4th-8th June, 2008, Shimla
vkjksX;e~ lq[klEinkvkjksX;e~ lq[klEink
Workshop for Senior and Mid-level Managers on Improving
Quality of Care in Health Sector
NIHFW
Organised by: Supported by:
Partner for the Future.Worldwide.
Jointly Organised by National Institute of Health and Family Welfare
and World Bank Institute with Technical Support of GTZ
National Institute of Health and Family WelfareBaba Gang Nath Marg, Munirka, New Delhi – 110067
Email: [email protected]: www.nihfw.org
Report

4th-8th June, 2008, Shimla
Workshop for Senior and Mid-levelManagers on Improving
Quality of Care in Health Sector
vkjksX;e~ lq[klEinkvkjksX;e~ lq[klEink
NIHFW
Organised by:
NAT
ION
AL
RURAL HEALTH MISSIO
N
jk"Vªh; xzkeh.k LokLF; fe'kujk"Vªh; xzkeh.k LokLF; fe'ku
Supported by:
Partner for the Future.Worldwide.
Jointly Organized by National Institute of Health and Family Welfare and World Bank Institute with Technical Support of GTZ
Report

3Quality of Care in Health Sector
Contents
S. No. Page
Abbreviations 4
Preface 5
Executive Summary 6
Background 7
Record of Proceedings 10
Overall Course Framework and Strategy 25
Next steps 29
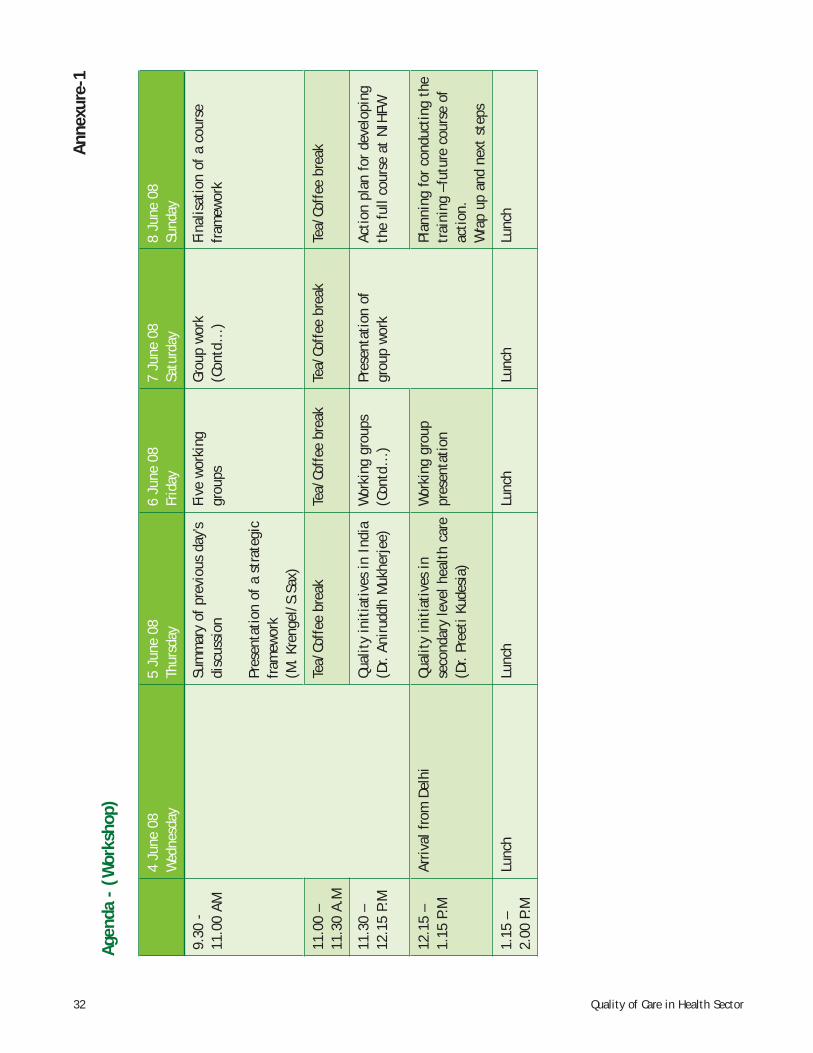
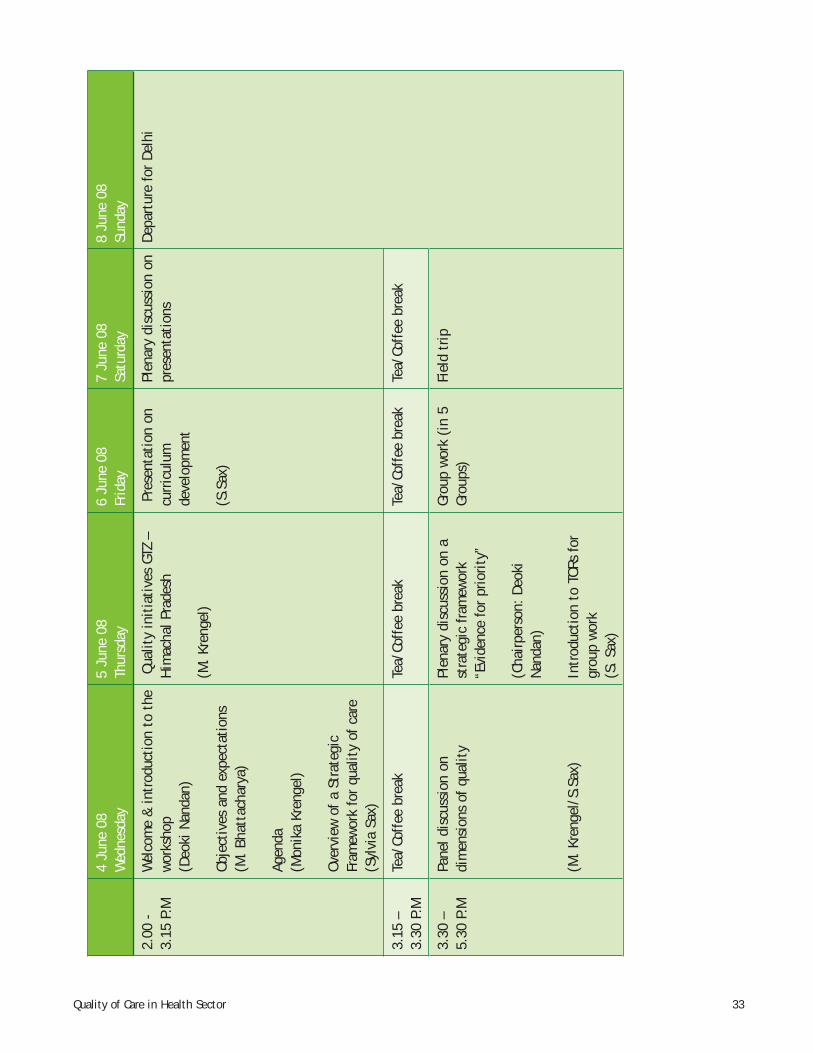
Annexure 1: Workshop Agenda 32
Annexure 2: Workshop Presentation by Ms. Sylvia Sax and Dr. Monika Krengel 34
Annexure 3: Workshop Presentation by Ms. Sylvia Sax 37
Annexure 4: Presentation by Dr. Aniruddh Mukerjee 41
Annexure 5: Presentation by Dr. Preeti Kudesia 49
Annexure 6: Presentation by Dr. Monika Krengel 52
Annexure 7: Presentation by Dr. Raghu, Block Medical Offi cer 58
Annexure 8: Workshop Terms of Reference and Results: Group work 1 65
Annexure 9: Workshop Terms of Reference and Results: Group Work 2 69
Annexure 10: An Introduction to NIHFW 74
Annexure 11: List of Participants 75
4 Quality of Care in Health Sector
AHA Academy of Hospital AdministrationCHC Community Health CentreCMOs Chief Medical Offi cersDQCG Directorate of Quality Core GroupEFQM European Foundation for Quality ManagementGOI Government of IndiaHAP British Hospital Accreditation ProgramHRD Human Resource DevelopmentIPHS Indian Public Health StandardsISO International Organisation for StandardisationJCI Joint Commission/USMOHFW Ministry of Health and Family Welfare
NABH National Accrededited Board of Hospitals and Healthcare providersNIHFW National Institute of Health and Family WelfareNRHM National Rural Health MissionOPD Out Patient DepartmentPDCA Plan Do Check ActPHREC Public Health Research and Education ConsortiumPLA Plan, Learn and ActQA Quality AssuranceQACs/Gs Quality Assurance Cells/GroupsQAP Quality Assurance ProgrammeQC Quality CirclesQCG Quality Core GroupsQCI Quality Council of IndiaQI Quality Initiatives
QM Quality ManagementQR Quality RepresentativeRCH Reproductive and Child HealthSIHFW State Institute of Health and Family WelfareSMOs State Medical Offi cersSOPs Standard Operating ProceduresSQCG State Quality Core GroupSTG Standard Treatment GuidelinesUNFPA United Nations Population FundWBI World Bank InstituteWHO World Health Organisation
Abbreviations
5Quality of Care in Health Sector
Quality of care in the health sector is a priority. Policy makers in our country have been struggling to probe and decide on the quality indicators which could be integrated in the existing and new initiatives for desirable outcomes. In this direction, a workshop on ‘Developing Training Curriculum for Improving Quality in Health Sector’ was conceptualised and conducted for senior and mid-level health managers at Shimla in June, 2008.
We, at the National Institute of Health and Family Welfare, thank the World Bank Institute for actively collaborating with us in this initiative and helping us in organising this workshop.
Special thanks are due to the team of Prof. Peter Berman, Ms. Alexandra Humme and Ms. Sheeja Nair for their constant support. GTZ took the initiative to invite international experts - Ms. Sylvia Sax and Dr. Monika Krengel to facilitate the workshop and lead the team of experts to develop the curriculum. Their efforts are laudable. Dr. J.P. Steinmann, Programme Advisor, GTZ, Dr. K.B. Singh, Mr. S. Malikarjuna, Mr. Amit Paliwal and Ms. Jhanavi Das from GTZ deserve special thanks for their support.
We owe our gratitude to Ms. Aradhana Johri, IAS, Joint Secretary, Ministry of Health and Family Welfare for her guidance and support to this activity. Dr. I.P. Kaur, Dr.Dinesh Boswal and Dr. S. Sikdar from MOHFW, GOI are sincerely thanked for their valuable advice. We are grateful to Dr. Dinesh Agarwal, UNFPA, Dr. Praveen Srivastava and Dr. S.K. Das, Government of India (GoI), for sharing the documents on Quality of Care.
Thanks are due to all the experts at the workshop, who took time out from their very busy schedules to attend and to enrich the deliberations with their vast knowledge and experiences to design a suitable curriculum.
The workshop could not have been organised at a short notice without the hard work put up by Dr. A.K. Bharadwaj from Shimla and his team.
Prof. Deoki NandanDirector, NIHFW
Preface
6 Quality of Care in Health Sector
The mission of development of a ‘Quality Management Course Curriculum’ towards improving quality of care in health sector in the form of a workshop from 4th-8th of June, 2008 was carried out at Shimla, India.
The mission was divided in two phases:1. Facilitation of a workshop on ‘Planning and Designing a Training Course for Improving Quality of Care in the
Health Sector.’2. Drafting of curriculum, identifi cation of further requirements and discussions on training contents and tools.
The objective of the curriculum development was: “To design the framework of a course for mid-level health offi cials on Improving Quality of Health Care so that they are able to conceive and frame policies and strategies to improve the quality parameters in the health care system at all levels.”
Expected Outcomes were: “A course framework for addressing quality issues by state level health offi cials, suggestions for course materials and case studies; an agreed way forward on how to implement the course.”
The decision to develop a nation-wide course refl ects: (i) a situation of extreme shortage of resource persons for providing training in quality management in health care, (ii) the need to integrate and exchange efforts and good practices from different states and institutions, and (iii) the need to build capacity amongst policy makers in quality management.
The course would contribute to the capacity building of policy makers and faculty members and other trainers and teachers involved in quality management.
By the end of the mission, a draft curriculum (Annexure 9), based on training gap analysis, prioritisation, etc. was developed, presented and discussed with all stakeholders, including faculty members of NIHFW, representatives of the World Bank and GTZ, HSS. The approach and outcomes, documented and presented by the international experts, were well received by the audience. Suggestions on how to continue with the formulation of the contents and materials to be used in the course are mentioned as curriculum essentials in the report. It is planned to fi nalise the further preparations by the end of October, 2008 and to conduct the fi rst workshop during the second half of November, 2008.
Executive Summary
7Quality of Care in Health Sector
Workshop for Senior and Mid-levelManagers on Improving Quality of Care in Health Sector4th-8th June, 2008 Shimla
Background
Increased investment by the government in social sectors like health and education over the last few years has generated widespread interest not only in the outcomes but also raised serious concerns about the quality and sustainability of these outcomes. In the past twenty years , the concept of improvement of health systems has moved away from top down control, compliance and punishment towards bottom up development , self–regulation and incentives; quality measurement has also shifted from resource inputs to performance outputs. It is widely acknowledged that in spite of the wealth of experience in quality the problem frequently faced by policy-makers at country level is to know which quality strategies complement or can be integrated with existent strategic initiatives to have the greatest impact on the outcomes delivered by their health systems despite available funds. The failure of quality initiatives lies in too much focus on standards and measurement rather than on changing the way people and organisations work. The report of the National commission on Macroeconomics and health attributes failures in the health system to poor governance and dysfunctional role of the state, lack of strategic vision and weak management.
It has been clearly established that any sustainable change in terms of institutionalisation of Quality Assurance (QA) will come from within the system and not from outside. The GTZ along with other donor partners is supporting the government of India and the states to develop a comprehensive framework and an achievable plan to improve the quality and safety of the health system.
A WHO review has broadly classifi ed the approaches to quality improvement into the following categories (also called the strategic framework):• Empowerment of consumers • Institutional development • Management development • Clinical practice development • Professional development
Currently in India the environment is very conducive for integrating strategies to improve quality in the health system. There is a strong political commitment for such action and increased funding to the sector. The Government of India under the National Rural Health Mission (NRHM) has re-emphasised the need to enhance quality of care in the health sector. The NHRM though focussing on rural health in general and RCH in particular, also seeks to defi ne standards (the Indian public health standards) at all provider levels which relate primarily to the availability of services, staff and equipment. However, the Ministry of Health and Family Welfare, Government of India is actively pursuing improvements in the quality of reproductive and child health (RCH)
8 Quality of Care in Health Sector
care provided through the vast network of public health institutions, RCH/sterilisation camps and outreach services. Assessing continuous improvement in the quality of RCH services is one of the thrust priorities of the NRHM/RCH II programme. In order to establish and institutionalise quality assurance and improvement in RCH services, an attempt is being made to set up a functioning ‘District Quality Assurance Cells’.
The Family Planning Division of GOI has formalised the Quality Assurance Cells( QAC) and by now all the states in the country are having a state and district quality assurance committee. Most of them have also updated these QACs as per the new pattern of memberships as per the guidelines of GOI. The challenge, therefore, is to operationalise these very QACs. An operational manual has also been developed by UNFPA.
A course curriculum should be developed keeping in view the membership profi le of these committees since the ambit of these committees have been enhanced by including the maternal health, child health and other RCH activities also.
Recently a need assessment study was carried out jointly by NIHFW and WBI in three states, namely UP, Rajasthan and Orissa. It has brought out the need for training health offi cials at state and district levels in improving the system and service delivery through capacity building, to initiate and implement the various reform processes initiated in the health sector especially the Quality Assurance in the system and service delivery.
To take forward these objectives, NIHFW in collaboration with WBI and with technical support of GTZ, organised a workshop to plan and design a training course for improving quality of care in health sector within a strategic framework so that quality does not remain the purview of few but of the whole workforce in the health sector. Hence the main purpose of the workshop was to design the framework for a course on Improving Quality of Health Care for senior and mid-level health offi cials including the members of the District Quality Assurance Group, so that they are able to conceive and frame policies and strategies to improve the quality parameters in the health care system at all levels.
The consensus building approach adopted, was a stakeholders workshop with a mix of experts national and international in quality assurance for hospital and health sector as a whole.
The participants were represented by the following categories (Annexure-11):1. Offi cials from the Ministry of Health and Family Welfare2. Offi cials from the Health Departments of State Governments and Training Institutions 3. Faculty from NIHFW4. Experts from Heidelberg University5. Representatives from Development Partners6. Representatives from Private sector, Hospitals, Associations, Medical Colleges, Academic Institutions, etc.
1. The World Bank has established a website and databank for the collection of training material, case studies, literature, as a supportive instrument for the development and execution of courses. They will continue this activity and it is planned to later hand this over to the NIHFW.
2. See “Quality Assurance for District Reproductive and Child Health Services in Public Health System”. An Operational Manual, Ministry of Health and Family Welfare, Government of India, New Delhi, April 2008; Quality Assurance Manual for Sterilisation Services, Research Studies & Standards Division Ministry of Health and Family Welfare, Government of India, October 2006.
9Quality of Care in Health Sector
The methodology used in the workshop was plenary discussion to outline the existing situation and share the results of the pilot projects conducted by GTZ, World Bank and UNFPA. After assessing the various options available, the members were divided into groups to brainstorm, do gap analysis and prioritisation on the fi ve areas of “Strategic Frame Work” according to given TORs and come out with suggestions which were then presented in a plenary session. This process was carried on till an agreed upon consensus was reached about the contents to be included in the course. The course would contribute to the capacity building of policy makers, faculty members and other trainers and teachers involved in quality management courses.
The international experts Ms. Sylvia Sax, University of Heidelberg, Germany, and Dr. Monika Krengel, EPOS Health Consultants, Germany, facilitated the whole workshop with the support of faculty members of NIHFW, especially Prof. Madhulekha Bhattacharya, Dean of Studies and the coordinator of the course. The mission was guided by Prof. Deoki Nadan, Director, NIHFW and supported by the inputs from the World Bank Institute team, Ms. Alexandra Humme, Dr. Preeti Kudesia and Ms. Sheeja Nair. Mr. Amit Paliwal and Mr. S. Mallikarjuna, from GTZ HSS, also accompanied the mission.
The objective of the curriculum development was: “To design the framework for a course for Top and Mid Level Health Offi cials on Improving Quality of Health Care so that they are able to conceive and frame policies and strategies to improve the quality parameters in the health care system at all levels.”
The outcomes were:• Course framework for addressing quality issues by state and district level health offi cials • Suggestions for course materials and case studies• An agreed way forward on conduction of the course.
Following the workshop, the team of international experts, Ms. S. Sax and Dr. M. Krengel worked with the faculty at NIHFW, to further work out the details and fi nalised the course curriculum. The agenda (Annexure-1) of the workshop was followed and the salient features of the day wise deliberations are given in the report.
10 Quality of Care in Health Sector
Record of proceedings
4th June 2008
Inaugural session of the workshop was chaired by a panel comprising of Prof. Deoki Nandan, Director, National Institute of Health and Family Welfare, Ms. Alexandra Humme, from the World Bank Institute, Ms. Sylvia Sax, expert from GTZ and Dr. Madhulekha Bhattacharya, Dean of studies and Head, Community Health Administration, National Institute of Health and Family Welfare and coordinator for the workshop. The session began with Prof. Deoki Nandan extending a warm welcome to all the participants, mainly comprising of the offi cials from the WBI, GTZ, Ministry of Health and Family Welfare, Government of India and states, experts from relevant fi elds and the faculty from the NIHFW (list annexed). This was followed by a self introduction by the participants.
In his opening address, Prof. Deoki Nandan gave a brief introduction of NIHFW on being an apex training Institute in the fi eld of health and Family Welfare and specially highlighted the collaborative activities with the development partners and the PHERC (Public Health Education and Research Consortium) initiative. Emphasizing on the need for a course on quality assurance in healthcare, he hoped that the workshop would provide the desired platform for designing the same. Ms. Alexandra Humme dwelled on the fruitful partnership with the NIHFW and explained the importance of quality management in healthcare. Elaborating on its fl agship programme on Quality, she emphasised on the need for public private partnership in health combined with high levels of accountability. Ms. Sylvia Sax gave a brief insight into the Quality course being conducted by the Heidelberg University. This was followed by a vote of thanks by Prof. M. Bhattacharya. • Plenary Session: began with Prof. Bhattacharya explaining the objective and the expected outcomes of the
workshop.• Ms. Sylvia Sax and Dr. Monika Krengel presented the strategy/approach for Quality Assurance (Annexure-2)
to be adopted during the workshop as given below:• Empowerment of consumer• Institutional development • Management development • Clinical practice development • Professional development
Ms. Sylvia Sax in her presentation on ‘Improving Quality of Care in India (annexure-3) explained the defi nition and dimensions of quality. She presented a simple model for quality including the (PCDA) quality cycle. And how it should be applied to the system pyramid which depicted involvement of functionaries at all levels responsible for achieving quality.
11Quality of Care in Health Sector
A panel discussion on ‘dimensions of quality’ had the following members as panelists for the discussion:• Dr. P.H Rao, Prof., Adminstrative Staff College of India, Hyderabad. • Dr. S.K Sikdar, Ministry of Health and Family Welfare, New Delhi• Mr. Bejon Misra, VOICE (A consumer organisation), New Delhi • Dr. N.A Khan , Academy of Hospital Administration, Noida• Dr. C.A.K Yesudian, TATA Institute of Social Sciences, Mumbai. • Prof. Deoki Nandan, Director, NIHFW.• Dr. B.S Garg, Prof. & Head, Deptt. of Community Medicine, Medical College, Wardha.
Dr. Bhattacharya initiated the panel discussion with the following questions:• Why quality was on the agenda? • How quality assurance needed to be institutionalised?• And why it was important to value quality?
Taking the panel discussion further Dr. Monika put forth before the panelists the following two questions: • What are the priority areas for improving quality services in India?• At what level in the health sector should the main efforts be directed to bring about this improvement?
Summary of Panel Discussion
• Need to keep the quality focus on secondary and primary health services. • Quality vs. quantity dilemma in health care• To create a competitive environment in the health sector.• Creating quality awareness by implementing quality at both district and community level. • Quality standards should be made uniformly applicable to both the public and the private sector as the same
would also facilitate the public private partnership model for delivery of healthcare. • Building of the human resource capacity for implementing quality. • Infrastructure and development of standards (IPHS) • patient’s charter and an effective complaint redressal system • Skill development for managing consumer complaints/disputes.• Need for defi ning quality • 3 A’s viz accessibility, availability and adaptability in relation to quality.• Building empathy and communication skills in the cadres involved in healthcare. • Change should start from something of immediate need and visibility• Link medical education with service delivery and to extend quality to beyond life services like post mortem.• Community version of health rights• Curriculum to manage the needs of the poor • Guidelines for healthcare providers• Prescription and provision of Drugs• Build in accountability for quality in both government and private• Training on statutory regulations, standards and audits.

12 Quality of Care in Health Sector
• Audit not a fault fi nding exercise but rather a monitoring mechanism legislation for consumers (Right to information),
• Cost of poor quality, generating resources for quality• Customer needs – internal, external, community – should be an essential reference point for all quality
initiatives, including right to information Emphasis on health and safety, customer protection (legal dimensions) and emergency of care.
• Political understanding and will to improve quality • Change from management to leadership• Customer Feedback to providers as an opportunity to improve• Standards to be communicated to patients in a user friendly and understandable way • Communities and consumers to be involved in planning, to have joint responsibility
Mr. Bijon Misra informed about the Hospital ranking study which had been published recently in magazine of Consumer Voice. Dr. N.A Khan made a power point presentation on the objectives of his academy (AHA) and briefl y informed about the courses and programs being run by them especially the ones relating to improving quality and role of National Accrededited Board of Hospitals and Healthcare providers (NABH) and the Quality Council of India (QCI)
5th June 2008
Ms. Sylvia Sax and Dr. Monika Krengel gave a presentation on ‘Strategic Framework for Quality Improvement in Health’ • Quality Challenges in Health• Health organisations are complex systems – clinical standards not enough• Cultural and organisational challenges• Competing power structures – politicians, Ministries and Departments, doctors, nurses, managers• Greatest challenge is to build capacity to manage these complexities
The principles and strategies of the strategic framework for improvement were explained. The pillars of the strategic framework was slightly changed from the framework given in GTZ • Consumer empowerment, protection, information, education, focus• Institutional development, regulations, framework, set-up• Management• Evidence based practice• Leadership and Human Resource Development
The presentation concluded with a note on the need to develop methods and tools for the above mentioned strategies keeping in view the cultural acceptability and also identify the ones responsible to implement, monitor, evaluate and adapt the same.
Dr. Annirudh Mukherjee made a presentation on QAP in West Bengal. The quality initiatives at primary level piloted in district Hoogly, and at the secondary hospital level piloted in two district hospitals and one sub
13Quality of Care in Health Sector
divisional hospital. The secondary level initiative and the focus was mainly on standards and documentation. The excel sheet based standard checklist (37 standard elements and 11 quality circles) developed was also demonstrated (Annexure 5).
The learning points were:• Keep on harping that QAP is not being enforced from the top- make it part of the system.• Identify champions in the system and utilise them in initial period. After some time QA becomes a culture. • Overcome initial scepticism with intense hand holding- authorities at higher levels should show personal
involvement• Keep focus on documentation- only policies and SOPs that are written get practiced• Keep documents simple- no document should cover more than 1 side of an A4 paper in 10 font size• Address training needs of all staff- keep them short, simple and focussed to needs• Develop a monitoring and evaluation plan right from the beginning• Develop measurable indicators for monitoring• Be patient- the start of the programme requires in extra effort. Hurrying up may be counter productive.
However, ask the facilities to prepare their timelines and monitor that they are being stuck to• Facilitation should be on site as far as practicable• Ensure physical comfort in all activities• Scale up with caution, QA requires intense hand-holding
The presentation by Dr. Preeti Kudesia, World Bank (Annexure 5) was on the state experiences of the secondary level hospital, quality improvement and management. The focus of the approach adopted was explained through the following case studies in a project undertaken by them:
The Quality improvement processes were:• Drug inventory and Rational Use of Drugs• Standard Treatment Protocols/Guidelines• Guidelines for action in emergency, OT, Labour room, OPD• Equipment Maintenance• Audits (case sheets, death reviews, prescription audits)• Patient Flow Management (time spent at different sites, overcrowding)• Hospital timings and rationalisation of duty hours• Healthcare Waste Management
Further dwelling on the mechanism of monitoring and evaluation, the key tools identifi ed were hospital information systems, activity and performance indicators, quality indicators, bench-marking and grading. The other areas, critical to quality initiatives were housekeeping, free services for the disadvantaged populations and behavioural changes in service providers. The presentation concluded with an enlisting of processes pertaining to quality enhancement and hospital systems improvement teams and process (HSIT).
A short fi lm on ‘quality improvement through HRD’ under the Maharashtra Health Systems Development Project (World Bank) was screened.
14 Quality of Care in Health Sector
Dr. Monika Krengel made a presentation on ‘Quality Management (QM) initiatives in Hospitals at Himachal Pradesh’. A diagrammatic presentation of the QM process was given along with the structure and levels of responsibility and how the development of standards took place through RUMBA approach. (Annexure 7)
The salient points of presentation are given below.
Steps of Introducing QM in HP
2002-2004: Basic Assessment, formation of Quality Circles, Quality Core Group and Quality Representatives in 6 Pilot Hospitals - 2004 onwards:1. Development and testing of Standards, using the Standards of the British Hospital Accreditation Programme
as a model for adaption, in 13 Hospitals (1st batch QM hospitals).2. Establishment of Directorate Quality Core Group (DQCG) and attempt to establish an Inter-sectoral Quality
Group. 3. Surveyor training and conduction of Self Assessments against the Standards, followed by gap analysis and
action planning in 26 Hospitals in 2005-2006 (1st and 2nd batch QM hospitals).4. Training of Peer Reviewers and conduction of external Peer Reviews in 13 hospitals (1st batch). 5. Conducted case studies in 6 pilot hospitals (2006). 6. Re-establishment of State Quality Core Group (SQCG) in 2006.7. Further revision of Hospital Standards (Version 3) in 2007
Tasks of the Hospital Quality Core Group (QCG)
• Formulation of Hospital’s QM Strategy and Policy • Sensitisation of Staff and awareness raising for quality improvement• Annual action planning and review of activities • Identifi cation of training needs and development of training plans • Support and supervision of Quality Circles and activities• Reporting of QM progress to the Directorate
Tasks of the Quality Representative (QR)
• Mediator between staff, QC and QCG• Report to QCG on the performance of the QC and progress of QM improvement plans• Monitoring, evaluation and documentation of QM activities, including follow up of the Annual Action Plan
Tasks of Quality Circles (QC)
• Identify problems or areas for improvement• Analyse problems or processes• Identify solutions• Prepare Action Plans
15Quality of Care in Health Sector
• Implement Improvement measures• Development of HP Hospital Standards
Steps in Quality programme for setting standards
The project and members of the Directorate studied and compared Standards and QM systems used by other countries, e.g. EFQM (European Foundation for QM), ISO, JCI (Joint Commission/US), British Hospital Accreditation Program (HAP)
Outcome
Basic contents and principles of all standards are very much the same: e.g. focus on patient satisfaction, on processes (instead of infrastructure), and on leadership and communication.
The Himachal Pradesh Standards were selected as a model, because they were:
• designed for small and middle scale hospitals,• Easily understandable, detailed and not leaving much scope for Interpretation• The British and the Indian Health System have some similarities• HAP allowed the Government of HP to use their standards as a model
Development of HP Hospital Standards
• The HAP Standards were reviewed and customised to local requirements through intensive group work at hospital (5 regional groups) and directorate level, following the RUMBA approach. Is the Standard
R – Relevant U – Understandable M – Measurable B – Behavioural (culturally acceptable and practical) and A – Achievable (within the next 5 years)
• Review and integration of local/national laws and regulations, e.g. Consumer Protection Act, Regulation of BIS, was done and new relevant criteria were added.
• It took about 6 months to draft the fi rst version (June to Dec. 2004), and another 9 months (Jan to Sep 2005) for testing and drafting of the second version.
• The third version of the HP Hospital Standards was reviewed by members of the SQCG and printed in 2007.
Some Achievements and Benefi ts of Quality programme
• Himachal Pradesh is the fi rst State in India that developed and applied Hospital Standards for the Public Sector, that provide a monitoring tool for performance and improvement.
• Compliance with the Standards is already quite satisfactory (40 % in the fi rst Self Assessment, improved to 53 % in the second Self-Assessment.
16 Quality of Care in Health Sector
• A team approach for problem solving and quality improvement has been initiated in all QM hospitals, through Quality Circles.
• Action planning and monitoring with an emphasis on Quality Improvement takes place for the fi rst time in those hospitals.
• Rationalisation of facilities/manpower and improved resource utilisation has started. • Innovative models for local good practices are implemented: e.g. improvement and monitoring of patient
satisfaction and communication, medical records, signage, bio-medical waste management, health and safety, repair and maintenance of medical equipment.
• More scope for staff initiative and education and for exchange of best practices.• The Quality of healthcare in the QM Hospitals has visibly and measurably improved, following the approach
to focus on promotion of competition between hospitals and introduction of low-cost incentives and learning through the exchange of best practices.
• Easy reachable, visible and mandatory changes, like improvement of sanitation, signage, patient information and safety.
• Strengthening of communication skills and means.• Most hospitals accepted QM as an opportunity to strengthen their position towards the Centre, Court
(consumer protection act) and Politicians • Effi cient knowledge transfer, through emphasis on high coverage in reaching professionals; see large amount
of trainings and workshops and successive inclusion of all districts (examples),• A group of about 20-30 key professionals who actively used concepts and material developed in their
environment and developed tools on their own, like in-house training modules for staff, standard operating procedures, draft publications on safety issues, fi rst aid and so on (even starting websites),
• A good documentation and dissemination of all trainings, workshops and tools
The next presentation was by Dr. Raghu, Block Medical Offi cer, CHC, Nagarota (Annexure 7) on ‘implementing quality’. He expressed quality as :1. Achievement of pre-defi ned Standards / Targets. 2. Doing the right thing in right way at right time.3. Generating resources and using them for further improvement4. Minimizing Confl icts.
He explained the mechanism of monitoring standards through formation of quality core group and quality circles. He outlined the specifi c policies and procedure adopted to operationalise quality. He informed about the facility of a medicine bank, suggestion box, the format of the patient exit form and the effort on funds generation. He explained how the income generated was being used to improve the surroundings and for the repair and maintenance of the equipments and infrastructure of the hospital.
He concluded by thanking GTZ and the Rogi Kalyan Samiti for their support to the quality initiative.
Ms. Sylvia made a presentation on the ‘key elements of curriculum development’ in which she explained the concept of the hierarchy of competencies and the general principles and the processes to be followed while developing a curriculum.
17Quality of Care in Health Sector
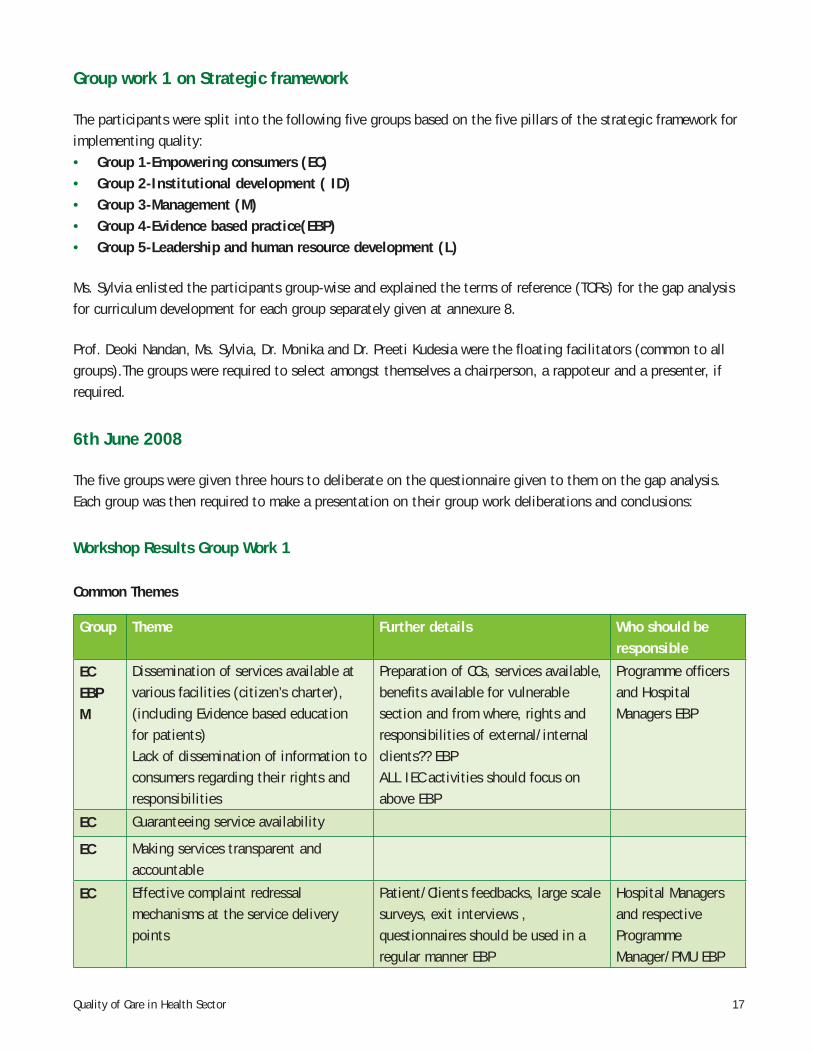
Group work 1 on Strategic framework
The participants were split into the following fi ve groups based on the fi ve pillars of the strategic framework for implementing quality:• Group 1-Empowering consumers (EC)• Group 2-Institutional development ( ID)• Group 3-Management (M)• Group 4-Evidence based practice(EBP)• Group 5-Leadership and human resource development (L)
Ms. Sylvia enlisted the participants group-wise and explained the terms of reference (TORs) for the gap analysis for curriculum development for each group separately given at annexure 8.
Prof. Deoki Nandan, Ms. Sylvia, Dr. Monika and Dr. Preeti Kudesia were the fl oating facilitators (common to all groups).The groups were required to select amongst themselves a chairperson, a rappoteur and a presenter, if required.
6th June 2008
The fi ve groups were given three hours to deliberate on the questionnaire given to them on the gap analysis. Each group was then required to make a presentation on their group work deliberations and conclusions:
Workshop Results Group Work 1
Common Themes
Group Theme Further details Who should be responsible
ECEBPM
Dissemination of services available at various facilities (citizen’s charter), (including Evidence based education for patients)Lack of dissemination of information to consumers regarding their rights and responsibilities
Preparation of CCs, services available, benefi ts available for vulnerable section and from where, rights and responsibilities of external/internal clients?? EBPALL IEC activities should focus on above EBP
Programme offi cers and Hospital Managers EBP
EC Guaranteeing service availability
EC Making services transparent and accountable
EC Effective complaint redressal mechanisms at the service delivery points
Patient/Clients feedbacks, large scale surveys, exit interviews , questionnaires should be used in a regular manner EBP
Hospital Managers and respective Programme Manager/PMU EBP
18 Quality of Care in Health Sector
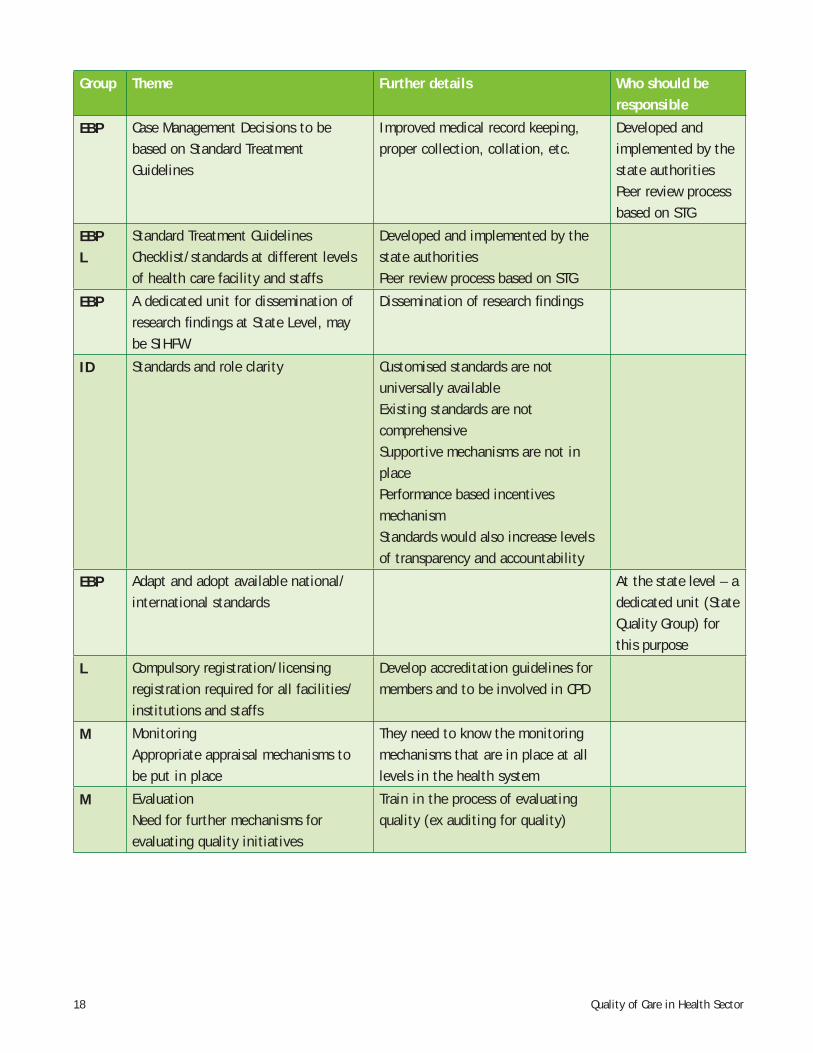
Group Theme Further details Who should be responsible
EBP Case Management Decisions to be based on Standard Treatment Guidelines
Improved medical record keeping, proper collection, collation, etc.
Developed and implemented by the state authorities Peer review process based on STG
EBPL
Standard Treatment GuidelinesChecklist/standards at different levels of health care facility and staffs
Developed and implemented by the state authorities Peer review process based on STG
EBP A dedicated unit for dissemination of research fi ndings at State Level, may be SIHFW
Dissemination of research fi ndings
ID Standards and role clarity Customised standards are not universally availableExisting standards are not comprehensiveSupportive mechanisms are not in place Performance based incentives mechanismStandards would also increase levels of transparency and accountability
EBP Adapt and adopt available national/international standards
At the state level – a dedicated unit (State Quality Group) for this purpose
L Compulsory registration/licensing registration required for all facilities/institutions and staffs
Develop accreditation guidelines for members and to be involved in CPD
M MonitoringAppropriate appraisal mechanisms to be put in place
They need to know the monitoring mechanisms that are in place at all levels in the health system
M EvaluationNeed for further mechanisms for evaluating quality initiatives
Train in the process of evaluating quality (ex auditing for quality)
19Quality of Care in Health Sector
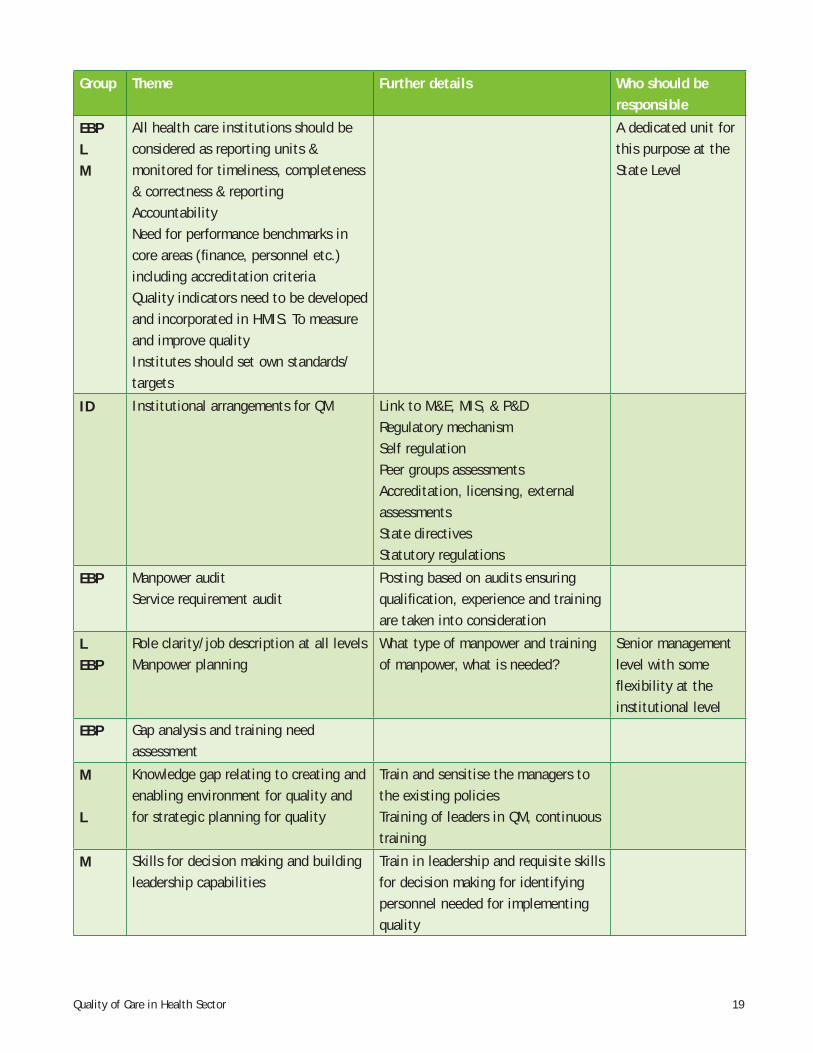
Group Theme Further details Who should be responsible
EBPLM
All health care institutions should be considered as reporting units & monitored for timeliness, completeness & correctness & reportingAccountability Need for performance benchmarks in core areas (fi nance, personnel etc.) including accreditation criteriaQuality indicators need to be developed and incorporated in HMIS. To measure and improve qualityInstitutes should set own standards/targets
A dedicated unit for this purpose at the State Level
ID Institutional arrangements for QM Link to M&E, MIS, & P&DRegulatory mechanismSelf regulationPeer groups assessmentsAccreditation, licensing, external assessmentsState directivesStatutory regulations
EBP Manpower auditService requirement audit
Posting based on audits ensuring qualifi cation, experience and training are taken into consideration
LEBP
Role clarity/job description at all levelsManpower planning
What type of manpower and training of manpower, what is needed?
Senior management level with some fl exibility at the institutional level
EBP Gap analysis and training need assessment
M L
Knowledge gap relating to creating and enabling environment for quality and for strategic planning for quality
Train and sensitise the managers to the existing policiesTraining of leaders in QM, continuous training
M Skills for decision making and building leadership capabilities
Train in leadership and requisite skills for decision making for identifying personnel needed for implementing quality
20 Quality of Care in Health Sector
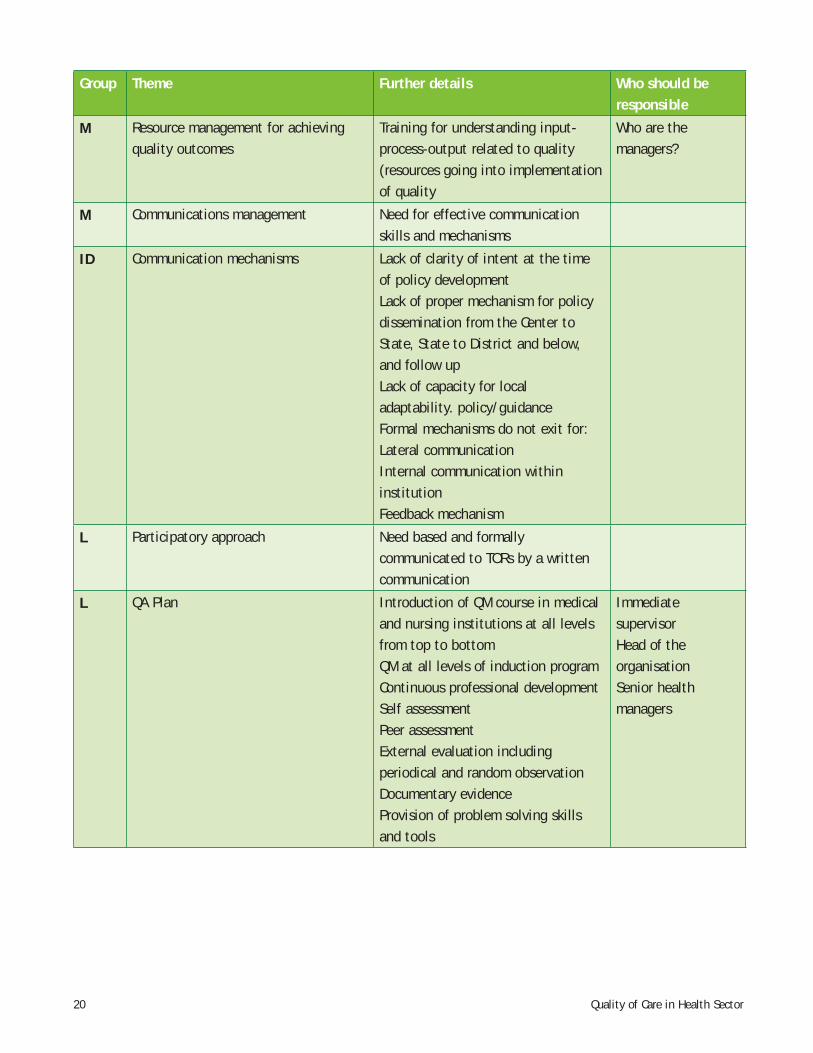
Group Theme Further details Who should be responsible
M Resource management for achieving quality outcomes
Training for understanding input-process-output related to quality (resources going into implementation of quality
Who are the managers?
M Communications management Need for effective communication skills and mechanisms
ID Communication mechanisms Lack of clarity of intent at the time of policy developmentLack of proper mechanism for policy dissemination from the Center to State, State to District and below, and follow upLack of capacity for local adaptability. policy/guidance Formal mechanisms do not exit for:Lateral communicationInternal communication within institutionFeedback mechanism
L Participatory approach Need based and formally communicated to TORs by a written communication
L QA Plan Introduction of QM course in medical and nursing institutions at all levels from top to bottomQM at all levels of induction program Continuous professional developmentSelf assessmentPeer assessmentExternal evaluation including periodical and random observationDocumentary evidenceProvision of problem solving skills and tools
Immediate supervisor Head of the organisationSenior health managers

21Quality of Care in Health Sector
Group Work 2 on Formulation of Key competencies, learning objectives, contents and learning methods
Next the TORs for the second round of the Group work were explained and distributed. The main tasks for group work 2 were to reconsider the identifi ed gaps and to formulate key competencies and learning objectives suitable to fi ll the gaps, to identify course contents that could help to attain the competency and to suggest learning methods that would enable the learning process. The groups were asked to prioritise the overall learning objectives and to select only two priority areas each.
7th June 2008
The groups continued their deliberations and the presentation began on schedule. Prof. Deoki Nandan welcomed Dr. I.P Kaur, Deputy Commissioner (Trg.), Ministry of Health and Family Welfare and requested her to chair the proceedings for the day( Details of presentation group work 2 at Annexure 9).
The fi rst presentation was made by the group on Empowering Consumers. Mr. Bejon Misra projected the following three areas as priority:• Consumer education and awareness• Developing relationship between service providers and patients• Complaint redressal and mechanism
He explained the course content for each of the areas mentioned above and also listed a variety of learning methods ranging from lectures to screening of short documentaries to achieve the desired learning objectives.
In the discussion, following the presentation, the learning objective pertaining to consumer feedback was widely debated and one of the participants suggested that the term feedback should be placed by a more constructive term ‘partnership’.
Dr. Sanjay Aggarwal made a presentation for the group on Institutional Development and identifi ed communication and standards as the priority area for curriculum development. The suggested course content and methods of learning were outlined with clear objectives in place.
The participants were concerned about the focus of institutional development to be limited to only two areas, it was however explained that the same was being done so as to avoid repetition of course content due to overlap of areas between fi ve pillars of the strategic framework.
Prof. Bhattacharya gave a presentation on behalf of the Management Group. She informed that since the area of management was very wide the group had chosen fi ve areas of priority each representing one session. The areas identifi ed were:• Sensitisation on quality management • Rationalisation of resources available for quality• Identifi cation and interpretation of quality indicators
22 Quality of Care in Health Sector
• Supportive supervision and monitoring • Evaluation
Responding to the presentation, the participants discussed the limitations of using the existing HMIS for monitoring quality and also debated on the importance of supportive supervision.
The group on Evidence Based Practice made their presentation wherein Dr. Aniruddha Mukherjee identifi ed the following three areas for priority:• Methods of acquiring data• Analysing data and preparing action plans • Hospital standards including standard treatment procedures
In the open session following the presentation, it was suggested that clinical data be generated using ICD-10 and there was also suggestion to include information on intellectual property rights in the course content of the area relating to methods of acquiring data. The issue of generating resources by disseminating data was also raised by one of the participants.
The fi nal presentation was on Leadership and Human Resource Development. Mr. Mallikarjuna identifi ed the following two areas as priority for curriculum development:• Overview and concept of quality management in healthcare.• Human resource development for QM in health care
In response to the presentation, the approach to QM was debated wherein the PLA (Plan, Learn and Act) approach and the 3A’s (Accessibility, Availability and Adaptability) approaches were suggested.
The post lunch session was a plenary discussion on the presentations; Dr. I.P Kaur was requested to chair the same. Prof Bhattacharya opened the session by inviting Ms. Sylvia to explain the future course of action in relation to development of the training course. Prof. Nandan requested the plenary to discuss the modalities for piloting the course and emphasised on the need to adopt the approach involving minimum fi nancial and HR implications. Accordingly the participants dwelled on the issues like course design, practical implementation, specifi city of the course content and focus on quality aspects. There was also a suggestion to set up a repository for literature on quality studies in India. One of the participants suggested setting up of a documentation cum research cell on quality at NIHFW. The participants were informed that the GTZ is preparing a document on quality initiatives in India and the same would be available in August this year. Dr. Kaur wanted an integrated approach to be adopted by the state in implementing quality initiatives with a specifi c reference to the Quality Assurance Cells/Groups (QAC/Gs) already set up at the district levels and also suggested a linkage between the SIHFWs and NIHFW in conducting comparative studies. Prof. Nandan was also of the view that since the QAGs at the state end district levels were mandatory, their members should also be empowered to implement quality. This was followed by a discussion on the QAGs, their present status and mandate. One of the participants suggested that while conducting resource mapping all the available institutions for implementing quality can be listed and assigned responsibilities keeping in view their capacities. The participants were informed that the curriculum developed through the deliberations of the group work would be further worked upon by a smaller group of experts. Thereafter, the Chairperson Dr. Kaur summed up the plenary by insisting on convergence
23Quality of Care in Health Sector
through a dynamic and synergistic approach leading to integration of programmes and institutions. She also stressed on the need to produce quality within existing resources and felt that the quality improvement process has to be in continuum.
The session for the day concluded with Ms. Sylvia thanking the participants for their valuable contributions.
8th June 2008
Session began with Ms. Sylvia giving a presentation on the agreed draft curriculum developed wherein she had divided the curriculum into two categories namely priority 1 and priority 2. She informed that the categorisation had been done on the basis of the priorities given by the groups and that during the training course the areas in the category 1 would be given more time than those listed in category 2. The areas under each category were as follows:
Priority 1 Priority 2
Quality management systemCommunicationStandardsEvaluation (i) Models and methods (ii) Quality indicators
Management overview Monitoring and supervisionProfessional development
The suggestions following the presentation included the ones relating to inclusion of supporting quality improvement as the fi fth area under category 1, building values, team management, maintenance of medical records and accreditation.
Dr. Raghu made a brief presentation on the database developed to monitor maternal and child care.
This was followed by a closing address from Dr. Monika and Ms. Sylvia wherein they once again thanked the participants for their valuable contribution and their commitment towards the workshop. Prof Bhattacharya requested the participants to give their parting comments wherein most of the participants thanked the organisers and described the workshop as a great learning experience and promised to extend their full co-operation and support to the cause of promoting quality in healthcare in India. The participants were also very appreciative of the initiative taken to adopt a systematic and scientifi c approach to curriculum development in the workshop.
Prof. Deoki Nandan concluded the session by stating that the workshop had achieved its purpose and accordingly called for a standing ovation for the organising team headed by Prof Bhattacharya and comprising of Dr. A. Bhardwaj and Dr. Nair. Prof. Nandan also thanked the World Bank for extending the fi nancial support and the GTZ for providing the technical expertise on the subject and stated that he looked forward to a very fruitful partnership between NIHFW and the Heidelberg University. Prof. Nandan also thanked the senior offi cials from the Ministry of Health and Family Welfare for extending their co-operation in organising the workshop.
24 Quality of Care in Health Sector
Discussion and fi nalisation of the contents of the training programme and brainstorming about the technical inputs required at NIHFW, New Delhi
In the course of the second week the curriculum essentials were completed and a fi rst draft of the course contents and learning methods was completed in discussion with the faculty members and presented to them and verbally approved by the Director of NIHFW, Prof. Deoki Nandan. The group of NIHFW, GTZ and international experts then drafted a daily schedule for the draft curriculum. An overview of the curriculum essentials and the main steps and outcomes in the curriculum development process is provided in the following:
Curriculum Essentials
Course title: Improving quality of care in the health sector
Target audience: Mid-level policy makers, including national (e.g. MoH), state (e.g. Senior offi cers from Directorate and Principals/faculty of the SIHFW) and District level (e.g. CMOs and SMOs of District Hospitals).
Number of participants: 20
Selection criteria: It was discussed at length if the application of selection criteria, apart from those determined by the target audience, is feasible in a Government setting. To add a percentage for female participants (e.g. 20%) was a suggestion by the consultants, 15 years experience and clear 5 years left in service were also discussed.
25Quality of Care in Health Sector
Length of the course: 6 days
Time frame: It was proposed that the fi rst course should take place in the 2nd half of November 2008 and that further preparations for the course content should take place in September, 2008. Further courses would be planned for 2009, e.g. in February and in May/June 2009.
Sponsors: It was suggested that GTZ Health Sector Support will sponsor this course.
Resource persons will be recruited from the NIHFW faculty itself and from other institutions in India. In the beginning, e.g. the fi rst two courses, it is planned to involve 2-3 international experts to provide a kind of tandem teaching and to exchange and share the material so that local and international perspectives and approaches are integrated.
Educational strategy: To design a framework for senior and mid-level health offi cials so that they are able to conceive and frame policies and strategies to improve the quality parameters in the health care system at all levels.
Overall course aim: To increase the competencies of decision makers to understand and apply concepts of quality management in healthcare and to support and promote the implementation of the same.
Learning objectives and contents:
Seven Overall Learning Objectives were identifi ed (below bold) and subdivided in specifi c learning objectives (bullets). The overall and specifi c learning objectives of the course will be that, by the end of the course, the participants will be able to:
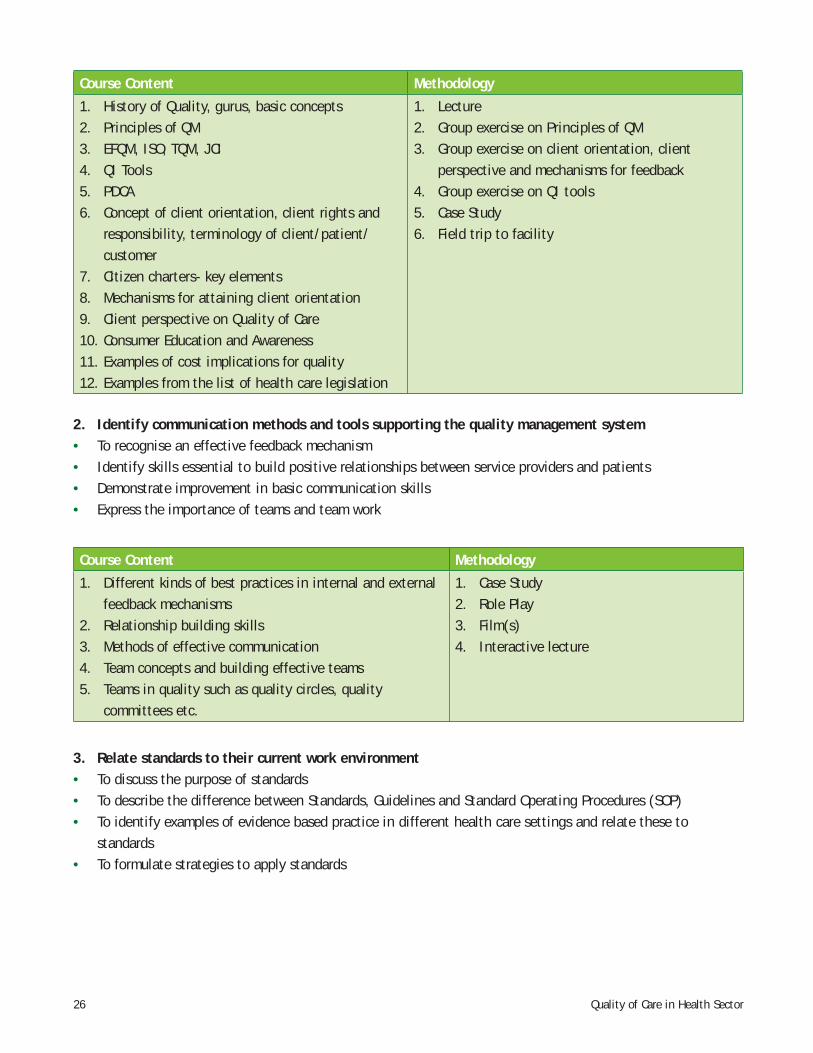
1. Describe a quality management system including its major components• Defi ne quality in healthcare • List principles in a quality management system• Explain user focus as central to a QM system• Recognise an effective Citizen’s Charter• Identify different quality management frameworks• Provide examples of the cost of poor quality and savings through implementing a QM system• Identify key legislation relevant to QM
Overall course framework and strategy
26 Quality of Care in Health Sector
Course Content Methodology
1. History of Quality, gurus, basic concepts2. Principles of QM3. EFQM, ISO, TQM, JCI4. QI Tools5. PDCA6. Concept of client orientation, client rights and
responsibility, terminology of client/patient/customer
7. Citizen charters- key elements8. Mechanisms for attaining client orientation9. Client perspective on Quality of Care10. Consumer Education and Awareness11. Examples of cost implications for quality12. Examples from the list of health care legislation
1. Lecture2. Group exercise on Principles of QM3. Group exercise on client orientation, client
perspective and mechanisms for feedback4. Group exercise on QI tools5. Case Study6. Field trip to facility
2. Identify communication methods and tools supporting the quality management system• To recognise an effective feedback mechanism• Identify skills essential to build positive relationships between service providers and patients• Demonstrate improvement in basic communication skills• Express the importance of teams and team work
Course Content Methodology
1. Different kinds of best practices in internal and external feedback mechanisms
2. Relationship building skills3. Methods of effective communication4. Team concepts and building effective teams5. Teams in quality such as quality circles, quality
committees etc.
1. Case Study2. Role Play3. Film(s)4. Interactive lecture
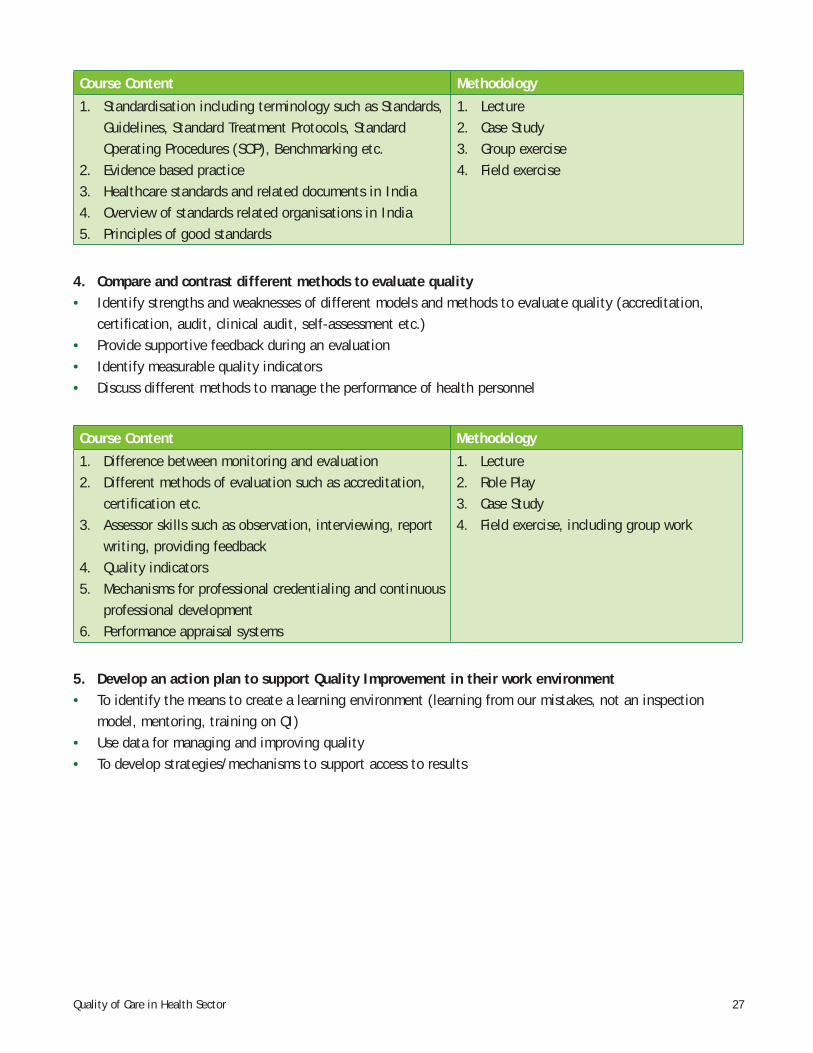
3. Relate standards to their current work environment• To discuss the purpose of standards• To describe the difference between Standards, Guidelines and Standard Operating Procedures (SOP)• To identify examples of evidence based practice in different health care settings and relate these to
standards• To formulate strategies to apply standards
27Quality of Care in Health Sector
Course Content Methodology
1. Standardisation including terminology such as Standards, Guidelines, Standard Treatment Protocols, Standard Operating Procedures (SOP), Benchmarking etc.
2. Evidence based practice3. Healthcare standards and related documents in India4. Overview of standards related organisations in India5. Principles of good standards
1. Lecture2. Case Study3. Group exercise4. Field exercise
4. Compare and contrast different methods to evaluate quality• Identify strengths and weaknesses of different models and methods to evaluate quality (accreditation,
certifi cation, audit, clinical audit, self-assessment etc.)• Provide supportive feedback during an evaluation• Identify measurable quality indicators• Discuss different methods to manage the performance of health personnel
Course Content Methodology
1. Difference between monitoring and evaluation2. Different methods of evaluation such as accreditation,
certifi cation etc.3. Assessor skills such as observation, interviewing, report
writing, providing feedback4. Quality indicators5. Mechanisms for professional credentialing and continuous
professional development6. Performance appraisal systems
1. Lecture2. Role Play3. Case Study4. Field exercise, including group work
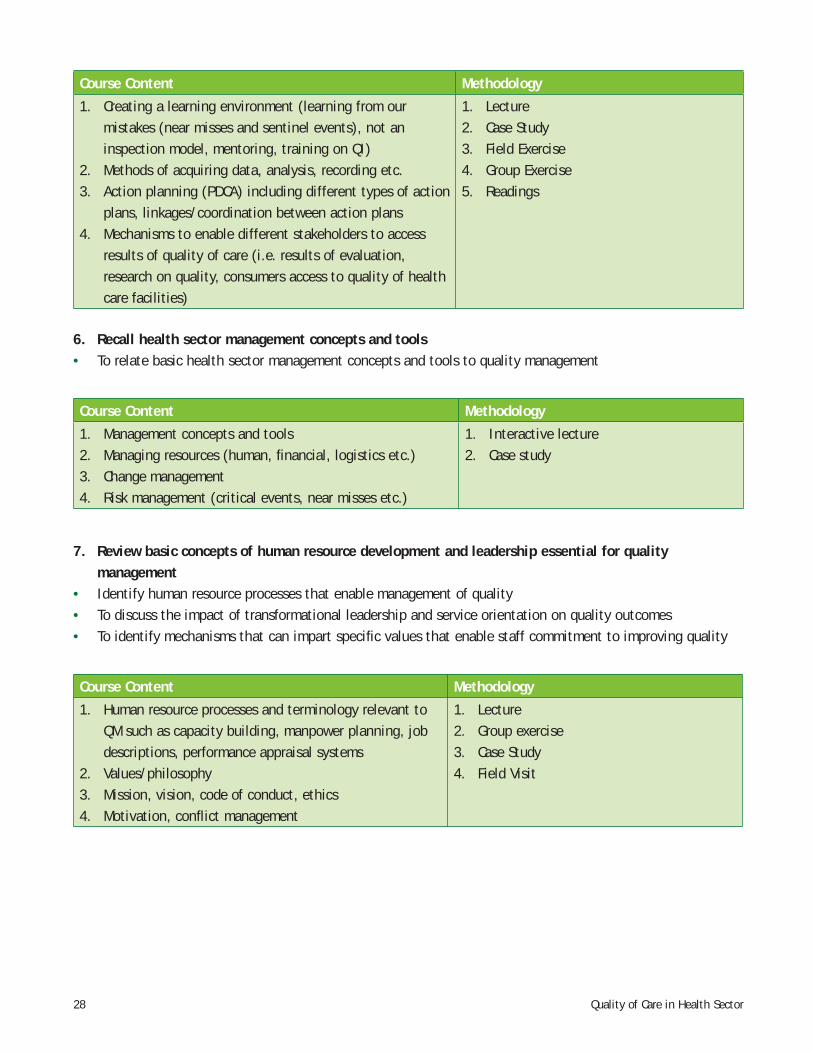
5. Develop an action plan to support Quality Improvement in their work environment• To identify the means to create a learning environment (learning from our mistakes, not an inspection
model, mentoring, training on QI)• Use data for managing and improving quality• To develop strategies/mechanisms to support access to results
28 Quality of Care in Health Sector
Course Content Methodology
1. Creating a learning environment (learning from our mistakes (near misses and sentinel events), not an inspection model, mentoring, training on QI)
2. Methods of acquiring data, analysis, recording etc.3. Action planning (PDCA) including different types of action
plans, linkages/coordination between action plans 4. Mechanisms to enable different stakeholders to access
results of quality of care (i.e. results of evaluation, research on quality, consumers access to quality of health care facilities)
1. Lecture2. Case Study3. Field Exercise4. Group Exercise5. Readings
6. Recall health sector management concepts and tools• To relate basic health sector management concepts and tools to quality management
Course Content Methodology
1. Management concepts and tools2. Managing resources (human, fi nancial, logistics etc.)3. Change management4. Risk management (critical events, near misses etc.)
1. Interactive lecture2. Case study
7. Review basic concepts of human resource development and leadership essential for quality management
• Identify human resource processes that enable management of quality• To discuss the impact of transformational leadership and service orientation on quality outcomes• To identify mechanisms that can impart specifi c values that enable staff commitment to improving quality
Course Content Methodology
1. Human resource processes and terminology relevant to QM such as capacity building, manpower planning, job descriptions, performance appraisal systems
2. Values/philosophy3. Mission, vision, code of conduct, ethics4. Motivation, confl ict management
1. Lecture2. Group exercise3. Case Study4. Field Visit
29Quality of Care in Health Sector
Next steps
• There is a need to orient the state level secretaries and mission directors to the need of such courses which can help them identify the needs of the state, prioritise them and then look for possible solutions. For this there can be an advocacy group formed at NIHFW along with the MOHFW and development partners which can try and convince the secretaries and other authorities about the usefulness of these courses.
• Regular feedback mechanism of interacting with participants needs to be developed. There is also a need to have some updation and re-orientation training after a certain period. This may be through the proposed e-health setup which NIHFW proposes to have by the year 2008-09.
• More active canvassing by NIHFW for the upcoming state level courses with the help of the development partners is needed.
• Having a web based resource centre where documents, presentations and case studies will be stored is also contemplated with the help of the WBI. This will help in updating the knowledge of the participants on a regular basis.
• This course on Quality of Care should be carried forward this year and GTZ has promised support for initial few courses, subsequently it will be institutionalised in the states also.
• Another short course is also proposed in collaboration with Harvard for only bureaucrats and director generals with support of WBI.

Annexures
32 Quality of Care in Health Sector
Anne
xure
-1
Agen
da -
(W
orks
hop)
4 Ju
ne 0
8W
edne
sday
5 Ju
ne 0
8Th
ursd
ay6
June
08
Frid
ay7
June
08
Satu
rday
8 Ju
ne 0
8Su
nday
9.30
-
11.0
0 AM
Sum
mar
y of
pre
viou
s da
y’s
disc
ussi
on
Pres
enta
tion
of
a st
rate
gic
fram
ewor
k (M
. Kr
enge
l/S.
Sax)
Five
wor
king
gr
oups
Gr
oup
wor
k(C
ontd
…)
Fina
lisat
ion
of a
cou
rse
fram
ewor
k
11.0
0 –
11.3
0 A.
MTe
a/Co
ffee
bre
akTe
a/Co
ffee
bre
akTe
a/Co
ffee
bre
akTe
a/Co
ffee
bre
ak
11.3
0 –
12.1
5 P.
MQu
alit
y in
itia
tive
s in
Ind
ia
(Dr.
Anir
uddh
Muk
herj
ee)
Wor
king
gro
ups
(Con
td…
)Pr
esen
tati
on o
f gr
oup
wor
k
Acti
on p
lan
for
deve
lopi
ng
the
full
cour
se a
t NI
HFW
12.1
5 –
1.15
P.M
Arri
val f
rom
Del
hiQu
alit
y in
itia
tive
s in
se
cond
ary
leve
l hea
lth
care
(D
r. Pr
eeti
Kud
esia
)
Wor
king
gro
up
pres
enta
tion
Plan
ning
for
con
duct
ing
the
trai
ning
–fu
ture
cou
rse
of
acti
on.
Wra
p up
and
nex
t st
eps
1.15
–
2.00
P.M
Lunc
hLu
nch
Lunc
hLu
nch
Lunc
h
33Quality of Care in Health Sector
4 Ju
ne 0
8W
edne
sday
5 Ju
ne 0
8Th
ursd
ay6
June
08
Frid
ay7
June
08
Satu
rday
8 Ju
ne 0
8Su
nday
2.00
-
3.15
P.M
Wel
com
e &
intr
oduc
tion
to
the
wor
ksho
p(D
eoki
Nan
dan)
Obje
ctiv
es a
nd e
xpec
tati
ons
(M. Bh
atta
char
ya)
Agen
da(M
onik
a Kr
enge
l)
Over
view
of
a St
rate
gic
Fram
ewor
k fo
r qu
alit
y of
car
e(S
ylvi
a Sa
x)
Qua
lity
init
iati
ves
GTZ
–H
imac
hal P
rade
sh
(M.
Kren
gel)
Pre
sent
atio
n on
cu
rric
ulum
de
velo
pmen
t (S
.Sax
)
Plen
ary
disc
ussi
on o
n pr
esen
tati
ons
Depa
rtur
e fo
r De
lhi
3.15
–
3.30
P.M
Tea/
Coff
ee b
reak
Tea/
Coff
ee b
reak
Tea/
Coff
ee b
reak
Tea/
Coff
ee b
reak
3.30
–
5.30
P.M
Pane
l dis
cuss
ion
on
dim
ensi
ons
of q
ualit
y
(M. Kr
enge
l/S.
Sax)
Plen
ary
disc
ussi
on o
n a
stra
tegi
c fr
amew
ork
“Evi
denc
e fo
r pr
iori
ty”
(Cha
irpe
rson
: De
oki
Nand
an)
Intr
oduc
tion
to
TORs
for
gr
oup
wor
k(S
. Sa
x)
Grou
p w
ork
(in
5 Gr
oups
)Fi
eld
trip
34 Quality of Care in Health Sector
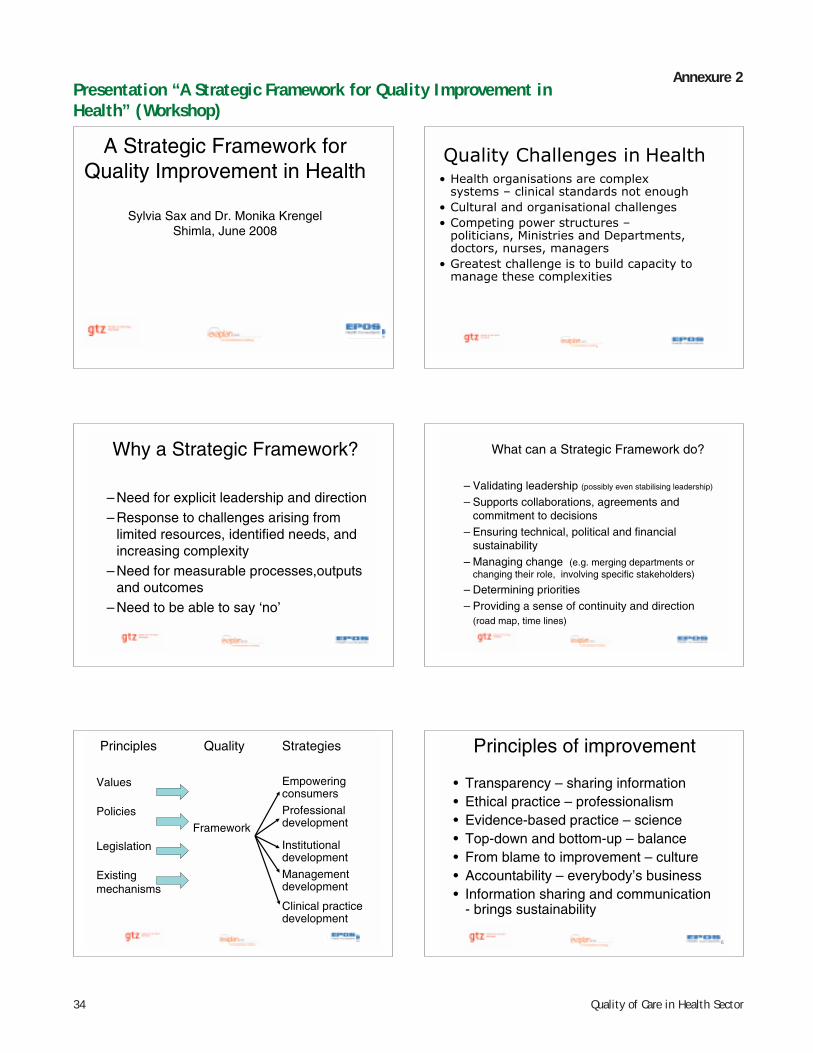
Annexure 2
A Strategic Framework for Quality Improvement in Health
Sylvia Sax and Dr. Monika KrengelShimla, June 2008
Quality Challenges in Health
• Health organisations are complex
systems – clinical standards not enough
• Cultural and organisational challenges
• Competing power structures –
politicians, Ministries and Departments,
doctors, nurses, managers
• Greatest challenge is to build capacity to
manage these complexities
Why a Strategic Framework?
– Need for explicit leadership and direction– Response to challenges arising from
limited resources, identified needs, and increasing complexity
– Need for measurable processes,outputsand outcomes
– Need to be able to say ‘no’
What can a Strategic Framework do?
– Validating leadership (possibly even stabilising leadership)
– Supports collaborations, agreements and commitment to decisions
– Ensuring technical, political and financial sustainability
– Managing change (e.g. merging departments or changing their role, involving specific stakeholders)
– Determining priorities– Providing a sense of continuity and direction
(road map, time lines)
Principles Quality Strategies
Values Empoweringconsumers
PoliciesFramework
Professionaldevelopment
Legislation Institutionaldevelopment
Existingmechanisms
Managementdevelopment
Clinical practice development
5
Principles of improvement
• Transparency – sharing information• Ethical practice – professionalism• Evidence-based practice – science• Top-down and bottom-up – balance• From blame to improvement – culture• Accountability – everybody’s business• Information sharing and communication
- brings sustainability
6
Presentation “A Strategic Framework for Quality Improvement in Health” (Workshop)
35Quality of Care in Health Sector
Strategies for improvement
• Empowering consumers• Professional development• Institutional development• Management development• Clinical practice developmentOver the next few days we will examine strategies
for improvement and ensure that they are relevant to the Indian context.
7
S1: Consumer empowerment, protection, information, education, focus ..
e.g.• Improvement of patient communication• Improvement and definition of patient’s rights and
obligations• Improvement of patient satisfaction, monitoring
and evaluation • Public access to information on health services
qualityClient focus always enjoy the top-priority in JCI, QCI and
otherQuality standards – include internal and external clients
S2 Institutional development, regulations, framework, set-up
• Licensing and supervision • National/state standards for service
delivery• Reliable assessment processes and
training• Feedback and organisational development• Inter-institutional communication and
knowledge sharing• Safe and appropriate environment
9
S3: Management
• General Management– Policy, planning, implementation, supervision, feedback
• Decentralisation– Giving skills and authority to local managers
• Resource management– Good services do not waste money
• Risk management– Systematic learning from mistakes– Prevention of damage and litigation
• Communications management – sharing good practices etc.
S4: Evidence based practice
• Unacceptable variations in clinical practices • Use data for decisions• Research support evidence based practice• Commitment to evidence based medicine • Knowledge about the latest medical research
results, change of practice • Sharing best practices • Applying standard Operating Procedures
S5: Leadership and Human Resource Development
• Technical competence of staff is essential to effective health care
• Unethical behaviour has killed patients and damaged organisations
• Shift to multidisciplinary team working, which is not possible without an effective organisation
• Ensure the right people are in the right job• Leaders are committed to quality improvement
36 Quality of Care in Health Sector
Basics Legal Challenges
CMEsPerformanceAppraisalIncentives/MotivationJob descriptions
RegistrationLicensingAdherence toStandards andRegulationsEthics
New modes of communicationand knowledge management
13
Methods and Tools of Principal Strategies
To be developed and agreed on in this workshop?
To be based on already approved approaches and on their cultural acceptability?
To be implemented, evaluated, monitored and adapted by whom?
37Quality of Care in Health Sector
Annexure 3
2
UniversitätsKlinikum Heidelberg
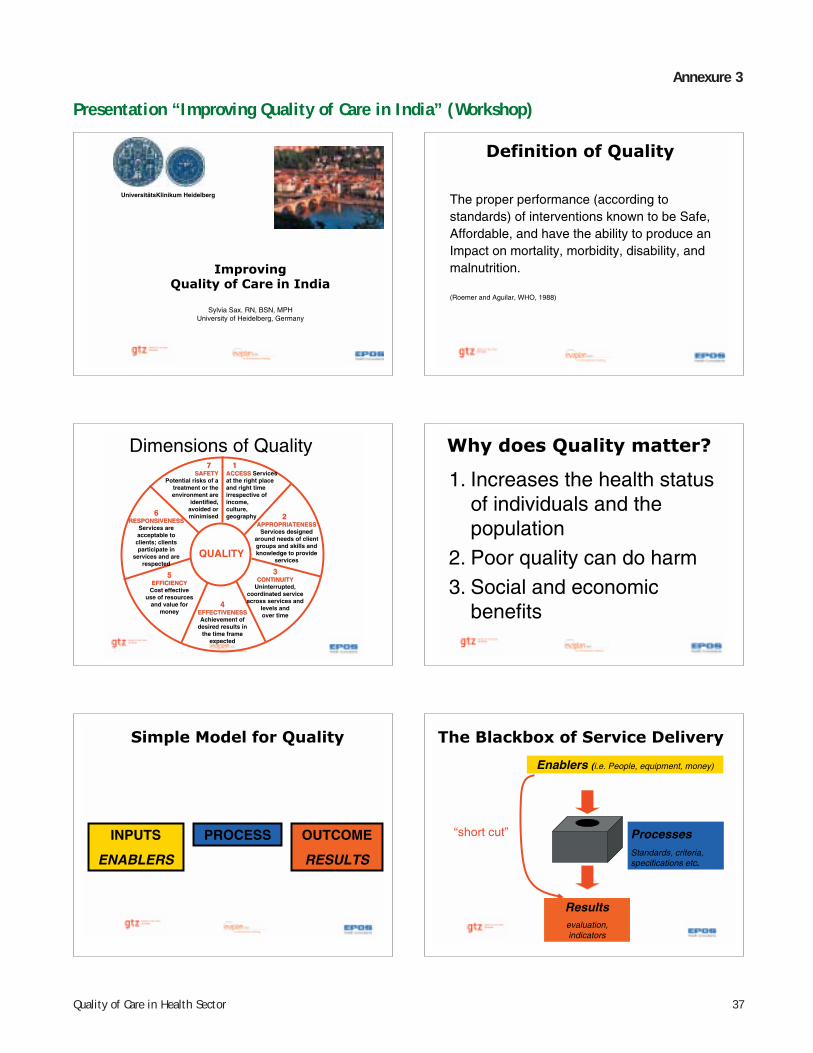
Improving
Quality of Care in India
Sylvia Sax. RN, BSN, MPHUniversity of Heidelberg, Germany
3
Definition of Quality
The proper performance (according to standards) of interventions known to be Safe, Affordable, and have the ability to produce an Impact on mortality, morbidity, disability, and malnutrition.
(Roemer and Aguilar, WHO, 1988)
4
Dimensions of Quality
QUALITY
11ACCESSACCESS Services at the right place and right time irrespective of income,culture,geography 22
APPROPRIATENESSAPPROPRIATENESSServices designed
around needs of client groups and skills and knowledge to provide
services
33CONTINUITYCONTINUITY
Uninterrupted,coordinated service across services and
levels andover time
44EFFECTIVENESSEFFECTIVENESSAchievement of
desired results in the time frame
expected
55EFFICIENCYEFFICIENCY
Cost effective use of resources
and value for money
66RESPONSIVENESSRESPONSIVENESS
Services are acceptable to clients; clients participate in
services and are respected
77SAFETYSAFETY
Potential risks of a treatment or theenvironment are
identified,avoided orminimised
5
Why does Quality matter?
1. Increases the health status of individuals and the population
2. Poor quality can do harm3. Social and economic
benefits
6
Simple Model for Quality
INPUTS
ENABLERS
PROCESS OUTCOME
RESULTS
7
The Blackbox of Service Delivery
Enablers (i.e. People, equipment, money)
Resultsevaluation,indicators
“short cut” ProcessesStandards, criteria, specifications etc.
Presentation “Improving Quality of Care in India” (Workshop)
38 Quality of Care in Health Sector
8
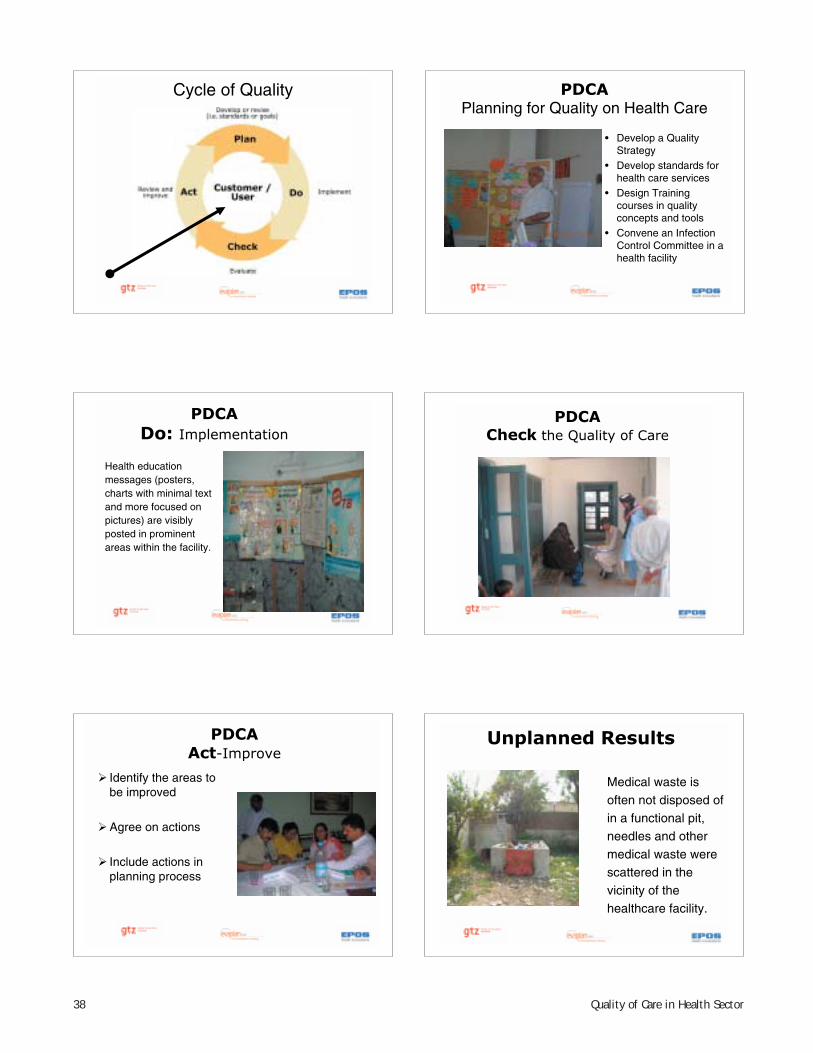
Cycle of Quality
9
PDCA
Planning for Quality on Health Care
• Develop a Quality Strategy
• Develop standards for health care services
• Design Training courses in quality concepts and tools
• Convene an Infection Control Committee in a health facility
10
PDCA
Do: Implementation
Health education messages (posters, charts with minimal text and more focused on pictures) are visibly posted in prominent areas within the facility.
11
PDCA
Check the Quality of Care
12
PDCA
Act-Improve
� Identify the areas to be improved
�Agree on actions
� Include actions in planning process
13
Unplanned Results
Medical waste is often not disposed of in a functional pit, needles and other medical waste were scattered in thevicinity of the healthcare facility.
39Quality of Care in Health Sector
14
Planned Results
Managing Medical WasteStandard:
Medical waste is disposed of in a functional pit (e.g. not accessible to children and animals) within the compound
15
Stories of success…
Improved drug storage at RHCImproved drug storage at RHC
16
Quality -
Services and Systems
Policy &
Infrastructure
Performance Monitoring &
macro management
Operations & Governance
Health Services Provision:
Professional accountability and patient satisfaction
National
National &
regional
Institutional
Individual
17
Quality is Everyone’s
Responsibility
• Capacity and commitment are needed
at all levels, starting at the top
• Everyone must know how they
contribute to quality
• Standards give staff guidance –
training gives them confidence and
competence
• The Quality Management Course
being planned is what all countries
want and need
18
A Quality Culture exists in
Aviation
19
Does a Quality Culture exist here?

40 Quality of Care in Health Sector
20
“No quality management system works unless people are empowered and committed to take responsibility for quality
-as an ongoing process –
in the end, quality becomes part of people's behaviour and attitudes”
21

41Quality of Care in Health Sector
Annexure 4
Quality Assurance Programmes
(QAP) in West Bengal
Dr Aniruddha Mukherjee
Technical Officer, Strategic Planning
& Sector Reforms Cell
Govt. of West Bengal
Types of Quality Assurance Initiatives
• At the primary health care level (Pilot in
Hooghly)
▫ Focus on RCH
▫ Types of facilities covered: Rural Hospitals (CHC),
BPHCs, PHCs, Sub Centres
• At the secondary hospital level (Pilot in 2
District Hospitals & 1 Sub Divisional Hospital)
▫ Focus on all case management activities
▫ Types of facilities to be covered: District Hospitals,
Sub divisional Hospitals, State General Hospitals
• Both initiatives facilitated by GTZ
QAP on
RCH II in
Hooghly
The beginningThe beginning
M & E Division of the MoHFW, GOI, M & E Division of the MoHFW, GOI,
decides to introduce QAP in RCHIIdecides to introduce QAP in RCHII
Develops Operational Manual from Develops Operational Manual from
field experience of UNFPAfield experience of UNFPA
Decides on piloting in seven districts Decides on piloting in seven districts
of six statesof six states
GTZ supports in Assam and West GTZ supports in Assam and West
BengalBengal
PATH as field partnerPATH as field partner
Action taken from the Action taken from the DoH&FWDoH&FW,, GovtGovt of West Bengalof West BengalParticipated in the Launching of the Participated in the Launching of the
Programme at the National Level onProgramme at the National Level on
21.12.0621.12.06
Signed MoU with the National Signed MoU with the National
Government 22.01.07Government 22.01.07
Constituted a State Working Group Constituted a State Working Group
on Quality Assurance Programme in on Quality Assurance Programme in
March 2007March 2007
Identification and notification of Identification and notification of
State Nodal OfficerState Nodal Officer
Action Taken at District LevelAction Taken at District LevelFormation of District Quality Assurance Group Formation of District Quality Assurance Group
and identification of District Nodal Officer.and identification of District Nodal Officer.
Training of DQAG (7th to 10th May 2007) and Training of DQAG (7th to 10th May 2007) and
constitution of DQA Teamconstitution of DQA Team
–– DQAG membersDQAG members--2020
–– Team membersTeam members--1212
Training of Facility Managers on 14th & 15th Training of Facility Managers on 14th & 15th
May 2007May 2007
No. of Institutions included during the pilot:No. of Institutions included during the pilot:
–– RH 8(100%)RH 8(100%)
–– BPHC 9 (100%)BPHC 9 (100%)
–– PHC 21 (33%)PHC 21 (33%)
–– S.C. 66 (10%)S.C. 66 (10%)
First round of visits completed by December First round of visits completed by December
2007, 22007, 2ndnd
round during Feb to May 2008round during Feb to May 2008
Presentation by Dr. Aniruddh Mukerjee, West Bengal

42 Quality of Care in Health Sector
QAP ProcessQAP Process
DQAG TeamDQAG Team
Facility visit by QA Teams
Facility wise checklists filled up on input,
process and patient satisfaction
Facilities graded, problems and solutions
identified
Timeline on action plans prepared for local,
district and state.
Follow up after six months
QAP Process QAP Process –– District levelDistrict level–– Compilation, analysis, discussion and follow up Compilation, analysis, discussion and follow up
actionaction
–– Coordinate the visits to ensure adherence to Coordinate the visits to ensure adherence to
scheduleschedule
–– Review visit reports and compilation reportsReview visit reports and compilation reports
–– Ensure technical quality of assessmentsEnsure technical quality of assessments
–– Take up issues from the action plans that require Take up issues from the action plans that require
action at the district level and facilitate them with action at the district level and facilitate them with
CMOH officeCMOH office
–– Take up issues from the action plans that require Take up issues from the action plans that require
action at the State level with relevant authorities action at the State level with relevant authorities
in the Departmentin the Department
–– Ensure regularity and participation of DQAG review Ensure regularity and participation of DQAG review
meetingsmeetings
–– Network with other stakeholders such as general Network with other stakeholders such as general
administration for necessary supportadministration for necessary support
QAP Process State levelQAP Process State level
Provide technical supportProvide technical support
Visit selected facilities to ensure Visit selected facilities to ensure
standardization of assessmentstandardization of assessment
Provide administrative and managerial Provide administrative and managerial
support to overcome bottleneckssupport to overcome bottlenecks
Participate in review meetings at Participate in review meetings at
district leveldistrict level
Organize state level review meetingsOrganize state level review meetings
Assist in institutionalization of the Assist in institutionalization of the
process to facilitate process to facilitate scaleupscaleup
Oversight of the whole process to Oversight of the whole process to
ensure that the pilot yields expected ensure that the pilot yields expected
resultsresults
Role of GTZ and PATHRole of GTZ and PATH
1.1. Training of Nodal Officers: District Training of Nodal Officers: District
and Stateand State
2.2. Training of DQAG and Facility Training of DQAG and Facility
HeadsHeads
3.3. Identify bottlenecks and inform Identify bottlenecks and inform
district and statedistrict and state
4.4. Process documentationProcess documentation
5.5. Contribute to standardization of Contribute to standardization of
the assessment the assessment
6.6. Support the Department to Support the Department to
institutionalize the initiativeinstitutionalize the initiative
OutputOutputFacilities visited against plannedFacilities visited against planned
Month Visits planned Visits made
May 07 12 10
June 07 14 10
July 07 16 16
August 07 24 22
September 07 20 17
October 07 9 12
November 07 8 17
103 104
No of facilities visited and their categorization No of facilities visited and their categorization
during first six monthsduring first six months
Type of facility No Category
RH 8 A 5(62 %), B 2(25%), C 1 (12%), D 0
BPHC 9 A 0, B 6 (66%), C 3 (33%), D 0
PHC 22 A 2 (9%), B 8 (36%), C 11 (50%), D 1 (4%)
SC 66 A 37 (56%), B 29 (43%), C 0 , D 0

43Quality of Care in Health Sector
Action points identified at Action points identified at different levelsdifferent levels
LocalLocal
Provision for clinic space (excepting GPHQ/
Govt Building)
Signage: Services/micro plan
Logistics for examination of Blood/Urine
Utilization of fund untied /JSY
Hands on training on IUD, RTI/STI
Management of sharps
Physical facilities for clients
SubCentre
BPHC/RHBPHC/RH
Supply and orientation on SOPsSupply and orientation on SOPs
Utilization of RKS fund to maintain servicesUtilization of RKS fund to maintain services
Utilization of JSY fund to popularizeUtilization of JSY fund to popularize
institutional deliveryinstitutional delivery
Inform district on requirement of trainingInform district on requirement of training
Put up signage on available servicesPut up signage on available services
Improvement of physical facilities for clientImprovement of physical facilities for client
Supply of equipment and medicineSupply of equipment and medicine
IntersectoralIntersectoral coordination (PRI/ Block coordination (PRI/ Block
HealthHealth SamitiSamiti))
Improving Bio Medical Waste Management Improving Bio Medical Waste Management
and Infection Control Practicesand Infection Control Practices
DistrictDistrict
Identification of training needs and Identification of training needs and organisingorganising
training programmestraining programmes
Inclusion of QAP during District Inclusion of QAP during District SamitiSamiti meetingsmeetings
along with sensitization of RKS and PRI during along with sensitization of RKS and PRI during
interinter--sectoralsectoral meetingsmeetings
Ensuring regular flow of RKS/JSY/ untied fundsEnsuring regular flow of RKS/JSY/ untied funds
Improving physical facilities at peripheral unitsImproving physical facilities at peripheral units
Ensuring regular supply of equipment, Ensuring regular supply of equipment,
contraceptives and medicinescontraceptives and medicines
Improved monitoring and supervision with Improved monitoring and supervision with
compilation and sharing of assessment reportscompilation and sharing of assessment reports
Improving BioImproving Bio--Medical Waste ManagementMedical Waste Management
Regular feed back to the stateRegular feed back to the state
StateStateTraining of different health staff onTraining of different health staff on
priority basispriority basis
Allocation of budget for QAPAllocation of budget for QAP
Increased supervision and Increased supervision and
monitoringmonitoring
Regular state level meeting on QAPRegular state level meeting on QAP
Finalization of BMWM strategy and Finalization of BMWM strategy and
implementationimplementation
Providing for infrastructure Providing for infrastructure
developmentdevelopment
Filling up of vacanciesFilling up of vacancies
Bottle necks IdentifiedBottle necks IdentifiedInitial assessments weak, with experience Initial assessments weak, with experience
assessments maturedassessments matured
More intensive monitoring required from More intensive monitoring required from
both state & district levelsboth state & district levels
Essential vacancies of Medical Officers, Essential vacancies of Medical Officers,
Nursing Staff and Nursing Staff and ANMsANMs need to be filledneed to be filled
Some facilities, Some facilities, espesp PHCsPHCs, require extensive , require extensive
infrastructure improvementinfrastructure improvement
QAP could be done in only Govt. owned QAP could be done in only Govt. owned
facilities, majority of facilities, majority of SCsSCs remain outside remain outside
the ambitthe ambit
Action plan implementation weakAction plan implementation weak
Hooghly Facility grading SCHooghly Facility grading SC
Hooghly District: Gradation of Sub-Centres (N=66)
Grade A56%
Grade B42%
Grade C2%
Grade A Grade B Grade C
Categorisation 2nd Assessment visits
Grade A59%
Grade B38%
Grade C3%
44 Quality of Care in Health Sector
Hooghly Facility grading PHCHooghly Facility grading PHC
Hooghly District: Gradation of PHCs (N=22)
Grade A9%
Grade D5%
Grade B36%Grade C
50%
Grade A Grade B Grade C Grade D
Categorisation 2nd Assessment visit
Grade B45%
Grade C50%
Grade D5%
Hooghly Facility grading BPHCHooghly Facility grading BPHC
Hooghly District: Gradation of BPHCs (N=9)
Grade B67%
Grade C33%
Categorisation 2nd Assessment visit
Grade A11%
Grade B78%
Grade C11%
Hooghly Facility grading RHHooghly Facility grading RH
Hoogly District: Gradation of Rural Hospitals (N=8)
Grade B25%
Grade A62%
Grade C13%
Categorisation 2nd Assessment visit
Grade A49%Grade B
38%
Grade C13%
2 Assessment visits Feb to Aprssess e s s eb o p0808
Chart showing the changes during the two assessments
13
2 7
5
615 49
20 3 5
0%
10%20%
30%40%
50%
60%70%
80%90%
100%
RH BPHC PHC SC
Type of Institutions
% C
han
ges Deteriorated
Same
Improved
Did the QAP have an impact? A Case Did the QAP have an impact? A Case Study March to April 08 1Study March to April 08 1
ObjectivesObjectives
––To find out the appropriate changes at facility To find out the appropriate changes at facility
level that have occurred as an effect of QAPlevel that have occurred as an effect of QAP
––To find out the immediate consequences of To find out the immediate consequences of
changeschanges
––To share the findings for making appropriate To share the findings for making appropriate
future plans for scaling upfuture plans for scaling up
Facility selectionFacility selection
––5 sub centres, 1 PHC, 1 BPHC and 1 RH5 sub centres, 1 PHC, 1 BPHC and 1 RH
Tools and MethodologyTools and Methodology
––Primary Data interviews with staff, clients & Primary Data interviews with staff, clients &
PRI members, observation of work practicesPRI members, observation of work practices
––Secondary data DQAG forms and reports, Secondary data DQAG forms and reports,
facility reportsfacility reports
Findings QAP Impact Assessment Study.. 1Findings QAP Impact Assessment Study.. 1
Access to servicesAccess to services
––Increased antenatal Increased antenatal
estimation of estimation of
haemoglobinhaemoglobin
((Panisheola and Kharial
SC) with concomitant with concomitant
increase in increase in
consumption of IFAconsumption of IFA
––Display of timings Display of timings
have empowered have empowered
clients to demand clients to demand
services to be services to be
delivered on timedelivered on time
Speaking Walls Kanaipur BPHC
45Quality of Care in Health Sector
Findings QAP Impact Assessment Study..2Findings QAP Impact Assessment Study..2Equipment and SuppliesEquipment and Supplies
––All facilities have an emergency trayAll facilities have an emergency tray
––All basic equipment like thermometers, All basic equipment like thermometers,
stethoscopes, BP apparatus, covered tray, stethoscopes, BP apparatus, covered tray,
fetoscopesfetoscopes andand haemoglobinometerhaemoglobinometer
available and functioningavailable and functioning
––Sterilisation equipment in all BPHCs and Sterilisation equipment in all BPHCs and
RH validated regularly during useRH validated regularly during use
––Better housekeepingBetter housekeeping
––RKS and untied funds utilisation more RKS and untied funds utilisation more
oriented towards service deliveryoriented towards service delivery
Findings QAP Impact Assessment StudyFindings QAP Impact Assessment Study……33Professional Standards and Technical CompetenceProfessional Standards and Technical Competence
–– Overall improvement due to availability of SOPs, guidelines Overall improvement due to availability of SOPs, guidelines
and manuals and technical discussions with DQAG membersand manuals and technical discussions with DQAG members
–– AllAll ANMsANMs had detailed knowledge of ECP, OCP, Kangaroo had detailed knowledge of ECP, OCP, Kangaroo
technique, IUDtechnique, IUD
–– Technical CME integral part of meetingsTechnical CME integral part of meetings
–– Doubt clearance and Doubt clearance and ‘‘reasons behindreasons behind’’ activities part of DQAG activities part of DQAG
themesthemes
–– Activities are more organised due to improved house keepingActivities are more organised due to improved house keeping
Findings QAP Impact Assessment StudyFindings QAP Impact Assessment Study……44
Physical InfrastructurePhysical Infrastructure
––Improvement of functional toilet facilities Improvement of functional toilet facilities
((Panisheola SC, Purba Thakurani Chowk SC)
, repair & up keep. The direct benefits are, repair & up keep. The direct benefits are
Collection of urine for testing, IUD insertions Collection of urine for testing, IUD insertions
easier, staff & clients remain for longer timeseasier, staff & clients remain for longer times
––ImprovedImproved signagessignages
––Privacy for patients is consciously ensuredPrivacy for patients is consciously ensured
––Needle cutters being used in all facilitiesNeedle cutters being used in all facilities
––Essential repairs identified and carried out Essential repairs identified and carried out
broken panes replacedbroken panes replaced
––Lighting improvedLighting improved
Some PhotographsSome Photographs-- Sub CentresSub Centres
Kharial Sub Centre
Panisheola SC
Balibela SC
Bhadur SC
Some PhotographsSome Photographs-- RHsRHs &BPHC&BPHC
Kanaipur BPHC
PA System Singur RH Haripal RH
Kanaipur BPHC
Findings QAP Impact Assessment StudyFindings QAP Impact Assessment Study…….5.5
Continuity of CareContinuity of Care
–– RKS and untied funds expenditure provides RKS and untied funds expenditure provides
assistance to keep services undisruptedassistance to keep services undisrupted
Service EnvironmentService Environment
–– Uninterrupted availability of equipment and Uninterrupted availability of equipment and
materialsmaterials
–– Better housekeeping each equipment in its own Better housekeeping each equipment in its own
placeplace
–– Functional toiletsFunctional toilets
–– Validated sterilisation facilities during sterilisation of Validated sterilisation facilities during sterilisation of
equipmentequipment
–– Use of glovesUse of gloves
–– Better ambienceBetter ambience
–– Privacy issues being looked intoPrivacy issues being looked into
46 Quality of Care in Health Sector
Findings QAP Impact Assessment StudyFindings QAP Impact Assessment Study……66
Informed Decision MakingInformed Decision Making
––More knowledgeable staff more More knowledgeable staff more
confident in giving informationconfident in giving information
––‘‘One windowOne window’’ counselling provides better counselling provides better
information, saves timeinformation, saves time
––More choices for contraceptive services More choices for contraceptive services
actually availableactually available
––Better relevant communication at Better relevant communication at
service deliveryservice delivery
Summing UpSumming UpProcesses of ANC check up improvedProcesses of ANC check up improved
Knowledge level improved with regards to IUD, New Knowledge level improved with regards to IUD, New
Born Care and Family PlanningBorn Care and Family Planning
Improved housekeepingImproved housekeeping
Improved infection control & waste managementImproved infection control & waste management
Improvement in record maintenanceImprovement in record maintenance
SOP material used for reference wherever it is SOP material used for reference wherever it is
availableavailable
Conscious hygiene maintenanceConscious hygiene maintenance
PRI aware on expenditure of untied funds for quality PRI aware on expenditure of untied funds for quality
improvementimprovement
Improvement in supply of equipments and material Improvement in supply of equipments and material
and its maintenanceand its maintenance
Signage and Charters in placeSignage and Charters in place
Emphasis on follow up of plans e.g. ToiletsEmphasis on follow up of plans e.g. Toilets
A tool for monitoring visits by supervisory officers. A tool for monitoring visits by supervisory officers.
West Bengal Hospital Standards ver 1
• West Bengal Hospital Standards
▫ 37 Standard Elements
▫ Sub divided into 4 sections
� Hospital Management- 6 Standard Elements
� Clinical Services- 19 Standard Elements
� Support Services- 5 Standard Elements
� Cross Departmental Issues- 7 Standard Elements
• Support Documents
▫ Technical Document- Elaborating the
requirements of the Standard Elements
▫ Checklists for 11 Quality Circles
The Break up of the Check lists
QualityCircle
Document
Equipment
Personel
Infrastructure
Policies
Practice
Signage
Training Total
MATERNITY 68 23 12 20 38 101 28 23 313
SURGERY 57 58 9 17 33 118 27 20 339
MEDICINE 33 17 3 7 23 66 27 12 188
NURSING 81 40 10 31 24 113 12 43 354
OPD 15 25 6 31 28 74 23 4 206
• DoHFW decided to introduce QAP in secondary hospitals as
part of HSDI
• State Working Group set up in March 2007 to formulate the
QAP process
• QAP state level workshop held in June 2007 followed by
fortnightly brain storming sessions
• Review of different international and national standards, QA
processes done
• Resource persons sent for international and national
exposures on QA methodologies
• West Bengal Hospital Standards (draft) developed and
presented to Department in Feb 08
• Integrated as activity of Planning & Development Branch
QAP in Secondary Level Hospitals
Challenges with selling the Idea
• Why speaking of quality in Govt. healthcare?
• Quantity vs Quality
• Overburdening of Staff
• Expensive
• Admission of “Not Quality Services Provided
Now”
• Will it be sustainable
• The modifications made- were they
compromises?
47Quality of Care in Health Sector
The QAP Process…….. 1
• Sensitisation of key stake holders in hospitals
(Off site)- Introduction to QA Programme
▫ Superintendent
▫ Nursing Superintendent
▫ Non Doctor Administrator- Asst Superintendent/
Ward Master
• Sensitisation of key stake holders from all
functional areas (On site)- Introduction to QAP
and Self Assessments
▫ Doctors & Pharmacists
▫ Nursing Supervisors
▫ Technicians- Diagnostics, Imaging, Physiotherapy
▫ Office Staff and Store Keepers
The QAP Process ………… 2
• Formation of Quality Circles (QC) - 3 members each:
1 doctor, 1 nursing staff and 1 technical person
▫ OPD, Casualty & Minor OT
▫ Surgical & Allied Departments like Eye, ENT
▫ Medicine & Allied Departments like Paediatrics
▫ Maternity and Allied Departments like Neonatology
▫ Nursing Services- 2 Quality Circles
▫ Diagnostic Services including Lab and Imaging
▫ Safety, Infection Control and Waste Management
▫ Facility Management andProcurement
▫ Records
▫ Contract Management
The QAP Process ………… 3
• Sensitisation of Convenors of QCs (on site)- Use of
checklists for self assessments and preparation of
action plans and identification of areas of
improvement for next 3 months
• Documentation of Baseline indicators for
improvement
• Training of Convenors of QCs on simple quality
tools like cause & effect diagrams, Pareto Charts,
work flow analysis, spaghetti diagrams to detect
problems and work out probable solutions
• Training of Hospital staff on Infection Control,
Waste Management, Safety, Disaster Management
and Fire Safety
The QAP Process ………… 4
• Assessment of Action Plan by QA Group and
improvement strategies discussed
• Annual Action Plan formulated
• Repeat self Assessment after 9 months of 1st
Self
Assessment
• Peer Assessment
• Accreditation/ Certification
The Present Status
• Pilot in 3 Hospitals- all with > 90% bed occupancy
▫ 1 District Hospital with QA Working Group member
▫ 1 District Hospital with no QA experience
▫ 1 Sub Divisional Hospital
• Sensitisation Meeting for key stake holders done
in April 2008
• QC formed in May 2008, sensitisation of self
assessment done
• Action plans for next 3 months and determination
of baseline indicators in progress
• Assessment of 1st
phase implementation in Sept 08
• 2nd
Assessment by Dec 08
• Scale up decision- July 2008
The Learning
• Keep on harping that QAP is not being enforced from the
top- make it part of the system
• Identify champions in the system and utilise them in
initial period. After some time QA becomes infectious
• Overcome initial scepticism with intense hand holding-
authorities at higher levels should show personal
involvement
• Keep focus on documentation- only policies and SOPs
that get written get practiced
• Keep documents simple- no document should cover
more than 1 side of an A4 paper in 10 size font
• Address training needs of all staff- keep them short,
simple & focussed to needs

48 Quality of Care in Health Sector
The Learnings ………… 2
• Develop a monitoring and evaluation plan right
from the beginning
• Develop measurable indicators for monitoring
• Be patient- the start of the programme requires all
to put in extra effort. Hurrying up may be counter
productive. However, ask the facilities to prepare
their timelines and monitor that they are being
stuck to
• Facilitation should be on site as far as practicable
• Ensure physical comfort in all activities
• Scale up with caution, QA requires intense hand-
holding
Thank You
49Quality of Care in Health Sector
Annexure 5
Secondary Level Hospital Quality Improvement & Management – State Experiences
Dr Preeti KudesiaSenior Public Health SpecialistHealth, Nutrition & Population The World Bank
June 4 - 7, 2008NIHFW-WBI, Shimla Workshop
Overview of Bank support to Health Sector in India
HIV/AIDS III (ongoing)TB II (ongoing) VBDC (under preparation)Leprosy (2001-04)Cataract Blindness(1994-2002)
� F & D control
� Disease surveillance
� Andhra Pradesh-secondary and primary
� Karnataka (KHSDP completed; KHSDRP ongoing)
� Punjab
� West Bengal
� Orissa
� Maharashtra
� Uttar Pradesh (ongoing)
� Uttarakhand (ongoing)
� Rajasthan (ongoing)
� Tamil Nadu (ongoing)
RCH II (ongoing) RCH I (1997-2001)IPPs I-IX (1980-95)Nutrition (1980-06)
Cross-CuttingPrograms
State Health Systems Strengthening Program
Central Programs
Objectives and interventions of State Health Systems Projects
Since 1996– State Health Systems Projects providing interventions at District Hospital and Sub-district level (secondary level of health care) with broad objectives to:� Improve efficiency and quality of services� Enhance access to and ensure equitable
services for disadvantaged populations
Quality Improvement Aspects
� Rationalization of service norms –infrastructure, equipment, manpower
� Monitoring and Performance evaluation� Housekeeping/ ‘hotel’ functions� Behavior change of service providers� Quality enhancement of processes� Certification & Accreditation
Rationalization of service norms
A four pronged approach
� Services provided: Services (including manpower) to be provided at each level - Rajasthan Health Systems Development Project
� Equipment requirements: Equipment norms - Tamil Nadu Health Systems Project
� Drugs and supplies: Essential drug list - Rajasthan State Health Systems Project
It was agreed with the state governments that these norms will be met by adopting various strategies, eg: procurement, repair, contractual recruitment of staff
Manpower Norms
� Norms developed for each state for each level of facility� Placement/Recruitment to fulfill norms� Retention of staff� Motivation of staff
� Skill up-gradation and training
� Doctors: skill upgradation, equipment and procedure based training
� Nurses training: AP,Punjab, Rajasthan
� Technicians: RHSDP - general training by CSIO/ equipment based training from manufacturers at time of delivery
Presentation by Dr. Preeti Kudesia
50 Quality of Care in Health Sector
Manpower norms: A case study of CEmONCs from Tamil Nadu
The critical issue of manpower was put on high priority by GoTN to enable Govt. hospitals (FRU’s) to function as Comprehensive Emergency Obstetric & Neonatal Centers (CEmONCs).
� A GIS mapping of CEmONCs was done and a sample of 83 were selected to ensure access within one hour of travel (subsequently 30 minutes of travel)
� An in-depth analysis of existing and required manpower for CEmONCs was done based on established norms
� Specialists posted in peripheral and primary level positions where their skills were not being utilized were identified and relocated
� Shortfall in specialist services post relocation was calculated and doctor and nursing staff was recruited on contractual basis
� Remuneration of specialists raised by 150%� 41 CEmONCs have been assessed based on a set of parameters
and certified as fully functional CEmONCs.
Equipment Requirement, Repair and Maintenance
� Inventories developed of existing equipment� Equipment that was fully functional� Equipment that needed repairs and maintenance� Equipment that needed to be condemned
� Decisions taken regarding equipment maintenance: Rajasthan—An options paper prepared for most effective equipment management and repair system for the state
� One-time repair of all faulty equipment � New equipment purchased according to the norms developed for each level of
facility
Challenge: Setting up sustainable system for equipment maintenanceBudgetary allocation for equipment maintenance
Innovation: Karanataka: Six Centers streamlined processes and to obtain ISO Certification for Equipment Repair and Maintenance Centers.
Housekeeping & ‘Hotel’ Functions
An important function raised in most patient satisfaction surveys
� Cleaning� Laundry� Diet� Security
Lessons Learnt� Outsourcing through PPPs� Model contract development� Contract management� Supervision� Government commitment to resources (Experience from KHSDP:
financially more viable to contract out housekeeping/hotel functions)
Free services to disadvantaged populations
Barriers to seeking healthcare from government services
Lack of� Information Access: Campaigns (VCD, IEC, Counselors)
� Physical Access: Renovation/Up-gradation, emergency transport services, outreach camps
� Social Access: Targeted approach to BPL, SC, ST populations� Financial Access: User fees exempt, free drugs and diagnostics for
poor (RMRS from RHSDP)
Drug supplies
� Drug logistics� Inventory� Supply chain management
Tamil Nadu Medical Services Corporation (TNMSC)
Monitoring & Performance Evaluation
� Hospital Information Systems
� Hospital activity indicators and performance indicators: Indicators from Rajasthan Health Systems Development Project� Maharashtra Health Systems Project—performance indicators and external
validation of data
� West Bengal State Health Systems Development Project – Quality Assurance and grading of hospitals with data from all levels of facilities
� Andhra Pradesh Health Systems Project– Grading up to PHC level� Punjab Health Systems Project – Use of data for management purposes
� Quality indicators� Benchmarking� Grading/rating
51Quality of Care in Health Sector
Behavior Change of Service Providers
Attitude of service providers a major barrier for populations toaccess healthcare at government facilities
Training for 3 cadres of service providers (doctors, nurses/technicians, class IV) to
� Improve client orientation, service behavior and communication skills so as to improve quality of service delivery
� Increase sense of team spirit amongst service providers� Increase sense of organizational belonging and ownership among providers
Strategies: Training of BCC trainers: Tamil Nadu Health Systems Project Facility-wise training and TOT: Rajasthan Health Systems ProjectFacility-wise training: Uttaranchal Health Systems Project
An overview to mechanism of stimulating Behavior Change amongst service providersThe Maharashtra Example
Quality Enhancement of Processes
� Drug inventory and Rational Use of Drugs
� Standard Treatment Protocols/Guidelines
� Guidelines for action in emergency, OT, Labor room, OPD
� Equipment Maintenance
� Audits (case sheets, death reviews, prescription audits)
� Patient Flow Management (time spent at different sites, overcrowding)
� Hospital timings and rationalization of duty hours
� Healthcare Waste Management
Hospital Systems Improvement Teams
To improve the quality of health care offered at all health carefacilities and health systems performance through
� A continuous internal process of problem identification
� Solution finding
� Implementation of best solutions and
� Working with staff, funds, information, supplies, transport, communications, management etc in an integrated manner
The HSIT process
HSIT: An innovative pilot initiative in Rajasthan Health Systems Development Project to stimulate quality improvement at each facility level with complete ownership of all cadres of service providers
Quality is never an accident; it is always the result of high Quality is never an accident; it is always the result of high intentions, sincere effort, intelligent direction and skilful exintentions, sincere effort, intelligent direction and skilful executionecution
Thank you!
52 Quality of Care in Health Sector
Annexure 6
Quality Management Initiatives in Himachal Pradesh
Dr. Monika KrengelShimla, June 2008
HSSHP - Programme Setup
Jan 2000 – Dec 2007, 3 Phases• Basic Health Project Himachal Pradesh (BHPHP) – until
2004• From 2004 onwards integration into the GTZ Indo-
German Health Programme (IGHPHP), Delhi, in 2005 changed into GTZ Health Sector Support (HSSHP)
• Cooperation with two other GTZ projects: West Bengal and Maharashtra.
• Only the HP project focussed on secondary healthcare support, following a request of the HP health department
Enabling Environment for Introducing QM in 2002
1. Himachal Health Vision 2020 envisions Continuous Quality Improvement
2. Sectoral reforms in the Health Sector with focus on Decentralisation and Hospital Autonomy
3. Creation of Hospital Welfare Societies and introduction of User Charges in Himachal (2002)
4. Decision of the Department to strengthen Secondary Health Care and to use Quality Management for Service Improvement
General Problems
• Accessibility – poor road connectivity• Availability of health services - very few private health
facilities• Limited range of services and shortage of specialists• High spending by patients on travel and medicines (over
prescription)• Absence of planning and innovations, shortage of
adequate equipment and infrastructure, low level of maintenance, etc.
• Strong centralisation and little decision making powers of hospitals – shortage of budged
Goals and Objectives of HSSHP
• Decentralised health systems are supported– Establishment of Hospital Societies – 2000-2003– Strategic Planning Workshops – 2001-2005– Leading to the introduction of Quality Management in
2002• Health Management Information System (HMIS) is strengthened
– 2001-2007• Community involvement in health is increased – 2001-2005• Human Resource Development Systems and Strategy initiated• Asset/Material Management Systems are demonstrated
– Rational Use of Drugs (RUD) – 2001-2005– Biomedical Waste Management (BMWM) – 2003–2006– Repair and Maintenance of Equipment – 2001-2006
Objectives and ActivitiesMain Areas of Activities
Quality Management 2002-2007;143 Workshops, 2855 participants
Health Management InformationSystem(HMIS)2001-2007, 82Workshops, 2018 participants
Rational Use of Drugs(RUD) 2001-2005, 68 Workshops, 1310participants
Community Involvement in Health2001-2005; 66 Workshops; 1633participants
Strategic Planning 2001-2005; 61Workshops; 1060 participants
Repair and Maintenance ofEquipment 2001-2004; 20Workshops; 215 participants
Biomedical Waste Management(BMWM) 2003-2005; 13Workshops; 339 participants
Presentation “Quality Management Initiative in Hospital Management in Himachal Pradesh”
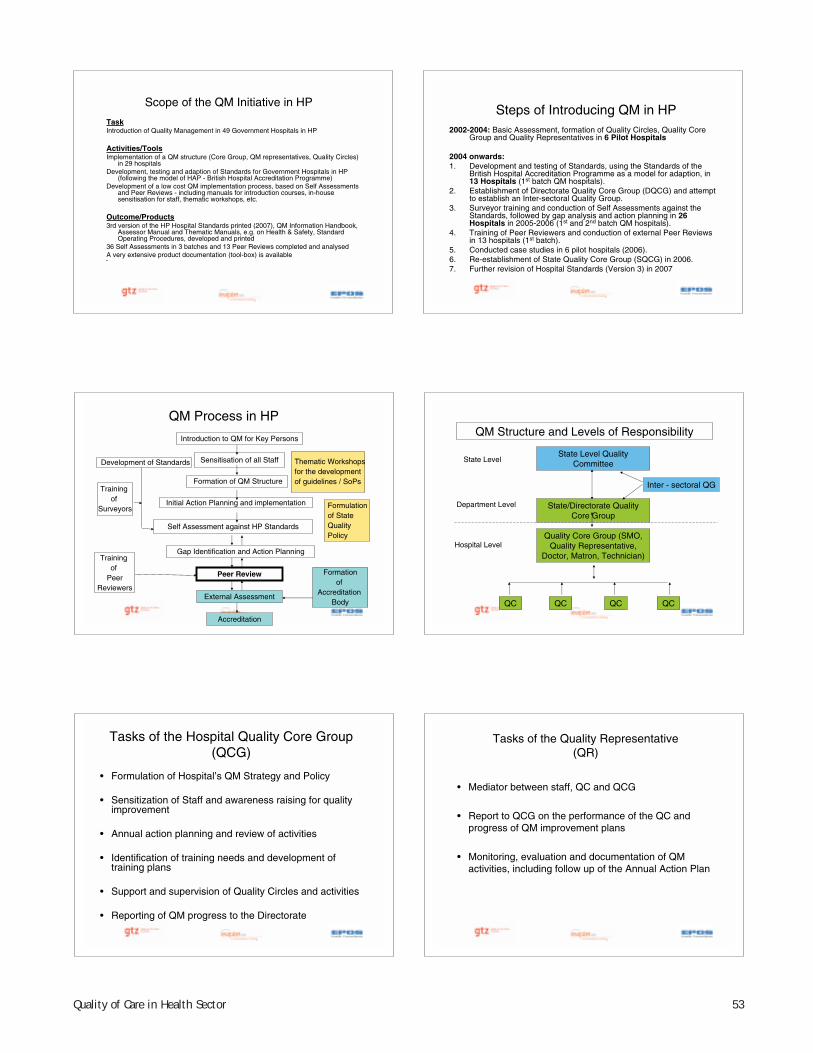
53Quality of Care in Health Sector
Scope of the QM Initiative in HP
TaskIntroduction of Quality Management in 49 Government Hospitals in HP
Activities/ToolsImplementation of a QM structure (Core Group, QM representatives, Quality Circles)
in 29 hospitalsDevelopment, testing and adaption of Standards for Government Hospitals in HP
(following the model of HAP - British Hospital Accreditation Programme)Development of a low cost QM implementation process, based on Self Assessments
and Peer Reviews - including manuals for introduction courses, in-house sensitisation for staff, thematic workshops, etc.
Outcome/Products3rd version of the HP Hospital Standards printed (2007), QM Information Handbook,
Assessor Manual and Thematic Manuals, e.g. on Health & Safety, Standard Operating Procedures, developed and printed
36 Self Assessments in 3 batches and 13 Peer Reviews completed and analysedA very extensive product documentation (tool-box) is available•
Steps of Introducing QM in HP2002-2004: Basic Assessment, formation of Quality Circles, Quality Core
Group and Quality Representatives in 6 Pilot Hospitals
2004 onwards:1. Development and testing of Standards, using the Standards of the
British Hospital Accreditation Programme as a model for adaption, in 13 Hospitals (1st batch QM hospitals).
2. Establishment of Directorate Quality Core Group (DQCG) and attempt to establish an Inter-sectoral Quality Group.
3. Surveyor training and conduction of Self Assessments against theStandards, followed by gap analysis and action planning in 26Hospitals in 2005-2006 (1st and 2nd batch QM hospitals).
4. Training of Peer Reviewers and conduction of external Peer Reviews in 13 hospitals (1st batch).
5. Conducted case studies in 6 pilot hospitals (2006). 6. Re-establishment of State Quality Core Group (SQCG) in 2006.7. Further revision of Hospital Standards (Version 3) in 2007
QM Process in HP
Sensitisation of all Staff
Formation of QM Structure
Self Assessment against HP Standards
Gap Identification and Action Planning
Peer Review
Accreditation
Development of Standards
Trainingof
Surveyors
External Assessment
Trainingof
PeerReviewers
Formationof
AccreditationBody
Thematic Workshopsfor the development of guidelines / SoPs
Initial Action Planning and implementation
Introduction to QM for Key Persons
Formulationof State QualityPolicy Quality Core Group (SMO,
Quality Representative, Doctor, Matron, Technician)
QC QC QC QC
State/Directorate Quality Core Group
Department Level
Hospital Level
State Level Quality CommitteeState Level
Inter - sectoral QG
QM Structure and Levels of Responsibility
Tasks of the Hospital Quality Core Group (QCG)
• Formulation of Hospital’s QM Strategy and Policy
• Sensitization of Staff and awareness raising for quality improvement
• Annual action planning and review of activities
• Identification of training needs and development of training plans
• Support and supervision of Quality Circles and activities
• Reporting of QM progress to the Directorate
Tasks of the Quality Representative (QR)
• Mediator between staff, QC and QCG
• Report to QCG on the performance of the QC and progress of QM improvement plans
• Monitoring, evaluation and documentation of QM activities, including follow up of the Annual Action Plan
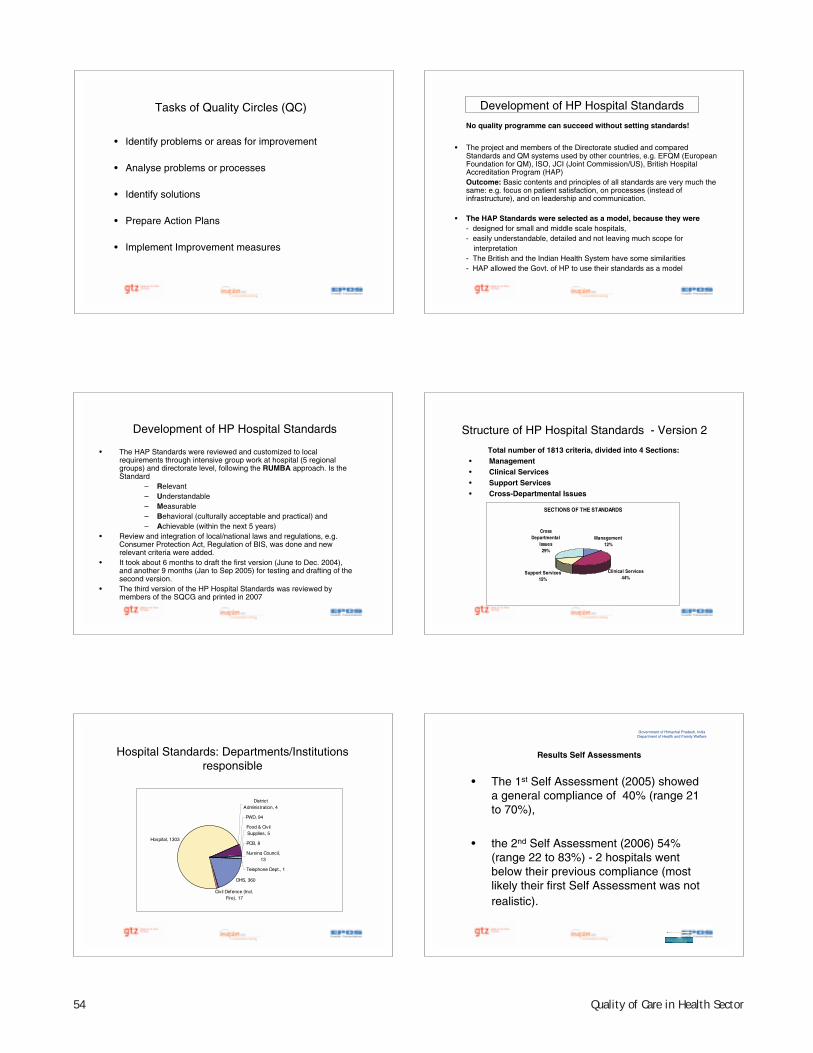
54 Quality of Care in Health Sector
Tasks of Quality Circles (QC)
• Identify problems or areas for improvement
• Analyse problems or processes
• Identify solutions
• Prepare Action Plans
• Implement Improvement measures
No quality programme can succeed without setting standards!
• The project and members of the Directorate studied and compared Standards and QM systems used by other countries, e.g. EFQM (European Foundation for QM), ISO, JCI (Joint Commission/US), British Hospital Accreditation Program (HAP)Outcome: Basic contents and principles of all standards are very much the same: e.g. focus on patient satisfaction, on processes (instead of infrastructure), and on leadership and communication.
• The HAP Standards were selected as a model, because they were- designed for small and middle scale hospitals,- easily understandable, detailed and not leaving much scope for
interpretation- The British and the Indian Health System have some similarities- HAP allowed the Govt. of HP to use their standards as a model
Development of HP Hospital Standards
Hospital Standards: Departments/Institutions responsible
DHS, 360
Civil Defence (Incl. Fire), 17
Hospital, 1303
District Administration, 4
PWD, 94
Food & Civil Supplies, 5
PCB, 8
Nursing Council, 13
Telephone Dept., 1
Results Self Assessments
• The 1st Self Assessment (2005) showed a general compliance of 40% (range 21 to 70%),
• the 2nd Self Assessment (2006) 54% (range 22 to 83%) - 2 hospitals went below their previous compliance (most likely their first Self Assessment was not realistic).
Government of Himachal Pradesh, IndiaDepartment of Health and Family Welfare
Development of HP Hospital Standards
• The HAP Standards were reviewed and customized to local requirements through intensive group work at hospital (5 regional groups) and directorate level, following the RUMBA approach. Is the Standard
– Relevant– Understandable– Measurable– Behavioral (culturally acceptable and practical) and– Achievable (within the next 5 years)
• Review and integration of local/national laws and regulations, e.g. Consumer Protection Act, Regulation of BIS, was done and newrelevant criteria were added.
• It took about 6 months to draft the first version (June to Dec. 2004), and another 9 months (Jan to Sep 2005) for testing and drafting of the second version.
• The third version of the HP Hospital Standards was reviewed by members of the SQCG and printed in 2007
Structure of HP Hospital Standards - Version 2
Total number of 1813 criteria, divided into 4 Sections:• Management• Clinical Services • Support Services • Cross-Departmental Issues
SECTIONS OF THE STANDARDS
Management12%
Clinical Services44%
Support Services15%
Cross Departmental
Issues29%

55Quality of Care in Health Sector
Results Self Assessment
Overall Response
Government of Himachal Pradesh, IndiaDepartment of Health and Family Welfare
Yes55%
?3%
No34%
No Response8%
Results Self Assessments
Comparison of hospital compliance with standards, 2005 and 2006
Government of Himachal Pradesh, IndiaDepartment of Health and Family Welfare
0102030405060708090
100
Una
Cham
ba
Hamirp
ur
Palam
pur
Bilasp
ur
Ghum
arwin
DDUSM
LRoh
ru
Rampu
r
Baijna
thSola
n
Man
di
Sunde
r Nag
ar
2005
2006
Achievements and Lessons Learnt
• Efficient knowledge transfer, through emphasis on– high coverage in reaching professionals; see large
amount of trainings and workshops and successive inclusion of all districts (examples),
– a group of about 20-30 key professionals who actively used concepts and material developed in their environment and developed tools on their own, like in-house training modules for staff, standard operating procedures, draft publications on safety issues, first aid and so on (even starting websites),
– good documentation and dissemination of all trainings, workshops and tools
Challenges
The only challenge is how to achieve sustainability.
Some Achievements and Benefits
• Himachal Pradesh is the first State in India that developed and applied Hospital Standards for the Public Sector, that provide a monitoring tool for performance and improvement.
• Compliance with the Standards is already quite satisfactory (40 % in the first Self Assessment, improved to 53 % in the second Self-Assessment.
• A team approach for problem solving and quality improvement has been initiated in all QM hospitals, through Quality Circles.
• Action planning and monitoring with an emphasis on Quality Improvement takes place for the first time in those hospitals.
• Rationalization of facilities/manpower and improved resource utilization has started.
• Innovative models for local good practices are implemented: e.g.improvement and monitoring of patient satisfaction and communication, medical records, signage, bio-medical waste management, health and safety, repair and maintenance of medical equipment.
• More scope for staff initiative and education and for exchange of best practices.
Achievements and Lessons Learnt
The Quality of healthcare in the QM Hospitals has visibly and measurably improved, following the approach to focus on
– promotion of competition between hospitals and introduction of low-cost incentives and learning through the exchange of best practices,
– easy reachable, visible and mandatory changes, like improvement of sanitation, signage, patient information and safety,
– strengthening of communication skills and means.– Most hospitals accepted QM as an opportunity to strengthen
their position towards the Centre, Court (consumer protection act) and Politicians
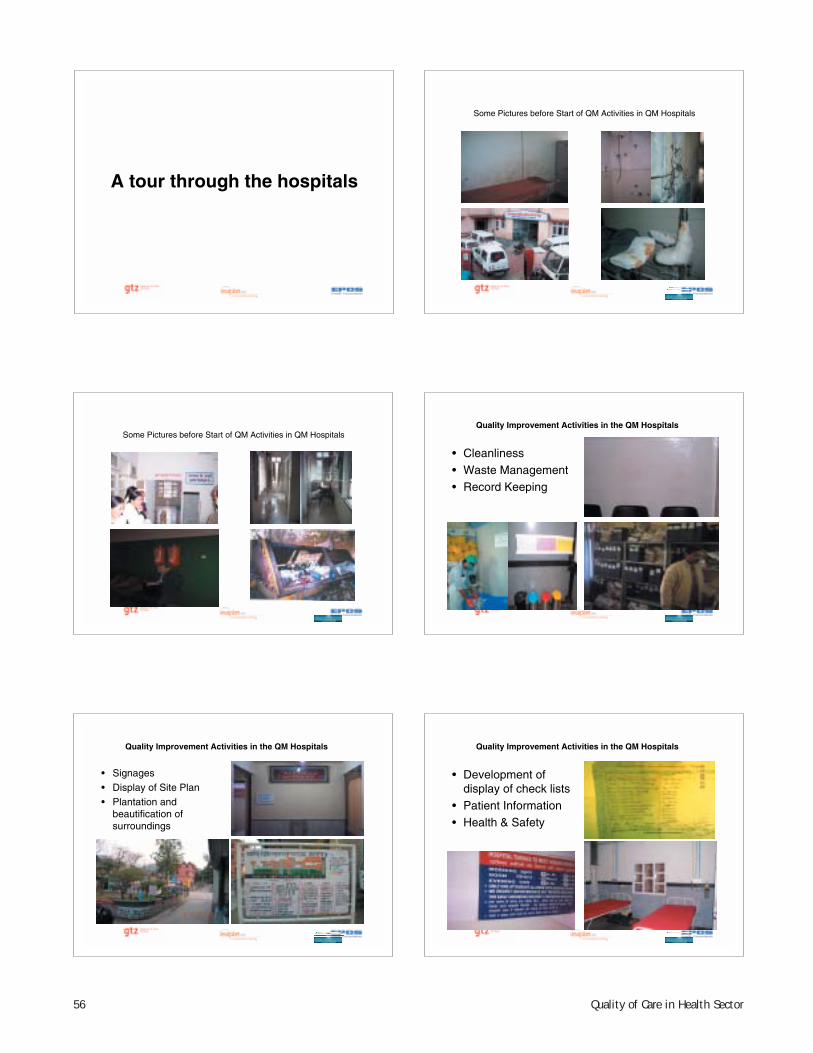
56 Quality of Care in Health Sector
A tour through the hospitals
Some Pictures before Start of QM Activities in QM Hospitals
• Signages• Display of Site Plan• Plantation and
beautification of surroundings
Quality Improvement Activities in the QM Hospitals
Some Pictures before Start of QM Activities in QM Hospitals
• Cleanliness• Waste Management• Record Keeping
Quality Improvement Activities in the QM Hospitals
• Development of display of check lists
• Patient Information• Health & Safety
Quality Improvement Activities in the QM Hospitals
57Quality of Care in Health Sector
Quality Improvement Activities in the QM Hospitals
• Display of hospital vision statement and patient Responsibilities
• Display of Patient Rights • Display of SoPs
Quality Improvement Activities in the QM Hospitals
• Display of Hospital Profile/statistics
• Patient oriented services: Privacy
• Display of organizational chart
Thank You
Quality Improvement Activities in the QM Hospitals
Patient Focused Services:• Information on doctors on duty and
price list of various services/tests• Display and monitoring of
standards for waiting time in OPD, X-ray, Lab
• Newspaper facility for patients
Quality Improvement Activities in the QM Hospitals
• Improved vertical and lateral Communication
• Regular Staff Meetings• Improved ambulance
services
58 Quality of Care in Health Sector
Annexure 7
QUALITY
Quality for me is :-1.Achievement of Standards / Targets fixed 2.Doing the right thing in right way at right time.3.Generating resources.4.Minimizing Conflicts.
STANDARDS OF MY HOSPITAL
• 1. Registration----------15 minutes.
• 2. Examination by Medical Officer---30 minutes
• 3. Lab.Report.----------2 Hrs.
• 4. X-Ray Report--------2 Hrs.
• 5. Treatment to be started to admitted Pt.-Immediately.
ACHIEVEMENT OF STANDARDS
• Employed receptionist from Rogi Kalyan Samiti.Job Responsibilities of Receptionist :-
1. Registration.2. To guide the clients.3. To help the patients who have no attendants.4. To Keep watch on serious patients and to direct such
patients to go directly to emergency management room and to inform the Medical Officer on duty through intercom provided by GTZ.
5. To keep watch on unwanted elements / unwanted events and to inform BMO immediately about it.
EXAMINATION BY MEDICAL OFFICER -30 Minutes
• Provided separate chambers to individual Medical Officers.
• Ensured Punctuality .
• Waiting room provided between OPD 1 & 2 with facilities of water and fan.
LAB. REPORT-2 Hrs.
• Purchased Auto analyzer.
• Employed one attendant for help
X-Ray-Report-2 Hrs.
• Purchased new X-Ray Machine.
• Employed one Helper through RKS.
Presentation by Dr. Raghu, Block Medical Offi cer

59Quality of Care in Health Sector
IDENTIFICATION OF CONFLICT AREAS :-
For Emergency Cases.
1.Non availability of Staff
Immediately :-
Solution :-Night Watch man room near gate
2. Non availability of stretcher / Wheel Chair.
Solution :- Fixed place for stretcher / Wheel Chair
QUALITY CORE GROUP :-
• Block Medical Officer.• Senior Medical Officer.• Chief Pharmacist.• Ward Sister• Meeting held on every last working day of
the month.• Donation box and suggestion box opened
on the same day
QUALITY CIRCLES :-
• 1.Quality Circle OPD :-• SMO In-charge.
• Pharmacist
• Lab. Technician.
• X-Ray Technician
Meeting on every Ist Monday every month at 3.30 PM
Q.C.Contd.
• 2.Quality Circle Indoor :-• Medical officer in-charge indoor.
• Ward Sister.
• Trained Dai.
• Sweeper
Meeting on every I st. Tuesday of the month.
QualityCircles-Contd.
• 3.Quality Circle-Bio Medical Waste :--Medical Officer entrusted the job of Bio Medical Waste.
-All Supervisors-Ward Sister-All Sweepers
Meeting-Every IstWednesday of every month
POLICIES & PROCEDURES
• 1. OUT PATIENT DEPARTMENT :--Reception / Registration—Receptionist to be available here.-Sufficient waiting area with facilities of news desk/drinking
water and fans.-One Doctor made responsible for OPD.-Staff Duty Roster available one month advance.-Patient choice regarding examination by particular Doctor.-Rights and responsibilities of clients clearly written in Hindi
and English.-Privacy Maintained.
60 Quality of Care in Health Sector
OPD POLICIES CONTD.
• Toilet facility available near OPD.
• Waiting room available .
• Wheel Chair / Stretchers available near OPD.
• Facility of separate queues facility for males, females and senior citizens at registration and Pharmacy
POLICIES & PROCEDURES CONTD.
• 2. INDOOR :--Ward Sister is responsible for
looking after the wards.-Next Senior staff nurse given the
responsibility to look after the wards during the absence of ward sister.
-Every new admission provided clean bed sheet.
-Bed Sheets are changed on every third day.
POLICIES & PROCEDURES CONTS--INDOOR
• Each ward has :-Bed Head LightT.V. Facility.News Paper facility.Under bed light facility.Working ClockCalendar of current year.Exhaust fan facility.Changing room facility.Refrigerator facility
MEDICINE BANK :-
• Medicine bank has been established in the hospital . Medicines collected in this bank are given to poor / needy patients.
SUGGESTION BOX:-
• Exit inter view scheme has been started to get the feedback from the clients. Exit interview forms are put at suitable places and the clients are to fill these forms and put into the suggestion box. Suggestion box is opened on the last working day of the month and action taken is conveyed within fortnight.
SPECIMEN OF EXIT INTERVIEW FORM
• 1. Behavior of Doctors……..
• 2. Behavior of staff nurses…..
• 3. Cleanliness……….
• 4. Beds & Bed Sheets……
• 5. Condition of toilets….
• 6. X-Ray……
• 7. Lab. Facilities…..
61Quality of Care in Health Sector
Specimen of Exit interview Contd. :-
• 8 Hospital stay—(days)……• 9. Time between admission and starting of
treatment.• 10. Any medicine provided from hospital• 11. Total Expenditure on tests & Medicines.• 12.Any suggestions to make the hospital services
better.• 13.Staff member whose services you feel are the
best.
FUNDS GENERATION :-
• Five shops constructed through Rogi KalyanSamiti. Rs.1,11,000/-income per month from these shops.
Improvement of Surrounding area Surrounding area
• This area was full of Bhang Plants
Surrounding area Surrounding Area Contd.
62 Quality of Care in Health Sector
SURROUNDING AREA CONTD.This area was used for toilet and parking by local
people
The same area Being converted into a Garden Contd.
Contd. Contd.
63Quality of Care in Health Sector
Garden developed Bed Condition
Bed Condition Contd. Same beds after repair
Condition of furniture Same furniture after repair
64 Quality of Care in Health Sector
Repair work Repair work Contd.
Tiling work Tiling work complete.
FRU NAGROTA BAGWAN THANKS
65Quality of Care in Health Sector
Anne
xure
8Gr
oup
wor
k 1-
Term
s of
Ref
eren
ce a
nd R
esul
ts
Com
mon
the
mes
Grou
pTh
eme
Furt
her
deta
ilsW
ho s
houl
d be
res
pons
ible
EC EBP
M
Diss
emin
atio
n of
ser
vice
s av
aila
ble
at
vario
us f
acili
ties
(ci
tize
n’s
char
ter)
, (i
nclu
ding
Evi
denc
e ba
sed
educ
atio
n fo
r pa
tien
ts)
Prep
arat
ion
of C
Cs,
serv
ices
ava
ilabl
e, b
enefi
ts
avai
labl
e fo
r vu
lner
able
sec
tion
and
fro
m w
here
, rig
hts
and
resp
onsi
bilit
ies
of e
xter
nal/
inte
rnal
cl
ient
s??
EBP
All I
EC a
ctiv
itie
s sh
ould
foc
us o
n EB
P
Prog
ram
me
offi c
ers
and
hosp
ital
m
anag
ers
-EBP
EC ECM
akin
g se
rvic
es t
rans
pare
nt a
nd
acco
unta
ble
ECEf
fect
ive
com
plai
nt r
edre
ssal
m
echa
nism
s at
the
ser
vice
del
iver
po
ints
Pati
ent/
clie
nt f
eedb
ack,
larg
e sc
ale
surv
eys,
exi
t in
terv
iew
s ,
ques
tion
naire
s sh
ould
be
used
in a
re
gula
r m
anne
r EB
P
Hos
pita
l man
ager
s an
d re
spec
tive
pr
ogra
mm
e m
anag
er/P
MU
EBP
EBP
Case
Man
agem
ent
Deci
sion
s to
be
base
d on
Sta
ndar
d Tr
eatm
ent
Guid
elin
es
Impr
oved
med
ical
rec
ord
keep
ing
like
prop
er
colle
ctio
n, c
olla
tion
Deve
lope
d an
d im
plem
ente
d by
the
sta
te
auth
orit
ies
Peer
rev
iew
pro
cess
bas
ed o
n ST
GEB
PL
Stan
dard
Tre
atm
ent
Guid
elin
esCh
eckl
ist/
stan
dard
s at
dif
fere
nt le
vels
of
hea
lthc
are
faci
lity
and
staf
fs
Deve
lope
d an
d im
plem
ente
d by
the
sta
te
auth
orit
ies
Peer
rev
iew
pro
cess
bas
ed o
n ST
GEB
PA
dedi
cate
d un
it f
or d
isse
min
atio
n of
re
sear
ch fi
ndin
gs a
t St
ate
Leve
l, m
aybe
SI
HFW
Diss
emin
atio
n of
res
earc
h fi n
ding
s
IDSt
anda
rds
and
role
cla
rity
Cust
omis
ed s
tand
ards
are
not
uni
vers
ally
av
aila
ble
Exis
ting
sta
ndar
ds a
re n
ot c
ompr
ehen
sive
Supp
orti
ve m
echa
nism
s ar
e no
t in
pla
ce
Perf
orm
ance
bas
ed in
cent
ives
mec
hani
smSt
anda
rds
wou
ld a
lso
incr
ease
leve
ls o
f tr
ansp
aren
cy a
nd a
ccou
ntab
ility
EBP
Adap
t an
d ad
opt
avai
labl
e na
tion
al/
inte
rnat
iona
l sta
ndar
dsAt
the
sta
te le
vel –
a d
edic
ated
uni
t (S
tate
Qu
alit
y Gr
oup)
for
thi
s pu
rpos
e
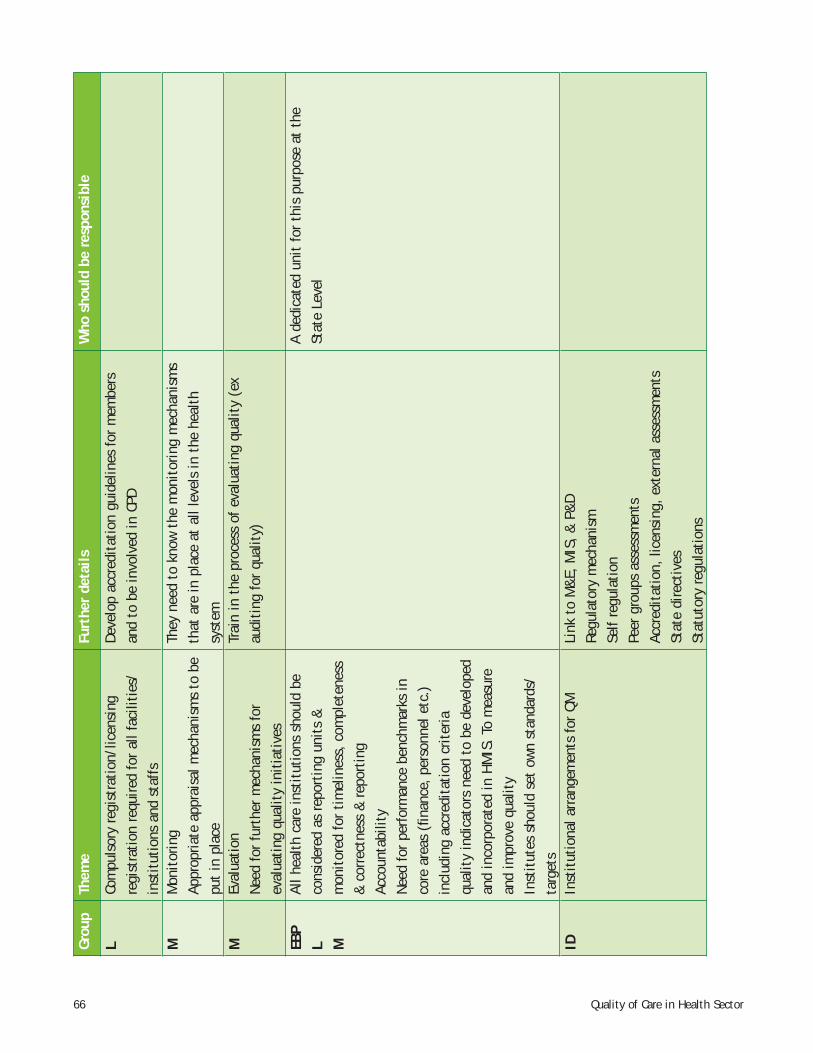
66 Quality of Care in Health Sector
Grou
pTh
eme
Furt
her
deta
ilsW
ho s
houl
d be
res
pons
ible
LCo
mpu
lsor
y re
gist
rati
on/l
icen
sing
re
gist
rati
on r
equi
red
for
all f
acili
ties
/in
stit
utio
ns a
nd s
taff
s
Deve
lop
accr
edit
atio
n gu
idel
ines
for
mem
bers
an
d to
be
invo
lved
in C
PD
MM
onit
orin
gAp
prop
riate
app
rais
al m
echa
nism
s to
be
put
in p
lace
They
nee
d to
kno
w t
he m
onit
orin
g m
echa
nism
s th
at a
re in
pla
ce a
t al
l lev
els
in t
he h
ealt
h sy
stem
MEv
alua
tion
Need
for
fur
ther
mec
hani
sms
for
eval
uati
ng q
ualit
y in
itia
tive
s
Trai
n in
the
pro
cess
of
eval
uati
ng q
ualit
y (e
x au
diti
ng f
or q
ualit
y)
EBP
L M
All h
ealt
h ca
re in
stit
utio
ns s
houl
d be
co
nsid
ered
as
repo
rtin
g un
its
&
mon
itor
ed f
or t
imel
ines
s, c
ompl
eten
ess
& c
orre
ctne
ss &
rep
orti
ngAc
coun
tabi
lity
Need
for
per
form
ance
ben
chm
arks
in
core
are
as (
fi nan
ce, pe
rson
nel e
tc.)
in
clud
ing
accr
edit
atio
n cr
iter
iaqu
alit
y in
dica
tors
nee
d to
be
deve
lope
d an
d in
corp
orat
ed in
HM
IS.
To m
easu
re
and
impr
ove
qual
ity
Inst
itut
es s
houl
d se
t ow
n st
anda
rds/
targ
ets
A de
dica
ted
unit
for
thi
s pu
rpos
e at
the
St
ate
Leve
l
IDIn
stit
utio
nal a
rran
gem
ents
for
QM
Link
to
M&
E, M
IS,
& P
&D
Regu
lato
ry m
echa
nism
Self
regu
lati
onPe
er g
roup
s as
sess
men
tsAc
cred
itat
ion,
lice
nsin
g, e
xter
nal a
sses
smen
tsSt
ate
dire
ctiv
esSt
atut
ory
regu
lati
ons
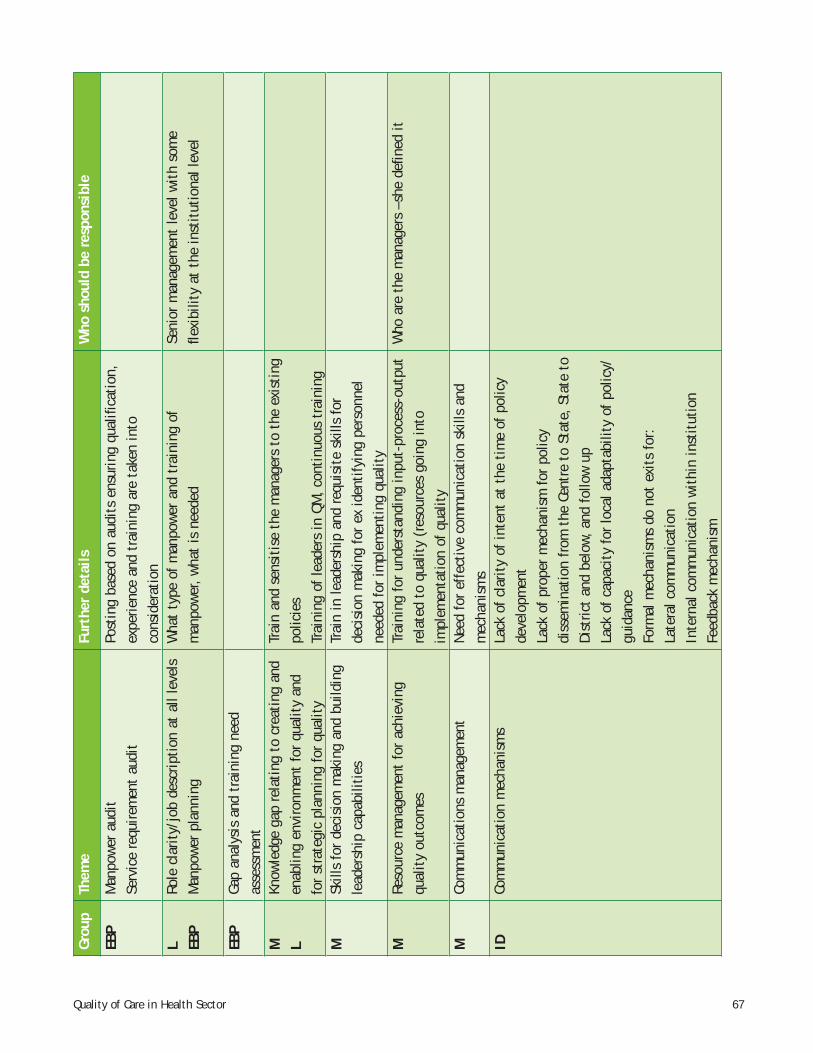
67Quality of Care in Health Sector
Grou
pTh
eme
Furt
her
deta
ilsW
ho s
houl
d be
res
pons
ible
EBP
Man
pow
er a
udit
Serv
ice
requ
irem
ent
audi
tPo
stin
g ba
sed
on a
udit
s en
suri
ng q
ualifi
cat
ion,
ex
perie
nce
and
trai
ning
are
tak
en in
to
cons
ider
atio
nL EB
PRo
le c
lari
ty/j
ob d
escr
ipti
on a
t al
l lev
els
Man
pow
er p
lann
ing
Wha
t ty
pe o
f m
anpo
wer
and
tra
inin
g of
m
anpo
wer
, w
hat
is n
eede
dSe
nior
man
agem
ent
leve
l wit
h so
me
fl exi
bilit
y at
the
inst
itut
iona
l lev
el
EBP
Gap
anal
ysis
and
tra
inin
g ne
ed
asse
ssm
ent
M LKn
owle
dge
gap
rela
ting
to
crea
ting
and
en
ablin
g en
viro
nmen
t fo
r qu
alit
y an
d fo
r st
rate
gic
plan
ning
for
qua
lity
Trai
n an
d se
nsit
ise
the
man
ager
s to
the
exi
stin
g po
licie
sTr
aini
ng o
f le
ader
s in
QM
, co
ntin
uous
tra
inin
gM
Skill
s fo
r de
cisi
on m
akin
g an
d bu
ildin
g le
ader
ship
cap
abili
ties
Trai
n in
lead
ersh
ip a
nd r
equi
site
ski
lls f
or
deci
sion
mak
ing
for
ex id
enti
fyin
g pe
rson
nel
need
ed f
or im
plem
enti
ng q
ualit
yM
Reso
urce
man
agem
ent
for
achi
evin
g qu
alit
y ou
tcom
esTr
aini
ng f
or u
nder
stan
ding
inpu
t-pr
oces
s-ou
tput
re
late
d to
qua
lity
(res
ourc
es g
oing
into
im
plem
enta
tion
of
qual
ity
Who
are
the
man
ager
s –s
he d
efi n
ed it
MCo
mm
unic
atio
ns m
anag
emen
tNe
ed f
or e
ffec
tive
com
mun
icat
ion
skill
s an
d m
echa
nism
sID
Com
mun
icat
ion
mec
hani
sms
Lack
of
clar
ity
of in
tent
at
the
tim
e of
pol
icy
deve
lopm
ent
Lack
of
prop
er m
echa
nism
for
pol
icy
diss
emin
atio
n fr
om t
he C
entr
e to
Sta
te,
Stat
e to
Di
stric
t an
d be
low,
and
fol
low
up
Lack
of
capa
city
for
loca
l ada
ptab
ility
of
polic
y/gu
idan
ce
Form
al m
echa
nism
s do
not
exi
ts f
or:
Late
ral c
omm
unic
atio
nIn
tern
al c
omm
unic
atio
n w
ithi
n in
stit
utio
nFe
edba
ck m
echa
nism
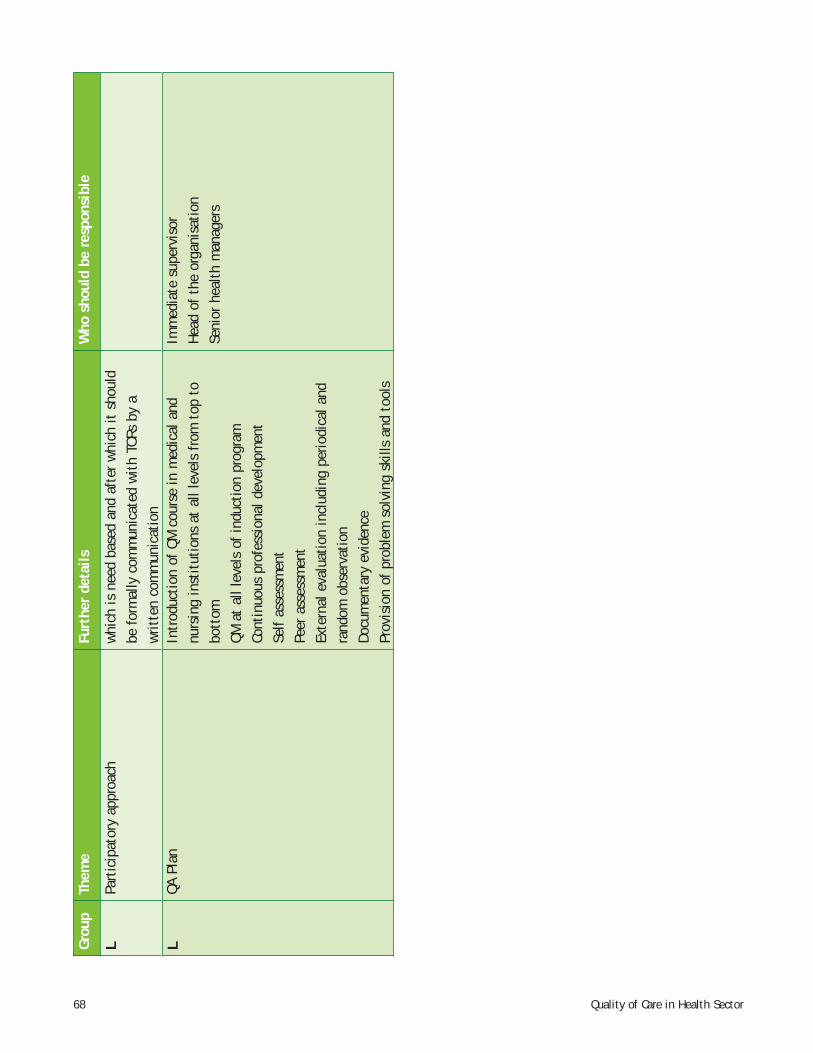
68 Quality of Care in Health Sector
Grou
pTh
eme
Furt
her
deta
ilsW
ho s
houl
d be
res
pons
ible
LPa
rtic
ipat
ory
appr
oach
w
hich
is n
eed
base
d an
d af
ter
whi
ch it
sho
uld
be f
orm
ally
com
mun
icat
ed w
ith
TORs
by
a w
ritt
en c
omm
unic
atio
nL
QA P
lan
Intr
oduc
tion
of
QM c
ours
e in
med
ical
and
nu
rsin
g in
stit
utio
ns a
t al
l lev
els
from
top
to
bott
omQM
at
all l
evel
s of
indu
ctio
n pr
ogra
m
Cont
inuo
us p
rofe
ssio
nal d
evel
opm
ent
Self
asse
ssm
ent
Peer
ass
essm
ent
Exte
rnal
eva
luat
ion
incl
udin
g pe
riodi
cal a
nd
rand
om o
bser
vati
onDo
cum
enta
ry e
vide
nce
Prov
isio
n of
pro
blem
sol
ving
ski
lls a
nd t
ools
Imm
edia
te s
uper
viso
r H
ead
of t
he o
rgan
isat
ion
Seni
or h
ealt
h m
anag
ers
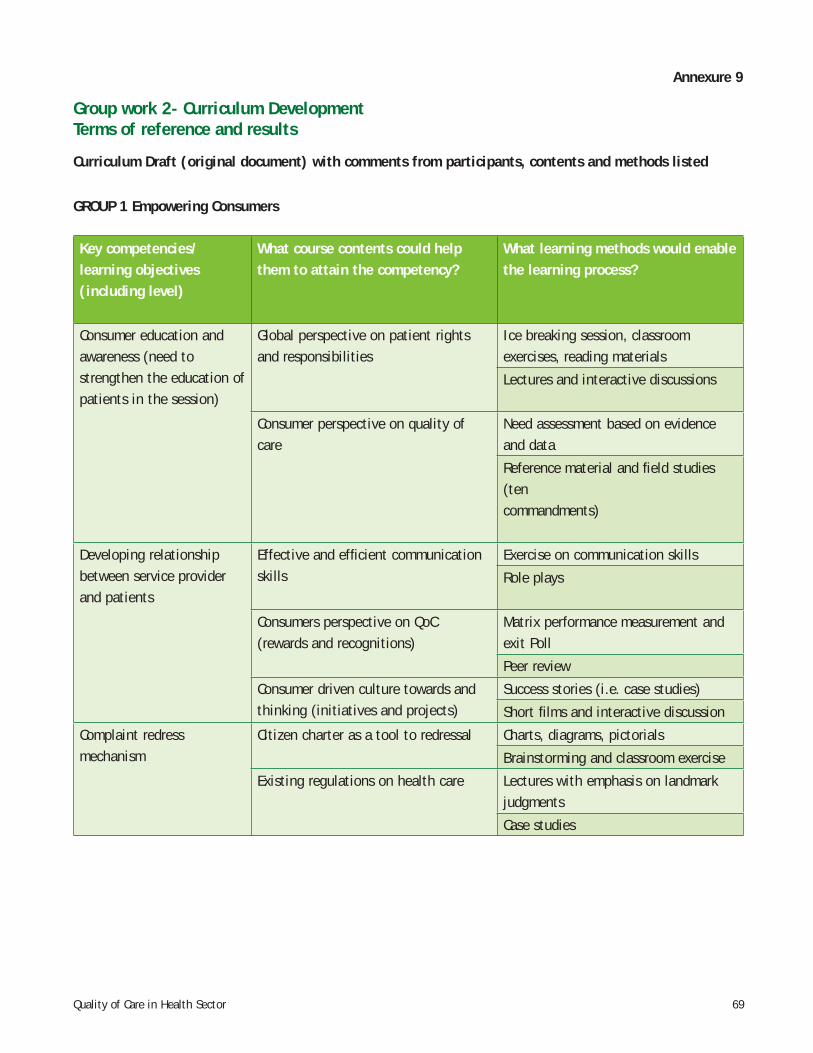
69Quality of Care in Health Sector
Annexure 9
Group work 2- Curriculum DevelopmentTerms of reference and results
Curriculum Draft (original document) with comments from participants, contents and methods listed
GROUP 1 Empowering Consumers
Key competencies/learning objectives(including level)
What course contents could helpthem to attain the competency?
What learning methods would enable the learning process?
Consumer education and awareness (need to strengthen the education of patients in the session)
Global perspective on patient rightsand responsibilities
Ice breaking session, classroom exercises, reading materials
Lectures and interactive discussions
Consumer perspective on quality of care
Need assessment based on evidence and data
Reference material and fi eld studies (tencommandments)
Developing relationship between service provider and patients
Effective and effi cient communicationskills
Exercise on communication skills
Role plays
Consumers perspective on QoC(rewards and recognitions)
Matrix performance measurement and exit Poll
Peer review
Consumer driven culture towards andthinking (initiatives and projects)
Success stories (i.e. case studies)
Short fi lms and interactive discussion
Complaint redress mechanism
Citizen charter as a tool to redressal Charts, diagrams, pictorials
Brainstorming and classroom exercise
Existing regulations on health care Lectures with emphasis on landmark judgments
Case studies
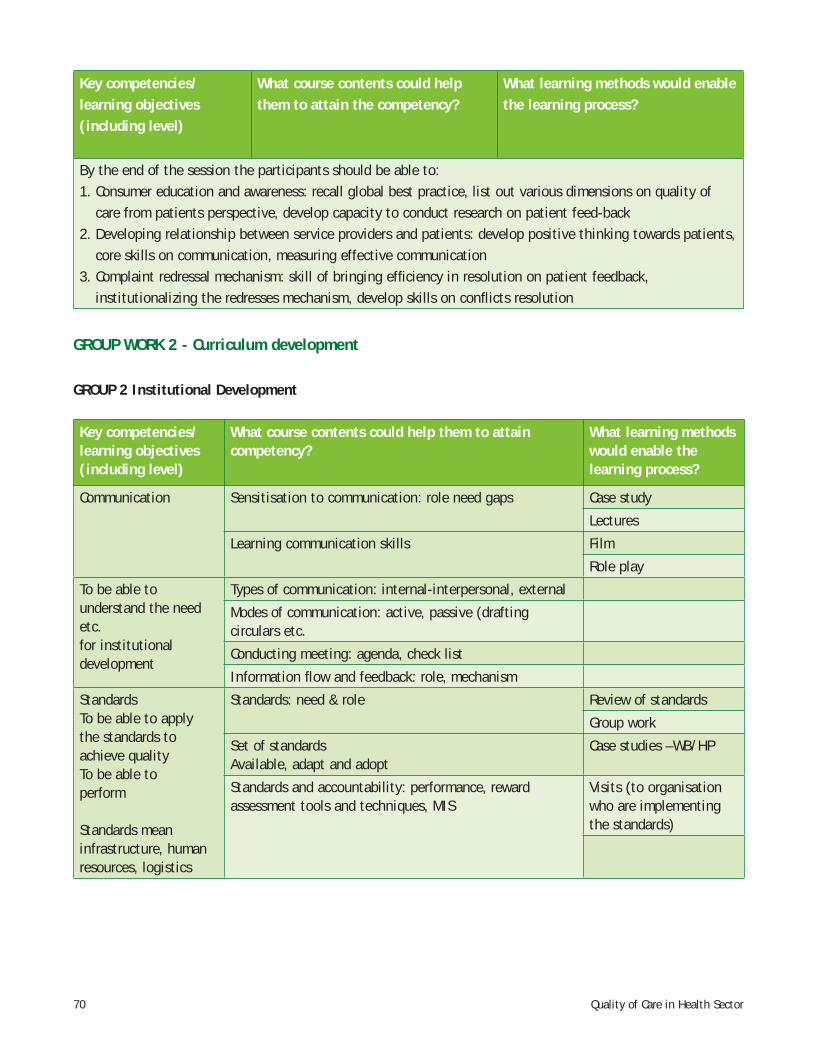
70 Quality of Care in Health Sector
Key competencies/learning objectives(including level)
What course contents could helpthem to attain the competency?
What learning methods would enable the learning process?
By the end of the session the participants should be able to:1. Consumer education and awareness: recall global best practice, list out various dimensions on quality of
care from patients perspective, develop capacity to conduct research on patient feed-back2. Developing relationship between service providers and patients: develop positive thinking towards patients,
core skills on communication, measuring effective communication3. Complaint redressal mechanism: skill of bringing effi ciency in resolution on patient feedback,
institutionalizing the redresses mechanism, develop skills on confl icts resolution
GROUP WORK 2 - Curriculum development
GROUP 2 Institutional Development
Key competencies/learning objectives(including level)
What course contents could help them to attain competency?
What learning methods would enable the learning process?
Communication Sensitisation to communication: role need gaps Case study
Lectures
Learning communication skills Film
Role play
To be able tounderstand the need etc.for institutionaldevelopment
Types of communication: internal-interpersonal, external
Modes of communication: active, passive (drafting circulars etc.
Conducting meeting: agenda, check list
Information fl ow and feedback: role, mechanism
StandardsTo be able to applythe standards toachieve qualityTo be able toperform
Standards meaninfrastructure, humanresources, logistics
Standards: need & role Review of standards
Group work
Set of standardsAvailable, adapt and adopt
Case studies –WB/HP
Standards and accountability: performance, reward assessment tools and techniques, MIS
Visits (to organisation who are implementing the standards)
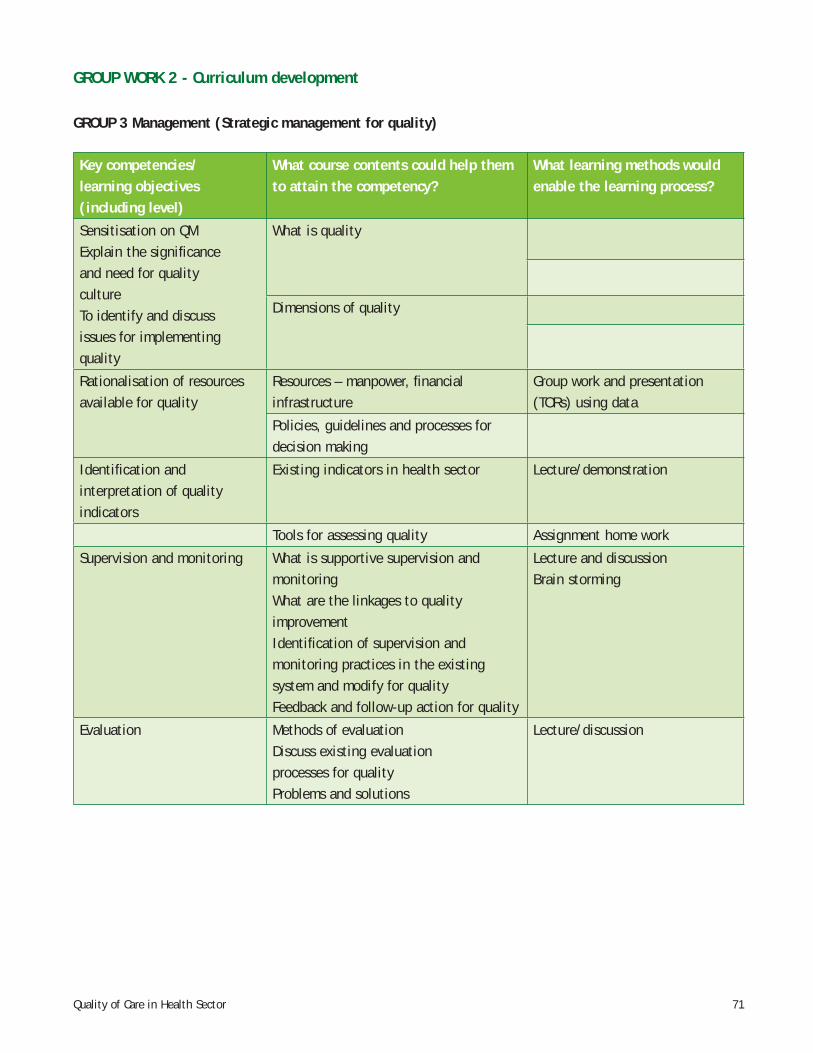
71Quality of Care in Health Sector
GROUP WORK 2 - Curriculum development
GROUP 3 Management (Strategic management for quality)
Key competencies/learning objectives(including level)
What course contents could help them to attain the competency?
What learning methods would enable the learning process?
Sensitisation on QM Explain the signifi canceand need for qualitycultureTo identify and discussissues for implementing quality
What is quality
Dimensions of quality
Rationalisation of resources available for quality
Resources – manpower, fi nancial infrastructure
Group work and presentation (TORs) using data
Policies, guidelines and processes for decision making
Identifi cation and interpretation of quality indicators
Existing indicators in health sector Lecture/demonstration
Tools for assessing quality Assignment home work
Supervision and monitoring What is supportive supervision andmonitoringWhat are the linkages to qualityimprovementIdentifi cation of supervision andmonitoring practices in the existing system and modify for qualityFeedback and follow-up action for quality
Lecture and discussionBrain storming
Evaluation Methods of evaluationDiscuss existing evaluationprocesses for qualityProblems and solutions
Lecture/discussion
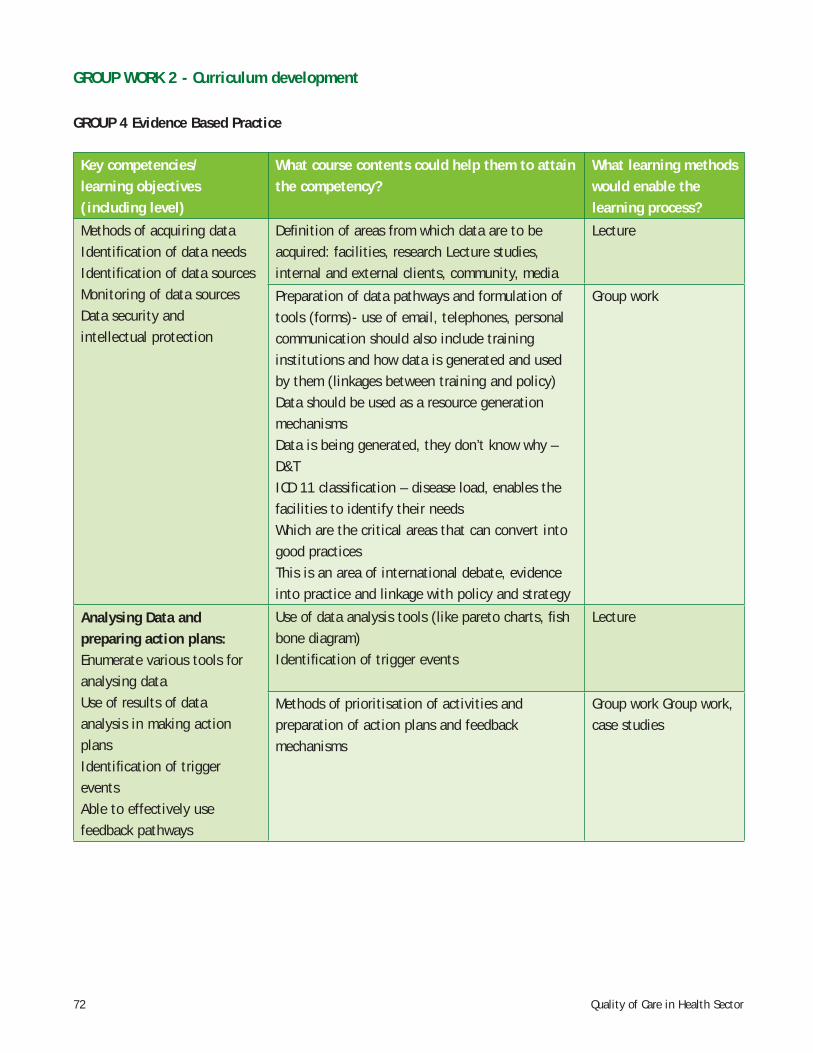
72 Quality of Care in Health Sector
GROUP WORK 2 - Curriculum development
GROUP 4 Evidence Based Practice
Key competencies/learning objectives(including level)
What course contents could help them to attain the competency?
What learning methods would enable thelearning process?
Methods of acquiring dataIdentifi cation of data needsIdentifi cation of data sourcesMonitoring of data sourcesData security and intellectual protection
Defi nition of areas from which data are to be acquired: facilities, research Lecture studies, internal and external clients, community, media
Lecture
Preparation of data pathways and formulation of tools (forms)- use of email, telephones, personal communication should also include training institutions and how data is generated and used by them (linkages between training and policy)Data should be used as a resource generation mechanismsData is being generated, they don’t know why – D&TICD 11 classifi cation – disease load, enables the facilities to identify their needsWhich are the critical areas that can convert into good practicesThis is an area of international debate, evidence into practice and linkage with policy and strategy
Group work
Analysing Data andpreparing action plans:Enumerate various tools foranalysing dataUse of results of dataanalysis in making actionplansIdentifi cation of triggereventsAble to effectively usefeedback pathways
Use of data analysis tools (like pareto charts, fi sh bone diagram) Identifi cation of trigger events
Lecture
Methods of prioritisation of activities and preparation of action plans and feedback mechanisms
Group work Group work, case studies
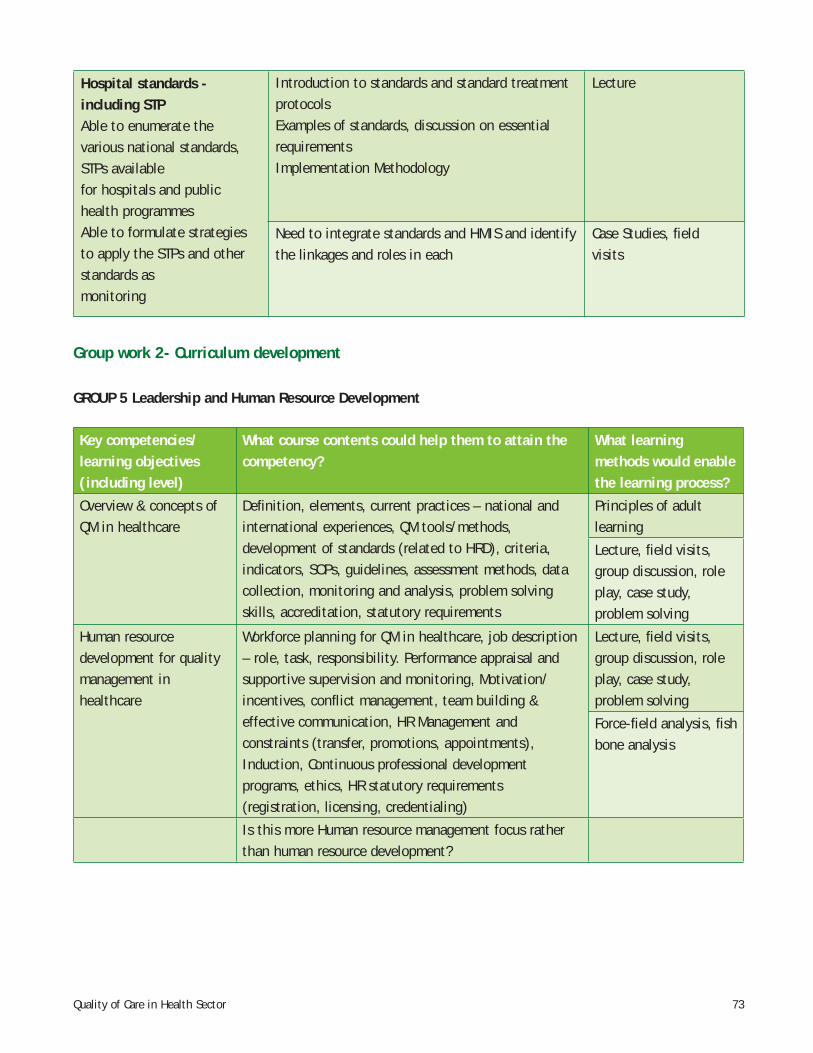
73Quality of Care in Health Sector
Hospital standards - including STPAble to enumerate thevarious national standards, STPs availablefor hospitals and publichealth programmesAble to formulate strategiesto apply the STPs and otherstandards asmonitoring
Introduction to standards and standard treatment protocolsExamples of standards, discussion on essential requirementsImplementation Methodology
Lecture
Need to integrate standards and HMIS and identify the linkages and roles in each
Case Studies, fi eldvisits
Group work 2- Curriculum development
GROUP 5 Leadership and Human Resource Development
Key competencies/learning objectives(including level)
What course contents could help them to attain the competency?
What learning methods would enable the learning process?
Overview & concepts ofQM in healthcare
Defi nition, elements, current practices – national and international experiences, QM tools/methods, development of standards (related to HRD), criteria, indicators, SOPs, guidelines, assessment methods, datacollection, monitoring and analysis, problem solving skills, accreditation, statutory requirements
Principles of adultlearning
Lecture, fi eld visits,group discussion, roleplay, case study,problem solving
Human resourcedevelopment for qualitymanagement inhealthcare
Workforce planning for QM in healthcare, job description – role, task, responsibility. Performance appraisal and supportive supervision and monitoring, Motivation/incentives, confl ict management, team building & effective communication, HR Management and constraints (transfer, promotions, appointments), Induction, Continuous professional development programs, ethics, HR statutory requirements (registration, licensing, credentialing)
Lecture, fi eld visits,group discussion, roleplay, case study,problem solving
Force-fi eld analysis, fi shbone analysis
Is this more Human resource management focus rather than human resource development?
74 Quality of Care in Health Sector
Annexure- 10
An Introduction to National Institute of Health and Family Welfare (NIHFW)
The NIHFW is an autonomous body registered under the Societies Act, which gives it the freedom to make its own rules and to also charge for the courses delivered. However, policies and decisions are also guided by rules and regulations, approved by the governing body, of which the Minister of Health and Family Welfare, Government of India is the Chairman, the Secretary (Health and Family Welfare) is the Vice Chairman and Director of the institution, is the member secretary.
The institution has its own vision and mission. The Programme Advisory Committee (PAC) supports and monitors the teaching, research and training activities, and also gives guidance for improvement of the programmes, which are reviewed on a regular basis.
The institute was established in 1977 by amalgamation of two erstwhile institutions namely, National Institute of Health Administration and Education (NIHAE) and the National Institute of Family Planning (NIFP). The objective of the institute is to promote Health and Family Welfare programmes in the country through education, training, research, evaluation, consultancy and specialised services.
The institute provides advisory and consultancy services to the central government, state governments and other national and international agencies, and conducts training and research in the fi eld of public health. It also imparts postgraduate teaching in the fi eld of community health administration, including hospital administration. The institute with the support of European Commission, established a professional development course on ‘public health, management and health sector reforms for district medical offi cers’ and at present, this course is being imparted in cooperation with 15 State Institutes of Health and Family Welfare and private institutions. Hospital and health management are also the key areas of the one year post graduate certifi cate distance learning courses conducted by the institute. The institute recently established a Public Health Research and Education Consortium - network and partnership. 167 medical colleges, 34 training institutions of health and family welfare, 168 nursing colleges and schools; and 125 NGOs are the partners. It provides a very good platform for exchanging information and providing opportunities to introduce quality management in the curriculum of other institutions as well.
Recently, NIHFW, in partnership with UNFPA has also undertaken Rapid Appraisal of Health Interventions (RAHI) under NRHM. During the fi rst phase, technical and fi nancial support was given to 12 partner institutions in NRHM states and in the second phase, 12 more partner institutions are involved.
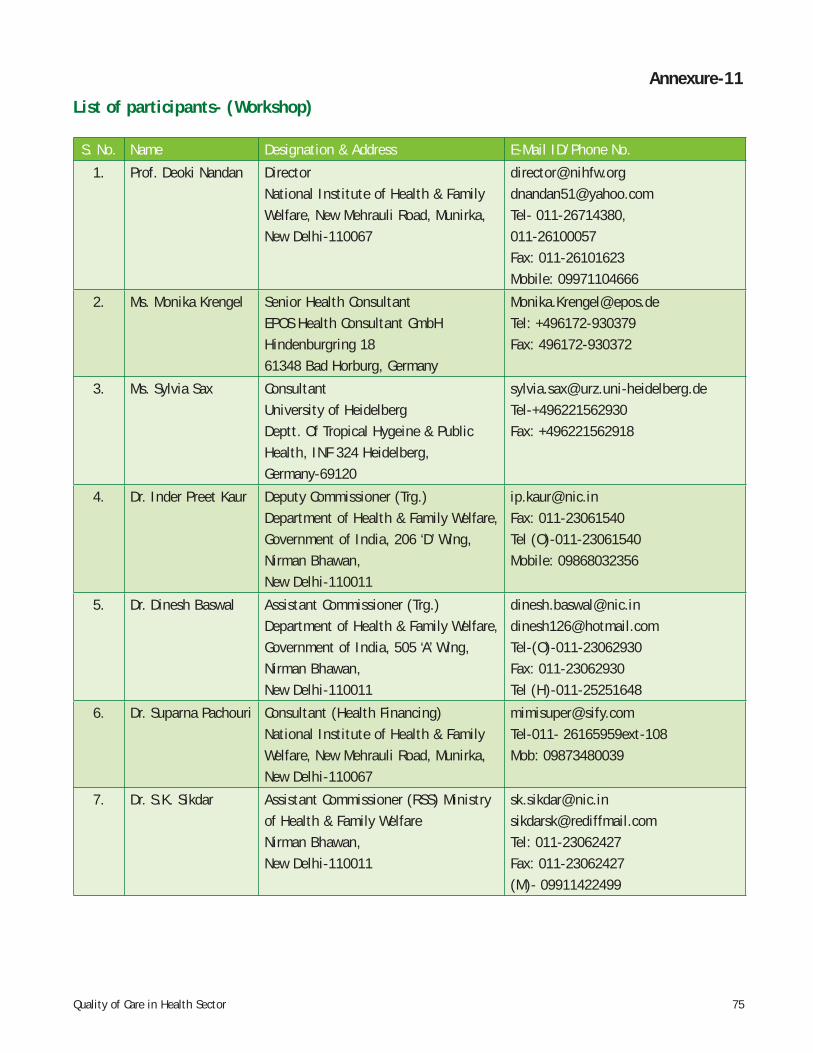
75Quality of Care in Health Sector
Annexure-11
List of participants- (Workshop)
S. No. Name Designation & Address E-Mail ID/Phone No.
1. Prof. Deoki Nandan DirectorNational Institute of Health & Family Welfare, New Mehrauli Road, Munirka, New Delhi-110067
[email protected] [email protected] 011-26714380, 011-26100057Fax: 011-26101623Mobile: 09971104666
2. Ms. Monika Krengel Senior Health Consultant EPOS Health Consultant GmbHHindenburgring 1861348 Bad Horburg, Germany
[email protected]: +496172-930379Fax: 496172-930372
3. Ms. Sylvia Sax ConsultantUniversity of HeidelbergDeptt. Of Tropical Hygeine & Public Health, INF 324 Heidelberg, Germany-69120
[email protected]+496221562930Fax: +496221562918
4. Dr. Inder Preet Kaur Deputy Commissioner (Trg.)Department of Health & Family Welfare, Government of India, 206 ‘D’ Wing, Nirman Bhawan, New Delhi-110011
[email protected]: 011-23061540Tel (O)-011-23061540Mobile: 09868032356
5. Dr. Dinesh Baswal Assistant Commissioner (Trg.)Department of Health & Family Welfare, Government of India, 505 ‘A’ Wing, Nirman Bhawan, New Delhi-110011
[email protected]@hotmail.comTel-(O)-011-23062930Fax: 011-23062930Tel (H)-011-25251648
6. Dr. Suparna Pachouri Consultant (Health Financing)National Institute of Health & Family Welfare, New Mehrauli Road, Munirka, New Delhi-110067
[email protected] 26165959ext-108Mob: 09873480039
7. Dr. S.K. Sikdar Assistant Commissioner (RSS) Ministry of Health & Family WelfareNirman Bhawan, New Delhi-110011
[email protected] [email protected]: 011-23062427Fax: 011-23062427(M)- 09911422499
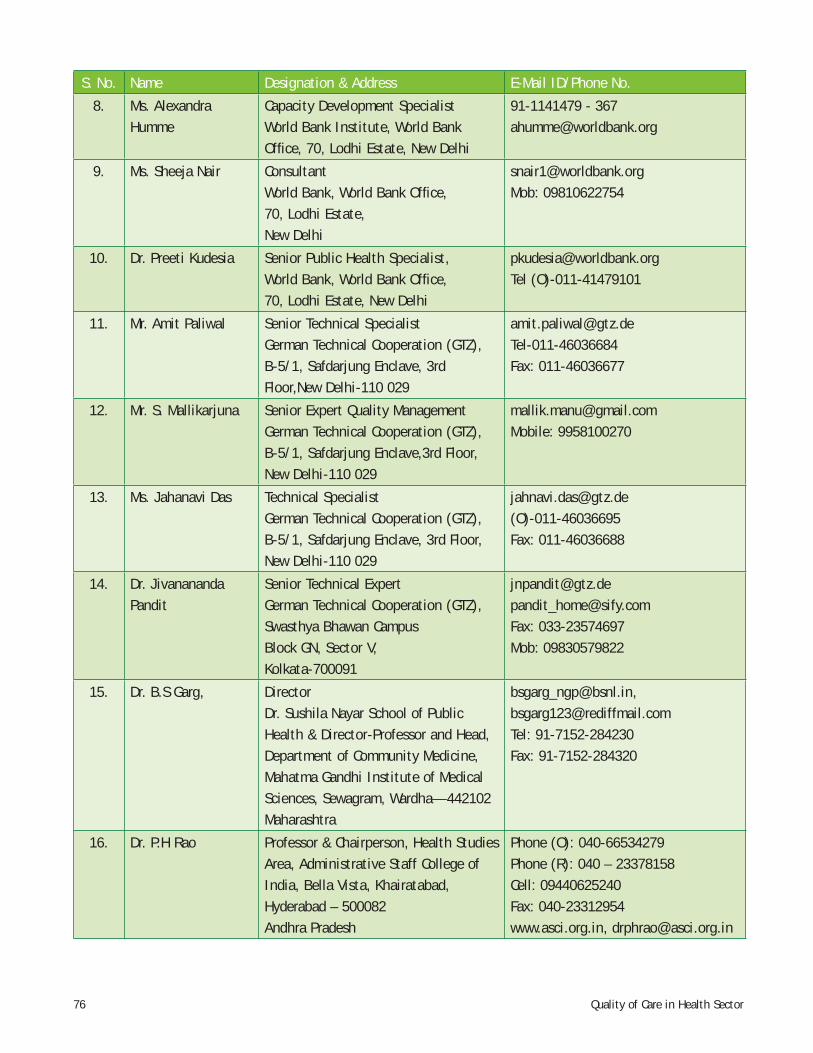
76 Quality of Care in Health Sector
S. No. Name Designation & Address E-Mail ID/Phone No.
8. Ms. Alexandra Humme
Capacity Development SpecialistWorld Bank Institute, World Bank Offi ce, 70, Lodhi Estate, New Delhi
91-1141479 - [email protected]
9. Ms. Sheeja Nair ConsultantWorld Bank, World Bank Offi ce, 70, Lodhi Estate, New Delhi
[email protected]: 09810622754
10. Dr. Preeti Kudesia Senior Public Health Specialist, World Bank, World Bank Offi ce, 70, Lodhi Estate, New Delhi
[email protected] (O)-011-41479101
11. Mr. Amit Paliwal Senior Technical SpecialistGerman Technical Cooperation (GTZ), B-5/1, Safdarjung Enclave, 3rd Floor,New Delhi-110 029
[email protected]: 011-46036677
12. Mr. S. Mallikarjuna Senior Expert Quality ManagementGerman Technical Cooperation (GTZ), B-5/1, Safdarjung Enclave,3rd Floor,New Delhi-110 029
[email protected]: 9958100270
13. Ms. Jahanavi Das Technical Specialist German Technical Cooperation (GTZ), B-5/1, Safdarjung Enclave, 3rd Floor, New Delhi-110 029
[email protected](O)-011-46036695Fax: 011-46036688
14. Dr. Jivanananda Pandit
Senior Technical ExpertGerman Technical Cooperation (GTZ), Swasthya Bhawan CampusBlock GN, Sector V, Kolkata-700091
[email protected][email protected]: 033-23574697Mob: 09830579822
15. Dr. B.S Garg, DirectorDr. Sushila Nayar School of Public Health & Director-Professor and Head, Department of Community Medicine, Mahatma Gandhi Institute of Medical Sciences, Sewagram, Wardha—442102Maharashtra
[email protected], [email protected]: 91-7152-284230Fax: 91-7152-284320
16. Dr. P.H Rao Professor & Chairperson, Health Studies Area, Administrative Staff College of India, Bella Vista, Khairatabad, Hyderabad – 500082Andhra Pradesh
Phone (O): 040-66534279Phone (R): 040 – 23378158Cell: 09440625240Fax: 040-23312954www.asci.org.in, [email protected]
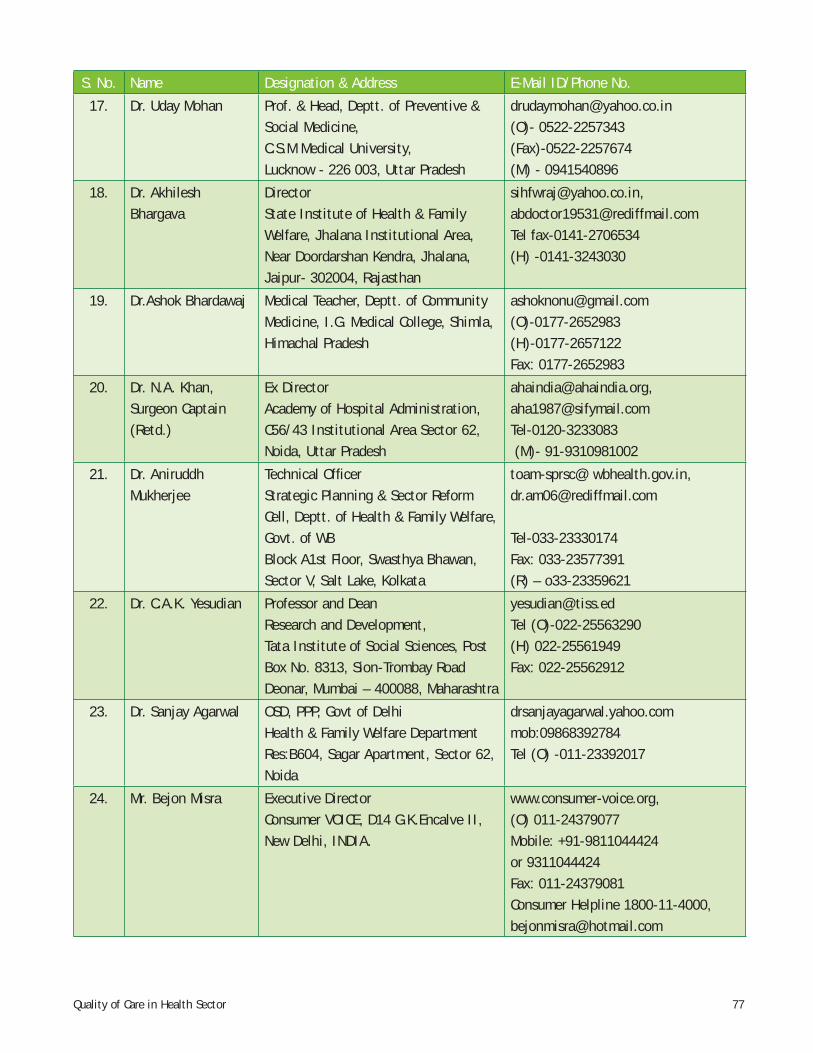
77Quality of Care in Health Sector
S. No. Name Designation & Address E-Mail ID/Phone No.
17. Dr. Uday Mohan Prof. & Head, Deptt. of Preventive & Social Medicine, C.S.M Medical University,Lucknow - 226 003, Uttar Pradesh
[email protected](O)- 0522-2257343(Fax)-0522-2257674(M) - 0941540896
18. Dr. Akhilesh Bhargava
DirectorState Institute of Health & Family Welfare, Jhalana Institutional Area, Near Doordarshan Kendra, Jhalana, Jaipur- 302004, Rajasthan
[email protected], [email protected] fax-0141-2706534(H) -0141-3243030
19. Dr.Ashok Bhardawaj Medical Teacher, Deptt. of Community Medicine, I.G. Medical College, Shimla, Himachal Pradesh
[email protected](O)-0177-2652983(H)-0177-2657122Fax: 0177-2652983
20. Dr. N.A. Khan,Surgeon Captain (Retd.)
Ex DirectorAcademy of Hospital Administration, C56/43 Institutional Area Sector 62, Noida, Uttar Pradesh
[email protected], [email protected] (M)- 91-9310981002
21. Dr. Aniruddh Mukherjee
Technical Offi cerStrategic Planning & Sector Reform Cell, Deptt. of Health & Family Welfare, Govt. of WBBlock A1st Floor, Swasthya Bhawan, Sector V, Salt Lake, Kolkata
toam-sprsc@ wbhealth.gov.in, [email protected]
Tel-033-23330174Fax: 033-23577391(R) – o33-23359621
22. Dr. C.A.K. Yesudian Professor and DeanResearch and Development, Tata Institute of Social Sciences, Post Box No. 8313, Sion-Trombay Road Deonar, Mumbai – 400088, Maharashtra
[email protected] (O)-022-25563290(H) 022-25561949Fax: 022-25562912
23. Dr. Sanjay Agarwal OSD, PPP, Govt of DelhiHealth & Family Welfare DepartmentRes:B604, Sagar Apartment, Sector 62, Noida
drsanjayagarwal.yahoo.commob:09868392784Tel (O) -011-23392017
24. Mr. Bejon Misra Executive DirectorConsumer VOICE, D14 G.K.Encalve II, New Delhi, INDIA.
www.consumer-voice.org,(O) 011-24379077Mobile: +91-9811044424 or 9311044424Fax: 011-24379081Consumer Helpline 1800-11-4000, [email protected]
78 Quality of Care in Health Sector
S. No. Name Designation & Address E-Mail ID/Phone No.
25. Dr. M. Bhattacharya Prof. & HeadDeptt. of C.H.A., Dean of studies, National Institute of Health & Family Welfare, New Mehrauli Road, Munirka, New Delhi-110067
Tel: 011-26714378, Fax: 26101623,26165959 (Ext) [email protected], [email protected],
26. Dr. K. Kalaivani Nodal Offi cer, RCH and Prof. & Head,Deptt. of RBM, National Institute of Health & Family Welfare, New Mehrauli Road, Munirka, New Delhi-110067
91-11-26165959, 26166441 Ext. 333, 330(F): 011-26101623 (M): [email protected]@gmail.com
27. Dr. T. Mathiyazhagan Prof. & HeadDeptt. of Communication, National Institute of Health & Family Welfare, New Mehrauli Road, Munirka, New Delhi-110067
91-11-26165959, 26166441 Ext. 368(Fax): 011-26101623(R): 011-25250057(M): [email protected][email protected]
28. Dr. J.K Das Prof. & HeadDeptt. of Epidemiology, National Institute of Health & Family Welfare,New Mehrauli Road, Munirka, New Delhi-110067
91-11-26165959, 26166441 Ext. [email protected]: 011-26101623
29. Dr. A.M Khan Prof. & HeadDeptt. of Social Science, National Institute of Health & Family Welfare,New Mehrauli Road, Munirka, New Delhi-110067
91-11-26165959, 26166441 Ext.308(Fax): 011-26101623(M): [email protected][email protected]
30. Dr. Sanjay Gupta Reader, Deptt. of C.H.A., National Institute of Health & Family Welfare,New Mehrauli Road, Munirka, New Delhi-110067
91-11-26165959, 26166441 Ext. 338(F): [email protected]
31. Dr. K. S. Nair Lecturer (Health Economics)Deptt. of Planning & Evaluation, National Institute of Health & Family Welfare, New Mehrauli Road, Munirka, New Delhi-110067
91-11-26165959, 26166441 Ext. 197Mobile: [email protected][email protected]
79Quality of Care in Health Sector
S. No. Name Designation & Address E-Mail ID/Phone No.
32. Dr.D.S.Chandel SMO I/C Civil Hospital PalampurDistt. Kangra H.P.
[email protected](o)1894-234101(H) 1894230857Mob: 09418105470
33. DR. A.R. Raghu BMO, CHC Nagrota, Bagwan Distt. Kangra Himachal Pradesh.
09816043403
34. Dr. Surender Kashyap
Principal, Indira Gandhi Medical College, Shimla, H.P. 171001
[email protected]: 01772804251Fax: 0177 2658339
35. Dr. T Bir Reader, Department of Social Sciences NIHFW, New Delhi 110067
[email protected][email protected]
36. Dr. Abhilash Sood Department of Community Medicine, IGMC Shimla, H.P.
[email protected] 09418076890
37. Dr. Prem Poonam Deputy Director, Health ServicesDirectorate of Health Services Shimla, H.P
0177- 2622444



4th-8th June, 2008, Shimla
vkjksX;e~ lq[klEinkvkjksX;e~ lq[klEink
Workshop for Senior and Mid-level Managers on Improving
Quality of Care in Health Sector
NIHFW
Organised by: Supported by:
Partner for the Future.Worldwide.
Jointly Organised by National Institute of Health and Family Welfare
and World Bank Institute with Technical Support of GTZ
National Institute of Health and Family WelfareBaba Gang Nath Marg, Munirka, New Delhi – 110067
Email: [email protected]: www.nihfw.org
Report
Recommended