Psoriatic ArthritisClinical Features and
Epidemiology
Dafna D. Gladman MD, FRCPC
Director, Psoriatic Arthritis Program,
University Health Network
Centre for Prognosis Studies in the Rheumatic Diseases
Toronto Western Hospital
Toronto Western Hospital

Psoriatic Arthritis
An inflammatory arthritis Associated with psoriasis Usually seronegative for
rheumatoid factor
Definition

Psoriatic Arthritis Clinical Patterns
Distal predominant (Distal inter-phalangeal joints of fingers and toes).
Oligo-articular (<5 joints) often in an asymmetric distribution.
Poly-articular (5 joints), rheumatoid arthritis-like.
Spinal Involvement. ‘Arthritis Mutilans’.
Moll & Wright, Seminars Arthritis Rheum 1973;32:181

Psoriatic Arthritis Patterns
Oligoarthritis Distal Arthritis

Psoriatic Arthritis Patterns
Polyarticular Pattern

Psoriatic Arthritis Patterns
Arthritis Mutilans

Psoriatic Arthritis Patterns
Arthritis Mutilans Telescoping

Psoriatic Spondyloarthropathy

Psoriatic Spondyloarthropathy

Dactylitis in PsA

Edema in PsA

Heel Lesions in PsA
Achilles Tendon Insertion ErosionPlantar Spur
Achilles Tendon Spur

Other Radiological Features of PsA
Tuft resorption
Periostitis

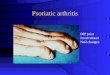
Hidden Psoriasis

PsA Reported Series*
Feature Roberts Kammer Gladman Torre-Alonso
Veale Jones
Year 1976 1979 1987 1991 1994 1994 Site Leeds Boston Toronto Spain Leeds Bath No. 168 100 220 180 100 100 M/F 67/101 45/55 104/116 99/81 59/52 43/57 Age 40 39 37 39 34 38 J < S ? 30 17 15 ? 18 SI NA 11 26 20 14 16 Asymm ? 53 21 45 43 26 Sym. 78 28 48 42 33 63 Distal 17 10 12 1 16 1 Back ? 2 3 7 4 6 Mutilans 5 7 16 5 2 4
*Includes only series with > 100 Patients

Psoriatic arthritis: A distinct entity ? Dutch study found no association
between psoriasis and polyarthritis. No association between HLA antigens and
seronegative polyarthritis with psoriasis. No radiological features in seronegative
polyarthritis with psoriasis.– van Romunde LKJ, et al.Rheumatology
International 1984;4:55-73.
? fortuitous association – Cats A. Cutis 1990;46:323-329.

Psoriatic arthritis
Prevalence of psoriasis in the general population: 0.1-2.8%.
Prevalence of psoriasis in arthritis patients: 2.6-7.0%.
Prevalence of arthritis in the general population: 2-3%.
Prevalence of arthritis in psoriatic patients: 6-42%.
Epidemiological Evidence

Psoriatic arthritis: A distinct entity !
Previous population studies. Epidemiological studies. Dutch study found DIP joints disease
more common in patients with seronegative polyarthritis and psoriasis.
A distinct form of arthritis, with different patterns, associated with psoriasis.

A comparison between Psoriatic Arthritis and Rheumatoid Arthritis
Psoriatic Arthritis
Rheumatoid Arthritis
DIP Involvement Common Uncommon
Symmetry Less Common Common
Erythema of joint Common Uncommon
Back Involvement Common Uncommon
Skin Lesions Always Uncommon
Nail Lesions Common Uncommon
Dactylitis Common Uncommon
Enthesitis Common Uncommon
Rheumatoid nodules Never Common
Rheumatoid Factor Uncommon Common
HLA-B*27 40-50% 4-8%

Assessment of Tenderness
RA N=51
PsA N=50
Test P Value
Fibromyalgia (N) 29 12 2=9.99 0.0016
Dolorimeter (Kg) Tender Points
4.77 6.60 t=5.23 <0.0001
Dolorimeter (Kg) Control Points
5.99 7.58 t=5.18 <0.0001
Dolorimeter (Kg) Active Joints
4.19 6.78 t=10.18 <0.0001
Psoriatic Arthritis Vs. Rheumatoid Arthritis
Buskila D, et al. J Rheumatol 1992;19:1115-9.

Psoriatic Arthritis
Classified with the Seronegative Spondyloarthropathies:– It is usually seronegative for
rheumatoid factor.
– It may be associated with a spondyloarthropathy.
– It is associated with HLA-B27.
Classification

Differentiating PsA from other SpA
Feature PsA AS ReA IBDM:F 1:1 9:1 8:1 1:1
Age onset 35-45 20 20 AnyPeripheral 96% 25% 90% Common
Distribution Any AxialLower limbs
Lowerlimbs
Lowerlimbs
Dactylitis 35% Uncommon Common Uncommon
Enthesitis Common Common Common Unommon
Sacroiliitis 40% 100% 80% 20%HLA-B*27 ~50% >90% 80% 40%

Psoriatic Arthritis Prevalence
Exact prevalence unknown. Estimated figures vary from 0.1% in
Rochester Minnesota to 1.4% in the Faroe Islands.
Recent Survey by National Psoriasis Foundation suggests prevalence of 1.4% of general population in the US.
Recent study from Toronto suggests a prevalence of 2.5%.

Psoriatic ArthritisPrevalence among people with psoriasis
Author (yr) Centre No. Ps. Pts. % PsA
Leczinsky (1948) Sweden 534 7
Vilanova (1951) Barcelona 214 25
Little (1975) Toronto 100 32
Scarpa (1984) Napoli 180 34
Stern (1985) Boston 1285 20
Zaneli (1992) Winston-Salem 459 17
Barisic-Drusko (1994) Osijek region 553 10
Salvarani (1995) Regio Emilia 205 36
Shbeeb (2000) Mayo Clinic 1056 6.25
Brockbank (2001) Toronto 126 31
NPF (2002) US 4.4 m 23

Psoriatic arthritis
PsA is much more serious than previously recognized.
20% of patients with PsA develop clinical deformities and damage, resulting in functional disability.
5 deformities were detected in 55% of patients after 10 years of follow-up.
Gladman DD et al. Quart J Med 1987;62:127.Torre Alonso et al. Brit J Rheumatol 1991;30:245.
Clinical Outcome

The University of Toronto Psoriatic Arthritis Program
Duration <1 yr 1-5 yr 6-10 yr >10 yr
Visit 1st Last 1st Last 1st Last 1st Last
No Deformities 53% 51% 70% 50% 64% 35% 59% 22%
< 5 deformities 28% 30% 20% 28% 17% 28% 26% 23% 5 deformities 19% 19% 10% 22% 19% 37% 15% 55%
Development of Deformities during follow-up
Gladman DD. Baillière’s Clinical Rheumatology1994;8:379.

Prognostic Indicators in PsA
Progression of damage defined by a change in damage state:– State 1 = 0 damaged joints– State 2 = 1-4 damaged joints– State 3 = 5-9 damaged joints– State 4 = 10 damaged joints
Analysis by model for rate of transition between damage states.
Clinical Indicators of Progression
Gladman DD et al. J Rheumatology 1995;22:675.

Prognostic Indicators in PsA
Relative Risk Variable 1 to 2 2 to 3 3 to 4 2 P value > 4 Effusions 1.6 1.6 1.6 5.7 0.017 ESR < 15 0.61 0.61 - 6.68 0.01
Rx 1.78 1.78 1.78 7.8 0.005
Steroids 1.55 1.55 1.55 5.46 0.019
Multivariate model for Clinical Indicatorsof Clinical Progression*
Gladman DD et al. J Rheumatology 1995;22:675.
*Based on clinical features at presentation

Prognostic Indicators in PsA
Variable Relative Risk X2 P value 1 to 2 2 to 3 3 to 4 B22 0.19 0.19 0.19 0.002
B27 1.06 1.06 1.06 0.06 0.81
B27xDR7 2.47 2.47 2.47 5.39 0.02
B39 7.05 - - 16.40 <0.001 DR7 0.83 0.83 0.83 0.63 0.43
DQw3 1.63 0.63 1.63 6.86 <0.001
DQw3xDR7 0.54 0.54 0.54 3.09 0.08 > 4 Efusions 1.27 1.27 1.27 1.18 0.28 ESR < 15 0.83 0.83 0.83 1.91 0.17 High Past Rx 2.25 2.25 2.25 8.10 0.004 Steroids 1.58 1.58 1.58 6.73 0.0001
Multivariate Model for Clinical Damage
Gladman DD & Farewell VT. Arthritis Rheum 1995;38:845.Gladman DD, et al. J Rheumatol 1998;25:730.

Prognostic Indicators in Psoriatic Arthritis
Factor Relative Damage Rate
95% CI P value
No. AJ 1.04 1.02,1.07 <0.001 FC 1.86 1.05,2.16 0.027 Male gender 0.65 0.47,0.92 0.013 Current Damage 3.95 2.52,6.20 <0.001
Initial ESR 0.61 0.42,0.90 0.013 Pre Clinic Rx 1.83 1.20,2.79 0.005
Final Multivariate Model for Time Varying Clinical Indicators
Gladman DD, Farewell VT. J Rheumatol 1999;26:2409

Outcome in Psoriatic arthritis
PsA patients are at an increased risk of death.
Overall risk is 1.62 that of Ontario Residents.
» 1.66 for women, 1.59 for men
Causes of Death are similar to general population.
Risk of death is related to previously active and severe disease.
Wong K, et al. Arthritis Rheum 1997;40:1868-7.Gladman DD, et al. Arthritis Rheum 1998;41:1103-10.
Mortality Studies

Mortality in Psoriatic Arthritis
Primary Cause N (%) Circulatory system 17 (36.2)
Myocardial Infarction 13 (27.6)
Cerebrovascular accident 2 ( 4.3)
CHF/arteriosclerosis 2 ( 4.3)
Respiratory system 10 (21.3)
Pneumonia 7 (14.9)
COPD 3 ( 6.4)
Digestive system (liver) 4 ( 8.5)
Malignant neoplasms 8 (17.0)
Injuries/poisoning 7 (14.9)
Other 1 ( 2.1)
Total known cause 47 ( 100)
Primary causes of death in 53 patients

Survival in Psoriatic Arthritis
Time Since Clinic Entry (Years)
Su
rviv
al P
rob
abili
ty
0 5 10 15 20
0.5
0.6
0.7
0.8
0.9
1.0
All patients

Mortality in Psoriatic Arthritis
Factor Relative risk
Confidence interval
P value
Prior Medication
1.83
0.93, 3.60
0.079
Radiological damage 3.88 1.32,11.35 0.014
ESR > 15 3.77 1.31,10.83 0.013
Nail changes 0.33 0.14, 0.76 0.009
Prognostic Factors: Final Multivariate Model
Gladman DD, et al. Arthritis Rheum 1998;41:1103-10.

Remission in Psoriatic Arthritis
Summary Remission occurred in 17.6% of our PsA
patients. Male gender and less active and severe
arthritis at presentation to Clinic were associated with remission.
Only 6 (8.7%) of the PsA patients sustained “true remission”,
35 (52%) had subsequent flares.
Gladman DD et al. J Rheumatol 2001;28:1045-8.

Psoriatic Arthritis Prognostic Factors
Progression of Damage: High effusion count at presentation High joint count at each visit High medication level at presentation Low ESR is “protective”
Death: Elevated ESR High prior medication level Radiological Damage
Remission Male Gender Low joint count at presentation

Psoriatic Arthritis
Not just skin and joints! An inflammatory arthritis associated with
psoriasis. More common than previously thought. About one fifth of the patients have a
severe debilitating disease, although some patients achieve remission.
Earlier studies suggesting that PsA was a mild disease included patients with early disease.

Psoriatic Arthritis Program
Cathy Schentag MsC Research AssociateCPSRD, TWH
Richard Cook, PhDBiostatisticianWaterloo, Ontario
Vern Farewell, PhDBiostatisticianMRC, Cambridge, UK
Dr. Dafna Gladman - Director
Janice Husted, PhD EpidemiologistWaterloo, Ontario
Nicole Anderson, BScResearch AssistantCPSRD, TWH
Fawnda Pellett, BSCResearch TechnologistCPSRD, TWH
Research Fellows, Rheumatology Residents, Students,Patients

Psoriatic Arthritis Program - Support Ontario Ministry of Health Medical Research Council / Canadian
Institutes of Health Research The Arthritis Society Centre for Prognosis Studies in The
Rheumatic Diseases University of Toronto / University Health
Network Arthritis Centre of Excellence Krembil Foundation PsA Patients
Recommended