R. POLOSA - COI last 5 yrs
Lecture fees: Pfizer, GlaxoSmithKline, a number of european electronic cigarette industry and trade associations (including FIVAPE in France and FIESEL in Italy);
Research grants: Pfizer and GlaxoSmithKline;
Consultancy services: Pfizer, Global Health Alliance for treatment of tobacco dependence, ECITA, Health Diplomats;
Scientific advisor (pro bono): LIAF, IBVTA, CASAA
Chair: European Technical Committee for standardization on “Requirements and test methods for emissions of electronic cigarettes” (CEN/TC 437; WG4).

Impact of long term EC use on lung health
Prof. Riccardo Polosa
Institute of Internal Medicine
University of Catania
ITALY

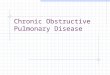
PRODUCT TOBACCO
PRESENT
AEROSOL
FORMATION
MECHANISM
NUMBER OF
COMPOUNDS
IN AEROSOL
NUMBER
OF
TOXICANTS
TOXICANT FORMATION
MECHANISMS
UNTARGETED
EMISSIONS
CIGARETTE Yes Combustion &
pyrolysis of
tobacco
>7000 100–150 Transfer from tobacco
Pyrosynthesis of tobacco
Pyrolysis
Combustion
E-CIG No Vaporisation
of e-liquid 10–100 <5 Poorly quality e-liquids
(eg. contaminants)
Thermal degradation of
PG/VG (‘Dry wicking’)
Transfer of extractables &
leachables from device
during storage or heating
GCxGC-TOF-MS chromatograms
of cigarette smoke vs EC aerosol
E-cigarettes: reduced toxicants emission

Reduced exposure to toxicants in EC users M.L. Goniewicz et al. Nicotine Tob Res 2017
≈ 60% reduction ≈ 80% reduction
≈ 75% reduction ≈ 70% reduction

• EC use common and increasing
• Concern about the long-term health effects of vaping (in
vitro systems, animal studies, surveys)
• Very little is known about the health impact of long-term
vaping
The problems

• What is the long-term health impact of vaping (in real-life
situation)?
• Can we answer the question by prospective studies of well-
characterized EC users?
The questions

• large prospective studies of well-characterized EC users
(impractical, costly)
• extrapolating responses to EC in cell lines and/or in animal
models (does not directly apply to real-life situation)
• surveys (issues with working definitions, design, etc.)
Substantiating evidence for the long-term health impact of EC - 1
Risk Reduction

• detecting early changes of subclinical injury with highly sensitive functional tests (“healthy” smokers)
• documenting changes with more robust and validated investigational tools (EC users with pre-existing disease)
• population modelling (smoking related morbidity and mortality)
Risk Reductio
Risk Reduction
Substantiating evidence for the long-term health impact of EC - 2

Impact of long term EC use on lung function in “healthy” smokers switching to ECs
Campagna D, Cibella F, Russo C, et al. Clin Sci. 2016

Campagna D, Cibella F, Russo C, et al. Clin Sci. 2016
Impact of long term EC use on lung function in “healthy” smokers switching to ECs

Quitters Reducers Failures
0
5
10
15
20
pp
b
BL W-12 W-24 W-52
FeNO Between subject effects: p<0.0001
Impact of long term EC use on FeNO in “healthy” smokers switching to ECs
CHANGES IN BREATHOMICS: 1-YR RANDOMIZED SMOKING CESSATION TRIAL OF ECs
D. Campagna, et al. Eur J Clin Invest 2016

• NCT02396381
• NCT02649556
• NCT02103751
• NCT03020667
• ….

• Smoking abstinence by using ECs may improve respiratory function and symptoms
• No data about EC use in smokers with pre-existing disease
• We investigated changes in subjective and objective asthma outcomes in smoking asthmatics who switched to EC

1st F/up Visit
Assessment Timepoints
Baseline Pre-Baseline
Fo
rce
d E
xp
ira
tory
Vo
lum
e in 1
se
co
nd
(L
)
3.0
3.2
3.4
3.6
3.8
2nd F/up Visit
**
Impact of EC use on lung function in asthma
FEV1 improvement from baseline to 24 months
p=0.005 mean increase of 100mls
Harm
Reversal!
Regular EC use
3rd F/up Visit
Polosa et al. Discov Med 2016

FE
F2
5-7
5 (
L/s
ec)
2.4
2.6
2.8
3.0
3.2
3.4
1st F/up Visit
Assessment Timepoints
Baseline Pre-Baseline
2nd F/up Visit
**
***p=0.006
mean increase of 250mls/sec
p=0.001 mean increase of 360mls/sec
Harm
Reversal!
Regular EC use
3rd F/up Visit
Polosa et al. Discov Med 2016
Impact of EC use on lung function in asthma FEF25-75 improvement from baseline to 24 months

Pre-Baseline
Me
tha
cho
line
PC
20
(m
g/m
L)
1.0
1.5
2.0
2.5
3.0
3.5
Baseline 2nd F/up Visit
1st F/up Visit
Assessment Timepoints
**
p=0.003 mean increase of 1.2 DD
Harm
Reversal!
Regular EC use
3rd F/up Visit
Polosa et al. Discov Med 2016
Impact of EC use on lung function in asthma PC20 improvement from baseline to 24 months

AC
Q s
co
res
1.2
1.4
1.6
1.8
2.0
2.2
2.4
1st F/up Visit
Assessment Timepoints
Baseline Pre-Baseline
2nd F/up Visit
***
***p=0.001
mean decrease of 0.43
p=0.001 mean decrease of 0.56
Harm
Reversal!
Regular EC use
3rd F/up Visit
Polosa et al. Discov Med 2016
Impact of EC use on lung QoL in asthma ACQ improvement from baseline to 24 months

• Smoking abstinence by using ECs may improve respiratory function and symptoms
• No data about EC use in smokers with COPD
• We investigated changes in subjective and objective respiratory outcomes in COPD smokers who switched to EC

Time
Baseline 12 Months 24 Months 36 Months
Post
-Bro
nch
odila
tor
FE
V1 (
L)
0.6
0.8
1.0
1.2
1.4
1.6
1.8
2.0
COPD EC Users
COPD Controls
p = 0.233
Polosa R et al. Respir Res 2017
No change in post B/Dil FVC No change in %FEV1/FVC
Impact of EC use on lung function in COPD No change from baseline to 36 months

Time
Baseline 12 Months 24 Months 36 Months
CO
PD
Exa
cerb
atio
ns/y
ear
0
1
2
3
4
COPD EC Users
COPD Controls
p = 0.004
Polosa R et al. Respir Res 2017
Less respiratory exacerbations
Impact of EC use on clinical outcomes in COPD Improvement from baseline to 36 months

Time
Baseline 12 Months 24 Months 36 Months
CO
PD
Ass
ess
ment
Tool (
CA
T)
Sco
res
10
15
20
25
30
COPD EC Users
COPD Controls
p=0.019
Polosa R et al. Respir Res 2017
Improved CAT score
Impact of EC use on QoL in COPD Improvement from baseline to 36 months

Time
Baseline 12 Months 24 Months 36 Months
6-M
inu
te W
alk
Dis
tan
ce (
me
tre
s)
200
300
400
COPD EC Users
COPD Controls
p = 0.001
Polosa R et al. Respir Res 2017
Improved 6MWD
Impact of EC use on physical performance in COPD Improvement from baseline to 36 months

• The large majority of EC users are smokers or ex-smokers
• Smoking hx and previous smoking hx are key confounders
• Changes in health outcomes take time (early sensitive
indicators – e.g. HRCT, FEF25-75)
The challenges

STUDY OBJECTIVE:
Detecting early changes of subclinical lung damage in a prospective study of well-
characterized EC users who have never smoked in their life

Results – Spirometry

Results – eCO and eNO

Results – Lung HRCT
Scans showed no pathological findings. In particular no CT
features compatible with early signs of :
• COPD (i.e. parenchymal micronodules, ground-glass
opacity, or macroscopic emphysema)
• Lipoid pneumonia
• Popcorn lung disease
Of note, no early pathological signs were observed in subjects with the highest e-liquid consumption (i.e. 5
mls/day) and longest overall vaping hx
(i.e. 57 months)

Impact of long term EC use on lung health Take Home Message
ECs are unlikely to raise significant health concerns for the respiratory tract under normal condition of use
Former smokers using and smokers intending to use ECs should receive correct information about residual risks and potential benefits
Promoting further access to ECs may reduce risk and reverse harm

Fabio Cibella National Research Council of Italy, Institute of Biomedicine and Molecular Immunology, Palermo, Italy Donald W. Cockroft Department of Medicine, Division of Respirology, Royal University of Saskatchewan, Canada Donald P. Tashkin David Geffen School of Medicine, UCLA, Los Angeles, California, USA Mario Malerba Department of Internal Medicine, University of Brescia and AOU Spedali Civili, Brescia, Italy Umberto Prosperini Ospedale “San Vincenzo” - ASP Messina, Taormina (ME), Italy. Cristina Russo Giovanni Ciampi MCAU ARNAS Garibaldi, Catania, Italy. Jaymin B. Morjaria Department of Respiratory Medicine, Royal Brompton & Harefield Hospital Foundation Trust, UK
Pasquale Caponnetto Marilena Maglia
Valeria Vinci Centro Prevenzione e Cura Tabagismo, University of Catania
Riccardo Polosa Cosimo M. Bruno Massimo Caruso Alfredo Fisichella Davide Campagna Maria Domenica Amaradio Dipartimento di Medicina Clinica e Sperimentale, University of Catania
Acknoweldgements
Recommended