Look for associated pleur-al effusion or hilar lymphadenopathy.Proximal tumours can cause distal con-solidation or collapse. Local rib destruc-tion or multiple bony metastases can alsooccur so look for these.
I would like to thank Dr Anju Sahdev,Dr Brian Holloway, and Dr Robert Dickfor contributing some of the films whichare illustrated.
Elizabeth Dick, specialist registrar in radiology, North Thames Deanery
Fig 6 Pneumocystis carinii pneumonia in a patient with AIDs. PCP has varied appearances. Here there is an air spaceshadowing in the lower zones plus a cyst in the right upper zone (arrow)
Fig 7 Cavitating right hilar carcinoma (arrow)
L
Box 2 – Primary lung carcinoma—features to look for
● Any site (from central to peripherallung)
● May cavitate● Spiculated, irregular outline● Distal consolidation or collapse● Pleural effusion● Hilar lymphadenopathy● Local bony destruction● Multiple bony metastases
L
See Web Extra at
studentbmj.com for our
web-based x ray quiz
Recommended
















