
Psychoneuroimmunology :Clinical Application of an
Emerging Field in Medicine
Elizabeth A. Stuller, M.D. ABPN Board Certified in Adult and Addiction Psychiatry
MAOP Maryland Association of Osteopathic Physicians Annual Meeting 2013
December 5‐8, 2013 Baltimore, Maryland

Learning Objectives
Recognize emerging trends in brain science
Explore the convergence of the fields of psychiatry, neurology,
immunology, and endocrinology, the most rapidly advancing
areas in medical science.
An overview of the interconnected super system and additional
applications in addiction psychiatry and medicine.

The Brain Initiative
The Brain InitiativeIn February, 2013, Obama unveiled funding for the initiative, called Brain Research Through Advancing Innovative Neurotechnologies, or BRAIN.
The White House says it "aims to help researchers find new ways to treat, cure, and even prevent brain disorders, such as Alzheimer's disease, epilepsy, and traumatic brain injury."
Global Positioning System ‐GPS

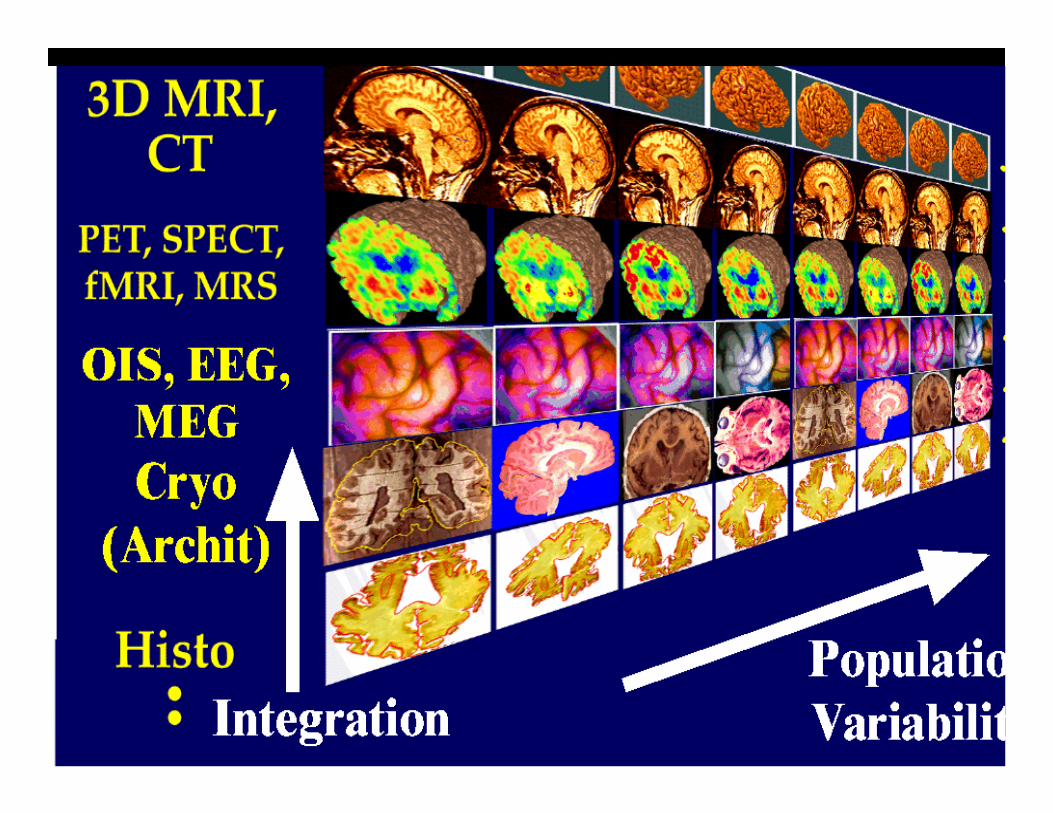
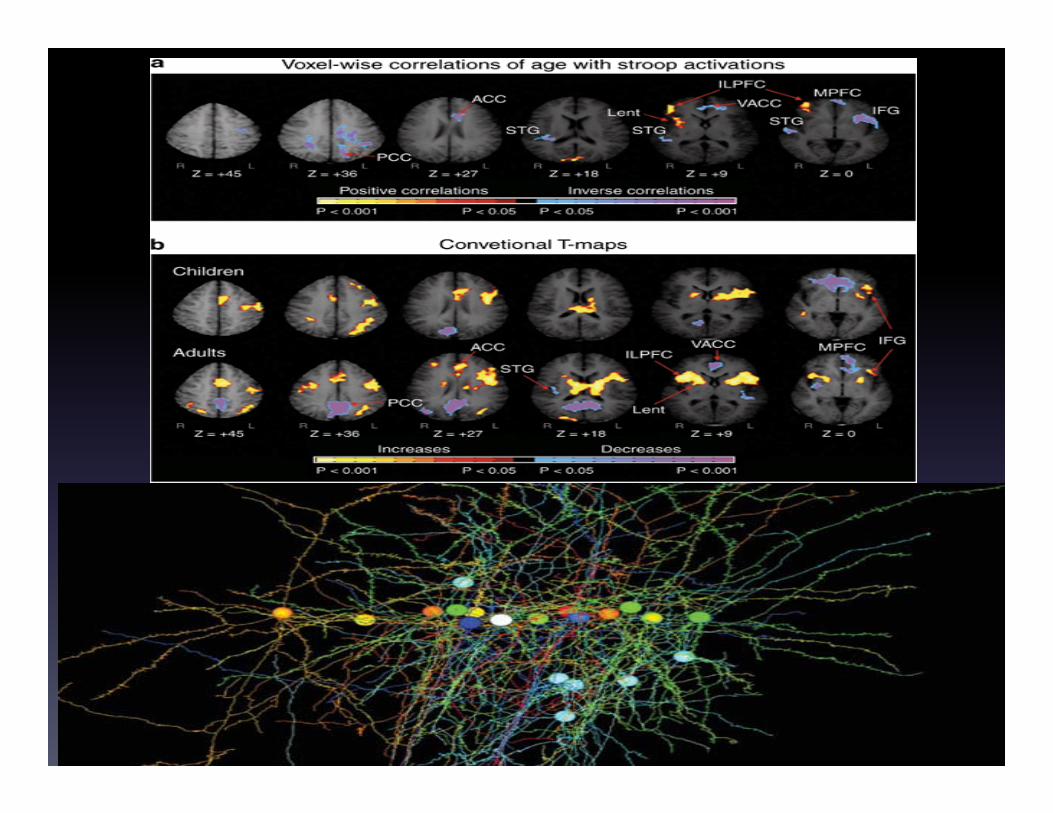
Emerging Neuroimaging Advancements
Emerging Brain Activity Maps
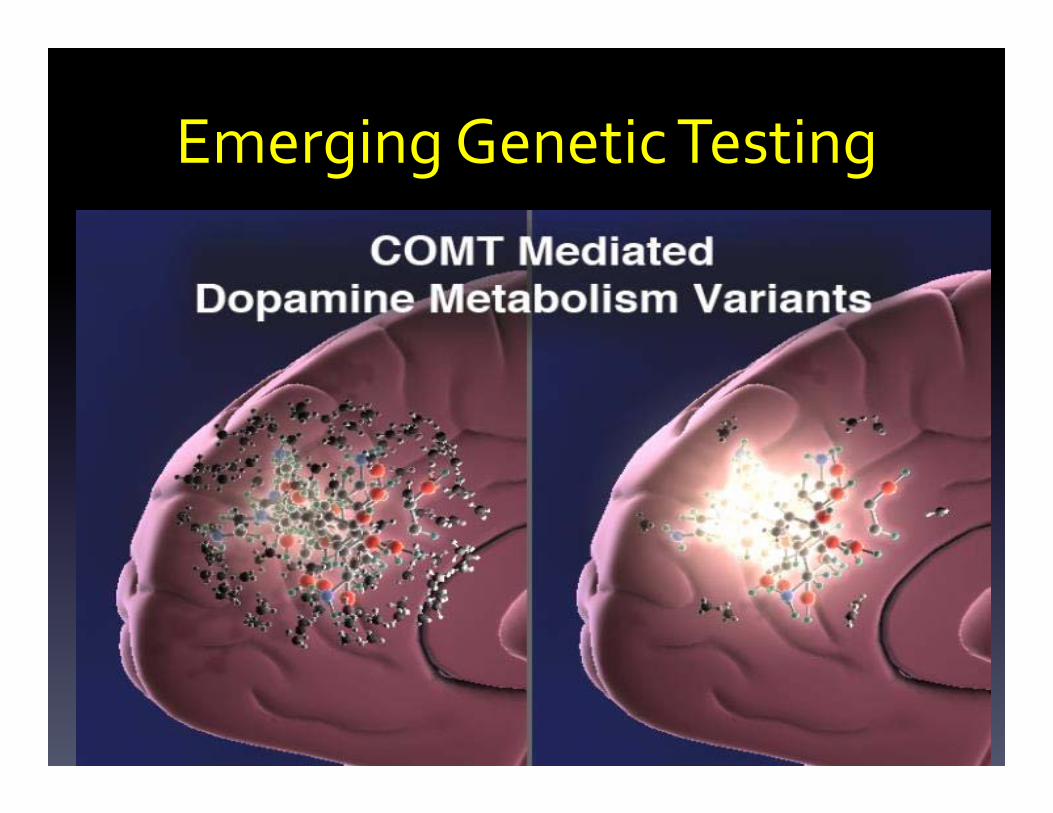
Emerging Genetic Testing
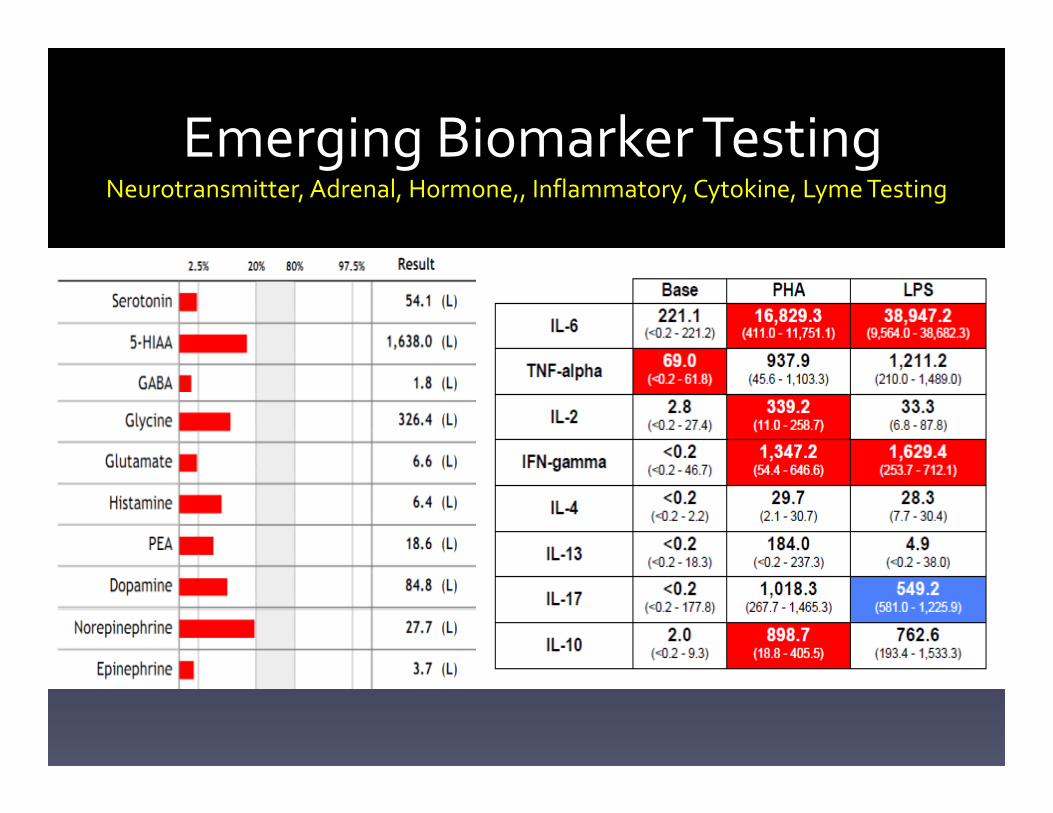
Emerging Biomarker TestingNeurotransmitter, Adrenal, Hormone,, Inflammatory, Cytokine, Lyme Testing
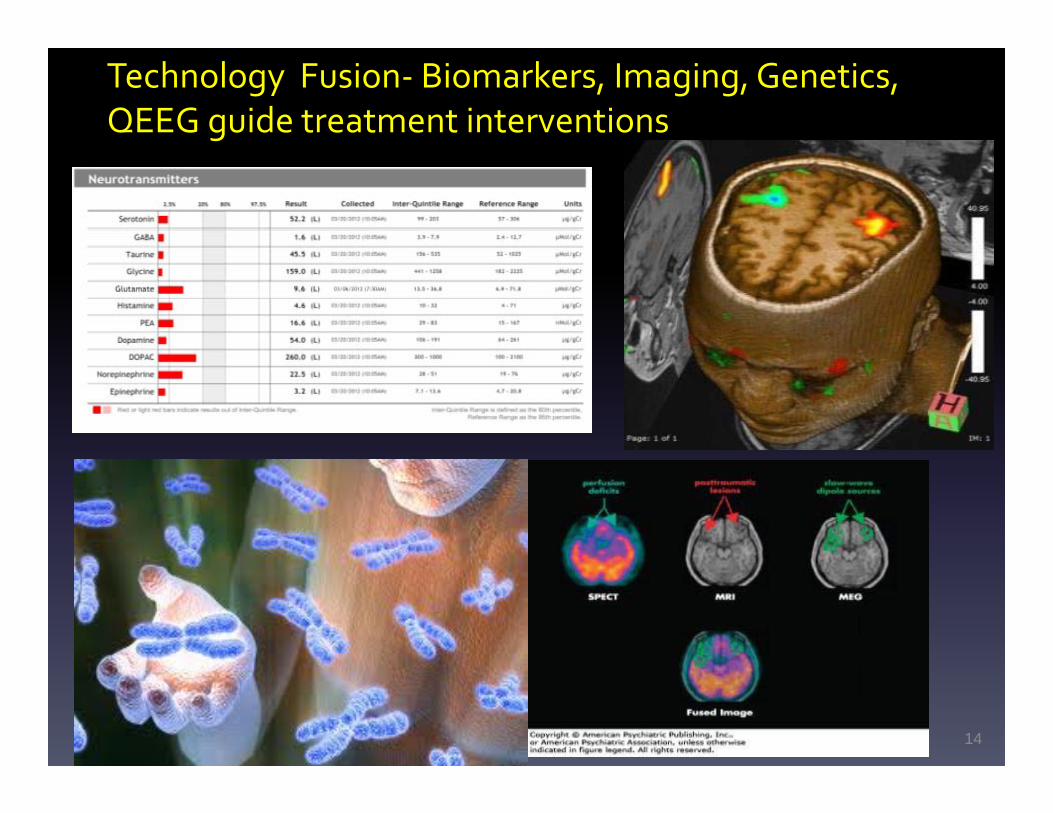
Technology Fusion‐ Biomarkers, Imaging, Genetics, QEEG guide treatment interventions
14
Putting it all Together


January 1, 2013 on 60 MinutesIncredible Brain‐Machine Interface Research
Leading To Robotic Prosthetics
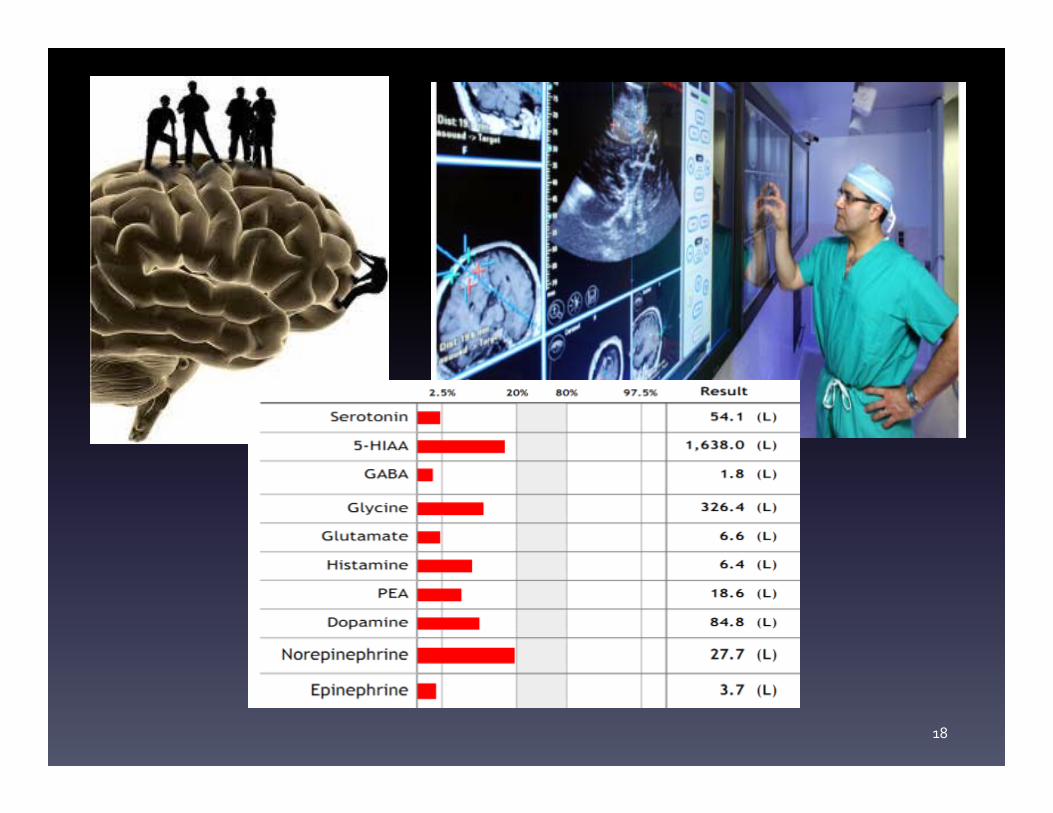
18

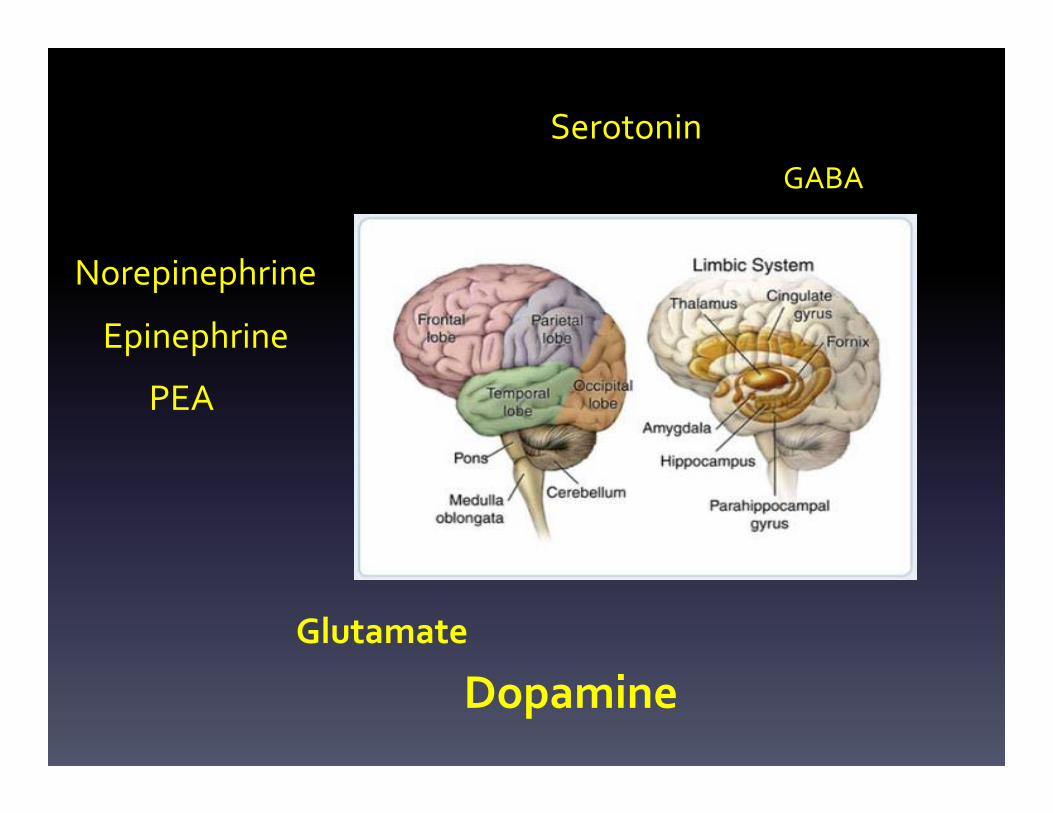
Neurotransmitters are biomarkers of nervous system function
Serotonin
Dopamine
GABA
Glutamate
Epinephrine
Norepinephrine
Histamine
PEA
Irwin, M, et al. Brain, Behavior, and Immunity. 2003:17;365-372Vashadze, S. Georgian Med. News 2007;(150):22-4
Neurotransmitters as Biomarkers
• Have been used in academia for 60 years1
• Can be accurately and affordably measured using ELISA‐
based methods
• Serve as clinical correlates to a host of neuropsychiatric
conditions2
• Provides insight into deficiencies/imbalances of the neuro‐
endo‐immune supersystem3
1. von Euler, U., et al. (1951). Br J Pharmacol Chemother. 6(2):286-288.
2. See “Urinary Neurotransmitter Testing: Myths & Misconsceptions” for review
3. Cohrs, S., et al. (2004). Neurosci Letters. 360:161-164.
What do urinary neurotransmitter measurements represent?
• Non‐invasive, quantitative analysis of whole body neurotransmitter excretion
• Biomarkers of peripheral and central nervous system function
• Clinical correlates of various neuropsychiatric conditions
• Acts as guide for nutritional, supplemental, pharmaceutical interventions
21
Serotonin
Glutamate
Norepinephrine
Dopamine
GABA
Epinephrine
PEA

Serotonin
GABAGlutamate
NorepinephrineDopamine
GABA
Epinephrine
Biomarkers and AddictionPredicting Behavioral Patterns
For Example : The still developing Pre‐Frontal Cortex

Young and Impaired Prefrontal Cortex
“Addiction without treatment…
………………is progressive and
can result in
disability or
premature death.”
http://www.asam.org/advocacy/find‐a‐policy‐statement/view‐policy‐statement/public‐policy‐statements/2011/12/15/the‐definition‐of‐addiction
Addiction and the brain:The role of neurotransmitters in the cause and
treatment of drug dependence
RECENT SCIENTIFIC ADVANCES HAVE LED to a greater understanding of
the neurobiological processes that underlie drug abuse and addiction. These
suggest that multiple neurotransmitter systems may play a key role
in the development and expression of drug dependence.
These advances in our knowledge promise not only to help us identify the
underlying cause of drug abuse and dependence, but also to aid in the
development of effective treatment strategies.
Tomkins DM, et. al. (2001). CMAJ. 164(6): 817‐21.
Neurotransmitter Biomarkers are needed to allow health care providers to choose more accurately and to
avoid guessing
28
Neurotransmitter Testing Applications in Clinical Settings
• Determine treatment therapy
• Identify individuals with a high‐risk for relapse
• Determine the need for a more aggressive or extended therapy to increase the probability of obtaining sobriety
• A tool for treatment response to medications
Depression
30
Insomnia Panic
31
Anxiety
32

Insomnia and Early Morning Awakenings
33

Challenges in Treating Complex Patients
Diagnosis often symptomatic in
Psychiatry
Diagnosis often symptomatic in
Psychiatry
Patients may present with multiple
medication failures
Patients may present with multiple
medication failures
Medications can cause symptomsMedications can cause symptoms
Patients lose trust in practitioner
Patients lose trust in practitioner
Lost quality of life secondary to persistent symptoms
Lost quality of life secondary to persistent symptoms
Poor work productivityPoor work productivity
Relational issues with families and
coworkers
Relational issues with families and
coworkers
35
Fatigue
Optimal Range
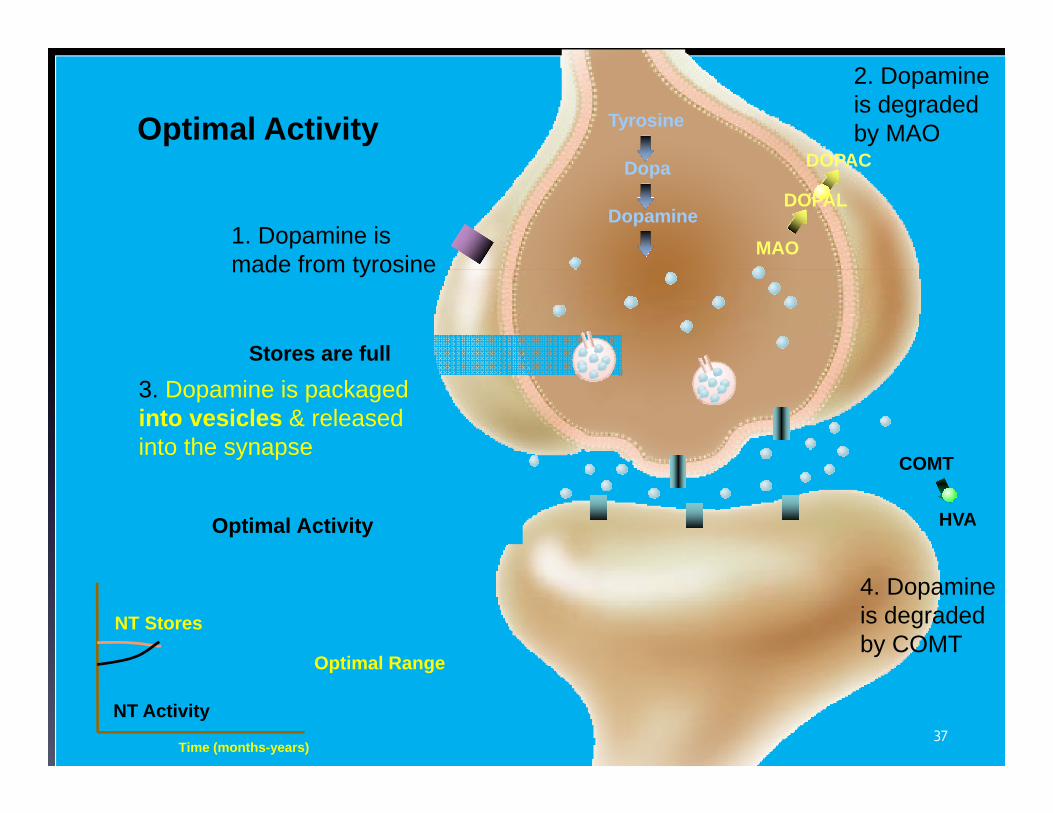
Optimal Activity
Tyrosine
Dopa
Dopamine
COMT
HVA
MAO
DOPAL
DOPACOptimal Activity
Stores are full
NT Stores
Time (months-years)
1. Dopamine is made from tyrosine
2. Dopamine is degraded by MAO
3. Dopamine is packaged into vesicles & released into the synapse
4. Dopamine is degraded by COMT
NT Activity37
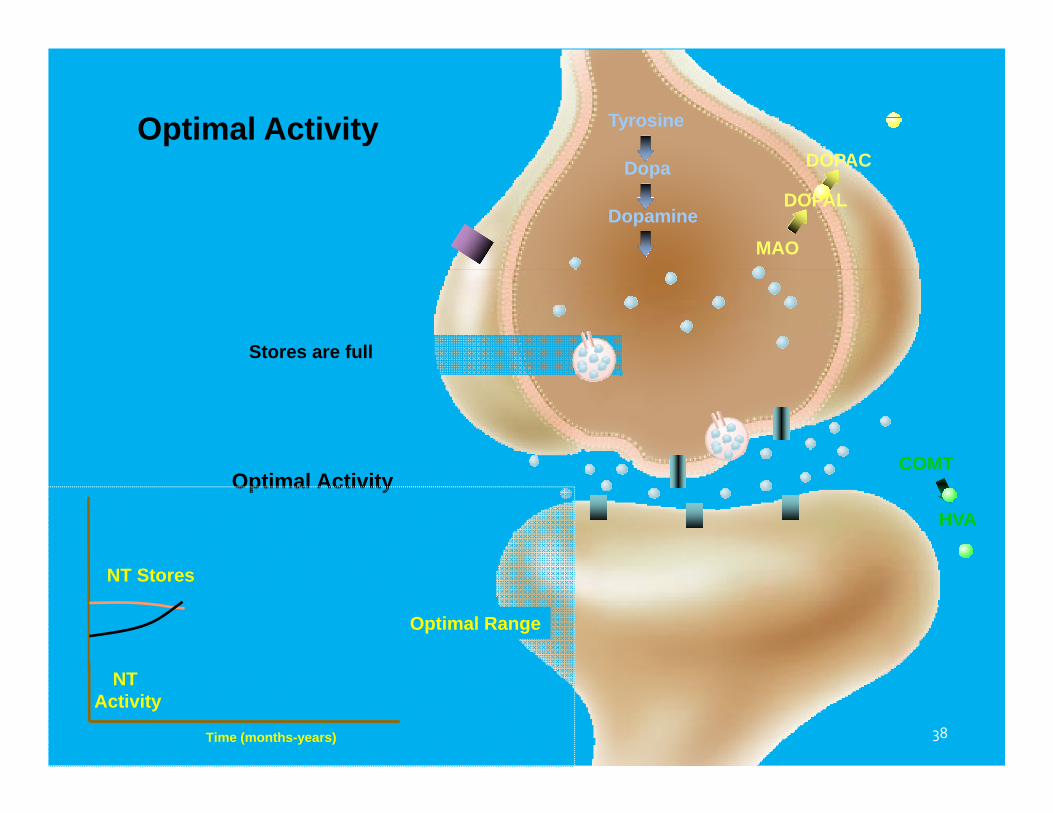
Optimal Activity
Tyrosine
Dopa
Dopamine
COMT
HVA
MAO
DOPAL
DOPAC
Stores are full
Optimal Activity
NT Stores
Time (months-years)
NT Activity
Optimal Range
38
Time (months-years)
Optimal Range
NT Activity
NT Stores
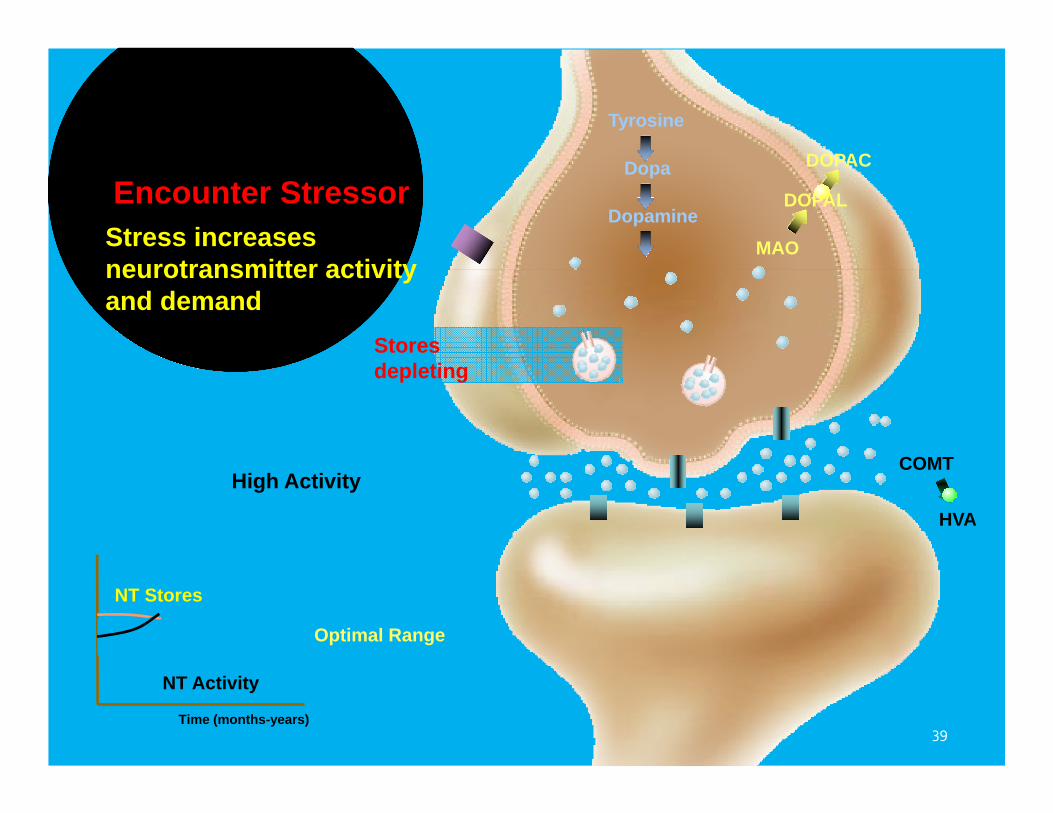
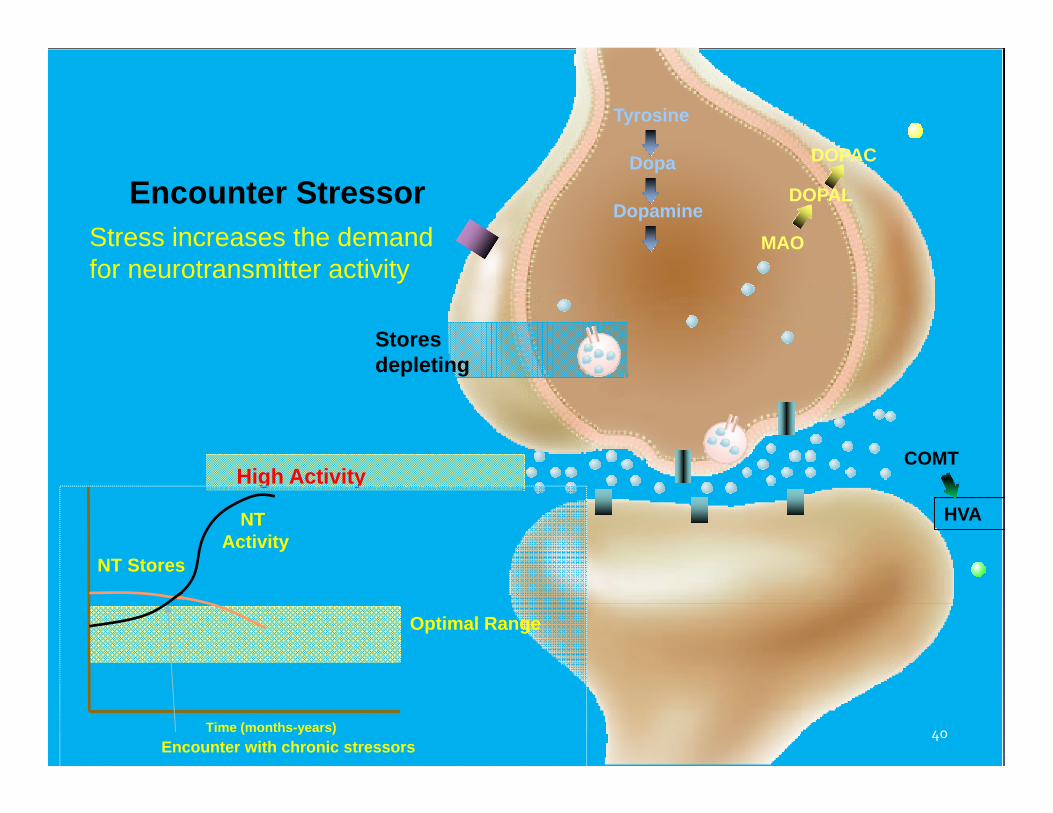
High Activity
Tyrosine
Dopa
DopamineMAO
DOPAL
DOPAC
Encounter Stressor
Stores depleting
COMT
HVA
Stress increasesneurotransmitter activity and demand
39
High Activity
Tyrosine
Dopa
DopamineMAO
DOPAL
DOPAC
Stores depleting
COMT
HVA
Optimal Range
Time (months-years)Encounter with chronic stressors
Encounter StressorStress increases the demandfor neurotransmitter activity
NT Stores
NT Activity
40
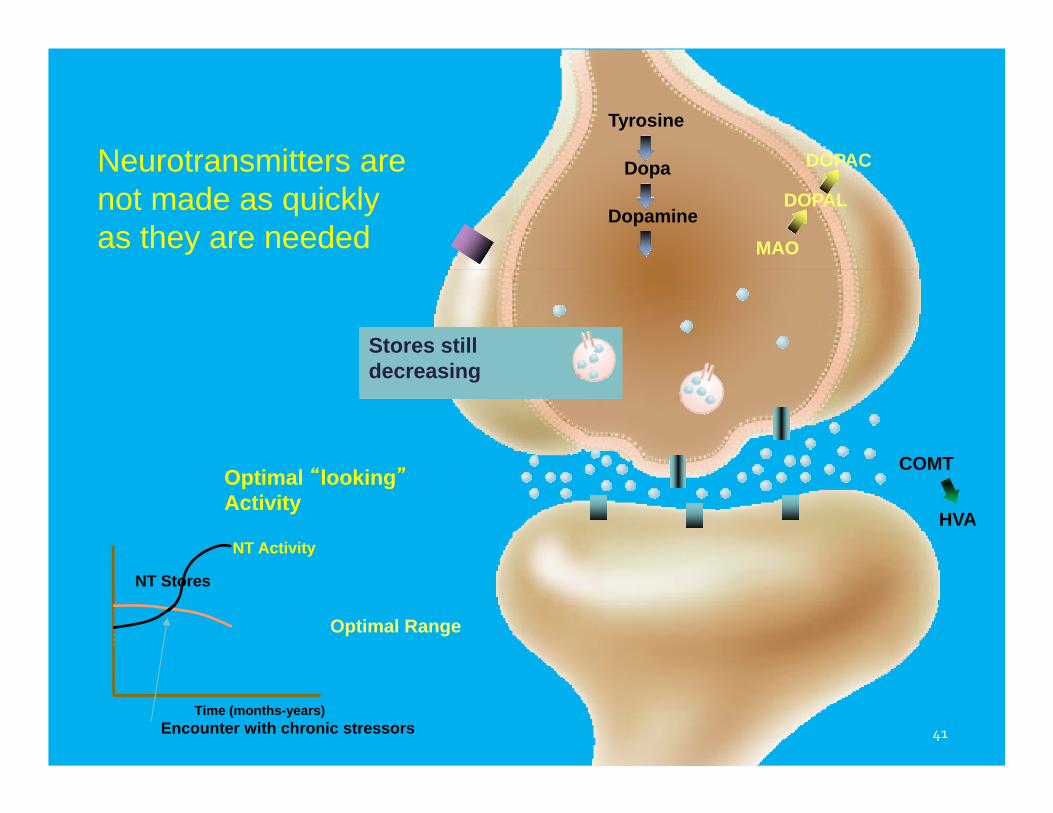
Optimal “looking”Activity
Tyrosine
Dopa
Dopamine
COMT
HVA
MAO
DOPAL
DOPAC
Stores still decreasing
Time (months-years)
Optimal Range
NT Activity
NT Stores
Encounter with chronic stressors
Neurotransmitters are not made as quickly as they are needed
41
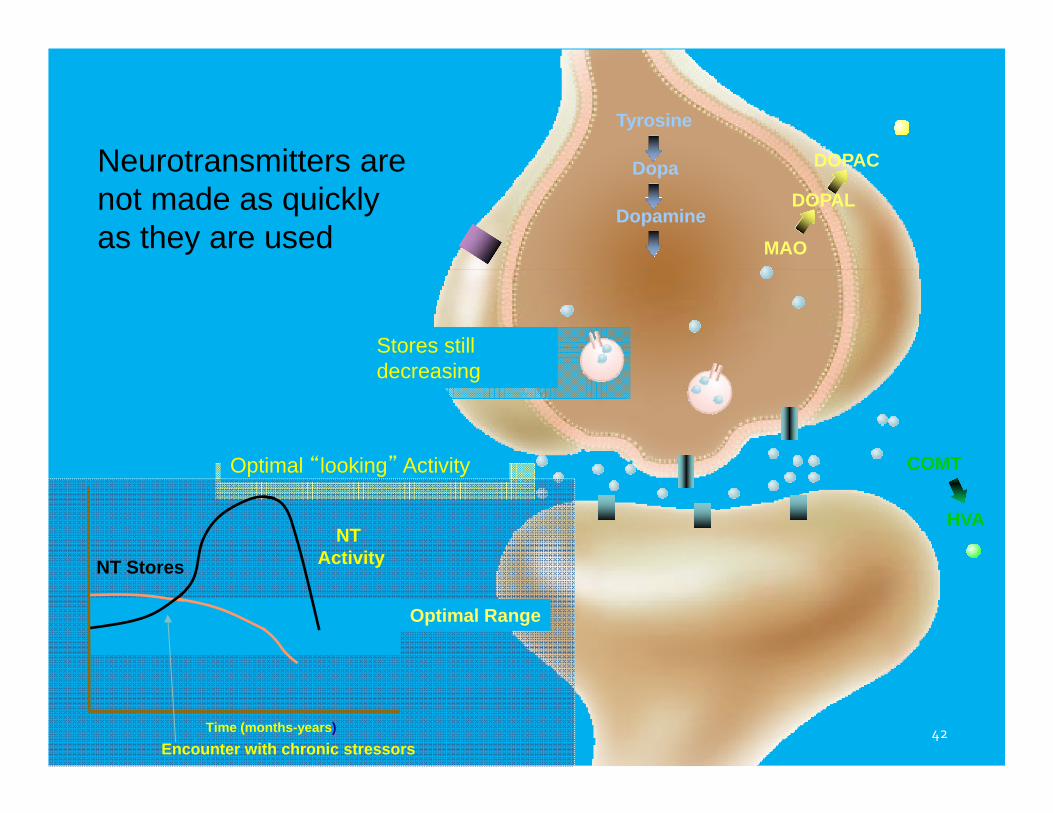
Optimal “looking” Activity
Tyrosine
Dopa
Dopamine
COMT
HVA
MAO
DOPAL
DOPAC
Stores still decreasing
Optimal Range
Encounter with chronic stressors
NT Stores
Neurotransmitters are not made as quickly as they are used
Time (months-years)
NT Activity
42
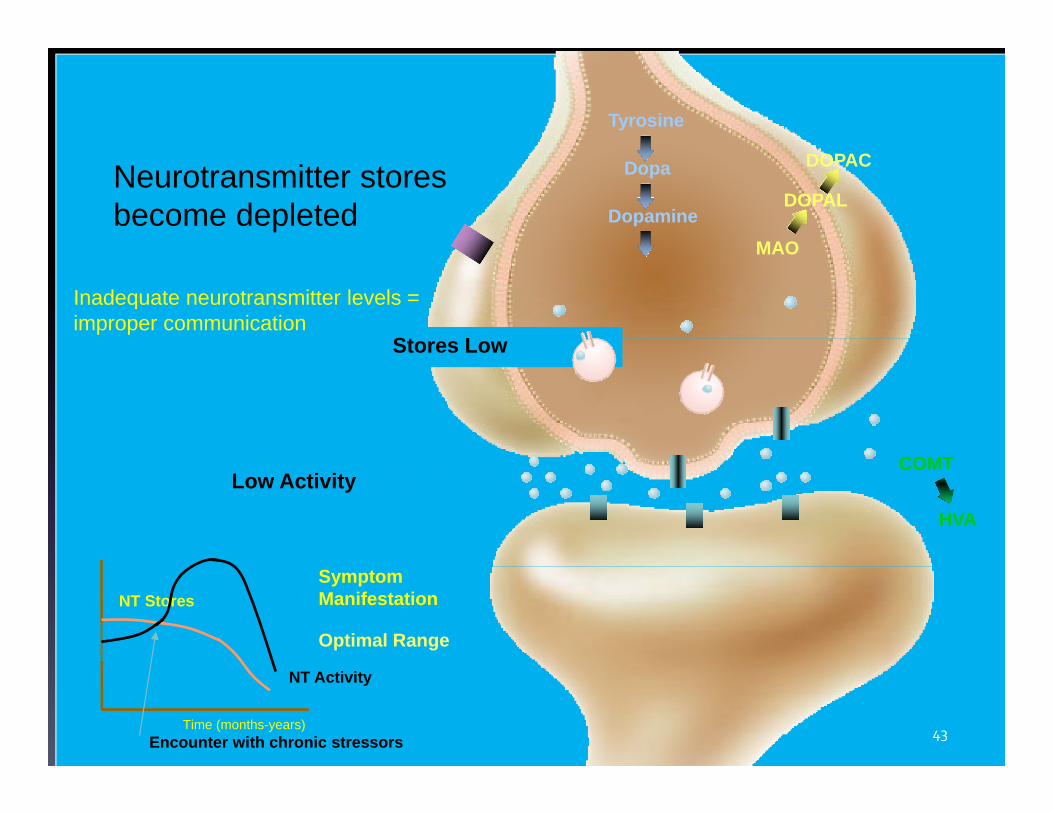
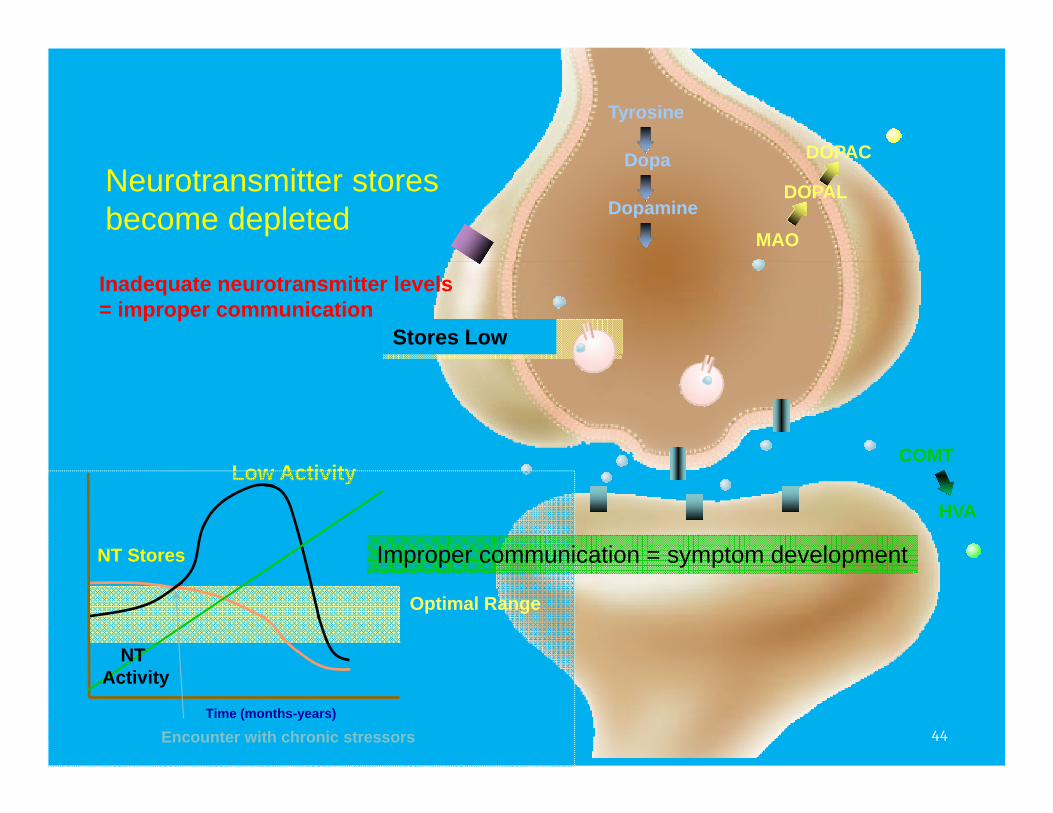
Low Activity
Tyrosine
Dopa
Dopamine
COMT
HVA
MAO
DOPAL
DOPAC
Stores Low
Time (months-years)
Optimal Range
SymptomManifestation
NT Activity
NT Stores
Encounter with chronic stressors
Neurotransmitter stores become depleted
Inadequate neurotransmitter levels = improper communication
43
Low Activity
Tyrosine
Dopa
Dopamine
COMT
HVA
MAO
DOPAL
DOPAC
Stores Low
Optimal Range
Encounter with chronic stressors
NT Stores
Time (months-years)
Neurotransmitter stores become depleted
Improper communication = symptom development
NT Activity
Inadequate neurotransmitter levels = improper communication
44
Recognizing Neurotransmitter Patterns
45
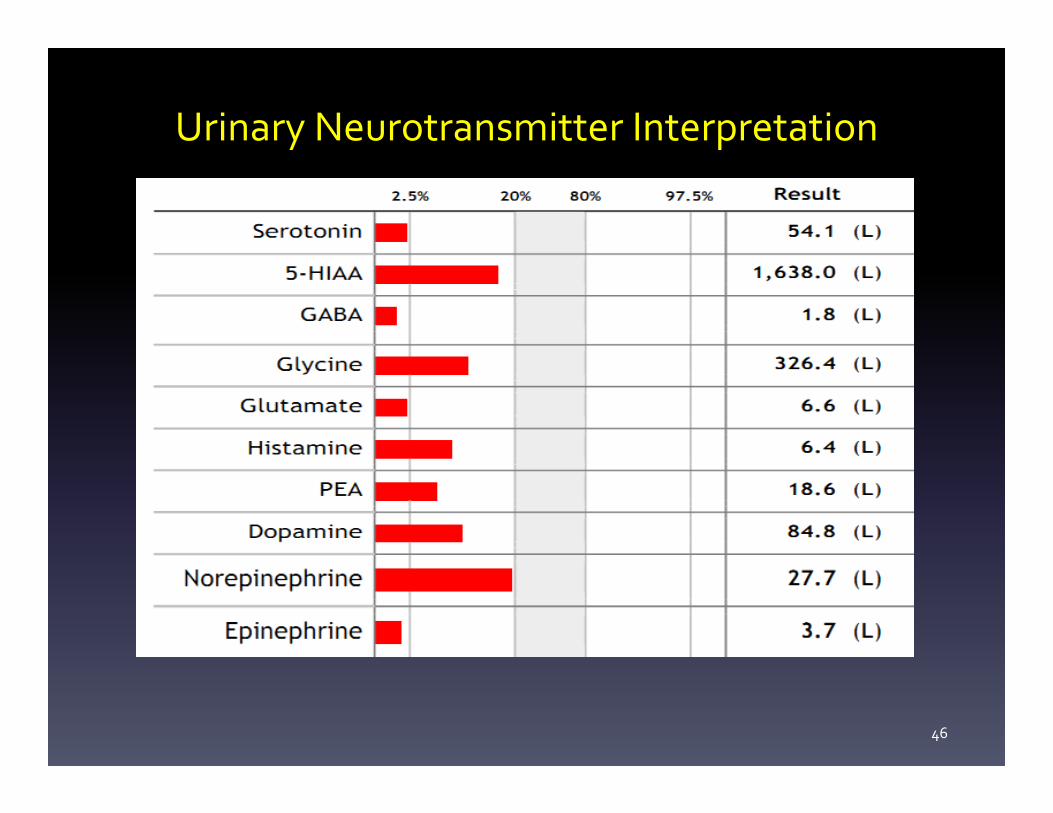
Urinary Neurotransmitter Interpretation
46
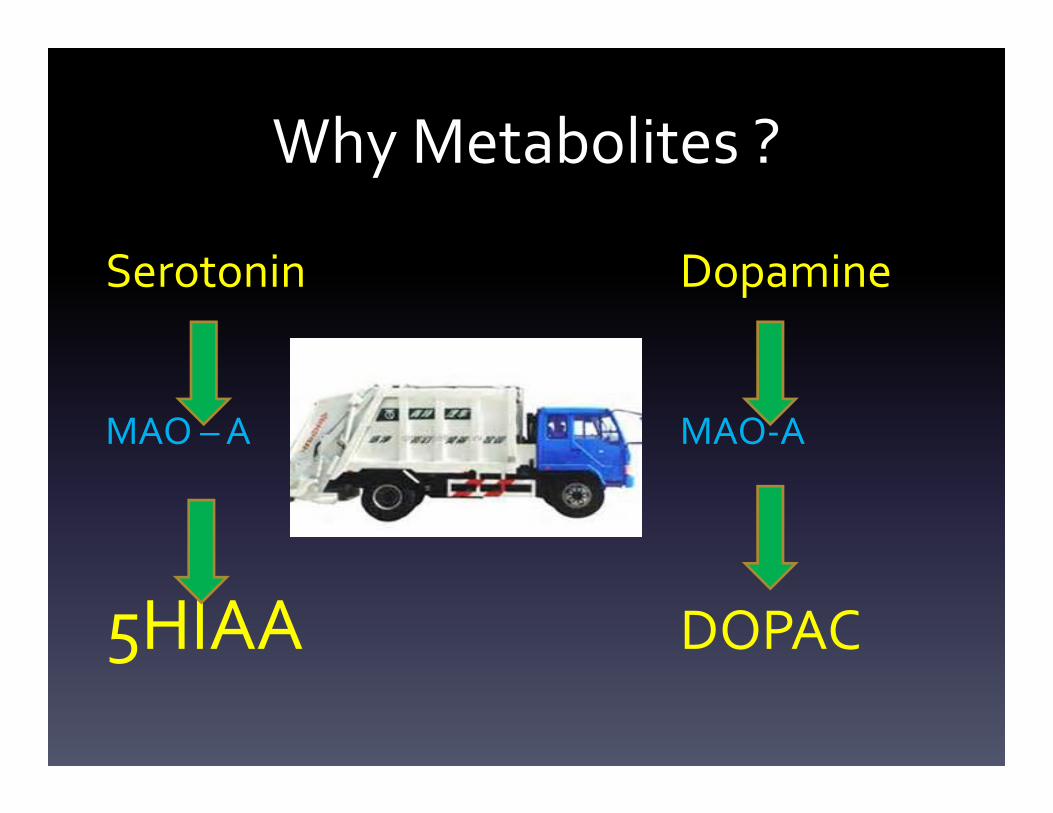
Why Metabolites ?
Serotonin Dopamine
MAO –A MAO‐A
5HIAA DOPAC
Meet the Neurotransmitters
48
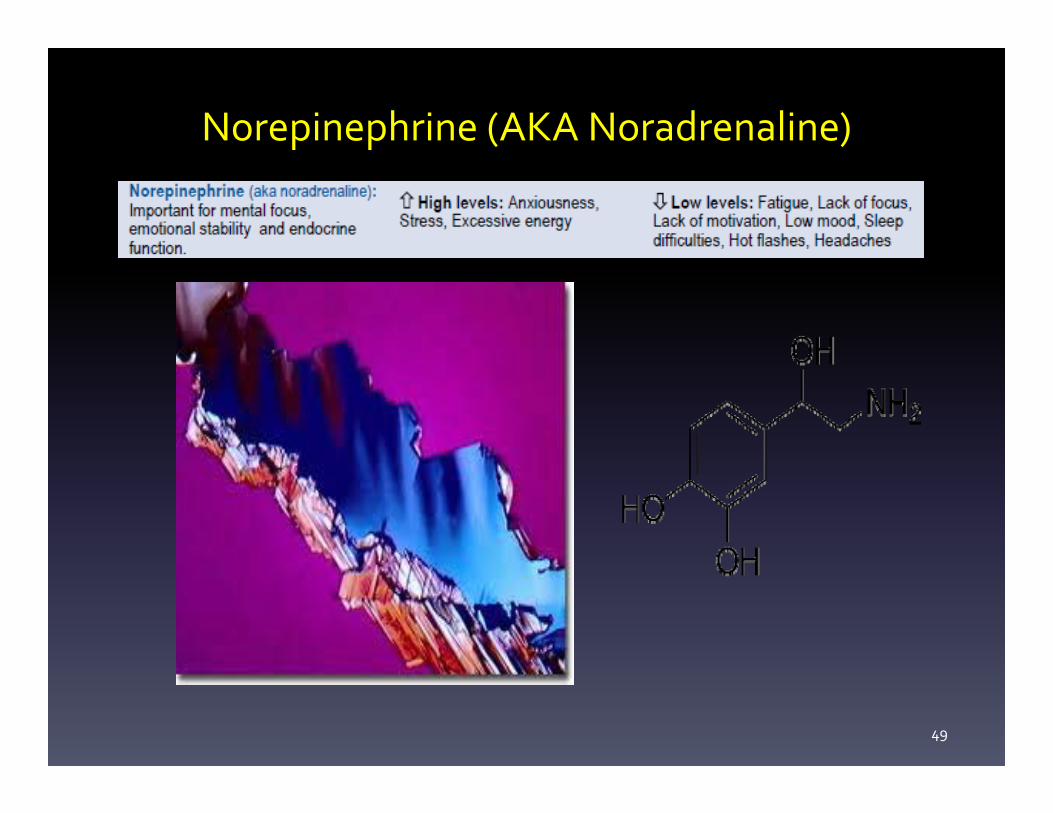
Norepinephrine (AKA Noradrenaline)
49
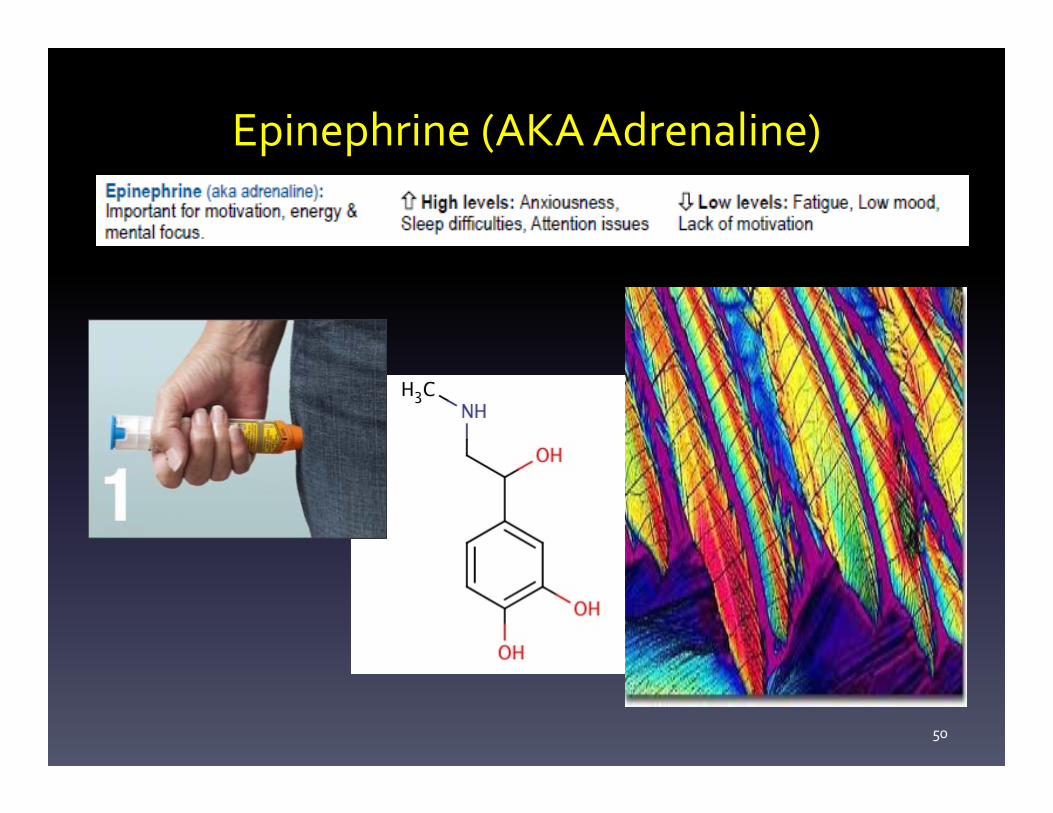
Epinephrine (AKA Adrenaline)
50
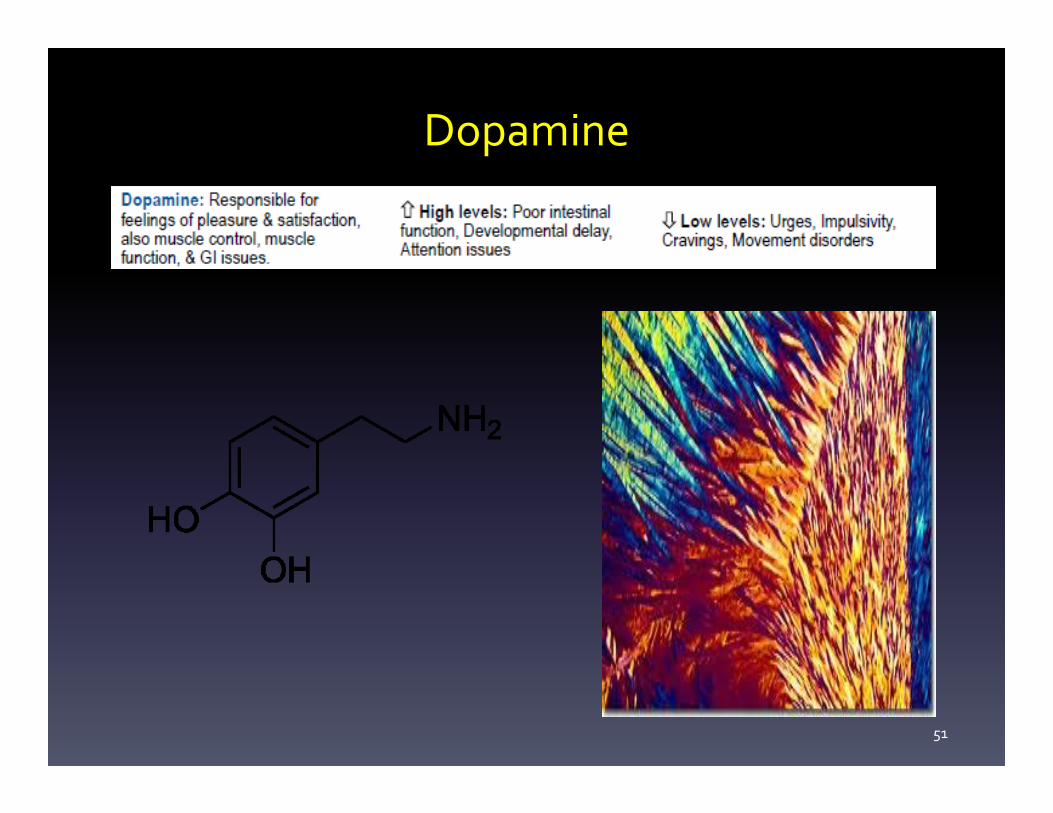
Dopamine
51

Glutamate
52
Glutamate is involved in Depression
“Coverging lines of evidence indicate that the glutamatergic system might be a promising target for a novel antidepressant therapy.”
“Coverging lines of evidence indicate that the glutamatergic system might be a promising target for a novel antidepressant therapy.”
Palucha, A, et al. (2005) Drug News and Perspectives. 18(4):262.
53

PEA (Phenylethylamine)
54
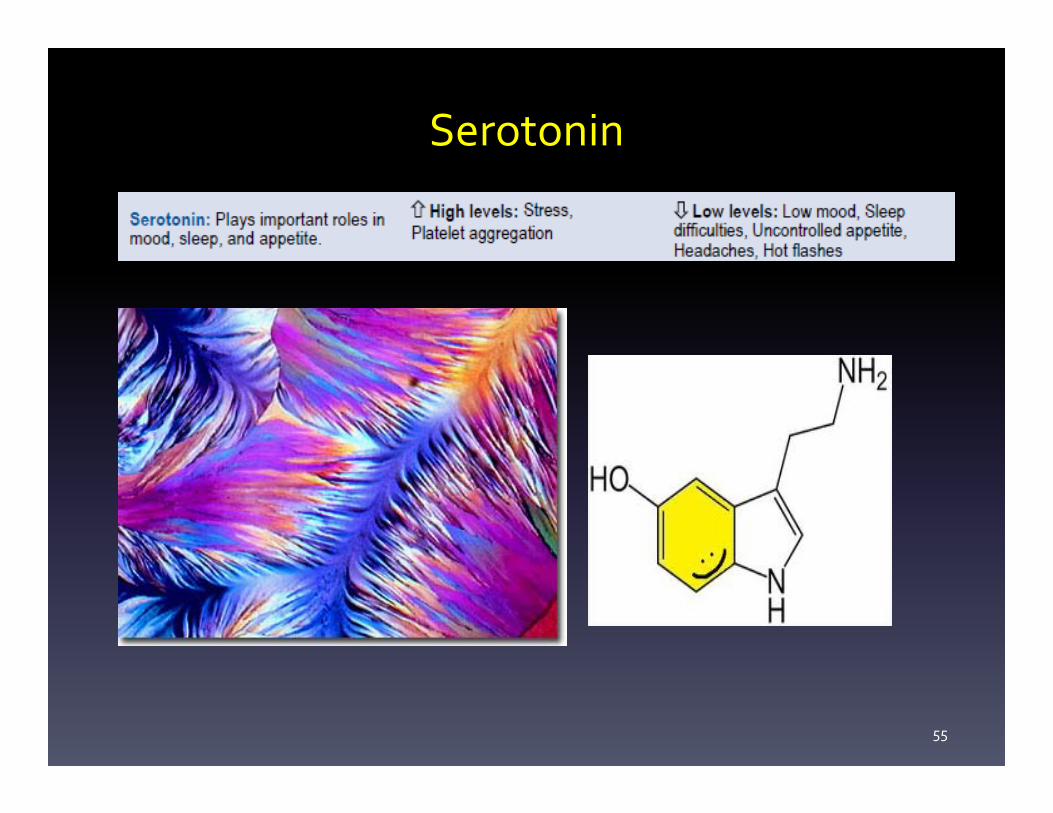
Serotonin
55
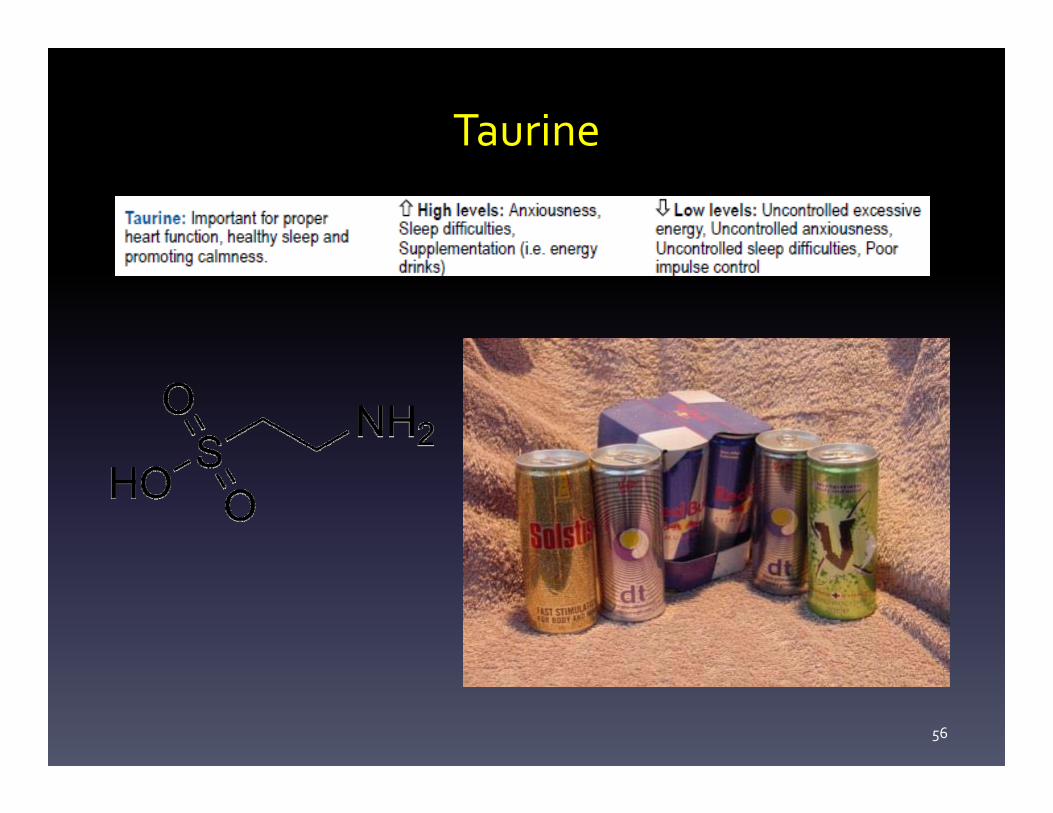
Taurine
56
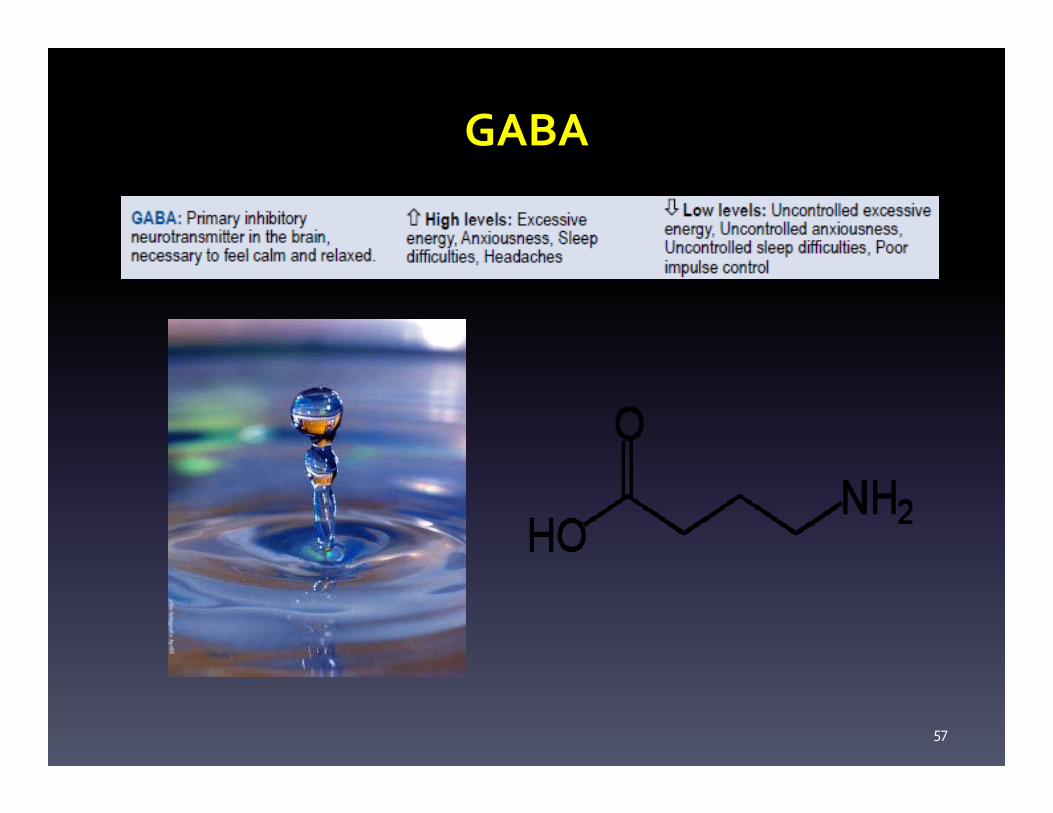
GABA
57

Glycine
58
Histamine
59
Recognizing Neurotransmitter Patterns
60
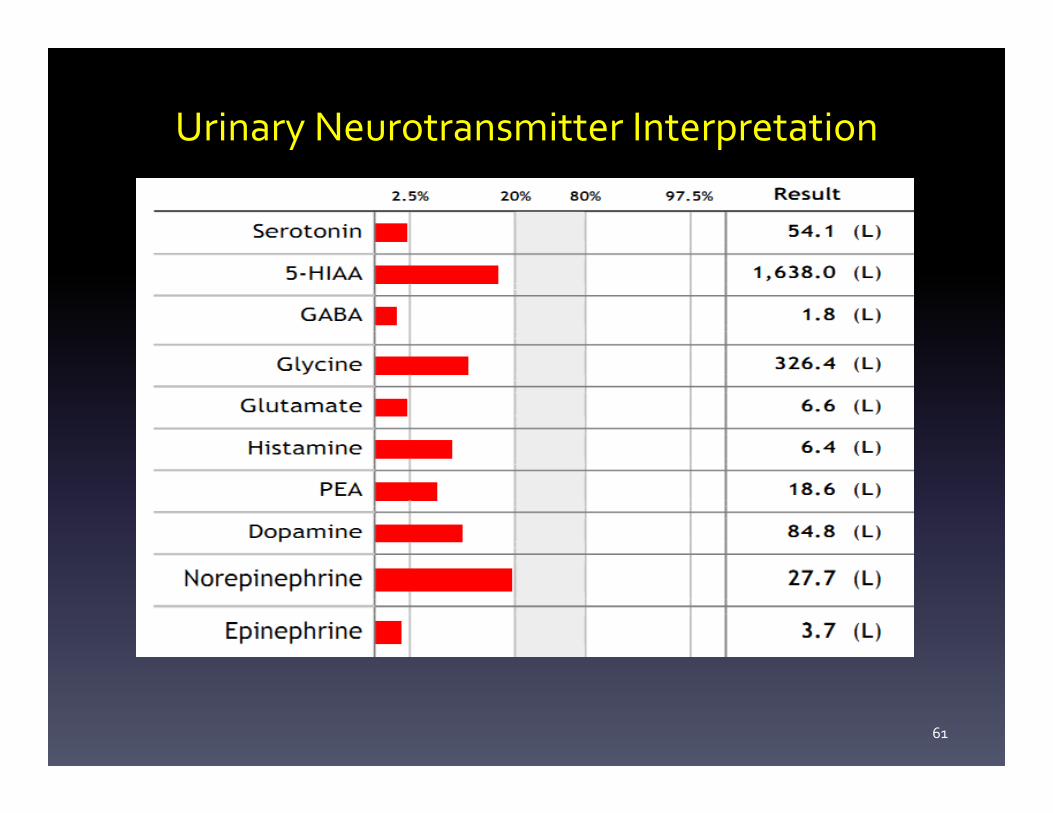
Urinary Neurotransmitter Interpretation
61
62
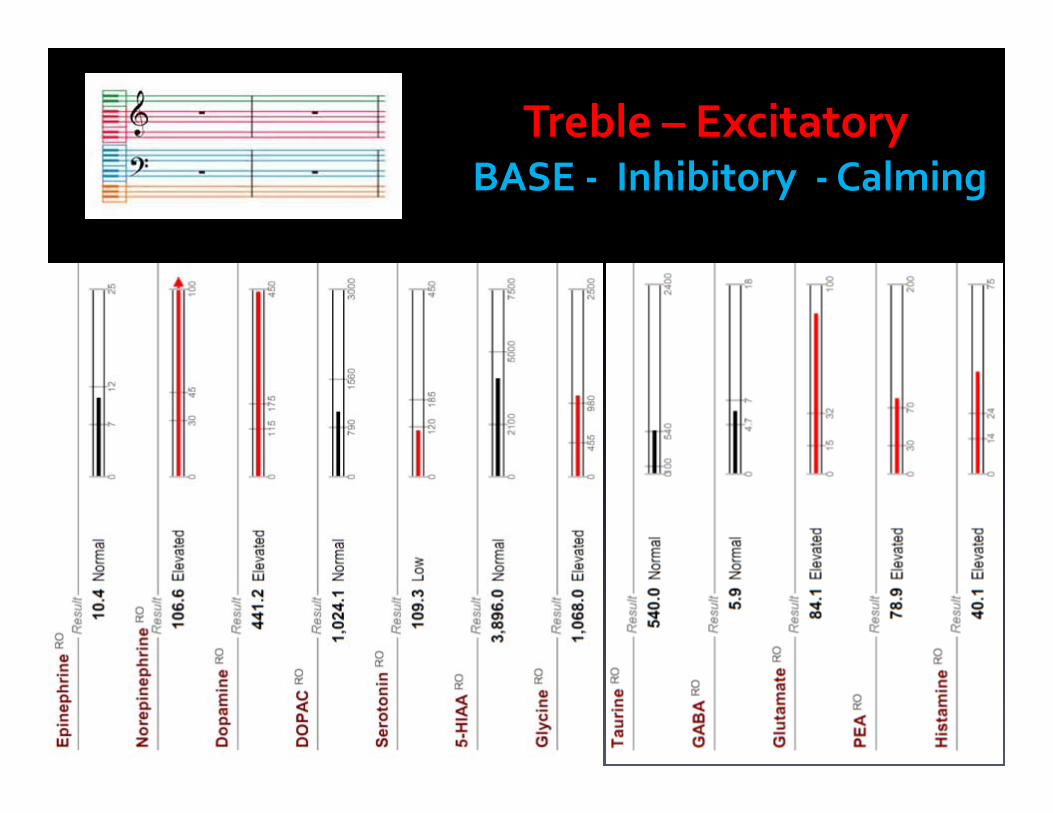
Treble – Excitatory BASE ‐ Inhibitory ‐Calming

Treble – Excitatory(usually)
Norepinephrine
Epinephrine
Dopamine
Glutamate
PEA
Histamine
Cortisol

BASE ‐ Inhibitory ‐Calming(usually)
• GABA
• Serotonin
• Glycine
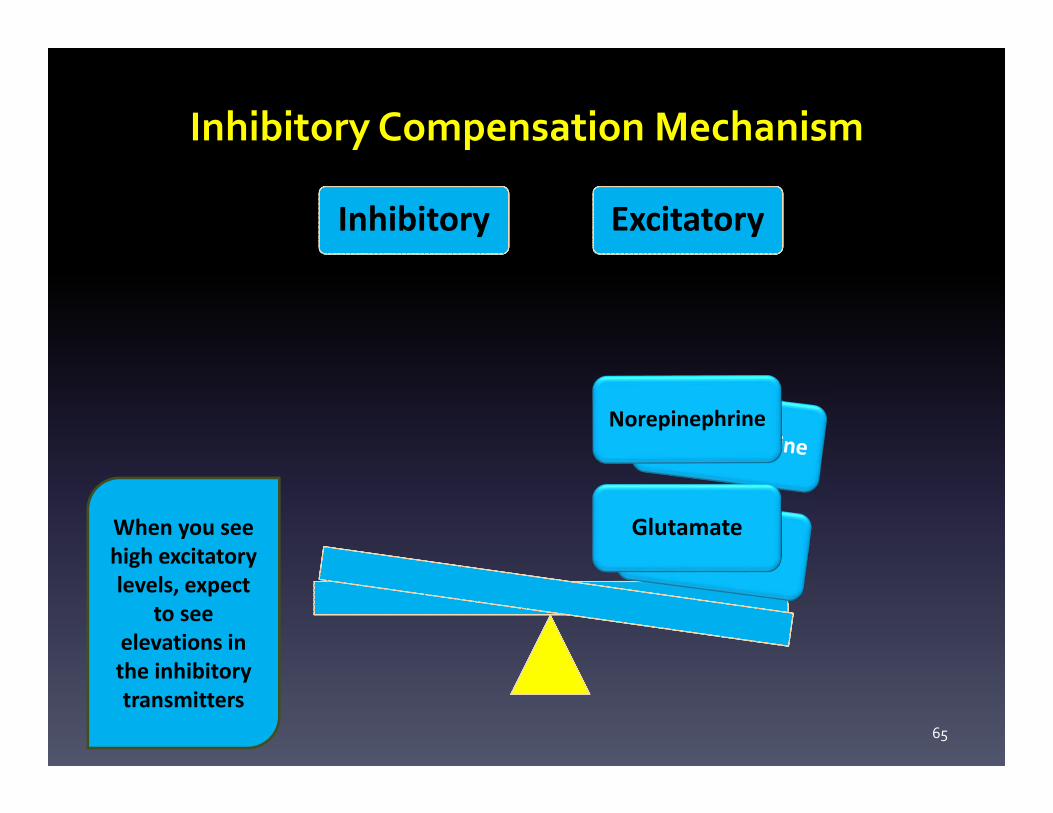
Inhibitory Compensation Mechanism
65
InhibitoryInhibitory ExcitatoryExcitatory
GlutamateWhen you see high excitatory levels, expect
to see elevations in the inhibitory transmitters
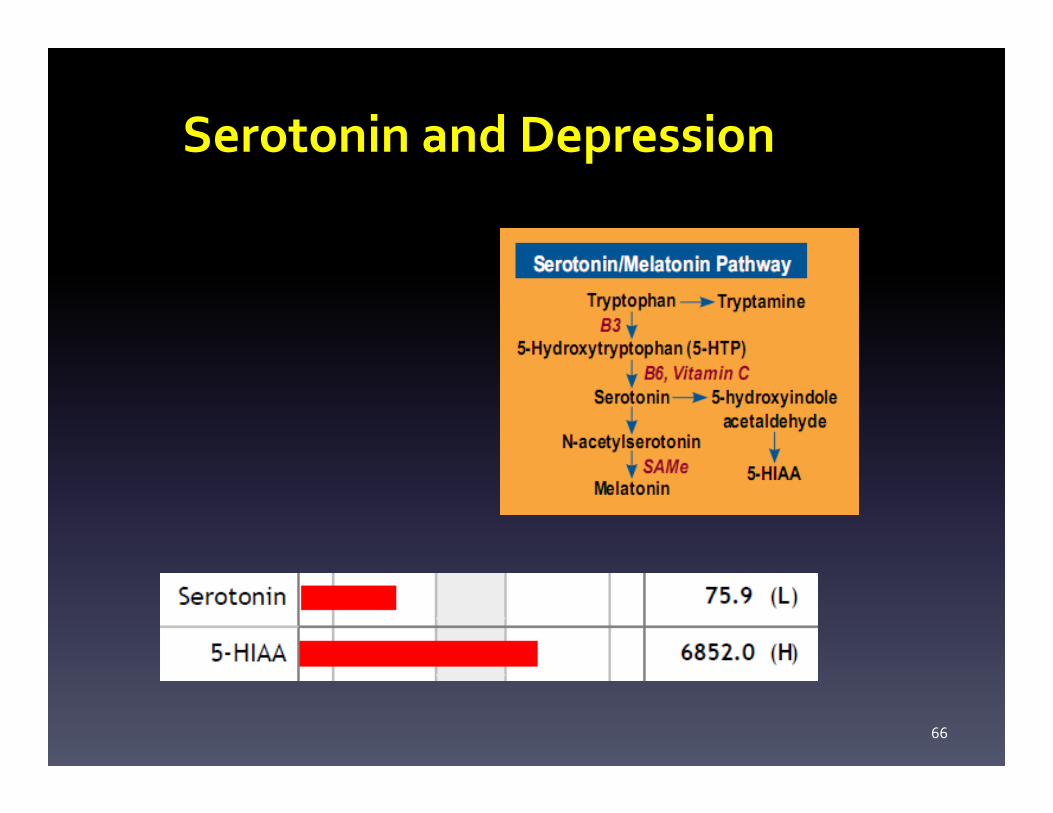
Serotonin and Depression
66
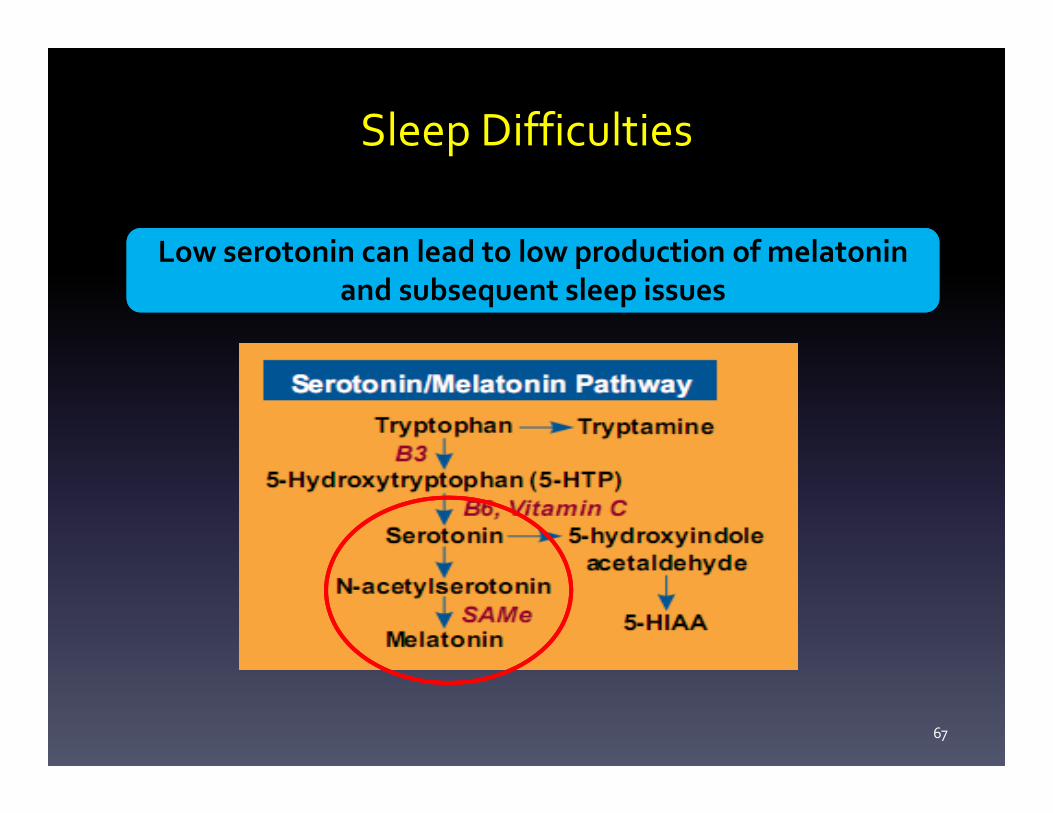
Sleep Difficulties
67
Low serotonin can lead to low production of melatonin and subsequent sleep issues
Low serotonin can lead to low production of melatonin and subsequent sleep issues
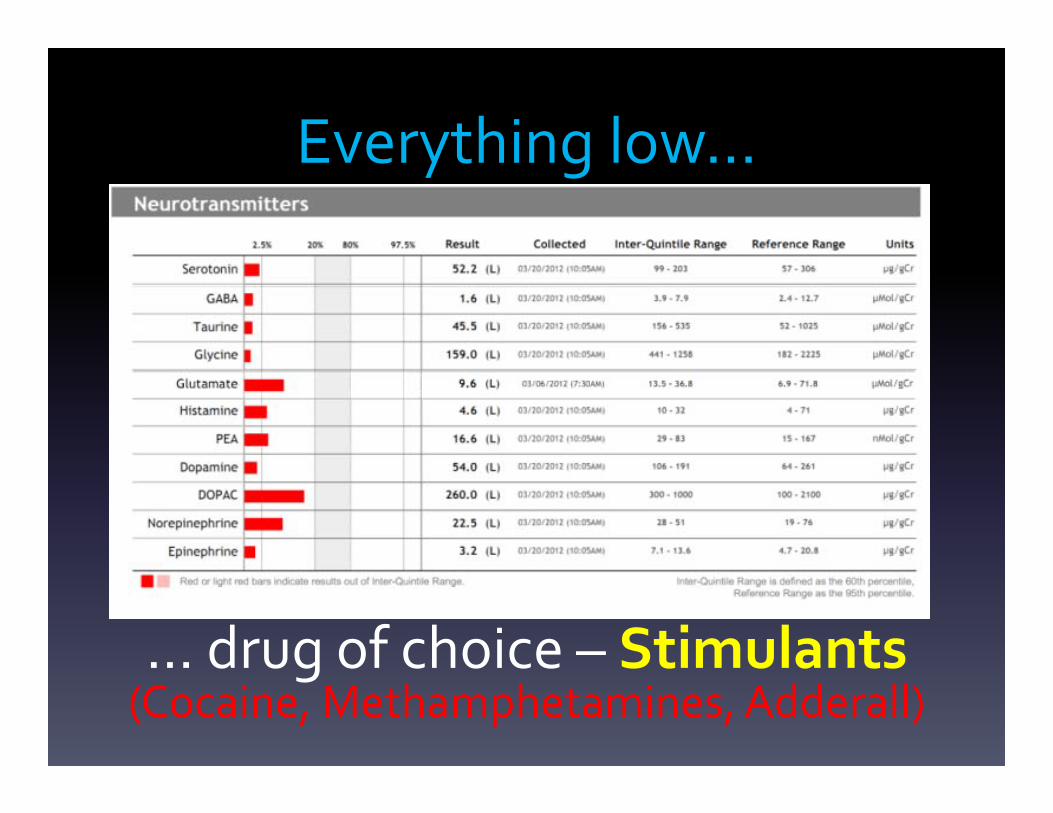
Everything low…
… drug of choice – Stimulants(Cocaine, Methamphetamines, Adderall)
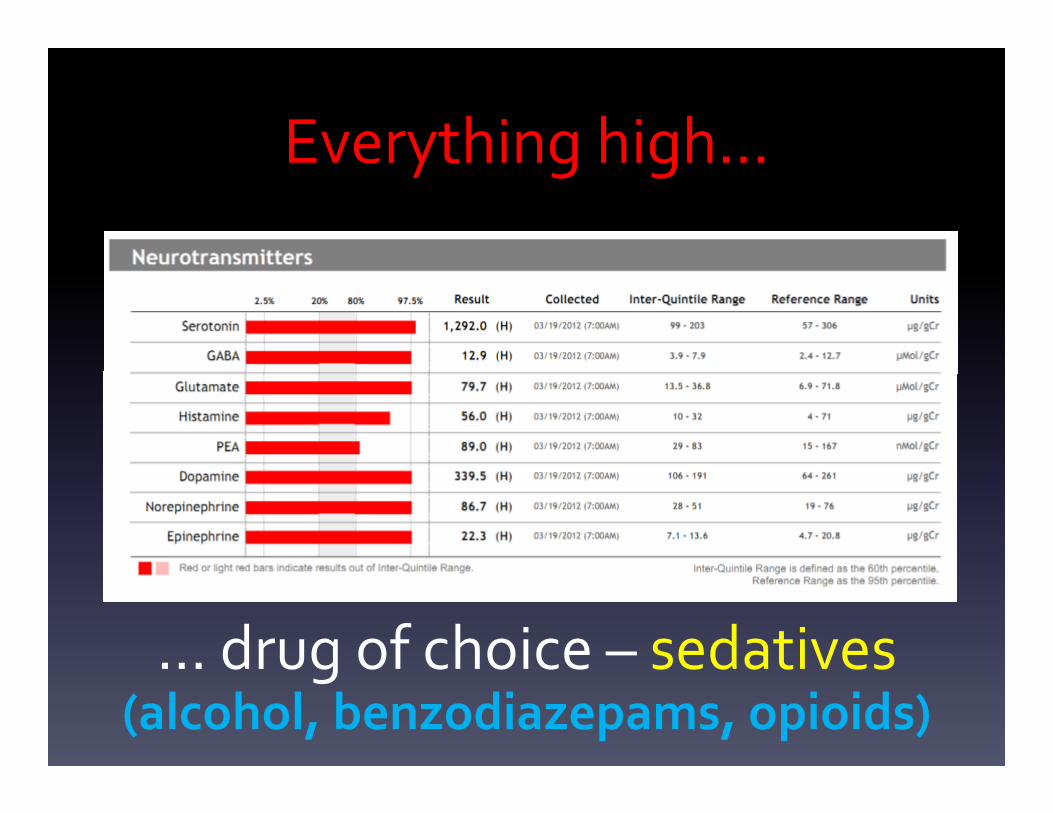
Everything high…
… drug of choice – sedatives(alcohol, benzodiazepams, opioids)
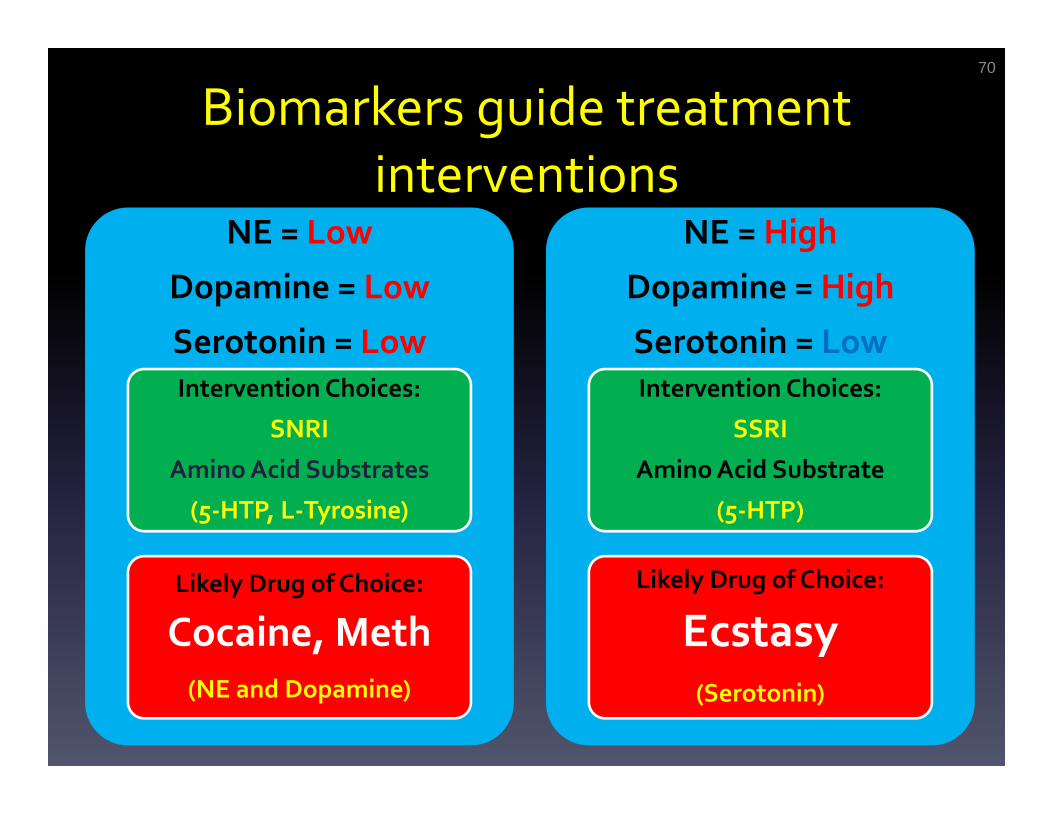
Biomarkers guide treatment interventions
70
NE = Low
Dopamine = Low
Serotonin = LowIntervention Choices:
SNRI
Amino Acid Substrates
(5‐HTP, L‐Tyrosine)
Likely Drug of Choice:
Cocaine, Meth (NE and Dopamine)
NE = High
Dopamine = High
Serotonin = LowIntervention Choices:
SSRI
Amino Acid Substrate
(5‐HTP)
Likely Drug of Choice:
Ecstasy(Serotonin)
Low GABA and Taurine
Imbalances such as low GABA and Taurine are
associated with anxiety, panic, insomnia and
clinically observed cravings for sedating drugs
(prescription or recreational) and/or alcohol.

Observed clinical patternsLow Serotonin – enjoys ecstasy
Low GABA – enjoys alcohol and benzdiazepines
Low PEA , NE, Dopamine– enjoys or abuses stimulants
High Dopamine – enjoys benzodiazepines, alcohol
High Taurine – metabolic issues
High Norepinephrine and Low Epinephrine – patient needs SAMe as cofactor
Low Serotonin and High 5‐HIAA –Consider 5HTP, SSRI, MAO‐Inhibitor
High Dopamine and Low Serotonin – increasing Serotonin will lower
Dopamine
High Dopamine and High Serotonin – must use antipsychotic to lower
dopamine
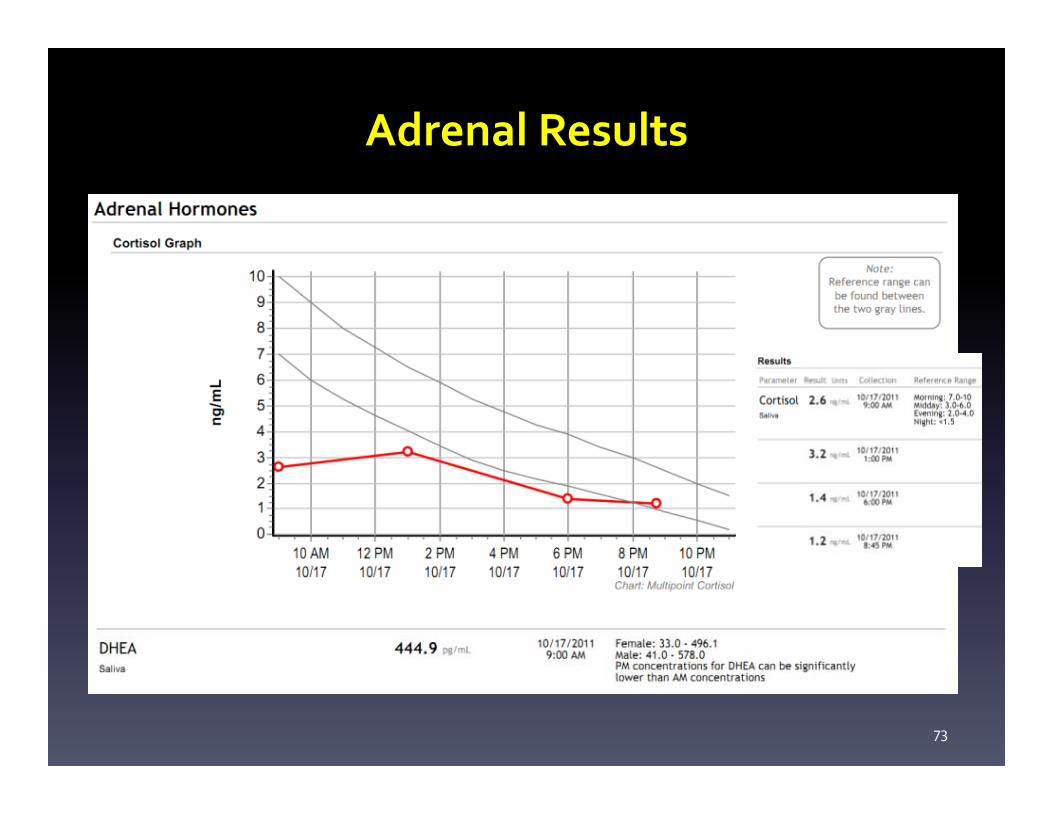
Adrenal Results
73

Modulating Adrenal/Cortisol Function
74
Phosphadityl Serine

Urinary norepinephrine correlates with severity of depression and anxiety
Hughes, JW, et al. (2004) J Psychosom Res. 57:353‐358.
“…higher levels of depression and anxiety symptoms are related to increased urinary norepinephine (NE) and cortisol (CORT) among women…”
“…higher levels of depression and anxiety symptoms are related to increased urinary norepinephine (NE) and cortisol (CORT) among women…”
75
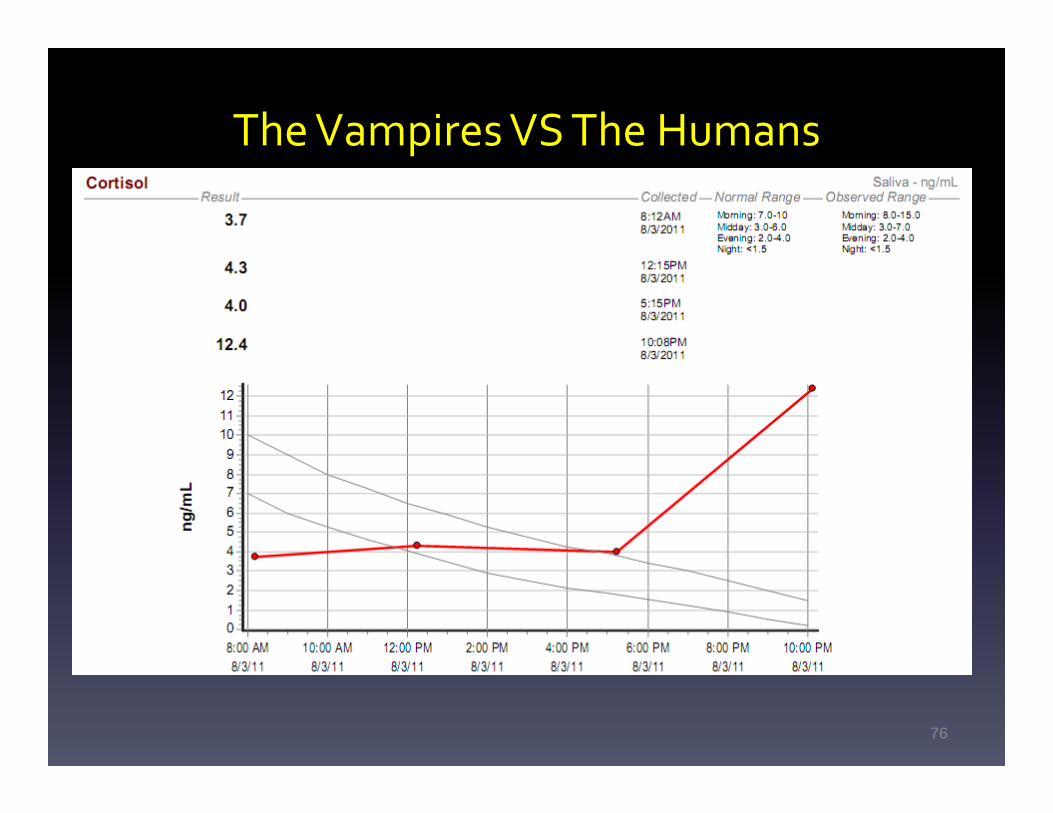
The Vampires VS The Humans
76

Rhodiola Supports Adrenal Function*
77
Low Dose RhodiolaAshagwanda
Holy Basil
Getting a Good Clinical Historyfor Neurotransmitter Correlation
78
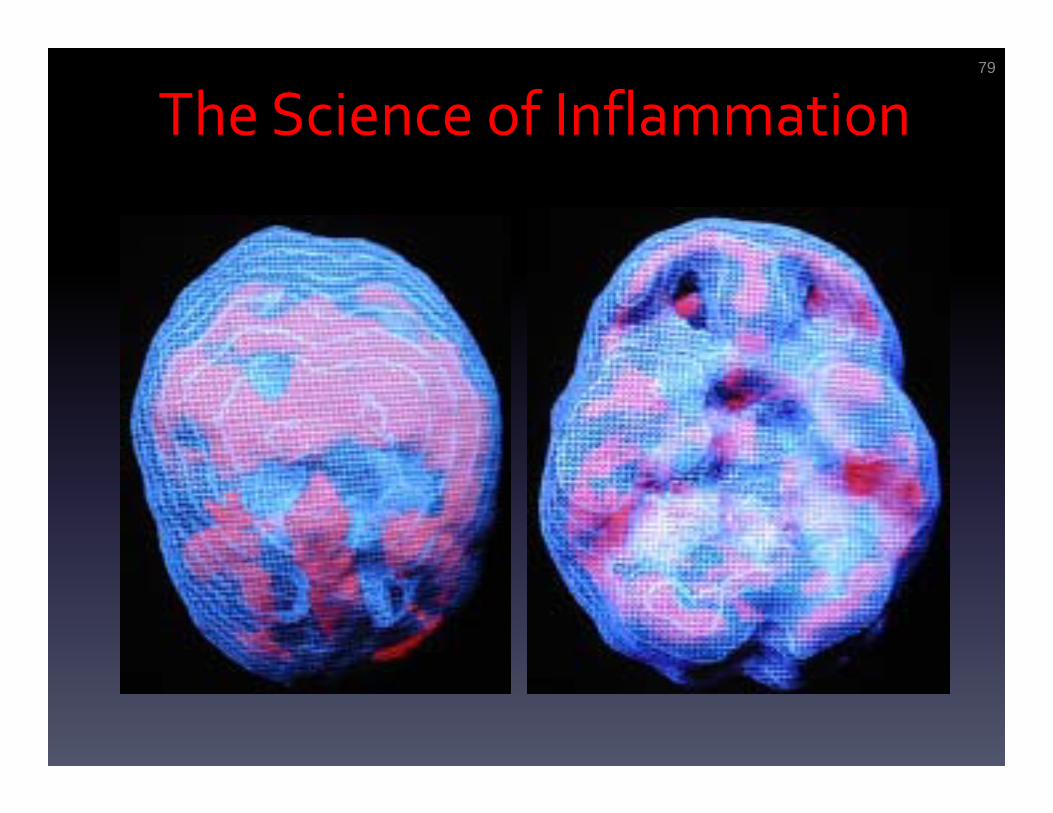
The Science of Inflammation79
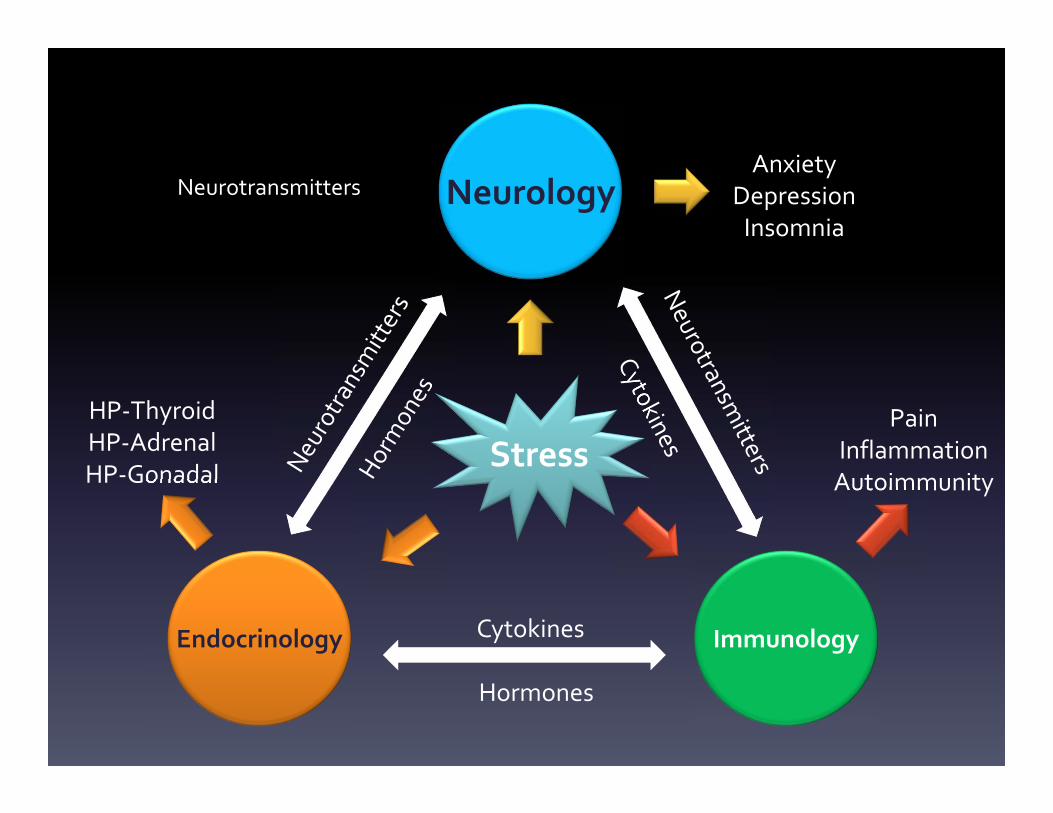
Hormones
Cytokines
AnxietyDepressionInsomnia
PainInflammationAutoimmunity
HP‐Thyroid HP‐AdrenalHP‐Gonadal
Endocrinology Immunology
Neurology
Stress
Neurotransmitters

Surface SPECTAt Rest Concentration
Internal SPECTat rest concentration

Finding Root Cause
• Food Sensitivities
Mold Toxicity Metals ToxicityBacterial/Viral
Lyme Disease
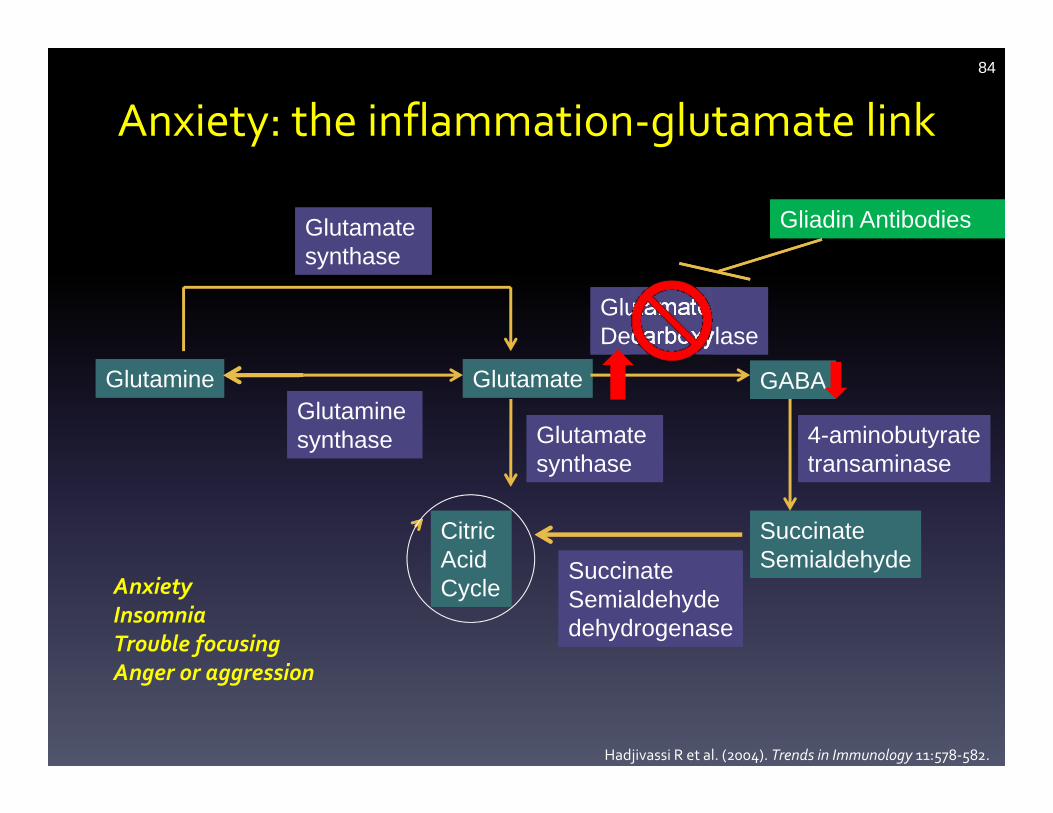
Anxiety: the inflammation‐glutamate link84
Gliadin AntibodiesGliadin Antibodies
AnxietyInsomniaTrouble focusingAnger or aggression
Hadjivassi R et al. (2004). Trends in Immunology 11:578‐582.
GlutamineGlutamine
SuccinateSemialdehydeSuccinateSemialdehyde
GlutamateGlutamateGlutamine synthaseGlutamine synthase
Glutamate synthaseGlutamate synthase
GABAGABA
Glutamate DecarboxylaseGlutamate Decarboxylase
4-aminobutyratetransaminase4-aminobutyratetransaminase
Succinate Semialdehydedehydrogenase
Succinate Semialdehydedehydrogenase
Citric AcidCycle
Citric AcidCycle
Glutamate synthaseGlutamate synthase

Is It Thyroid ?
Hi Normal / Low Normal can be symptomatic in psychiatric patients with a history of mood
disorders• TSH• Free T4• Free T3• TPO• Reverse T3
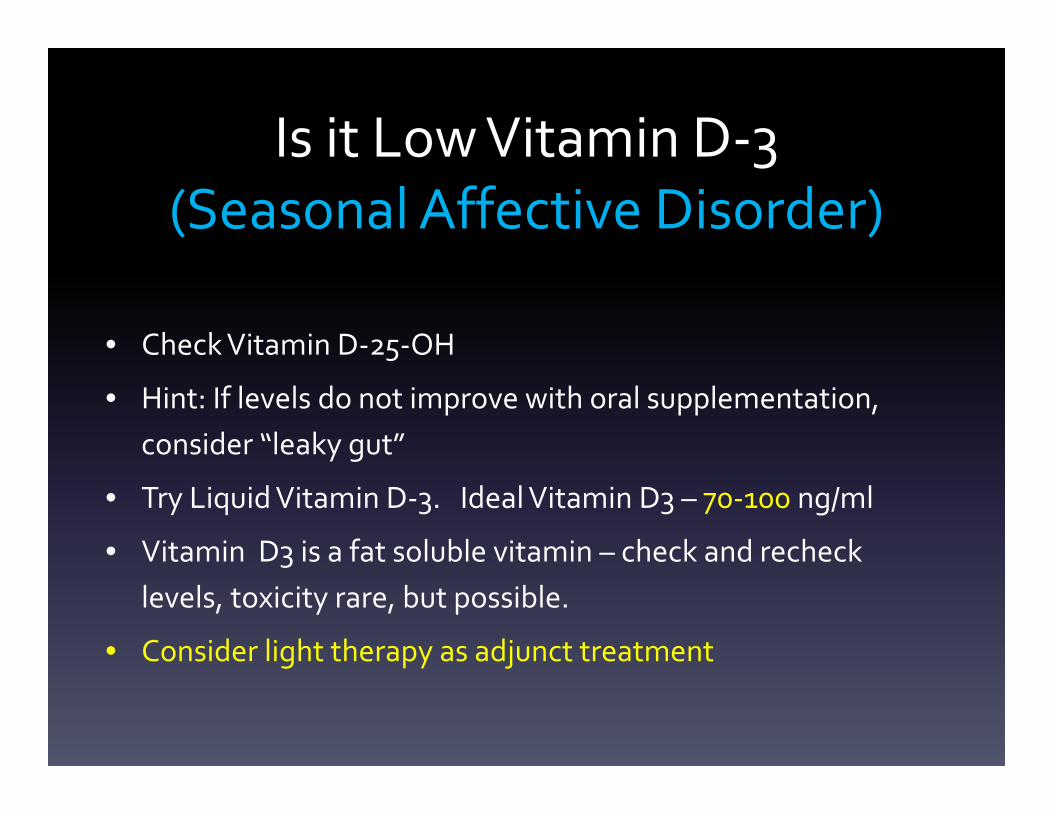
Is it Low Vitamin D‐3 (Seasonal Affective Disorder)
• Check Vitamin D‐25‐OH
• Hint: If levels do not improve with oral supplementation, consider “leaky gut”
• Try Liquid Vitamin D‐3. Ideal Vitamin D3 – 70‐100 ng/ml
• Vitamin D3 is a fat soluble vitamin – check and recheck levels, toxicity rare, but possible.
• Consider light therapy as adjunct treatment
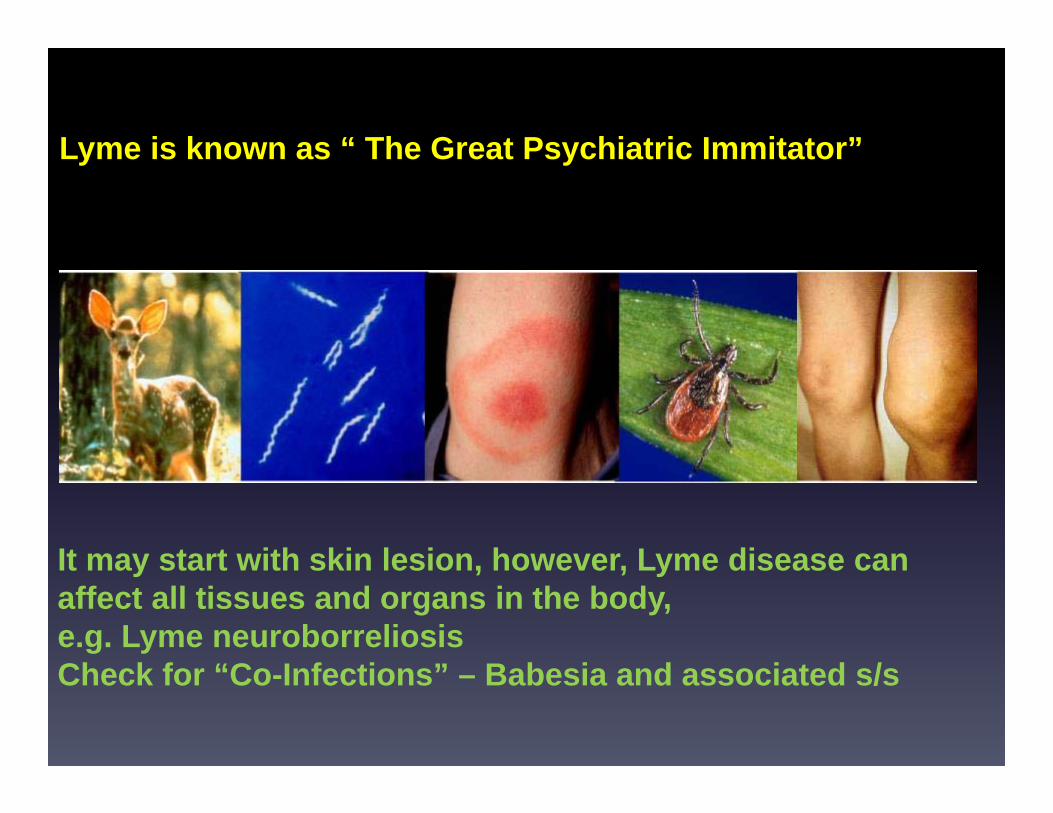
Lyme is defined as an infectious illness caused by tLyme is known as “ The Great Psychiatric Immitator”chete, Borrelia burgdorferi
It may start with skin lesion, however, Lyme disease can affect all tissues and organs in the body, e.g. Lyme neuroborreliosisCheck for “Co-Infections” – Babesia and associated s/s
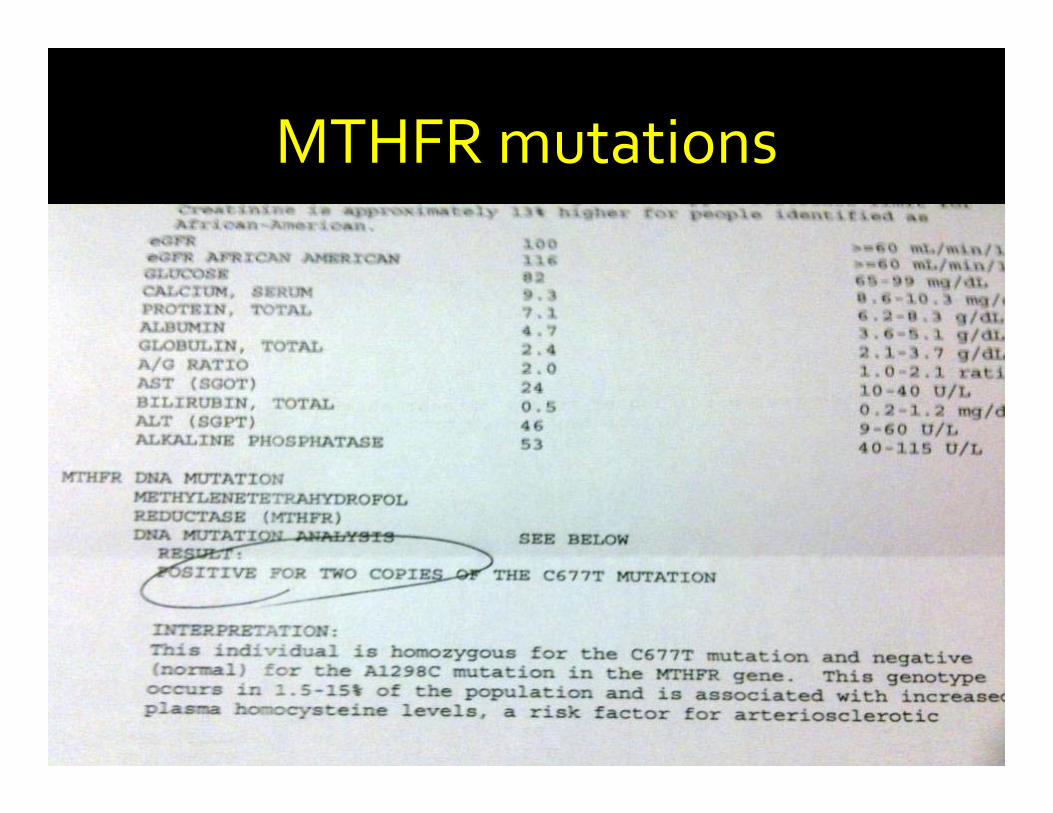
MTHFR mutations
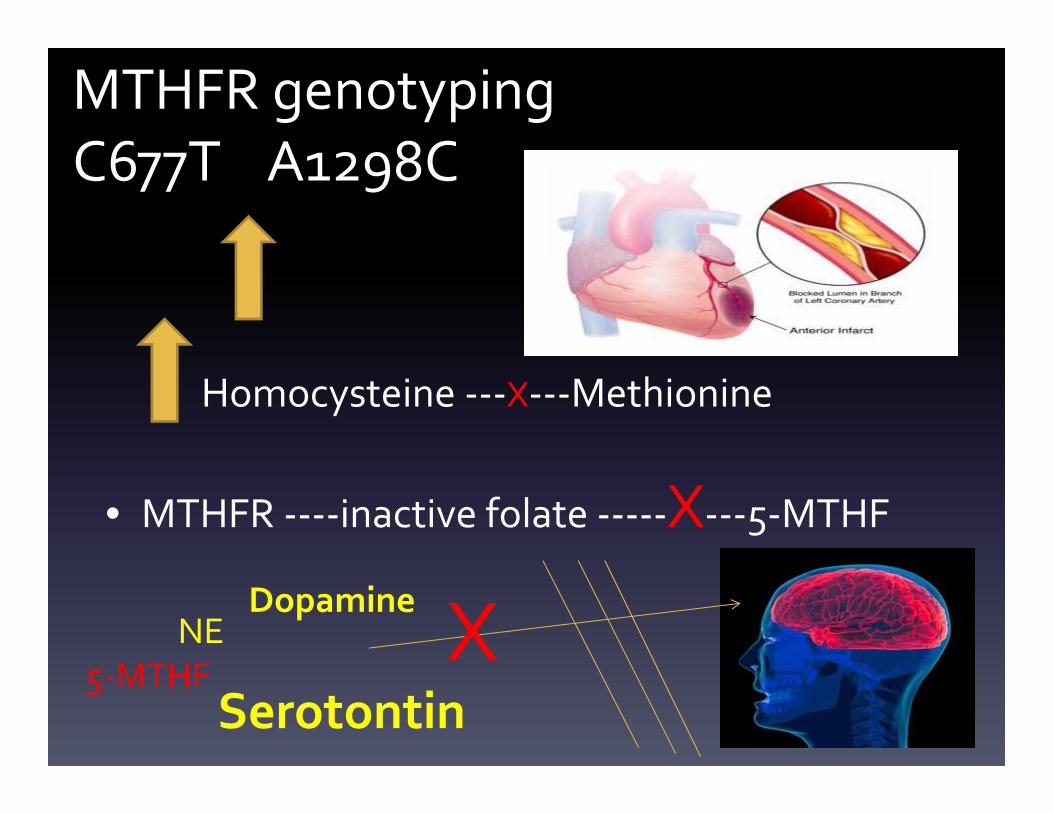
MTHFR genotypingC677T A1298C
Homocysteine ‐‐‐X‐‐‐Methionine
• MTHFR ‐‐‐‐inactive folate ‐‐‐‐‐X‐‐‐5‐MTHF
X5‐MTHF
NEDopamine
Serotontin
90
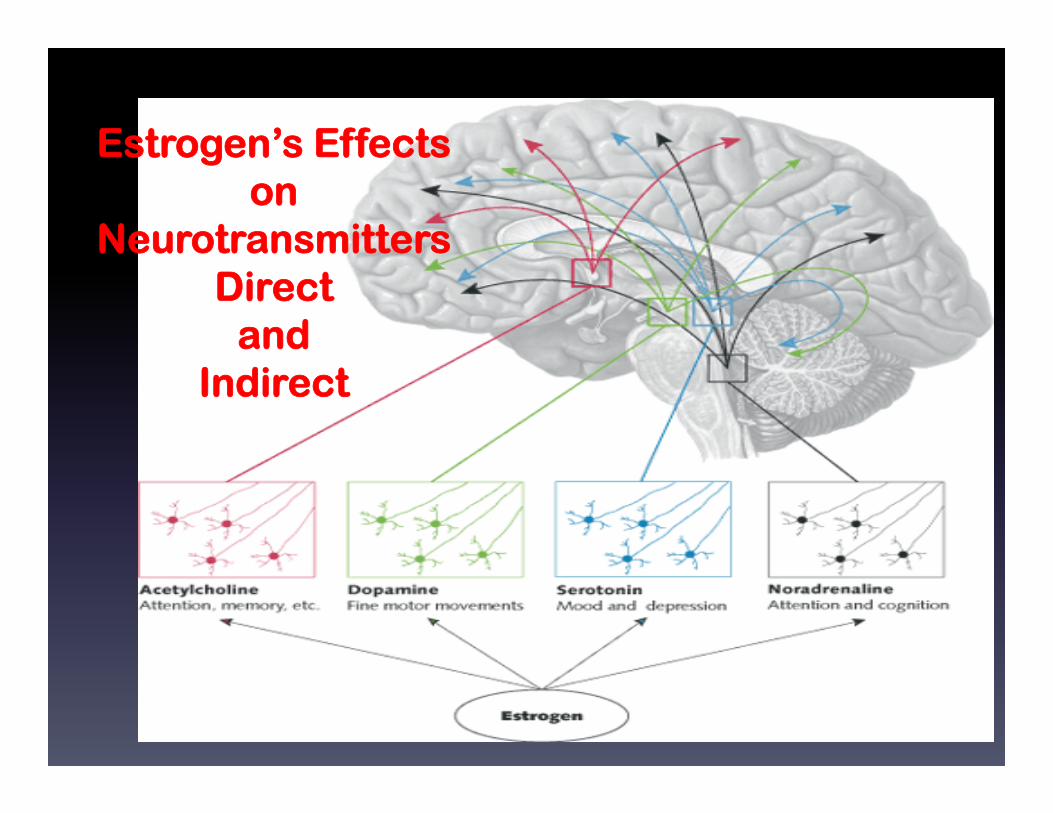
Estrogen’s Effects on
Neurotransmitters Direct
and Indirect

91
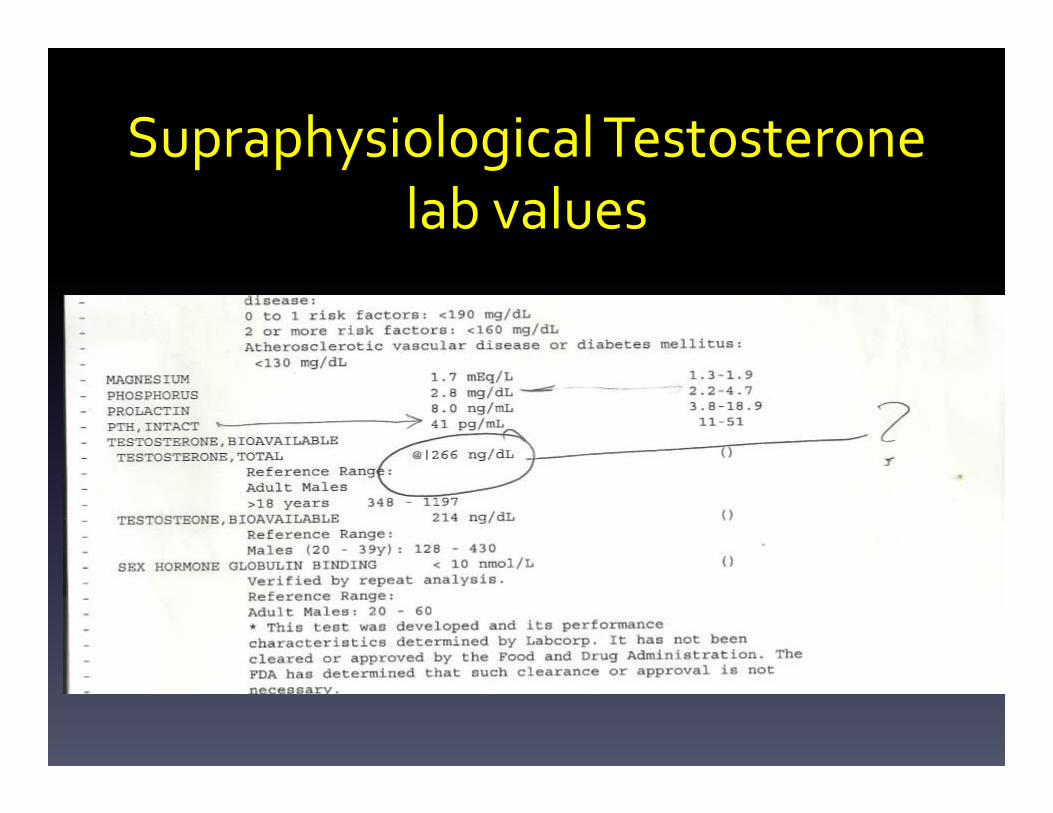
SupraphysiologicalTestosterone lab values

Bacterial, Fungal, Parasitic Overgrowth
Mold Toxicity
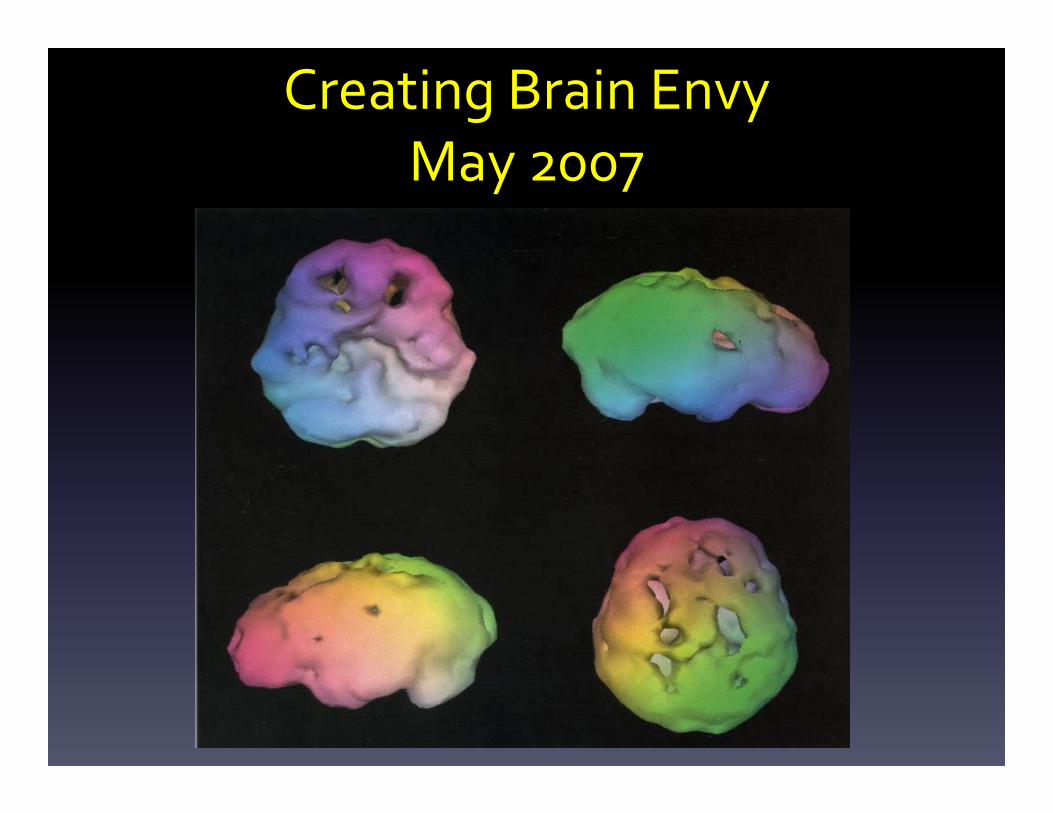
Creating Brain EnvyMay 2007
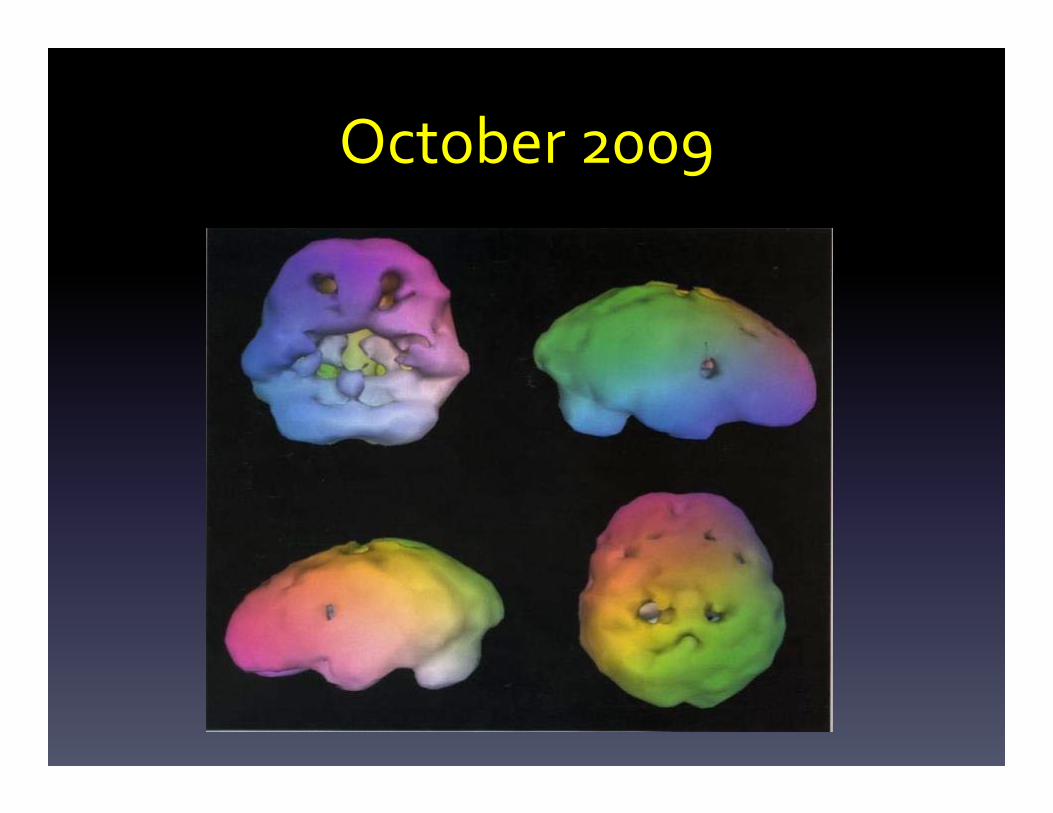
October 2009
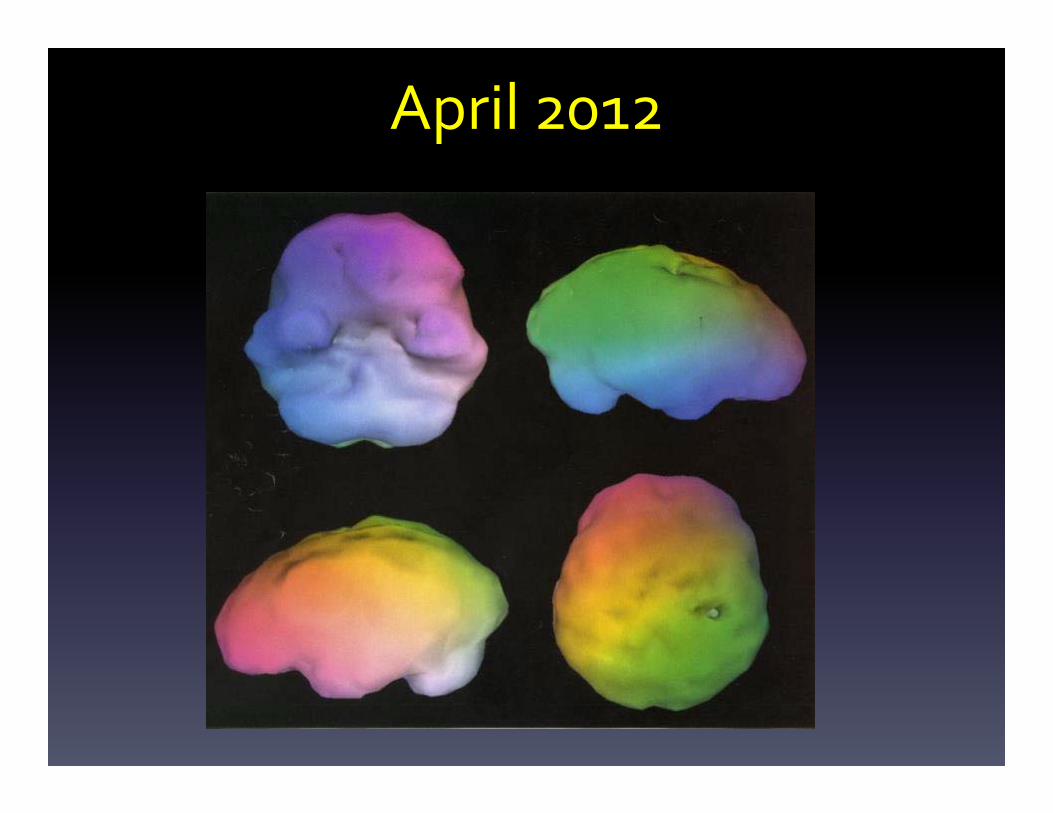
April 2012
Thank you!
Recommended

















