
Prostate MRI 7/30/2018 SAR DFP Case
Staging: Focus on Neurovascular Bundles
Ben SpilsethAssistant Professor of RadiologyUniversity of [email protected]
Paari MuruganAssistant Professor Department of Laboratory Medicine and PathologyUniversity of Minnesota

Background
• 66 year old male with prostate cancerdiagnosed as Gleason 4+4=8 onnontargeted biopsy referred for furthertreatment
• Staging MRI performed
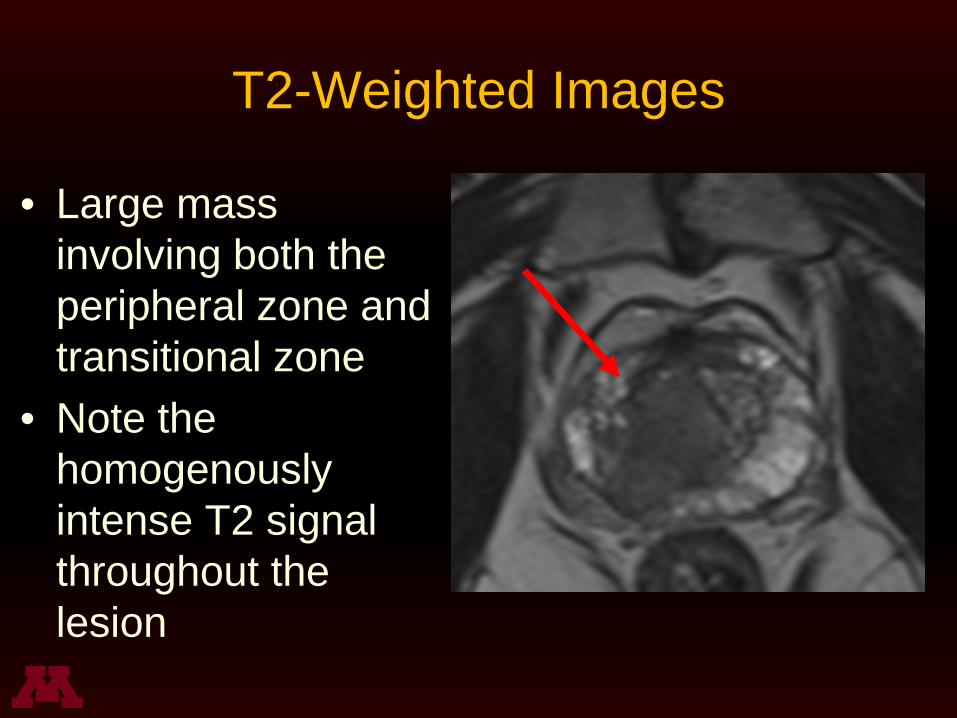
T2-Weighted Images
• Large massinvolving both theperipheral zone andtransitional zone
• Note thehomogenouslyintense T2 signalthroughout thelesion

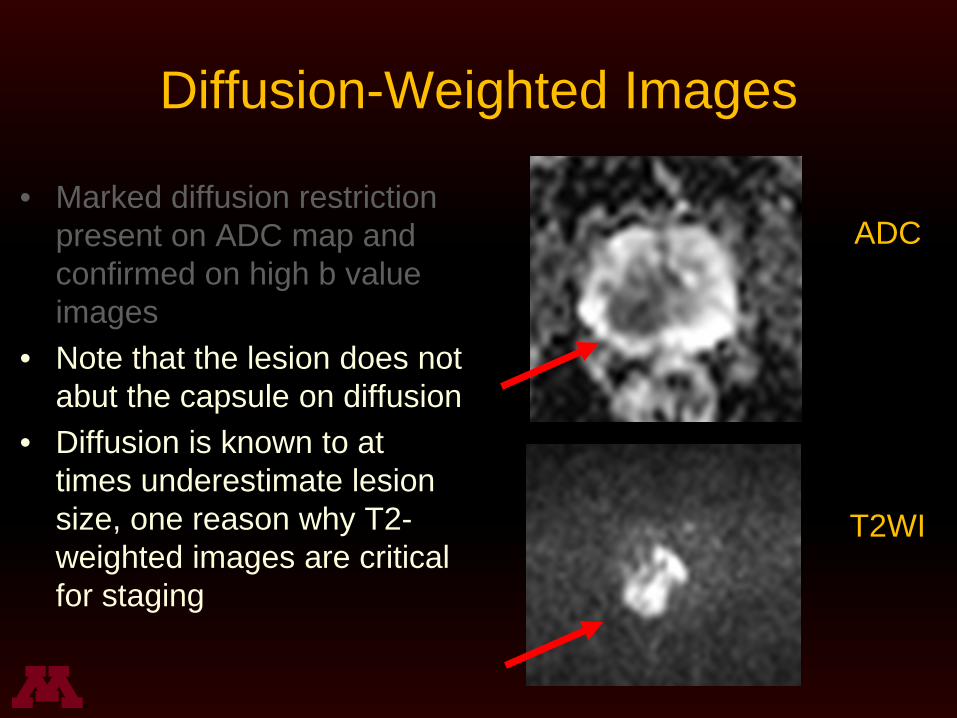
Diffusion-Weighted Images
• Marked diffusion restrictionpresent on ADC map andconfirmed on high b valueimages
B 2000
ADC
Diffusion-Weighted Images
• Marked diffusion restrictionpresent on ADC map andconfirmed on high b valueimages
• Note that the lesion does notabut the capsule on diffusion
• Diffusion is known to attimes underestimate lesionsize, one reason why T2-weighted images are criticalfor staging
T2WI
ADC

Dynamic Contrast Enhancement
• Brisk earlyenhancement ispresent

PIRADS Assessment
• T2WI – 5• DWI – 5• DCE – 5• Overall – 5
• But what about staging?

Staging –Extraprostatic Extension?
• Extraprostaticextension evidencedby the followingfactors– Broad tumor contact
(>10mm)– Angulation/step-off
appearance of tumor– Asymmetry of
neurovascular bundle

Staging – Normal Neurovascular Bundles
• Located at 5 and 7o’clock positions, thoughexact location variable
• Small “dots and dashes”normally seen
• Tumor often escapesthe capsule and spreadsalong the neurovascularbundles
T2WI

This case - Involvement of Neurovascular Bundles
• Thickening or directextension of tumorindicates neurovascularbundle involvement (redarrow)
• Note normal leftneurovascular bundle(green arrow)
T2WI

Interpretation and Management
• Case interpreted as PIRADS 5• Right mid gland extraprostatic extension• Suspected involvement of the
neurovascular bundles

Interpretation and Management
• Patient opted for surgical resection• Generally, nerve sparing surgery leaving the
neurovascular bundles intact is preferred topotentially maintain sexual function
• In our case, nerve sparing radical prostatectomywas planned on the left, with a wide margintaken on the right side due to suspectedneurovascular bundle involvement precludingbilateral nerve sparing surgery

Prostatectomy Results
• Radical prostatectomy performed, with unilateralnerve sparing on the left (right neurovascularbundle removed)
• Tumor extension from apex to base, peripheraland transitional zone, 50% of gland volume
• Extraprostatic extension at right mid gland andbilateral bases

• Ductal carcinomawithpseudostratifiednuclei in papillaryand cribriformgrowth pattern
• Gleason 4+5=9
Pathology slides courtesy of Paari Murugan

• MRI image at basewith suspectedextraprostaticextension
• Path slide of right baseextraprostatic tissues
• Extraprostaticextension confirmed,and nerve invasion,along withlymphovascularinvasion
Ganglion and nerve invasion
LVI
Fat
Pathology slides courtesy of Paari Murugan
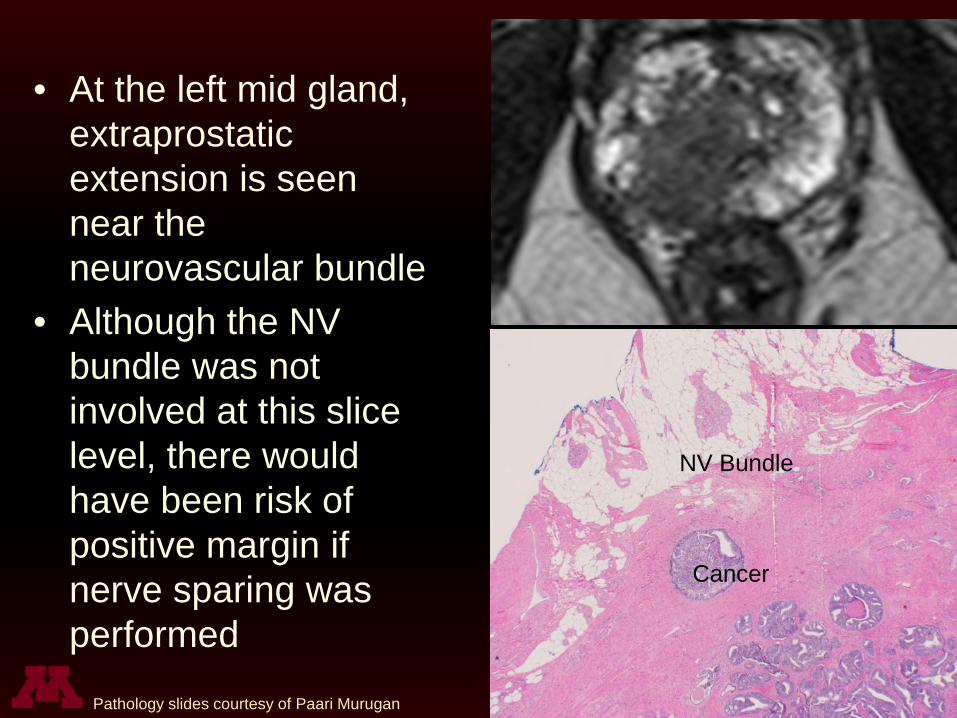
• At the left mid gland,extraprostaticextension is seennear theneurovascular bundle
• Although the NVbundle was notinvolved at this slicelevel, there wouldhave been risk ofpositive margin ifnerve sparing wasperformed
NV Bundle
Cancer
NV Bundle
Cancer
Pathology slides courtesy of Paari Murugan

Teaching Points
• Use T2-weighted images for staging– Highest spatial resolution– Best depiction of anatomy– Less likely to underestimate disease extent than DWI
• Identify lesion proximity to neurovascularbundles and evidence of direct involvement– Neurovascular bundle involvement has implications
for prognosis, surgical planning, and likelihood ofpostprocedural impotence if nerve sparing cannot beperformed
Thank You
Ben SpilsethAssistant Professor of RadiologyUniversity of [email protected]
Paari MuruganAssistant Professor Department of Laboratory Medicine and PathologyUniversity of Minnesota
Recommended









![Prostate Cancer Staging Registrars 11.05.2018 [Read-Only] · 10/30/2018 5 Very healthy 63 year old African American gentleman Prostate Cancer on TRUS bx for elevated PSA 4.3 GS 4+4](https://img.pdfslide.us/doc/110x75/5fbf6532b94f20688e6121d3/prostate-cancer-staging-registrars-11052018-read-only-10302018-5-very-healthy.jpg)







