Proliferation of Pathogenic Biofilms within Sealer-Root Dentin Interfaces is Affected by
Sealer Type and Aging Period
by
Karina Adriana Roth
A thesis submitted in conformity with the requirements
for the degree of Masters of Science (Endodontics)
Graduate Department of Dentistry
University of Toronto
© Copyright by Karina Adriana Roth 2011

ii
Proliferation of Pathogenic Biofilms within Sealer-Root Dentin Interfaces is Affected by Sealer Type and
Aging Period
Karina Roth
Masters of Science
Discipline of Endodontics
University of Toronto
2011
Abstract
Objective: To assess biofilm proliferation within the sealer-dentin interfaces of methacrylate
resin-based sealers, self-etch (SE) and total-etch (TE), and an epoxy resin-based sealer (EP).
Methods: Standardized human root specimens were filled with the test materials and were aged
for 1 week, 1, 3 or 6 months in saline (n=3/group). Monoclonal biofilms of Enterococcus
faecalis were grown on the specimens for 7 days in continuous media reactor. The extent of
biofilm proliferation of E. faecalis within the sealer-dentin interface for each material at each
incubation period was assessed using fluorescence microscopy of dihydroethidium-stained
specimens. Results: TE had less biofilm proliferation than EP and SE (p<0.01). Deeper biofilm
proliferation was detected in SE and EP specimens aged for 1 and 3 months than those aged for 1
week or 6 months (p<0.05). Conclusion: Self-etch and epoxy resin-based sealers were more
susceptible to interfacial biofilm proliferation than total-etch system at shorter incubation
periods.
iii
Acknowledgments
I would like to thank my principal supervisor, Dr. Yoav Finer to whom I wish to express my
deepest gratitude for his guidance, numerous hours of dedication and invaluable feedback
throughout this research project and during the preparation of the manuscript. I will be forever
grateful and thankful for having had the privilege of working with him, learning from his wealth
of knowledge, and most importantly for his immeasurable kindness and generosity throughout
my time at U of T, both at the professional level and for understanding and helping me during
personal hardships.
Next, thank you to Dr. Shimon Friedman, Head of the Discipline of Endodontics, for the
opportunity to be part of the Graduate program at the University of Toronto. Dr. Friedman has
been instrumental in bridging the endodontic and restorative/biomaterials aspect of the project
and contributed numerous hours to the correction and perfection of the manuscript.
Thank you to Dr. Céline Lévesque who taught me the ABC’s of her lab, supported me and was
always there for me providing constant moral and technical support in many aspects of the
project together with all of the wonderful people working with her.
I furthermore wish to extend my appreciation and thanks to Dr. Bettina Basrani and to Stephanie
Koyanagi, Richard Mair, Dr. Milos Legner, Dr. Babak Shokati and Dr. Jian Wang who helped
me with all of the technical aspects of my project.
Finally and most importantly, I would like to thank my dear husband Gustavo and amazing son
Max for their constant support and encouragement throughout my years of education. Their
constant love and patience in the numerous hours that I was away working and studying are what
made it possible for me to complete my work. To them, I owe the greatest debt of gratitude.
Karina A Roth, June 2011
iv
Table of Contents
Proliferation of Pathogenic Biofilms within Sealer-Root Dentin Interfaces is Affected by
Sealer Type and Aging Period ................................................................................................... ii
Abstract ...................................................................................................................................... ii
Acknowledgments ........................................................................................................................ iii
Table of Contents ........................................................................................................................... iv
List of Appendices ........................................................................................................................ iix
List of Abbreviations .......................................................................................................................x
Chapter 1 ..........................................................................................................................................1
1 Introduction .................................................................................................................................1
1.1 Purpose and Hypothesis .......................................................................................................3
1.1.1 Purpose of the study .................................................................................................3
1.1.2 Hypothesis................................................................................................................4
1.1.3 Objectives ................................................................................................................4
Chapter 2 ..........................................................................................................................................5
2 Literature review .........................................................................................................................5
2.1 The rationale for root canal treatment ..................................................................................5
2.2 Bacterial penetration into the dentin and along the dentin-sealer interface .........................6
2.3 Enterococcus faecalis ..........................................................................................................7
2.4 Biofilms and their role in disease progression .....................................................................9
2.5 The smear layer ..................................................................................................................11
2.6 Materials for root filling.....................................................................................................11
2.6.1 Epoxy-resin based sealers ......................................................................................13
2.6.2 Methacrylate resin-based root canal sealers ..........................................................14
2.7 Degradation of the bond between methacrylate resins and dentin ....................................21
v
2.8 Quality Assessment of the sealer-dentin interface .............................................................22
2.8.1 In vitro models .......................................................................................................22
2.8.2 In vivo models ........................................................................................................23
Chapter 3 ........................................................................................................................................24
3 Materials and Methods ..............................................................................................................24
3.1 Specimen Preparation ........................................................................................................24
3.2 Degradation media incubation of specimens .....................................................................27
3.3 Incubation of Specimens in Chemostat-Based Biofilm Fermentor (CBBF) .....................28
3.4 Reflected Light Microscopy (RLM) Analysis ...................................................................29
3.5 Scanning Electron Microscopy (SEM) Analysis ...............................................................30
3.6 Microbiological controls ....................................................................................................31
3.7 Statistical Analysis .............................................................................................................32
Chapter 4 ........................................................................................................................................33
4 Article ........................................................................................................................................33
Chapter 5 ........................................................................................................................................47
5 Discussion .................................................................................................................................47
Chapter 6 ........................................................................................................................................54
6 Conclusions ...............................................................................................................................54
Chapter 7 ........................................................................................................................................55
7 Recommendations .....................................................................................................................55
Chapter 8 ........................................................................................................................................57
8 Appendices ................................................................................................................................57
APPENDIX A: MEDIA AND SOLUTIONS ................................................................................58
APPENDIX B: GAMMA IRRADIATION ...................................................................................59
APPENDIX C: SAMPLE PREPARATION ..................................................................................60
APPENDIX D: STERILITY ASSAYS OF SPECIMEN PREPARATION ..................................62
vi
APPENDIX E: MICROBIOLOGY TECHNIQUES .....................................................................63
APPENDIX F: CHEMOSTAT-BASED BIOFILM FERMENTOR SET-UP ..............................66
APPENDIX G: STATISTICS........................................................................................................69
APPENDIX H: MICROSCOPIC IMAGES ..................................................................................71
APPENDIX I: SEM IMAGES .......................................................................................................75
APPENDIX J: BACTERIAL CELL PENETRATION .................................................................77
APPENDIX K: ETHICS APPROVAL ..........................................................................................78
References ......................................................................................................................................79
vii
List of Figures
Figure 1: Top images- Representative three-dimensional reconstruction of select Z-stack series
of E faecalis biofilms captured from sealer-dentin interfaces for the different materials.
Bottom images- Representative Z-stack images of E. faecalis captured from the sealer-dentin
interface of specimens aged for 1 month
Figure 2: E faecalis biofilm formation along the sealer-dentin interfaces for the different
materials.
Figure 3: Samples in sterile vial after being gamma irradiated.
Figure 4: Illustration of the sample preparation procedure.
Figure 5: Photograph of the sample preparation procedure.
Figure 6: Illustration and photograph of the 5 mm specimens.
Figure 7: Bacterial viability assessed using the plate counting technique.
Figure 8: Gram stain of E. faecalis cultured in experiment.
Figure 9: Analysis of immersing solution obtained from the vials.
Figure 10: Individual components of the chemostat-based biofilm fermentor (CBBF).
Figure 11: Image of the CBBF set-up within the laminar flow hood.
Figure 12: Microscopic image of a sample (10 X original magnification) denoting demarcation
of cardinal points to be subsequently analyzed (N = north, S = south, E = east, W = west). Four
points were randomly identified for each sample.
Figure 13: Mapping of selected points to be analyzed.
Figure 14: Photographic images through microscope’s optics of samples from different groups,
at 5X (original magnification).
viii
Figure 15: Microscopic images (5X original magnification) showing gap formation along the
dentin-sealer interface in specimens from different groups.
Figure 16: SEM images at 10 kV, 200 X original magnification, demonstrating gap formation in
samples from different groups.
Figure 17: Mean values for biofilm formation, for each sealer at each incubation time point.
ix
List of Appendices
Appendix A: MEDIA AND SOLUTIONS
Appendix B: GAMMA IRRADIATION
Appendix C: SAMPLE PREPARATION
Appendix D: STERILITY ASSAYS OF SPECIMEN PREPARATION
Appendix E: MICROBIOLOGY TECHNIQUES
Appendix F: CHEMOSTAT-BASED BIOFILM FERMENTOR SET-UP
Appendix G: STATISTICS
Appendix H: MICROSCOPIC IMAGES
Appendix I: SEM IMAGES
Appendix J: BACTERIAL CELL PENETRATION
Appendix K: ETHICS APPROVAL
x
List of Abbreviations
Bis-GMA Bisphenol A-glycidyl methacrylate
BHI Brain Heart Infusion broth
CBBF Chemostat-based Biofilm Fermentor
EDTA Ethylenediaminetetraacetic acid
EP Epoxy-resin based sealer
EBPADMA Ethoxylated bisphenol A dimethacrylate
HEMA Hydroxyethil methacrylate
MMPs Matrix metalloproteinases
MPa Megapascal
NaOCl Sodium hypochlorite
PBS Phosphate Buffer Saline
ROI Region of interest
SE Self-Etch system
SEM Scanning electron microscopy
SL Smear layer
TE Total-Etch system
TSB Trypticase Soy Broth
1
Chapter 1
1 Introduction
Bacterial invasion of the root canal space most frequently results in infection of the root canal
and periapical tissues of the affected tooth (1). To resolve infection, root canals are cleaned,
shaped and medicated, with the aim of reducing the bacterial load to a level that bacteriological
samples obtained from the canals yield no visible growth in culture. When no-growth cultures
are obtained, the probability of healing is high, in the range of 94%, compared to 68% when
cultures yield bacterial growth (2). Because of the invasion of bacteria into the dentinal tubules,
and because of anatomic irregularities of root canal systems, the conventional disinfection
regimens used clinically are only partially effective, resulting in residual bacteria and positive-
growth cultures in 10% to 70% of canals (3-5). Under favorable conditions in unfilled canals,
residual bacteria can proliferate to pre-treatment numbers within 2 to 4 days (6).
To eliminate residual bacteria or at least prevent their proliferation, the canal is filled after the
disinfection procedure (7). Root canal sealers should prevent the growth of microorganisms in
unfilled areas of the root canal system (isthmus, lateral canals, etc), and if any residual
microorganisms have remained after cleaning and shaping procedures, filling materials should
prevent their passage into periapical tissues (8). However, the currently used root filling
materials do not completely fulfill these requirements (9, 10). One of the factors influencing the
invasion of bacteria is the adaptation of the root filling to the canal wall (11). The standard root
filling is a combination of core material and sealer cement. The core acts as a piston on the
flowable sealer, causing the sealer to closely adapt to the dentin walls. The sealer layer should be
thin to minimize dimensional changes during and after setting. For resin-based sealers, in
particular, contraction/shrinkage after polymerization might lead to separation of the sealer from
the dentin, creating a potential pathway for future bacterial invasion.
2
In recent years, great emphasis has been placed on sealers that can bond to root dentin. This
trend, following those in restorative dentistry (10), is based on the premise that the bonded
interface may resist bacterial invasion. However, studies have consistently noted the difficulty to
establish a reliable bond between resin-based materials and dentin (12, 13). In the root canal, in
particular, bonding is undermined because the unfavorable cavity configuration causes increased
shrinkage stresses that de-bond the sealer from the dentin (14). Bonding can also be undermined
because of the dentin exposure to sodium hypochlorite, a potent oxidant producing an oxygen
rich layer on the dentin surface that inhibits polymerization (15, 16).
Eventual breakdown of the resin-dentin interface and subsequent penetration by oral fluids,
bacteria and their products might jeopardize the long-term outcome of the treated tooth. It has
already been well established that the primary cause of endodontic treatment failure is directly
related to the development of intraradicular infections in the form of biofilms (17).
The current gold standard for endodontic sealers, against which all new sealers are measured, are
epoxy-resin based sealers (18), such as AH Plus (Dentsply De Trey, Konstanz, Germany) which
adhere but do not bond to root dentin (19). Recently, methacrylate resin-based sealers have
gained popularity (20). The bond of these sealers to root dentin depends on the penetration of
hydrophilic resin monomers, incorporated to facilitate resin invasion into the wet dentinal
tubules (21), into the conditioned dentin surface to create micromechanical interlocking between
the dentin collagen and resin, forming a hybrid layer (22). Several types of adhesives for
methacrylate resin-based systems are available: (1) “Etch and rinse” (total-etch) systems
conventionally involve three steps with successive application of an acid etchant, primer and
bonding agent (23), and more recently two steps incorporating the primer and bonding agent into
one. The three-step approach produces the most durable bond (24) and is the gold standard for all
current bonded restorative systems. There are no current commercial total-etch endodontic
sealers available. “Self-etch” systems involve one step to etch, prime and bond, incorporating
the smear layer into the hybrid layer. Self-etch commercial endodontic sealers are available;
however, concerns have surfaced about inadequacy of their bond in the presence of a thick smear
layer (25, 26). The resin-dentin interface can undergo degradation over time, allowing salivary
3
and tissue fluid movement between the hybrid layer and dentin (24, 27-29) with consequent
breakdown of the covalent bonds within collagen fibrils and resin polymers (30). Products of
degradation eluting from composites can have an effect on bacterial cells by affecting their
intracellular functions and virulence factors (31, 32). As a result, interfacial bacterial penetration
and proliferation may occur (27), potentially resulting in endodontic failure.
1.1 Purpose and Hypothesis
1.1.1 Purpose of the study
Several commercially available products are currently available for root canal filling. Many have
undergone multiple modifications in their formulas due to unfavorable outcomes and due to the
emergence of evidence highlighting deleterious effects of some of their components. There
seems to be a continuous search for a material with ideal properties, that forms a single unity
between the dentin interface and the material itself, and that its long-term seal would not be
affected by some ulterior degradation or additional bacterial challenge. If subsequently the
dentin-sealer interface degrades over time, and if bacteria are present, they may form biofilms
which have been linked to endodontic failures.
The aim of my thesis was to compare the quality of seal of the sealer-dentin interface of two
methacrylate resin-based systems, self-etch (SE; RealSeal SE, Sybron Endo) and total-etch (TE;
Scotchbond MP, 3M, Bisfil 2B, Bisco), and an epoxy resin-based sealer (EP; AH Plus,
DENTSPLY/DeTrey) after aging the interfaces for up to 6 months using interfacial bacterial
invasion and biofilm proliferation as the biological markers for quality of the sealer-dentin
interface.
4
1.1.2 Hypothesis
The null hypothesis was that there will be no difference in the interfacial biofilm proliferation
and bacterial penetration of Enterococcus faecalis between root dentin and three test materials
(total-etch resin, self-etch sealer, epoxy resin sealer) following aging of the interfaces for up to 6
months.
1.1.3 Objectives
The objectives of the proposed study are:
To establish a physiologically relevant in vitro model for characterization of the sealer-
dentin interface following aging in physiological media, using biofilm proliferation and
bacterial invasion as the biological markers for the quality of the sealer-dentin interface.
To compare the quality of the sealer-dentin interface and the effect of aging of two
methacrylate resin-based systems, self-etch (SE; RealSeal SE, Sybron Endo) and total-
etch (TE; Scotchbond MP, 3M, Bisfil 2B, Bisco), and an epoxy resin-based sealer (EP;
AH Plus, DENTSPLY/DeTrey).
5
Chapter 2
2 Literature review
2.1 The rationale for root canal treatment
Bacterial invasion of the root canal space most frequently results in infection of the root canal
and periapical tissues; in the absence of bacteria, pulpal or periradicular pathoses would not
develop (1, 33, 34). Cleaning and shaping of the root canal is performed in order to reduce
bacterial concentrations within the root canal. Follow-up studies of endodontic treatment have
shown a higher rate of healing when bacterial culture obtained prior to root filling yielded no
visible growth (35); when samples were positive only 68% of the teeth healed, when samples had
no growth, as many as 94% of the teeth healed (2).
It has been established that mechanical (instrumentation) and chemical (irrigating solutions)
methods for cleansing root canals do not completely eliminate bacteria from the root canal (4, 5,
36-38). Several authors have demonstrated that under favorable conditions residual bacteria in
unfilled canals can proliferate to pre-treatment numbers within 2 to 4 days (6, 39). Therefore, one
of the goals of filling root canals is to prevent re-growth of bacteria. The second goal is to
prevent recontamination of the treated root canal system by ingress of endogenous bacteria
through the coronal pathway. Such ingress has the potential to re-infect the canal and periapical
tissues (40). This goal is achieved by combining the root canal seal with an impervious coronal
seal.
The ideal root canal filling should provide a seal impermeable to bacterial penetration to prevent
ingress of bacteria and bacterial by-products (41). Also, it should prevent percolation of substrate
to bacteria that survive treatment (7).
6
2.2 Bacterial penetration into the dentin and along the dentin-
sealer interface
Most of the radicular dentinal tubules run perpendicular to the pulp and the periphery in the root
canal. Their size and number differ along the root, with diameters ranging from 1 to 3 μm and
density from 4900 to 90,000 tubules per square millimeter (42). In the coronal dentin near the
pulp there can be as many as 42,000 tubules/mm2
(43) and the density decreases towards the root
apex, to just over 8,000 tubules/mm2
(44) at the apical level. Intratubular dentin is highly
mineralized (approximately 95 volume % mineral phase) compared with the less-mineralized
collagen matrix (about 30 volume % mineral phase) of intertubular dentin, and mineralization
increases with age resulting in a reduction in size of the tubules which can lead to a complete
obliteration. There is also a decrease in number of tubules due to physiologic aging of patients,
reaching to a reduction of up to 40% in 80 year-old patients compared to 20 year-old ones (44,
45).
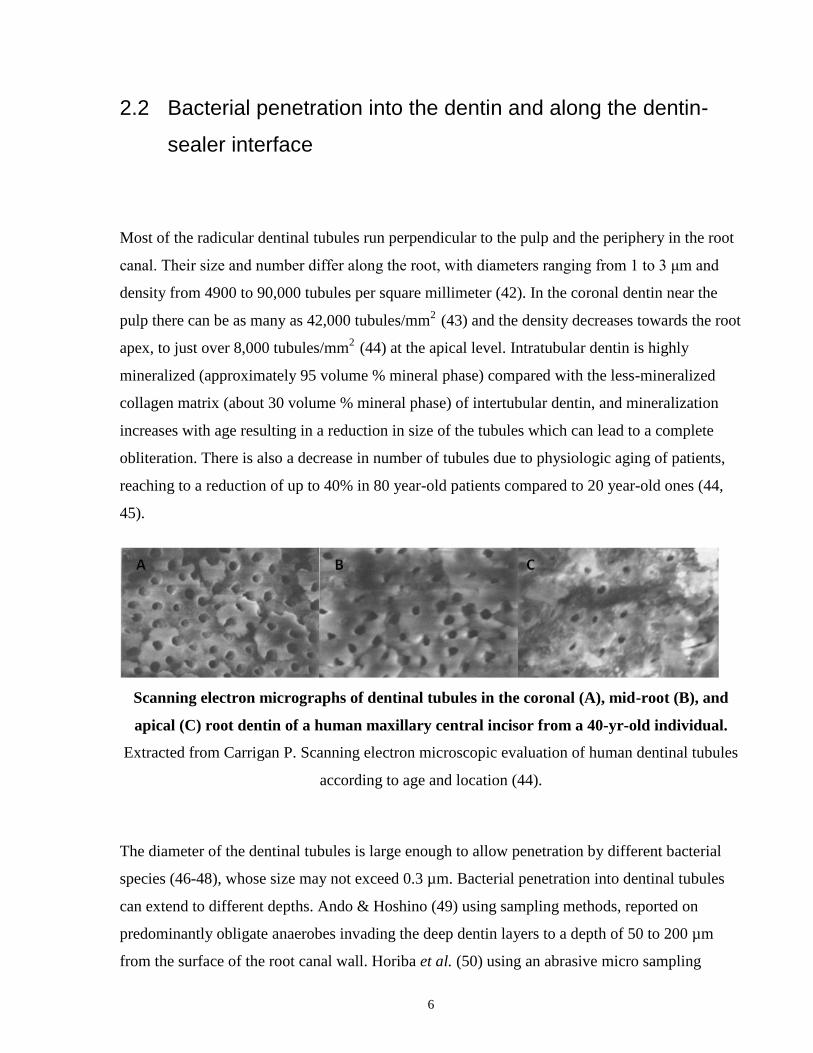
Scanning electron micrographs of dentinal tubules in the coronal (A), mid-root (B), and
apical (C) root dentin of a human maxillary central incisor from a 40-yr-old individual.
Extracted from Carrigan P. Scanning electron microscopic evaluation of human dentinal tubules
according to age and location (44).
The diameter of the dentinal tubules is large enough to allow penetration by different bacterial
species (46-48), whose size may not exceed 0.3 µm. Bacterial penetration into dentinal tubules
can extend to different depths. Ando & Hoshino (49) using sampling methods, reported on
predominantly obligate anaerobes invading the deep dentin layers to a depth of 50 to 200 µm
from the surface of the root canal wall. Horiba et al. (50) using an abrasive micro sampling
7
method, reported that the endotoxin from Gram-negative bacteria may be distributed mainly in
dentin from the pulpal surface of dentin up to a depth of 300 μm. Sen et al. (51) found bacteria
and yeasts in the dentinal tubules from 10 to 150 μm using scanning electron microscopy. Peters
et al. (52), using culturing methods and histological sections, found that the deepest penetration
from the canal towards the cementum was 375 μm. The degree of bacterial invasion depends on
the type of bacterial species, the time of incubation (51, 53) and the age of the patient: bacterial
infection of dentinal tubules occurs to a lesser extent in older patients (54) probably due to an
increase in mineral content within the dentinal tubules which in turn results in their occlusion.
2.3 Enterococcus faecalis
Periapical endodontic disease is strictly related to presence of microorganisms (34). In primary
endodontic infections, microorganisms that initially invade and colonize necrotic pulp tissue are
found. In persistent endodontic infections, primary or secondary microorganisms that resisted
intracanal antimicrobial procedures and endured periods of nutrient deprivation can colonize the
endodontic milieu, striving and multiplying causing disease (7, 55). Finally, even in some cases
where treatment has followed the highest standards, extraradicular infections might have been
established (56), microbial invasion of inflamed periradicular tissues ensues and is a sequel to the
intraradicular infection. Usually there is evidence of biofilm formation, with well-established
microbial communities that are more resistant and harder to eliminate through standard intracanal
endodontic procedures (17).
Bacteria invading coronal dentinal tubules, due to optimal environmental conditions, can further
multiply and invade radicular dentin (57) which has been proven to have a negative impact on the
outcome of endodontic treatment (58). Failed endodontic cases demonstrate only one or two
species of Gram-positive facultative anaerobic microorganisms per canal, and Enterococcus,
Streptococcus, Peptostreptococcus and Actinomyces are the most frequently identified (59).
Recently, Vagococcus fluvialis was detected in root canals for the first time, and Solobacterium
8
moorei and Fusobacterium nucleatum were the most prevalent species in root filled teeth
exhibiting periradicular lesions (60).
Enterococcus faecalis strains are rarely found in primary infections but frequently found in
previously endodontically treated teeth (7, 61, 62) which would indicate that they could gain
access into the root canal after treatment completion probably due to coronal leakage (63). In
failed cases, these microorganisms gain access into the root canal after treatment completion
probably as a result of coronal leakage (63) and proliferate due to their ability to compete with
other microorganisms, invade dentinal tubules, and resist nutritional deprivation.
Several static in vitro (64), in vivo (65) and ex-vivo (66) investigations have used Enterococcus
faecalis to study their behavior and aptitude to strive and survive in endodontically treated teeth,
showing that they can maintain viability for twelve months ex vivo (67). The choice of this strain
was based on their ability to penetrate into dentinal tubules in as little as 48 hours of inoculation
(67) adhering and forming communities of organized biofilms as monospecies over root canal
surfaces and because this organism is frequently found in failed endodontic treatments (63, 68).
When E. faecalis were grown on abiotic surfaces such as microtiter plates, it was found that their
ability to develop into biofilms was dependant on the surface attributes of the substratum and
that these could vary according to the environmental and nutritional conditions present (69).
These authors demonstrated that when E. faecalis was grown aerobically under nutrient-rich
medium, they demonstrated both biofilm formation and deeper penetration of bacteria into
dentinal tubules.
9
2.4 Biofilms and their role in disease progression
A biofilm is a mode of microbial growth where dynamic communities of interacting sessile cells
are irreversibly attached to a solid substratum as well as each other and are embedded in a self-
made matrix of extracellular polymeric substances (70). The basic structural unit of a biofilm is a
microcolony or cell clusters (discrete units of densely packed bacterial cells, single or
multispecies, aggregates). A glycocalix matrix made up of EPS surrounds the microcolonies and
anchors the bacterial cells to the substrate.
Biofilms are of concern in endodontics and can be found as:
1) Intracanal biofilms: (71) These biofilms are formed by multiple species of microorganisms.
They degrade the dentin substrate as a consequence of the interaction of bacteria and their
metabolic products on dentin (internal resorption can be a consequence of bacteria-mediated
substrate dissolution).
2) Extraradicular or root surface biofilms: Formed by multiple species of microorganisms
(cocci and short rods with cocci attached to the tooth substrate), plus filamentous and fibrillar
forms. Calcified biofilms over root surfaces have been reported by Ricucci (72) and Harn
(73) in teeth refractory to conventional root canal therapy.
3) Periapical biofilms: Actinomyces and Propionibacterium propionicum producing
sulphur granules. This granular biofilms structure consists of a central mass of intertwined
branching bacterial filaments held together by an extracellular matrix with periapical
radiating clubs. PMN’s and macrophages patrolling the periapex area are unable to engulf
bacteria in a matrix-enclosed biofilm structure.
4) Biomaterial-centered infection: bacteria adhere to an artificial material (for example: to
gutta-percha) (74).
10
There are different stages observed in biofilm formation:
STAGE 1: formation of a conditioning layer by adsorption of inorganic and organic molecules
to the solid surface (which takes places from minutes to hours).
STAGE 2: adhesion of microbial cells to this layer (days to weeks).
STAGE 3: bacterial growth and biofilm expansion / organization (months).
When biofilms are formed, their structure protects the residing bacteria from environmental
threats. Biofilms show higher resistance to both antimicrobial agents and host defense
mechanisms when compared with planktonic cells (75-77) due to the inability of chemicals to
penetrate the full depth of the biofilm.
There are several mechanisms by which the resistance to antimicrobial agents is created in
biofilms:
1) Collective metabolic activity: multiplying effects according to number / diversity.
2) Planktonic cells are eliminated by antimicrobial challenges (ones are sacrificed in expense of
others).
3) Persister cells accumulate in a biofilm since they revert less readily and are physically
retained by the biofilm matrix.
4) Collective neutralizing power of groups of cells leads to slow or incomplete penetration of
the antimicrobial into the biofilm.
The increase resistance to antimicrobial agents and host defense mechanisms provide biofilms
with increased virulence as compared with planktonic cells. Therefore, biofilms forming
processes are regarded as major contributors to disease pathogenesis
11
2.5 The smear layer
Instrumentation of the root canal during endodontic cleaning and shaping procedures results in
the production of a smear layer (78, 79). This layer is composed of organic and inorganic
substances- dentin, necrotic and viable tissue, remnants of odontoblastic processes, pulp tissue
and bacteria (79) which can be forced into the dentinal tubules to form smear plugs up to
different depths. Mader (78) reported that the smear layer was composed of two sections- a
superficial layer on the surface of the canal wall which is 1 to 2 μm thick and a more profound
layer which is condensed into the dentinal tubules reaching a depth of up to 40 μm.
There is much controversy regarding the removal or maintenance of this layer (80). This
controversy exists because the removal of the smear layer prior to sealing of the canal may affect
the following:
Bacterial penetration: the smear layer might disintegrate due to coronal or apical
microleakage thus providing a patent pathway for bacterial ingress.
It may shield remaining bacteria within the dentinal tubules, creating a protective micro-
environment and promoting their proliferation.
The ability of root canal irrigants and medications to penetrate into dentinal tubules.
The ability of sealers to adhere or have an intimate contact with the root canal walls.
2.6 Materials for root filling
The standard root filling is a combination of core material and sealer cement. The core acts as a
piston on the flowable sealer, causing the sealer to closely adapt to the dentin walls. The sealer
layer should be thin to minimize dimensional changes during and after setting. For resin-based
12
sealers, in particular, contraction / shrinkage after polymerization might lead to separation of the
sealer from the dentin, creating a potential pathway for future bacterial invasion.
In recent years, great emphasis has been placed on sealers that can bond to root dentin. This trend,
following tendencies in restorative dentistry (10), is based on the premise that the bonded interface
may resist bacterial invasion. However, studies have consistently noted the difficulty to establish a
reliable bond between resin-based materials and dentin (12, 13). In the root canal, in particular,
bonding is undermined because the unfavorable cavity configuration causes increased shrinkage
stresses that de-bond the sealer from the dentin (14). Bonding can also be undermined because of
the dentin exposure to sodium hypochlorite, a potent oxidant producing an oxygen rich layer on the
dentin surface that inhibits polymerization (15, 16). Eventual breakdown of the resin-dentin
interface and subsequent penetration by oral fluids, bacteria and their products might jeopardize
the long-term outcome of the treated tooth.
The current gold standard for sealers, against which all new sealers are measured, are epoxy-
resin based sealers (18). Epoxy resin sealers, such as AH Plus (Dentsply De Trey, Konstanz,
Germany) adhere but do not bond to root dentin (19). Nevertheless, they have been widely used
for many years with acceptable clinical outcomes.
In the beginning of the 21st century, methacrylate-based sealers were reintroduced with the
objective to bond directly to the root canal walls, and since then, they have increasingly gained
popularity (20). The bond of these sealers to root dentin depends on the penetration of
hydrophilic resin monomers, incorporated to facilitate resin invasion into the wet dentinal
tubules (21), into the conditioned dentin surface to create micromechanical interlocking between
the dentin collagen and resin, forming a hybrid layer (22). Several types of resin-based systems
are available:
(1) “Etch and rinse” (total-etch) systems conventionally involve three steps with successive
application of an acid etchant, primer and bonding agent (23), and more recently two steps
incorporating the primer and bonding agent into one. The three-step approach produces the most
13
durable bond (24) and is the gold standard for all current bonded restorative systems. Currently,
there are no commercial total-etch endodontic sealers available, possibly because of application
challenges within the root canal configuration.
(2) “Self-etch” systems involve one step to etch, prime and bond, incorporating the smear layer
into the hybrid layer. Self-etch commercial endodontic sealers are available; however, concerns
have surfaced about inadequacy of their bond in the presence of a thick smear layer (25, 26).
A number of studies have demonstrated that leakage occurs between the root canal wall and the
filling material (81-83). Factors influencing the adaptation of the root filling to the canal wall are
of great significance in determining the degree and extent of leakage (11).
2.6.1 Epoxy-resin based sealers
Epoxy-resin based sealers have been used for many years with clinical success and are widely
used due to their good mechanical properties and compatibility with subsequent restoration of
endodontically treated teeth with adhesive systems. Common materials of this group are AH 26
and AH Plus sealers (Dentsply, Tulsa Dental Specialties, Tulsa, OK, US). AH Plus consists of a
two-paste components system; one component is the catalyst (an epoxide) and the other is the
base (an amine paste). The two pastes are mixed in equal lengths until a uniform and
homogenous consistency with a single color is obtained. According to the manufacturer, the
epoxide paste contains diepoxide, calcium tungstate, zirconium oxide, aerosol and pigments; and
the amine paste contains 1-adamantane amine, N,N'-dibenzyl-5-oxa-nonandiamine-1,9, TCD-
diamine, calcium tungstate, zirconium oxide, aerosol and silicone oil (MSDS, Dentsply).
AH 26 and AH Plus sealers are thought to be able to react with any exposed amino groups in
collagen to form covalent bonds between the resin and collagen when the epoxide ring opens
14
during polymerization. Their bond strength to dentin is 2.06 MPa (Megapascal), and 2.93 MPa to
gutta-percha, suggesting that the resin can adhere to both substrates (84). Similarly, McComb
and Smith (85) found that AH26 had tensile bond strength to dentin of 1.62 MPa; Wennberg and
Ørstavik (86) reported 2.5 MPa bond strength.
Other studies compared bond strengths in the presence or absence of the smear layer (SL) with
contradictory results: 1.19 MPa and 0.30 MPa when the dentin had been pretreated with EDTA
(87) as opposed to 1.22 MPa with smear layer and 2 MPa without (88). In another study, Eldeniz
et al (89) tested the shear bond strength of three resin-based sealers (Diaket, AH Plus and Endo-
Rez) in presence or absence of smear layer, and found that AH Plus had the highest shear bond
strength among all of them both with or without smear layer present, and the highest values were
recorded when the smear layer had been removed.
2.6.2 Methacrylate resin-based root canal sealers
Methacrylate resin-based root canal sealers are gaining popularity amongst practitioners as they
may be used with dentin adhesives for bonding to intraradicular dentin (20). Hydrophilic resin
monomers are incorporated into the endodontic sealers to facilitate better resin penetration into
the wet dentinal tubules after the removal of the smear layer (21). The bond between the
adhesive systems and the dentine will depend on the penetration of the monomers into the
conditioned dentine surface to create micromechanical interlocking between the dentin collagen
and resin and thus to form a hybrid layer (22). It has been well established that it is impossible to
completely dry the root canals prior to their filling, and residual moisture could affect the seal of
the obturation. However, drying the canals with paper points or after using a low vacuum, and
despite the fact that some moisture was still present, methacrylate-based sealers demonstrated
significantly less leakage than zinc oxide-eugenol based sealers (90).
15
Historically, there have been four different generations of methacrylate resin-based sealers for
endodontic use (91):
The first generation appeared during the 70’s and was used until the 80’s with poor outcomes. It
contained a poly[2-hydroxyethyl methacrylate] (poly[HEMA]) as the principal component in
Hydron (Hydron Technologies, Inc, Pompano Beach, Fl, USA).
The second generation consisted of a non-etching hydrophilic resin that did not require the
adjunct utilization of a dentin adhesive (EndoRez, Ultradent Products Inc, South Jordan, UT,
USA).
The third generation consisted of self-etching sealers that contained a self-etching primer and a
dual-cured composite resin which was based on the concept of incorporating the smear layer
created during rotary preparation into the sealer-dentin interface. Materials comprised within this
generation are: FibreFill R.C.S. (Pentron Clinical Technologies, Wallingford, CT, USA), Resilon
(Resilon Research LLC, Madison, CT, USA), Epiphany (Pentron Clinical Technologies),
RealSeal (SybronEndo, Orange, CA), Resinate (Obtura Spartan Corp, Fenton, MO), and Smart
(Discus Dental, CulverCity, CA).
The fourth generation, are self-adhesive resins that have eliminated the separate
etching/bonding step and are represented by MetaSEAL (Parkell Inc, Edgewood, NY, USA),
Hybrid Bond SEAL (Sun Medical Co Ltd, Shiga, Japan) and RealSeal SE (SybronEndo, Orange,
CA, USA).
16
Current methacrylate-based systems require the use of adhesive systems for optimal
performance. These adhesive systems can be divided into two major categories:
1. Self-etch systems (SE)
2. Total-etch bonding agents (TE)
2.6.2.1 Self-etch systems (SE)
These materials contain an acidic resin which etches and primes and sometimes bonds
simultaneously, incorporating the smear layer and any residual irrigant components into the
hybrid layer. Sealers like RealSeal SE (SybronEndo, Orange, CA) combine in a single product a
self-etching primer and a moderately filled flowable composite thus eliminating the use of
separate self-etching primers (25). This approach potentially eliminates over etching and its
potential deleterious effects on the integrity of the resin-dentin interface (92).
According to the manufacturer (SybronEndo, Orange, CA), RealSeal SE is a self-etch
methacrylate/epoxy resin root canal sealer in a catalyst/base paste-paste formulation, which
combines a modified methacrylate chemistry based upon SE Epiphany Root Canal Sealer and
epoxy resin chemistry similar to AH Plus root canal sealer. Both pastes are contained within 2
separate chambers that after extrusion through an auto mix syringe, provides the sealer in its final
adequate consistency for delivery into the root canal system. According to the manufacturer, it
contains a mixture of EBPADMA, HEMA, BisGMA and acidic methacrylate resins, silane-
treated bariumborosilicate glasses, silica hydroxylapatite, Ca-Al-F-silicate, bismuth oxychloride
with amines, peroxide, photo initiator, stabilizers and pigments.
17
2.6.2.2 Clinical Performance of self-etch systems in endodontics
The quality of the adaptation of the sealer to the dentin wall is affected by the presence of the
smear layer. Concerns have been raised when using self-adhesive sealers, for multiple reasons:
first, due to the fact that these materials might not be aggressive enough to be able to etch
through thick smear layers thus creating micromechanical retention via dentin hybridization (26)
or in cases where there is incomplete removal of the smear layer in hard to reach areas (such as
the apical third). In these cases, EDTA (ethylenediaminetetraacetic acid) is used in order to
remove the smear layer (25). Kim et al (93) tested Real Seal versus Real Seal SE in dentin
covered with smear layer, intact dentin irrigated with sterile deionised water and dentin that had
been treated with 6.15% NaOCl and EDTA. They reported that Real Seal SE was not able to etch
the radicular dentin thus there was no bonding between the smear layer and the intact dentin.
When sterile water had been used, the demineralised dentin layer was very thin (< 100 nm-thick)
and when EDTA had been used, some apatite crystals remained within the partially
demineralised dentin after the self-adhesive resin had been used. They concluded that Real Seal
SE (with a pH of 3.9 versus the pH of 2.5 of Real Seal) was not acidic enough to etch through
smear layers to produce micromechanical retention to improve adhesion of the sealers to the
canal walls.
Another concern is that several studies have demonstrated that endodontic irrigants can produce
erosion of root canal walls, decrease the microhardness of the dentine by removing its organic
components and altering its mineral composition. Sodium hypochlorite which is widely used as
an endodontic irrigant is a deproteinizing agent and a potent biological oxidant, leaving behind
an oxygen rich layer on the dentin surface that reduces bond strength and increased microleakage
(15, 16, 94, 95). This oxidizing effect may be reversed with the use of reducing agents such as
sodium ascorbate or ascorbic acid (15, 16, 94-97) so that it would be possible to acid-etch and
bond immediately to endodontically treated teeth where sodium hypochlorite had been used as
an irrigating solution. Additionally, the manufacturer also claims that previous irrigation of the
root canal with sodium hypochlorite might negatively affect the bonding strength of the primer,
thus suggesting that the last irrigant to be used should be sterile water (2% chlorhexidine
18
gluconate does not affect the bond strength). Also lubricants containing peroxide might delay the
setting of the resins, so they should be rinsed with sterile water as well.
In vitro studies have shown that specimens where self-etching adhesives had been used
experienced a quick loss of structural integrity after aqueous aging (98). This was due to the
water content that was present within the dentinal tubules that might have inhibited the
polymerization of the acidic monomers. Also, the components that constitute the self-adhesive
systems are hydrophilic which enhances water sorption and hydrolytic breakdown in the mouth
(99) so after their application, the hybrid layers that are formed behave as semi-permeable
membranes that allow water movement across the bonded interface even after adhesive
polymerization (100).
A sealer should favor the reorganization of injured structures and should not interfere with tissue
repair. Numerous studies have reported that hydrophilic methacrylate resins can absorb water
largely in the resin matrix (101) and elute unreacted monomers (mostly released during the first
few days) which might promote cytotoxic reactions (102-104) and promote bacterial growth
(31).
Concerns over the toxicity of resin-based endodontic sealers were raised by several investigators.
Ames et al. (105) conducted a study where MetaSEAL, RealSeal SE and EndoREZ were tested
in self-cured mode, which is the mode of setting relevant to the apical third of the canal walls
and within the perirradicular tissues, thus representing the worst possible situation in which a
sealer would perform in a clinical scenario. The cytotoxicity of the methacrylate resin-based
sealers was investigated by the 3-(4, 5-dimethyl-thiazoyl)-2,5-diphenyl-tetrazolium bromide
assay, which measures cell viability by assessing its succinate dehydrogenase activity. All sealers
were severely cytotoxic at 72 hours after mixing. RealSeal SE was moderately cytotoxic during
the first two weeks, mildly cytotoxic at weeks 3-4 and nontoxic after the fifth week. The above
studies highlight the importance of a prolonged testing period in order to be able to detect long
19
term release of toxic un- polymerized components from the material due to the reduced degree of
conversion at the apex.
2.6.2.3 Total-etch bonding agents
These systems use an acid etching process (most commonly 30-40% phosphoric acid) in an
attempt to completely remove the smear layer, open the dentinal tubules and demineralise the
dentin leaving an exposed collagen matrix (106). Rinsing will remove the dissolved mineral
component of dentine and the remaining irrigating solutions or interaction by-products. This step
is followed by application of primer and a bonding agent, provided in 2 separate bottles (in
contrast to the SE system where all components are dispensed simultaneously). According to the
manufacturer (3M ESPE, St Paul, MN, USA), Scotchbond multi-purpose primer contains: water,
methacrylic acid, 2-hydroxyethyl ester, (2-hydroxyethyl-methacrylate) and ploycarboxylic acid.
The catalyst contains: bisphenol A diglycidyl ether dimethacrylate, methacrylic acid, 2-
hydroxyethyl ester and benzoyl peroxide. During the priming, the hydrophilic monomers that
diffuse across the demineralised dentin stabilize the hydrated collagen network and displace
water with polymerizable monomers (107). Then, the adhesive resins are applied to the primed
dentin and later polymerized.
After applying the adhesive system, the methacrylate based resin composites are applied. These
can be either light-cured (one component system) or self-cured (two component systems). One
self cure system is Bisfil II (BISCO, Schaumburg, IL, USA) t. According to the manufacturer,
Bisfil II composite is composed of a base paste. This resin system is mainly composed of Bis-
GMA, triethyleneglycol dimethacrylate (TEGDMA), glass fillers and amorphous silica.
The bonding mechanism of etch-and-rinse adhesives to dentin is primarily diffusion-based and
depends upon hybridization or infiltration of resin within the exposed collagen scaffold. The
adhesive resin fills the porosities between the collagen fibers forming resin tags that seal the
20
dentinal tubules that have been opened; they initiate the polymerization reaction, stabilize the
hybrid layer and provide enough methacrylate double bonds for copolymerization with the resin.
As the demineralised collagen fibril mesh is used as the bonding substrate, a wet bonding
technique is required to insure its full expansion (108). But even if the resin monomers are able
to penetrate the dentin, if the polymerization is not adequate, the resin-dentin bond might be
compromised. Several factors influence the degree of conversion inside the hybrid layer: the
mode of polymerization of the material (light-cured, chemically cured or a combination); the
area where the polymerization is initiated; the number of available double-carbon bonds and the
presence of substances that might inhibit the polymerization (traces of irrigation solutions,
lubricants, etc).
Even though most of the available systems that use the three bonding steps can produce high
resin bonding strengths, excessive etching of the dentin can produce a weak bonding because the
collagen fibers at the base are not completely impregnated by the resin (109). Also if the area is
dried in excess the collagen network can collapse. Another factor that must be taken into
consideration is the unfavorable cavity configuration present in a root canal system, where the
volume of monomer is reduced creating sufficient shrinkage stresses to debond the material from
the dentin decreasing retention thus increasing leakage (14).
Methacrylate resin-based total-etch systems are widely used in restorative dentistry as they
produce the most durable bond (24). However, no total-etch endodontic sealers are commercially
available, possibly because of application challenges within the root canal configuration.
Ceballos et al (108) evaluated the bond strength of total-etch versus self-etch adhesives to caries-
free versus normal dentine, and found that the total-etch systems yielded higher bond strength
values. Similarly, Bouillaguet et al (107) evaluated the microtensile bond strength of eight
different adhesive systems in vitro in bovine teeth and reported that Scotchbond 1 exhibited the
third highest tensile bond values (18.9 ± 3.2 MPa). This three step ethanol-water-based etch-and-

21
rinse adhesion strategy is the most conventional and effective approach to obtain an efficient,
durable and stable bond (24) and remains the gold standard technique in restorative dentistry.
2.7 Degradation of the bond between methacrylate resins and
dentin
The resin-dentin interface can undergo degradation over time, allowing salivary and tissue fluid
movement between the hybrid layer and dentin (24, 27, 28, 92) with consequent breakdown of
the covalent bonds within collagen fibrils and resin polymers (30). This process begins when the
dentin is acid-etched (110). Collagen degradation is enhanced by enzymes, particularly dentinal
matrix metalloproteinases (MMPs) (28) which degrade the collagen component of the hybrid
layer. Incorporation of MMP inhibitors, such as chlorhexidine (99) into the endodontic treatment
regimen and into future methacrylate-based sealers may arrest degradation of the hybrid layer
(20).
Methacrylate adhesives can also degrade in aqueous solution and salivary esterases can catalyze
this process and increase the degradation of the resin-dentin interface at a greater rate (27, 29). It
has been proven that after prolonged exposure of a restoration to the fluids present in the oral
cavity, water begins to penetrate the resin (101) promoting chemical hydrolysis of ester bonds in
the material. If the pH is neutral, the process will be slow, but in the presence of bacteria where
the pH might significantly drop, the process might be accelerated. “The carboxylate and alcohol
degradation products of ester hydrolysis are more hydrophilic than the parent ester, further
enhancing the local ingress of water” (92). These ester linkages are the weakest link, thus
considered one of the main reasons for resin degradation within the hybrid layer (111).
22
2.8 Quality Assessment of the sealer-dentin interface
Researchers have characterized the interface between sealers and root dentin using different
models.
2.8.1 In vitro models
When assessment of the quality of the root filling is investigated, in vitro microleakage studies
have been the most widely used approach due to their ease, reproducibility and cost. Initially,
dyes and tracers had been used (112); saliva (113-115); fluid filtration models (116, 117);
bacteria and endotoxins (9, 118, 119); glucose filtration (120) among many others with
questionable clinical relevance (83).
Bond strength has been used as a measure of adhesion quality (25, 121). However, it only
assesses mechanical properties and not interfacial porosity. It has been demonstrated that the
push-out strength for EndoREZ (in MPa) was 8.7±4.3, 9.1±2.9 and 7.6±2.1 for the coronal,
middle and apical thirds; for MetaSEAL 18.6±4.8, 18.2±4.8 and 16.1±4.6 and for RealSeal SE
12.6±4.3, 14.9±5.5 and 14.4±8.1 (25), but it should be noted that in this study a final rinse with
EDTA was performed following manufacturer’s instructions, thereby not being able to assess the
true self-etching potential of RealSeal and MetaSEAL, the two self-adhering resin-based sealers.
All push-out strengths values were independent of the location of the radicular dentin. The
authors concluded that the self-adhesive sealers exhibited higher push-out strengths than the non-
etching sealer and that the variations in tubular density or sclerotic dentin along the canal wall
would not be factors that would alter the mechanical retention of the studied sealers.
More recently, using the non-invasive confocal laser scanning microscopy (CLSM),
Kermanshahi et al (27) characterized the salivary enzyme catalyzed degradation of restorative
23
resin-dentin interfaces by measuring the extent of interfacial bacterial cells and biofilms of a
major species associated with dental caries, Streptococcus mutans. They used a constant media
model simulating in-vivo pathogenic oral conditions (27). Where hybrid layer disruption and
marginal gaps were present, bacterial biofilms proliferated into the resin-dentin interface and
invaded the dentinal tubules (27). This system utilizes both biologically relevant and
microbiological components, making it highly relevant to in vivo settings.
2.8.2 In vivo models
In vivo research encompasses both animal studies and results stemming from outcomes in
clinical practice. Several studies were conducted using dog models, where teeth with endodontic
fillings were challenged through bacterial ingress and later histological analysis was performed
to evaluate the response of the periradicular tissues to different tested materials (40, 122, 123).
However, correlation between these results and clinical outcomes is not straightforward as
demonstrated by Pitt Ford (124) where he showed a lack of correlation between dye penetration
and periapical tissue response in dogs’ teeth. This is further demonstrated by the fact that dye
penetration through root-filled teeth was shown to occur in teeth that had been clinically
successful (125). In clinical practice, only the patient’s signs and symptoms can be considered
as outcome predictors, as their treated teeth cannot be extracted and evaluated for
presence/absence of flaws. Conventional two-dimensional radiographs have limited ability in
assessing three-dimensional objects (126). More recently, cone beam CT (CBCT) has been
employed to assess the quality of endodontic treatment. Much speculation has been surrounding
this new diagnostic modality, and some concerns were raised about the amount of radiation that
patients would receive. Many studies were conducted in this regard, but analysis of their results
is difficult due to the multiple differences among them (different machines, technical parameters,
measurement methods, etc). Overall, it has been demonstrated that CBCT results in doses that
are three to seven times those of panoramic doses and 40% less than conventional CT doses
(127).
24
Chapter 3
3 Materials and Methods
3.1 Specimen Preparation
Human caries-free teeth with single canals were collected after extractions from anonymous
patients in an Oral Surgery practice (University of Toronto Human Ethics Protocol #24315). The
teeth were kept frozen until used. The teeth were inspected for cracks under the operating
microscope at 10X magnification. Cracked teeth were discarded and replaced with new ones,
until 45 suitable teeth were selected. To disinfect and prevent further bacterial contamination,
teeth were sterilized with Gamma irradiation (4080 Gy), shown not to alter the structure and
permeability of dentin (128). Endodontic treatment procedures leading to root filling were
performed in a sterility-controlled environment to avoid contamination (Labculture® Class II
Type A2 Biohazard Safety Cabinet, Esco Micro Pte Ltd, Singapore).
The tooth crowns were severed at the cemento-enamel junction. Canals were negotiated to the
apical foramen with K-files (Lexicon Flex SSK, Dentsply Tulsa Dental Specialties, Tulsa, OK,
USA) and cleaned and shaped with ProTaper rotary instruments (Dentsply Tulsa Dental
Specialties, Tulsa, OK, USA) up to a size F4 at the foramen, while being intermittently irrigated
with 5 mL of 5.25% of sodium hypochlorite (NaOCl) using a 30 gauge needle. The last rinse
with 5 mL of 5.25% NaOCl was activated with the EndoActivator (Dentsply Tulsa Dental
Specialties, Tulsa, OK, USA) to sonically agitate the irrigation solution, two cycles of 30
seconds each. Smear layer was removed with 5 mL of 17% EDTA solution (Vista Dental,
Racine, WI, USA), followed with 5 mL of 5.25% NaOCl and a final flush with 10 mL of
25
distilled water. Canals were dried with paper points. After the completion of cleaning and
shaping, teeth were randomly divided into three experimental groups and the canals filled.
A ProTaper #40 gutta-percha master cone was fitted in the canal to working length with
excellent tug-back. The selected sealer for each group was placed in the canal, master cone
inserted, seared off with an Elements System B plugger handpiece (SybronEndo, Orange, CA,
USA) for down-pack leaving the apical 3 mm of gutta-percha in the canal.
Group 1 (n=18): Self-etch sealer: RealSeal SE sealer (SybronEndo, Orange, CA) was
dispensed from the auto mix syringe and placed onto a sterile glass slab, then introduced into
the canal lumen using a Lentulo spiral filler (Dentsply Tulsa Dental Specialties, Tulsa, OK,
USA). Excess sealer was removed with paper points to ascertain uniform coating of the canal
walls with only a thin layer of sealer. The canal lumen was then filled with thermo-plasticized
RealSeal SE injectable gutta-percha (SybronEndo, Orange, CA, USA) using an Elements
obturation unit extruder handpiece (SybronEndo, Orange, CA, USA) with a 23 gauge needle
tip and at a temperature setting of 115°C. The coronal end of the root filling was condensed
with Schilder pluggers (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) to offset
shrinkage of the filling core mass and additionally light cured the coronal aspect for 40
seconds with Spectrum curing light unit (Dentsply Tulsa Dental Specialties, Tulsa, OK,
USA). According to the manufacturer, the sealer in the canal will self-cure within 45 minutes.
Group 2 (n=18): Total-etch system: 37% phosphoric acid without benzalkonium chloride
(BAC) (Bisco, Schaumburg, IL, USA) was used to etch the root canal walls for 15 seconds,
then rinsed with sterile water for 15 seconds and dried with compressed air (Memorex Air
Duster, Imation Enterprises Corp, Oakdale, MN, USA) for 5 seconds. Adper Scotchbond
multi-purpose primer (3M ESPE, St Paul, MN, USA) was applied to the etched dentin
surface and was dried gently for 5 seconds. Adper Scotchbond multi-purpose adhesive (3M
ESPE, St Paul, MN, USA) was applied to the primed dentin and was lightcured for 10
seconds. Equal amounts of base and catalyst of Bisfil 2B self-cured resin (BISCO,
26
Schaumburg, IL, USA) were dispensed on a sterile glass slab and mixed until paste was
uniform (15 seconds) and was placed in the canal with a K-file #40 (Lexicon Flex SSK,
Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) to coat the walls uniformly. RealSeal SE
gutta-percha points were added passively until the canal lumen was filled. Excess was
removed with Elements System B plugger handpiece (SybronEndo, Orange, CA, USA) and
condensed with Schilder pluggers (Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) to
offset shrinkage of the filling core mass.
Group 3 (n=18): Epoxy-resin sealer (AH Plus, Dentsply De Trey, Konstanz, Switzerland) and
gutta-percha. AH 26 sealer was dispensed on a sterile glass slab (equal amounts of both pastes
were mixed to a homogeneous consistency which broke when lifted 2 cm above the glass
slab), then introduced into the canal lumen using a Lentulo spiral filler (Dentsply Tulsa Dental
Specialties, Tulsa, OK, USA ). Excess sealer was removed with paper points to ascertain
uniform coating of the canal walls with only a thin layer of sealer. The canal lumen was then
filled with thermo-plasticized RealSeal SE injectable gutta-percha (SybronEndo, Orange, CA,
USA) using an Elements obturation unit extruder handpiece (SybronEndo, Orange, CA,
USA) with a 23 gauge needle tip and at a temperature setting of 115°C. The coronal end of the
root filling was condensed with Schilder pluggers (Dentsply Tulsa Dental Specialties, Tulsa,
OK, USA) to offset shrinkage of the filling core mass. This combination was selected after
results from a previous study that demonstrated that a more cohesive “monoblock” could be
obtained in a root canal when combining Resilon core material with the epoxy resin–based
sealer (AH-26) rather than Epiphany sealer (129).
All filled roots were stored for 72 hours in a 100% humid environment at 37°C (Hera Cell 150,
Heraeus, Newton, CT, USA) to allow the sealers to completely set. Subsequently, each root was
sectioned horizontally at 5 mm from its coronal end using a low-speed water-cooled rotary
diamond disc (Brasseler, Savannah, GA, USA) under sterile conditions. The remaining portion
of the roots was discarded. In this manner, standardized 5 mm-thick root dentin blocks with
filled canal lumens were obtained. Use of only the coronal portion of the roots was intended to
standardize specimens avoiding canal irregularities frequently encountered in the middle and
apical portions. Also, the coronal portion of root dentin is the most critical for investigation,
27
being the first challenged by bacteria invading through the pulp chamber (130). An indentation
with a round bur was performed on the coronal aspect of each specimen to clearly distinguish it
from the apical, so as to standardize the positioning for microscopic observation as described
below.
In all block specimens, the cementum periphery and exposed dentin on the coronal and apical
surfaces adjacent to the filled root canal margins was sealed with two layers of clear nail varnish
(Revlon, Mississauga, ON, Canada; no formaldehyde) to block cut dentinal tubules from access
to the sealer-dentin interface.
3.2 Degradation media incubation of specimens
Specimens underwent different incubation periods to expose the sealer-dentin interface to
potential degradation, before being incubated with E. faecalis (131).
Experimental groups: Three block specimens from each sealer group (Groups 1, 2, 3) were
incubated in sterile phosphate-buffered saline (Dulbecco's Phosphate Buffered Saline, containing
no calcium or magnesium; Invitrogen, Molecular Probes, Carlsbad, CA, USA) at 37°C, pH 7.0,
for each of the following periods:
7 days (n = 3/group)
1 month (n = 3/group)
3 months (n = 3/group)
6 months (n = 3/group)
28
3.3 Incubation of Specimens in Chemostat-Based Biofilm
Fermentor (CBBF)
At the end of their respective degradative incubation period, the specimens were suspended in a
chemostat-based biofilm fermentor (CBBF) (Appendix F). The continuous flow system consisted
of a 20 liter glass flask used as a reservoir to contain 16 liters of sterile TSB (BD Biosciences,
Sparks, MD, USA) that was supplemented with 200 cc of a 0.25% glucose (BDH Inc, Toronto,
Canada) solution that was placed on top of a hot plate stirrer (Corning stirrer, Corning, NY,
USA). The 0.25% glucose had been freshly prepared and filter-sterilized (Nalgene filters,
Thermo Fischer Scientific, Rochester, NY, USA). The tubing (LS25, Masterflex Precision pump
tubing, Cole Parmer instruments Co., Vernon Hills, IL, USA) coming from the flask was
attached to a drop counter to avoid any backflow and possible contamination due to negative
pressure back into the flask. Media flowed through the silicone tubing through a peristaltic pump
(Bio Rad Econo column pump; Hercules, CA, USA) that regulated the inflow rate into the glass
vessel that contained the samples in 400 cc sterile TSB in which 5 mL glucose had been added.
Another silicone tubing (LS16, Masterflex Precision pump tubing, Cole Parmer instruments Co.,
Vernon Hills, IL, USA, pumped out media through another peristaltic pump (Masterflex L/S,
Cole Parmer, Niles, IL, USA) and emptied into a waste vessel. All components of the system
were sterilized prior to each run by autoclaving at 121°C for 45 min (PRIMUS sterilizer Mc
Davis; North York, ON, Canada).Temperature in the fermentor’s vessel was set at 37°C and was
controlled through a temperature controller unit (Cole Parmer, Niles, IL, USA).
A mono-culture biofilm of E. faecalis (ATCC 47077) was established on the specimens for 7
days, through continuous flow of fresh medium (TSB supplemented with 0.25% glucose) which
was pumped into the vessel at a flow rate of 0.72 L/day (132) at a dilution rate of D=0.075/hour,
mimicking the resting flow rate of saliva over human oral tissues. E. faecalis was selected
because it is non-fastidious, biofilm-forming microorganism commonly found in the endodontic
flora of infected root-filled teeth (62, 133). The specific, non-pathogenic ATCC 47077 strain was
selected to meet the laboratory biosafety Level 1 requirement. After incubation in the CBBF, the
specimens were aseptically removed, gently rinsed with sterile phosphate-buffered saline and
29
stained using dihydroethidium (Invitrogen, Molecular Probes, Carlsbad, CA, USA). They were
then subjected to microscopic examination within 1 hour after staining, while maintained wet in
sterile PBS buffer.
Controls: To provide a baseline for bacterial presence and morphology for the subsequent
microscopic examination, one specimen from each sealer group (Groups 1, 2, 3) was subjected to
each one of the following procedures:
A. No pre-incubation, incubation in the CBBF without inoculation, staining.
B. No pre-incubation, incubation in the CBBF with inoculation, staining.
C. No pre-incubation, no incubation in the CBBF, staining.
3.4 Reflected Light Microscopy (RLM) Analysis
Biofilm proliferation and individual bacterial cell penetration were measured in specimens
stained with dihydroethidium (Invitrogen, Molecular Probes, Carlsbad, CA) using an
epifluorescence setup of the Leica DMIRE2 inverted microscope (Leica Microsystems; Wetzlar,
Germany). Red fluorescence of dihydroethidium was visualized by the TX2 filter cube
(excitation BP560/40, dichroic 595 nm, emission BP645/75). The object positioning was
controlled by an XY piezo Z stage (MS-2000, Applied Scientific Instrumentation Inc.).
Fluorescence imaging was performed by a black and white CCD camera (Hamamatsu) and
processed by a Power PC G5 (Apple Computer, Inc.Cupertino, CA, USA) using Openlab 4.0.2.
Software (Improvision Inc., Waltham, Massachussets, USA.). Selection of the regions of interest
(ROI) were performed by randomly assigning a “north” in the uppermost portion of the
specimen, and then establishing the corresponding opposite “south”, “east” and “west” for each
(all performed at 5X original magnification) (Fig. 12). Subsequently, those ROI were plotted into
a “map” and processed by a Power PC G5 (Apple Computer, Inc. Cupertino, CA, USA) using
Openlab 4.0.2 software (Improvision Inc., Waltham, Massachussets, USA.) (Fig. 13). The
30
imaging operations were programmable (using Openlab Automation) which substantially sped
up repetitive procedures and made them less invasive by reducing the irradiation of specimens.
Additionally, the software allows for re-evaluation of an area of interest multiple times, focusing
on the exact same analyzed point, as long as samples are not moved from the stage. Analysis of
the samples was performed in a corono-apical direction, establishing the zero at the base of the
sample (where it was contacting the base of the well) and progressing in an apical direction for
up to 500 µm, which was the maximum threshold available. Z stacks were obtained, establishing
the surface of the specimen as the zero, and in 5 µm incremental slices up to a maximum depth
of 500 µm. The depth of field was ± 1 µm.
Outcome measures: The depth of biofilm formation and bacterial invasion along the sealer-
dentin interface was recorded in microns from coronal to apical direction of the specimens.
Pictures were taken through the microscope’s eyepiece (Fig. 14) at 5X original magnification
and further analyzed at 10 X original magnification (Fig. 15).
3.5 Scanning Electron Microscopy (SEM) Analysis
Specimens were subjected to increasing concentrations of ethanol (30, 50, 70, 90, 95 and 100%)
for dehydration. Specimens were dried using a critical point dryer (Polaron CPD7501 critical
point dryer; Fisons instruments; Structure Probe Inc / SPI Supplies; West Chester, PA, USA).
Samples were sputter coated with platinum in a SEM coating system (Polaron coater SC515;
Fisons instruments; Structure Probe Inc / SPI Supplies; West Chester, PA, USA) and examined
by SEM (Hitachi S-2500; Sapporo, Japan) at 10 kV, (Fig. 16, 17).
31
3.6 Microbiological controls
Assessment of bacterial viability was conducted with the plate count method. Serial dilutions
(10-1
to 10-7
) were conducted both for the media obtained for the overnight culture and for the
media collected from the CBBF after the 1 week inoculation for each group aged for different
periods and for the controls, and plated onto BHI agar plates (and repeated in duplicates) (Fig.
7). Numbers of viable cells for the different time points (1 week, 1 month, 3 months and 6 month
samples) were comparable.
Gram staining was conducted for characterization of type of bacterial cells present in the media
extracted from the fermentor after 1 week inoculation and to confirm that a monospecies had
been growing. Results indicated homogeneity (Fig. 8).
PBS contained in the sterile vials where samples had been stored for the different degradation
times was analyzed. Undiluted media was plated in triplicate for each sample, and no growth was
observed for all the tested samples (Fig. 9).
• Samples were prepared with each sealer, stored individually in sterile vials for 72 hours
in a 100% humid environment at 37°C in a tri-gas cell culture incubator (HeraCell 150,
Heraeus, Newtown, CT, USA) to allow the sealers to completely set. They were then
placed in BHI, incubated at 37°C w/ 5% CO2 and OD600 readings were taken at 24, 48
and 72 hs. Results: no growth confirming sterility of samples.

32
3.7 Statistical Analysis
All study groups were run in parallel, with three independent samples in each group. One-way
ANOVA and LSD’ post-hoc analysis was conducted to determine the effect of sealer type and
incubation time on biofilm proliferation and bacterial penetration along the sealer-dentin
interface. The independent variables are the sealer type and the incubation time before
inoculation with bacteria. The dependent variables were biofilm proliferation and total bacterial
cells observed within the resin-sealer interface. The level of confidence was set to 95%.
33
Chapter 4
4 Article
Note: The following was submitted to the Journal of Endodontics
Proliferation of Pathogenic Biofilms within Sealer-Root Dentin
Interfaces is Affected by Sealer Type and Aging Period
Karina A Roth 1, DDS, Shimon Friedman
1 DMD, Céline M Lévesque PhD
2, Bettina R
Basrani DDS, PhD 1
and Yoav Finer DMD, PhD, FRCD(C)3
From the 1Discipline of Endodontics,
2Oral Microbiology and
3Biomaterials, Faculty of
Dentistry, University of Toronto, Toronto, Ontario, Canada.
Address requests for reprints to Dr Yoav Finer; Discipline of Biomaterials, Department of
Biological Sciences, Faculty of Dentistry, University of Toronto, Toronto, Ontario, Canada
Fax number: (416) 979-4760
Phone number: (416) 979-4903 ext. 4554
E-mail address: [email protected]

34
Acknowledgements: Stephanie Koyanagi; Richard Mair; Milos Legner, Babak Shokati, Jian
Wang.
Grants: The American Association of Endodontists Foundation, Alpha Omega Fraternity, Endo
Tech, Canadian Association of Endodontists Endowment Fund.
Sources of support: Dentsply Tulsa Dental Specialties; SybronEndo; Endo Tech.
Abstract
Background: Root canal fillings are intended to prevent microbial proliferation over time in the
canal after treatment. Objective: To assess biofilm proliferation within the sealer-dentin
interfaces of two methacrylate resin-based systems, self-etch (SE) and total-etch (TE), and an
epoxy resin-based sealer (EP), aged for up to 6 months. Methods: Standardized specimens
(n=45) comprising the coronal 5 mm of human roots were filled with the test materials and gutta-
percha. Specimens were either not pre-incubated (control; n=9), or incubated in sterile saline for
1 week, 1 month, 3 months or 6 months days (n=3/group). Monospecies biofilms of
Enterococcus faecalis were grown on the specimens for 7 days in a chemostat-based biofilm
fermentor mimicking pathogenic oral conditions. The extent of E. faecalis proliferation within
the sealer-dentin interface for each material and incubation period group was assessed using
fluorescence microscopy of dihydroethidium-stained specimens. Results: TE had less biofilm
proliferation than both EP and SE (p<0.01). Deeper biofilm proliferation was detected in SE and
EP specimens aged for 1 and 3 months than those aged for 1 week or 6 months (p<0.05).
Maximum depth of biofilm penetration was recorded for SE at 1 month (p<0.05). Conclusion:
Within the test model used, the self-etch and epoxy resin-based sealers were more susceptible to
interfacial biofilm proliferation than the total-etch restorative material. This susceptibility
diminished after aging the materials’ interfaces for 6 months.
Key words: resin-dentin interface, endodontic sealer, resin-composite, biofilm, E faecalis,
fluorescence microscopy
35
Introduction
Root canal fillings, comprising a core and a flowable sealer, should prevent bacterial ingress into
the canal after treatment (1). Sealers that adhere or bond to root dentin are expected to resist
bacterial proliferation within the sealer-dentin interface (2). Epoxy resin (ER)-based sealers
adhere to dentin and are considered the “gold standard” (3). Methacrylate resin (MR)-based
sealers bond to conditioned dentin (4) by penetrating the tubules (5) and interlocking with dentin
collagen forming a hybrid layer (6, 7). Two main MR-based systems are currently available: i)
“Total-etch” systems, requiring acid-etching, priming and bonding to form a hybrid layer (7).
Although they are the benchmark for bonded restorative systems (6), they are not available as
commercial endodontic sealers. ii) “Self-etch” systems employ one-step etching, priming and
bonding, incorporating the smear layer into the hybrid layer (8). They are available as endodontic
sealers, but concerns have recently emerged about inadequacy of their bond (8).
Bonding MR-based sealers to root dentin is challenging (9). Resin polymerization is inhibited by
dentin exposure to sodium hypochlorite (10), shrinkage-related debonding occurs due to
unfavorable cavity configuration (11), and interfacial degradation over time, allowing salivary
and tissue fluid movement between the hybrid layer and dentin (12), may lead to bacterial
proliferation and re-infection of the tooth (13).
Sealer-dentin interfaces have been studied using in-vitro static models measuring penetration of
dyes (14), endotoxins (15), inoculated bacteria (16) or saliva (17), with questionable clinical
relevance (18). Recently, our group has introduced the use of the chemostat-based biofilm
fermentor (CBBF) for assessment of interfacial bacterial biofilm proliferation of the cariogenic
biofilm organism Streptococcus mutans after aging of MR-dentin specimens (12). The purpose
of the present study was to assess biofilm proliferation within the sealer-dentin interface of two
MR-based systems, self-etch and total-etch, and an ER-based sealer, using the CBBF model.
36
Material and Methods
Specimen preparation and aging
Intact, human teeth with single canals (University of Toronto Human Ethics Protocol #24315)
were sterilized by gamma-irradiation (4080Gy) (19) and decoronated at the cemento-enamel
junction. Canals were prepared with ProTaper rotary instruments (Dentsply, Tulsa, OK), to size
F4 with intermittent 5.25% sodium-hypochlorite irrigation, flushed with 10mL distilled water
and dried with paper points. Roots were randomly divided into three sealer type groups
(n=18/group): EP, an ER-based sealer (AH Plus Dentsply, Konstanz, Switzerland); SE, a MR-
based self-etch sealer (RealSeal, SybronEndo, Orange, CA); TE, a MR-based total-etch
restorative material (Adper Scotchbond multi-purpose, 3M, St Paul, MN and Bisfil 2B self-cured
resin, Bisco, Schaumburg, IL).
In EP and SE, sealers were applied with a Lentulo (Dentsply), canals filled with injectable gutta-
percha (Elements, SybronEndo) compacted with Schilder pluggers (Dentsply), and the coronal
end light-cured (SE only). Canals in TE were etched with 37% phosphoric acid (Bisco) for 15
sec, rinsed with sterile water for 15 sec, lightly air-dried, treated with Scotchbond primer and
adhesive, light-cured, coated with Bisfil 2B, and filled with RealSeal SE gutta-percha points
(SybronEndo) using passive lateral compaction.
Filled roots were stored for 72hrs at 37°C and 100% humidity (Hera Cell 150, Heraeus, Newton,
CT), and sectioned horizontally 5mm from the coronal end with a slow-speed water-cooled
rotary diamond disc (Brasseler, Savannah, GA) under sterile conditions, obtaining standardized
5mm-long specimens. Peripheral cementum, apical surfaces and exposed coronal dentin adjacent
to root fillings were coated with nail varnish to prevent bacterial access to the sealer-dentin
interface through cut dentinal tubules. Specimens were subjected to aging in vials with sterile
37
phosphate-buffered saline (PBS), incubated (37°C, pH 7.0) for 7 days, 1, 3 or 6 months
(n=3/material group/time).
Biofilm cultivation
Aged specimens were suspended in CBBF (37°C) to cultivate monospecies biofilms of
Enterococcus faecalis (ATCC 47077) over interfacial margins (12), under continuous flow of
fresh Tryptic Soy Broth (BD Bioscience, Sparks, MD) with 0.25% (wt/vol) glucose, at 0.72L/d
(20) and dilution rate D=0.075/hr mimicking the resting salivary flow rate (13).
Specimens were aseptically removed after 7 days and gently rinsed with sterile PBS. To assess
bacterial viability, a 10 mL sample was collected from each vial, serially-diluted, and spot-plated
in triplicate onto Brain Heart Infusion agar for bacteria colony forming unit (CFU) counting after
24hr of incubation at 37°C. Bacterial counts in the order of 109
CFU/mL were obtained for all
tested samples.
Outcome assessment
Specimens were stained with dihydroethidium (Invitrogen, Molecular Probes, Carlsbad, CA) and
examined with an epifluorescence microscope (DMIRE2, Leica Microsystems; Wetzlar,
Germany). Red fluorescence was visualized with TX2 filter cube (excitation BP560/40, dichroic
595nm, emission BP645/75).
Biofilm proliferation and individual bacterial cell penetration were analyzed at 4 cardinal points
(100X magnification). Captured images (CCD; Hamamatsu, Shizuoka, Japan) were processed
38
(Openlab 4.0.2, Improvision, Waltham, MA) and Z-stack series established in a corono-apical
direction for each specimen in 5µm increments up to 500µm. Three-dimensional images of
biofilm formation were reconstructed from Z-stack series by Image J software (NIH).
Analysis
We performed one-way ANOVA and LSD post-hoc analysis (p<0.05) to determine the effects of
material and aging period on biofilm proliferation and bacterial cell penetration along the sealer-
dentin interfaces.
Results
Representative three-dimensional image reconstructions from Z-stack series captured from 1
month-aged specimens revealed different patterns of interfacial E. faecalis biofilm formation for
EP, SE and TE (Fig. 1, top). Z-stack images depict individual bacterial cells at different depths
within the interfaces of all test materials (Fig.1, bottom).
Mean interfacial biofilm proliferation depth ranged across test materials and aging periods (Fig.
2). Lumping aging periods together, biofilm proliferation depth differed significantly (p<0.005)
among test materials; TE had significantly less biofilm proliferation than EP and SE (p<0.01),
which did not differ significantly from each other.
SE and EP revealed biofilm proliferation for all aging periods with increased levels for
specimens aged for 1 and 3 months than those aged for 1 week or 6 months (p<0.05). Maximum
39
depth of biofilm proliferation was recorded for SE at 1 month (p<0.05). No biofilms were
detected for TE at 3 and 6 months periods.
Individual bacterial cells within the sealer-dentin interfaces were detected consistently deeper
than biofilm aggregates for all test materials at all aging periods (See Appendix J, Fig. 17). Their
mean depth ranged from 198±66µm for 6 month-aged TE specimens, to 431±21µm for 3 month-
aged EP specimens. TE showed less individual bacterial cell penetration depth than SE and EP
(p<0.05).
Discussion
Novel endodontic sealers require assessment with physiologically relevant models. Our
previously used experimental model (12) was adapted for assessment of root canal sealers’
interface with root dentin. Interfaces were post-aged in CBBF to simulate pathogenic intraoral
conditions, and subsequently challenged by E. faecalis, an endogenous oral bacterial species
frequently isolated in root canal infections (21). E. faecalis forms monospecies biofilms over
root dentin, survives disinfection regimens and nutritional deprivation, and invades filled canals
and dentinal tubules (22). Coronal-third root dentin was used, being the first challenged by
bacteria invading through the pulp chamber (13). Its structure differs from that of apical root
dentin where abundant branching and irregularities (23) preclude standardization of specimens.
Sealers that adhere or bond to dentin, a desirable property (24) expected to curtail interfacial
bacterial ingress and proliferation, were tested. ER-based AH Plus is widely used and frequently
tested against novel sealers (3). Scotchbond and Bisfil 2B are typical components of MR-based
total-etch systems, producing durable dentin bonds (6). This design allowed comparison of
RealSeal SE, representing the new direction of MR-based self-etch sealers, to the ER-based
40
sealer and MR-based total-etch restorative, both extensively tested and used clinically for many
years.
Interfacial bacterial ingress occurred consistently, with less biofilm proliferation than individual
bacterial cell penetration. Biofilm proliferation overall was deeper for SE than for TE, peaking in
specimens aged for 1 month when it was also deeper than for EP. The susceptibility of SE to
biofilm proliferation suggested that it did not fully satisfy the requirements for root filling
materials (24). After aging for 6 months, biofilm proliferation declined for SE and EP and was
undetected for TE, suggesting that prolonged aging of the materials’ interfaces might have
changed the ecological milieu in a manner that curtailed biofilm proliferation despite invasion of
individual bacterial cells. This change may be related to altered sealing capacity of the materials
(12) and to the materials' degradation by-products released into the interfacial margins (25).
Previous study showed that free-floating planktonic cells of E. faecalis readily invaded all
interfaces within 7 days of inoculation prior to formation of biofilms (26). This observation
supported the aforementioned hypothesis that the extent of biofilm proliferation could be
influenced by the ecological milieu within the interfaces, which in turn might be affected by
aging-related degradation.
Despite the ability of AH Plus to adhere to root dentin, its ability to resist bacterial invasion has
been disputed (27, 28). Adhesive and mixed failures of its bond with root dentin (29) might lead
to gaps where bacteria can invade and proliferate. Indeed, our results indicate that AH Plus was
susceptible to interfacial bacterial invasion, even though biofilm proliferation appeared to
diminish with prolonged aging of the sealer-dentin interface.
MR-based sealers are expected to form a micromechanical bond with root dentin, but undergo
biodegradation over time (12, 30) allowing bacterial invasion and biofilm formation (12, 16).
Interfacial areas where the resin does not completely infiltrate the dentin substrate, or where it
does not polymerize within the hybrid layer, are especially susceptible (31). RealSeal SE was
previously reported to be inferior to AH Plus (32). Our results indicated that after aging for 1
41
month, RealSeal SE was more susceptible to interfacial biofilm proliferation to a greater extent
than the total-etch and AH Plus systems. This phenomenon could be attributed to the greater
hydrophilicity of the self-etch MR-based system that promotes water sorption and hydrolytic
breakdown of the interface (33).
MR-based total-etch systems are widely used in restorative dentistry as they produce the most
durable bond (6). Acid etching enhanced bonding to cervical root canal dentin up to 200% (34).
Our results indicated that the total-etch restorative material was only minimally susceptible to
interfacial biofilm proliferation, and significantly less than the self-etch sealer. However, no
total-etch endodontic sealers are commercially available, possibly because of application
challenges within the root canal configuration. Thus, even though the self-etch sealers represent
an innovation (35), developing a sealer that would be impervious to interfacial biofilm
proliferation remains an elusive goal.
Conclusions
This study presented a non-invasive assessment of interfacial biofilm proliferation between
sealers and root dentin simulating pathogenic oral conditions. The self-etch and epoxy-resin
based endodontic sealers were more susceptible at early stages to interfacial biofilm proliferation
than the total-etch restorative material, but this susceptibility diminished after aging of the
materials’ interfaces for 6 months. Given the importance of biofilm forming processes in
protecting bacteria, and their relevance to disease pathogenesis, the experimental model
presented herein could be instrumental for testing novel strategies aimed at improving the
resistance of the sealer-dentin interface to bacterial invasion and biofilm proliferation.
42
REFERENCES
1. Nair PN. Apical periodontitis: a dynamic encounter between root canal infection
and host response. Periodontol 2000 1997;13:121-148.
2. Barthel CR, Zimmer S, Wussogk R, Roulet JF. Long-Term bacterial leakage along
obturated roots restored with temporary and adhesive fillings. J Endod 2001;27(9):559-
562.
3. Brackett MG, Martin R, Sword J, Oxford C, Rueggeberg FA, Tay FR, et al.
Comparison of seal after obturation techniques using a polydimethylsiloxane-based root
canal sealer. J Endod 2006;32(12):1188-1190.
4. Schwartz RS, Fransman R. Adhesive dentistry and endodontics: materials, clinical
strategies and procedures for restoration of access cavities: a review. J Endod
2005;31(3):151-165.
5. Tay FR, Loushine RJ, Monticelli F, Weller RN, Breschi L, Ferrari M, et al.
Effectiveness of resin-coated gutta-percha cones and a dual-cured, hydrophilic
methacrylate resin-based sealer in obturating root canals. J Endod 2005;31(9):659-664.
6. De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, et
al. A critical review of the durability of adhesion to tooth tissue: methods and results. J
Dent Res 2005;84(2):118-132.
7. Van Meerbeek B, De Munck J, Yoshida Y, Inoue S, Vargas M, Vijay P, et al.
Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future
challenges. Oper Dent 2003;28(3):215-235.
8. Babb BR, Loushine RJ, Bryan TE, Ames JM, Causey MS, Kim J, et al. Bonding of
self-adhesive (self-etching) root canal sealers to radicular dentin. J Endod 2009;35(4):578-
582.
9. Van Meerbeek B, Perdigao J, Lambrechts P, Vanherle G. The clinical performance
of adhesives. J Dent 1998;26(1):1-20.
10. Santos JN, Carrilho MR, De Goes MF, Zaia AA, Gomes BP, Souza-Filho FJ, et al.
Effect of chemical irrigants on the bond strength of a self-etching adhesive to pulp chamber
dentin. J Endod 2006;32(11):1088-1090.
11. Tay FR, Loushine RJ, Lambrechts P, Weller RN, Pashley DH. Geometric factors
affecting dentin bonding in root canals: a theoretical modeling approach. J Endod
2005;31(8):584-589.
12. Kermanshahi S, Santerre JP, Cvitkovitch DG, Finer Y. Biodegradation of resin-
dentin interfaces increases bacterial microleakage. J Dent Res 2010;89(9):996-1001.
43
13. Torabinejad M, Ung B, Kettering JD. In vitro bacterial penetration of coronally
unsealed endodontically treated teeth. J Endod 1990;16(12):566-569.
14. Stratton RK, Apicella MJ, Mines P. A fluid filtration comparison of gutta-percha
versus Resilon, a new soft resin endodontic obturation system. J Endod 2006;32(7):642-645.
15. Carratu P, Amato M, Riccitiello F, Rengo S. Evaluation of leakage of bacteria and
endotoxins in teeth treated endodontically by two different techniques. J Endod
2002;28(4):272-275.
16. Shipper G, Orstavik D, Teixeira FB, Trope M. An evaluation of microbial leakage
in roots filled with a thermoplastic synthetic polymer-based root canal filling material
(Resilon). J Endod 2004;30(5):342-347.
17. Khayat A, Lee SJ, Torabinejad M. Human saliva penetration of coronally unsealed
obturated root canals. J Endod 1993;19(9):458-461.
18. Wu MK, Wesselink PR. Endodontic leakage studies reconsidered. Part I.
Methodology, application and relevance. Int Endod J 1993;26(1):37-43.
19. White JM, Goodis HE, Marshall SJ, Marshall GW. Sterilization of teeth by gamma
radiation. J Dent Res 1994;73(9):1560-1567.
20. Pratten J, Andrews CS, Craig DQ, Wilson M. Structural studies of microcosm
dental plaques grown under different nutritional conditions. FEMS Microbiol Lett
2000;189(2):215-218.
21. Kaufman B, Spangberg L, Barry J, Fouad AF. Enterococcus spp. in endodontically
treated teeth with and without periradicular lesions. J Endod 2005;31(12):851-856.
22. Zehnder M, Guggenheim B. The mysterious appearance of enterococci in filled root
canals. Int Endod J 2009;42(4):277-287.
23. Mjor IA, Nordahl I. The density and branching of dentinal tubules in human teeth.
Arch Oral Biol 1996;41(5):401-412.
24. Grossman L. Antimicrobial effect of root canal cements. J Endod 1980;6(6):594-597.
25. Singh J, Khalichi P, Cvitkovitch DG, Santerre JP. Composite resin degradation
products from BisGMA monomer modulate the expression of genes associated with biofilm
formation and other virulence factors in Streptococcus mutans. J Biomed Mater Res A
2009;88(2):551-560.
26. Estrela C, Sydney GB, Figueiredo JA, Estrela CR. A model system to study
antimicrobial strategies in endodontic biofilms. J Appl Oral Sci 2009;17(2):87-91.
27. Hirai VH, da Silva Neto UX, Westphalen VP, Perin CP, Carneiro E, Fariniuk LF.
Comparative analysis of leakage in root canal fillings performed with gutta-percha and
Resilon cones with AH Plus and Epiphany sealers. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2010;109(2):e131-135.
44
28. Nawal RR, Parande M, Sehgal R, Rao NR, Naik A. A comparative evaluation of 3
root canal filling systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2011;111(3):387-393.
29. Teixeira CS, Alfredo E, Thome LH, Gariba-Silva R, Silva-Sousa YT, Sousa-Neto
MD. Adhesion of an endodontic sealer to dentin and gutta-percha: shear and push-out
bond strength measurements and SEM analysis. J Appl Oral Sci 2009;17(2):129-135.
30. Shokati B, Tam LE, Santerre JP, Finer Y. Effect of salivary esterase on the integrity
and fracture toughness of the dentin-resin interface. J Biomed Mater Res B Appl Biomater
2010;94(1):230-237.
31. Hashimoto M. A review--micromorphological evidence of degradation in resin-
dentin bonds and potential preventional solutions. J Biomed Mater Res B Appl Biomater
2010;92(1):268-280.
32. Saleh IM, Ruyter IE, Haapasalo M, Orstavik D. Bacterial penetration along
different root canal filling materials in the presence or absence of smear layer. Int Endod J
2008;41(1):32-40.
33. Yiu CK, King NM, Pashley DH, Suh BI, Carvalho RM, Carrilho MR, et al. Effect of
resin hydrophilicity and water storage on resin strength. Biomaterials 2004;25(26):5789-
5796.
34. Ferrari M, Mannocci F, Vichi A, Cagidiaco MC, Mjor IA. Bonding to root canal:
structural characteristics of the substrate. Am J Dent 2000;13(5):255-260.
35. Teixeira FB, Teixeira EC, Thompson J, Leinfelder KF, Trope M. Dentinal bonding
reaches the root canal system. J Esthet Restor Dent 2004;16(6):348-354; discussion 354.
45
Figure Legends
Figure 1. Top images- Representative three-dimensional reconstruction of select Z-stack series
of E faecalis biofilms captured from sealer-dentin interfaces of epoxy resin-based (EP), self-etch
(SE) and total-etch (TE) sealers, aged for 1 month. Specimens were dihydroethidium-stained and
examined using epifluorescence microscopy (excitation in the range of 560/40, dichroic 595 nm
and emission of 645/75 nm, 100X magnification). Analysis of the samples was performed in a
corono-apical direction, establishing the zero at the base of the sample (where it was contacting
the base of the well) and progressing in an apical direction for up to 500 µm, which was the
maximum threshold available. The depth of field was ± 1 µm. Three-dimensional Images were
reconstructed using Image J software (National Institutes of Health, Bethesda, MD). Levels of
luminescence demonstrate different patterns of biofilm formation for the different materials.
Bottom images- Representative Z-stack images of E. faecalis captured from the sealer-dentin
interface of specimens aged for 1 month. Images show differences in trends of biofilm presence
within the interface (µm from the specimen’s surface in an apical direction) for each material
group.
Figure 2: E faecalis biofilm formation along the sealer-dentin interfaces of epoxy resin-based
(EP), self-etch (SE) and total-etch (TE) methacrylate-based sealers. Specimens were aged in PBS
(37ºC, pH=7.0) for 1 week, 1, 3 and 6 months, then incubated with E. faecalis in biofilm forming
constant media conditions for 7 days. Mean ± SE values with same superscripts denote
statistically not-significant differences between groups (p > 0.05, one-way ANOVA, LSD post-
hoc test). Mean biofilms depths (from the specimen’s surface, in a corono-apical direction)
ranged from 0 to 355 ± 21 µm from the specimen’s surface. TE showed lower biofilm
proliferation than EP and SE (p<0.01). No biofilm were detected for TE specimens pre-incubated
for 3 and 6 months. Maximum depth of biofilm proliferation was recorded for SE at 1 month
(p<0.05).
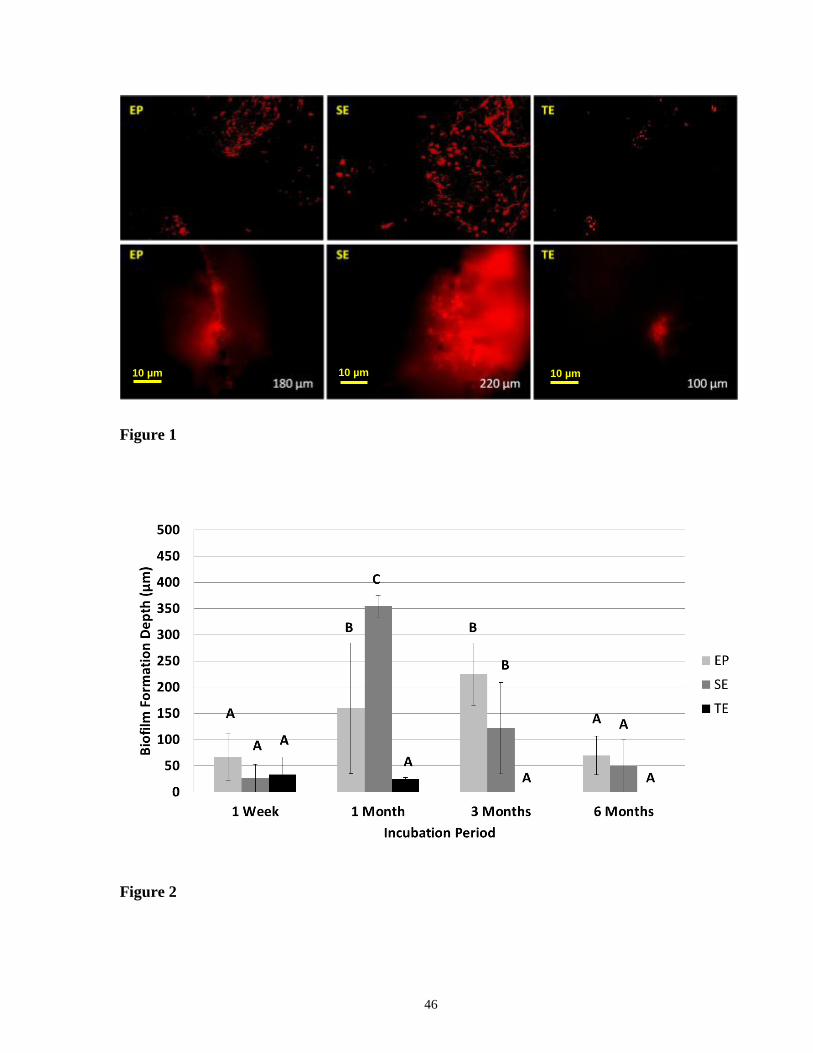
46
Figure 1
Figure 2
10 µm 10 µm 10 µm

47
Chapter 5
5 Discussion
Current and novel endodontic sealer systems require assessment with physiologically relevant
models. Our experimental model, based on previous research with S. mutans biofilms, coronal
dentin and MR-based restorative material (27), was adapted for assessment of root canal sealers’
interface with root dentin. Samples were individually kept in sterile glass vials containing PBS to
expose the interfaces to the different assigned study time points, after which, they were
asceptically removed and challenged with E faecalis in the chemostat-based biofilm fermentor to
simulate pathogenic intraoral conditions. These two separate phases were established in order to
separate the aging phase of the specimens (up to 6 months) from the exposure to bacteria in the
CBBF (all specimens being exposed for 7 days).
The previous timelines were chosen due to the fact that:
1. It is very demanding to run the CBBF for up to 6 months, with a high risk of contamination of
the samples.
2. There is limited space within the CBBF to accommodate all specimens from the different
groups and time frame for such a long period.
3. Different aging groups cannot be run in parallel due to the availability of a single vessel for
this purpose. Until complete run of the experiment for one group is completed, a subsequent one
48
cannot be studied. Use of a single vessel, eliminates the possibility of variation in the set-up
which could affect the outcomes.
4. Analysis of degradation products cannot be done in specimens from the CBBF due to the
continuous replacement of the media.
After sample shad been exposed to the different time points for degradation, they were
subsequently challenged by E. faecalis, a common constituent of the endodontic microflora in
root-filled teeth (59). E. faecalis forms monospecies biofilms over root dentin, survives
disinfection regimens and nutritional deprivation, and invades the filled canal and dentinal
tubules (63-67).
Specimens were prepared from the coronal portion of roots, the first challenged by bacteria
invading through the pulp chamber (130). Structure of root dentin differs from that of coronal
dentin, with abundant branching and irregularities in the apical area of the root (42) precluding
standardization of apical root segments.
We investigated sealers that can adhere or bond to root dentin, a desirable property (8) expected
to curtail microbial ingress. AH Plus is a widely used, epoxy-resin-based dentin-adhering sealer
(89), frequently used as the "gold standard" for comparison of novel sealers (18). RealSeal SE is
a typical MR-based self-etch sealer, while Scotchbond and Bisfil 2B comprise a typical MR-
based total-etch "gold standard" for dentin bonding restorative materials. This design allowed
49
comparison of the self-etch sealer, representing a new direction in root filling materials (134) , to
the ER-based sealer and MR-based total-etch restorative, both extensively tested and used
clinically for many years.
Biofilms develop preferentially on inert surfaces, or on dead tissue. A root canal system after
endodontic treatment has no defences against bacteria or their by-products. When biofilms are
formed, their structure protects the residing bacteria from environmental threats and host defense
mechanisms. Microorganisms in biofilm form show higher resistance to both antimicrobial
agents and host defense mechanisms when compared with planktonic cells (75-77). From an
endodontic perspective, it is possible to eradicate bacteria in planktonic state, and much harder to
eliminate well established biofilms.
Interfacial bacterial penetration was observed with all tested materials after all aging periods.
Biofilm proliferation consistently extended to less depth than that of planktonic bacteria.
Comparing the three test materials, SE allowed for significantly deeper biofilm proliferation than
TE, the “gold standard” for MR-based restorative materials. After aging for 1 month, biofilm
proliferation for SE was also deeper than for EP, the commonly used epoxy based-based sealer.
These findings suggested that after aging for 1 month, SE was more susceptible to biofilm
proliferation than the two widely used materials, and in this regard, it did not fully satisfy the
requirements for root filling materials (8). After aging for 6 months, biofilm proliferation for SE
and EP was comparable to aging for 1 week, and it was zero for TE, suggesting that with
prolonged aging, all test materials’ interfaces might have changed in a manner that curtailed
50
biofilm proliferation despite the invasion of planktonic bacteria. This suggestion was
substantiated by the comparison of the four aging periods, with 1 and 3 months showing
significantly deeper biofilm proliferation than 1 week and 6 months. The aging might have
affected changes in the ecological milieu, related to altered sealing capacity of the materials (27)
and to the materials' degradation by-products (32).
Interfacial invasion of planktonic bacterial cells in all materials and aging periods was expected,
as a stage preceding the formation of biofilms (135). Indeed, E. faecalis readily invaded all
interfaces within 7 days of inoculation, regardless of aging or material. This observation
supported the aforementioned suggestion that the extent of biofilm proliferation was affected by
the ecological milieu within the interfaces, which in turn was affected by aging-related
degradation.
Singh et al (32) reported a potential influence of resin monomer-derived biodegradation products
on biofilm formation. Hydrolysis of methacrylate monomers (such as TEGDMA) produces
biodegradation by-products such as methacrylic acid (MA) and triethylene glycol (TEG). These
by-products affect various cellular activities such as nutrient uptake, signal transduction, and
gene expression when directly contacting oral bacteria (31). For example, triethylene glycol
(TEG) proved to be a growth stimulant (136) being utilized as a carbon source by anaerobic
bacteria, and MA had an inhibitory effect on bacterial growth. Similarly, other degradation by-
product may affect bacterial growth and gene expression.
51
Comparable levels of bacterial cell penetration were measured for TE and SE specimens.
However, TE group had significantly lower biofilm formation vs. SE throughout the aging
periods, with no biofilm detected for 3 and 6 months aging groups. These findings lead to the
hypothesis that the material itself or possible breakdown products could perturb the local micro-
environment within the interfacial gap and inhibit bacterial growth (31, 32, 136). Concentration
of eluted components and degradation products from the sealer system could be relatively high in
such a small interfaces and in sufficient levels to affect biofilm formation. It is possible
therefore, that the difference in biofilm formation observed between SE and TE specimens, is
related to the materials’ different formulations and biostability.
Despite the ability of AH Plus to adhere to root dentin (89), its ability to resist bacterial invasion
has been disputed (137, 138). Adhesive and mixed failures of its bond with root dentin (19)
might lead to gaps where bacteria can proliferate. Indeed, our results indicate that AH Plus was
susceptible to interfacial bacterial invasion, even though biofilm proliferation appeared to
diminish with prolonged aging of the sealer-dentin interface.
MR-based sealers are expected to form a micromechanical bond with root dentin (91), but that
bond may undergo biodegradation over time (110) allowing bacterial invasion (10). Interfacial
areas where the resin did not completely infiltrate the dentin substrate, or where it did not
polymerize within the hybrid layer, are especially susceptible (139). In regards to bacterial
invasion, RealSeal SE was previously reported to be inferior to AH Plus (87). Indeed, our results
52
indicated that RealSeal SE was susceptible to interfacial biofilm proliferation to a greater extent
than the total-etch system and, after aging for 1 month, also the AH Plus sealer.
MR-based total-etch systems are widely used in restorative dentistry as they produce the most
durable bond (24). Acid etching enhanced bonding to cervical-level root canal dentin up to 200%
(140). Indeed, our results indicated that the total-etch restorative material was only minimally
susceptible to interfacial biofilm proliferation, and significantly less than the self-etch sealer.
However, as yet no total-etch endodontic sealers are commercially available, possibly because of
application challenges within the root canal configuration. Thus, even though the self-etch
sealers represent an innovation (134), developing a sealer that would be impervious to interfacial
biofilm proliferation remains an elusive goal.
The differences in dentin bonding mechanisms among the three test materials notwithstanding, it
should be taken into account that the high ratio of the bonded surface area in a cavity to the
unbounded surface area (C factor) present in root canals could affect shrinkage-related
debonding (14), potentially leading to bacterial ingress. During polymerization, the volume of
monomers is reduced, which creates sufficient shrinkage stresses to debond the material from
dentin, thereby decreasing retention and increasing leakage. Bonding of adhesive root-filling
materials to root canals is challenging due to the configuration of the root canal space. SEM
analysis revealed interfacial gaps along the sealer dentin interface of all specimens studied.
These gaps provided pathways for bacterial invasion and subsequent proliferation and biofilm
formation. A distinct pattern of gap formation amongst the different materials was found, with

53
larger gaps for SE, followed up EP, while the smallest gaps were found for TE. These findings
were consistent for all specimens at all time points. It can therefore be hypothesized that the
magnitude of the interfacial gap affected bacterial cell penetration, and even more significantly
affect biofilm formation within the interface as evidenced by the statistical results.
54
Chapter 6
6 Conclusions
This study presented a non-invasive assessment of interfacial biofilm proliferation between
sealers and root dentin simulating pathogenic oral conditions. The self-etch and epoxy-resin
based endodontic sealers were more susceptible at early stages to interfacial biofilm proliferation
than the total-etch restorative material, but this susceptibility diminished after aging of the
materials’ interfaces for 6 months. Given the importance of biofilm forming processes in
protecting bacteria, and their relevance to disease pathogenesis, the experimental model
presented herein could be instrumental for testing novel strategies aimed at improving the
resistance of the sealer-dentin interface to bacterial invasion and biofilm proliferation.
Overall, the total-etch system demonstrated less interfacial biofilm proliferation and penetration
of individual E. faecalis cells. Therefore, the null hypothesis that “that there will be no difference
in the interfacial bacterial penetration and biofilm proliferation of E. faecalis between root dentin
and three test materials (total-etch resin, self-etch sealer, epoxy resin sealer) following aging of
the interfaces for up to 6 months” is rejected.
55
Chapter 7
7 Recommendations
Improvements / modifications to the established protocol / future directions:
• Use of confocal microscopy to analyze bacterial cell and biofilm formation within the
resin-dentin interface. This will increase the optical resolution and contrast of the
acquired images due to its ability to eliminate out-of-focus light in specimens that are
thicker than the focal plane. Additionally, this technique is able to generate three
dimensional images by superimposing the obtained images without the need of additional
software or image transfer.
• Standardize to cylindrical samples: if further analysis could be conducted with the use of
confocal laser microscopy, due to the pattern of light reflection, samples must have
parallel walls to allow light transmission / reflection. Human roots, are tapered, thus
analysis through this modality is not possible unless modifications are made.
Alternatively, use of bovine teeth would not only have the benefit of more parallel root
canals, but also, due to their larger size, a wider area for analysis could be obtained.
• Use of more specific fluorescent dyes and/or markers. This will allow for better analysis
of bacterial cells and biofilms within the interface and reduce optical interference from
materials and tooth structures. For example utilization of the dead/live (Baclight) in
combination with confocal microscopy will allow for bacterial live/dead ratio and further
investigate if the eluted products exert any effects on bacteria at the different evaluated
time points.
56
• Human saliva and periapical tissues contain enzymes which are capable of degrading the
resin-dentin at accelerated manner compared with buffer alone. Evaluate performance
difference between the materials with relevant enzyme containing-degradative media will
provide better simulation of in-vivo conditions.
• Analysis of incubation media for the presence of degradation by-products. This will
allow for quantitative measurement of the degradation of the sealer materials and possible
correlation with actual degradation of the interface and interfacial biofilm proliferation.
57
Chapter 8
8 Appendices
Appendix A: MEDIA AND SOLUTIONS
Appendix B: GAMMA IRRADIATION
Appendix C: SAMPLE PREPARATION
Appendix D: STERILITY ASSAYS OF SPECIMEN PREPARATION
Appendix E: MICROBIOLOGY TECHNIQUES
Appendix F: CHEMOSTAT-BASED BIOFILM FERMENTOR SET-UP
Appendix G: STATISTICS
Appendix H: MICROSCOPIC IMAGES
Appendix I: SEM IMAGES
Appendix J: BACTERIAL CELL PENETRATION
Appendix K: ETHICS APPROVAL
58
APPENDIX A: MEDIA AND SOLUTIONS
Sterile glucose solutions
Stock solutions of glucose (1% (wt/vol), 20% (wt/vol)) were prepared by dissolving D-Glucose
Anhydrous (BDH Inc.) in sterile distilled deionised water (Milli-Q Gradient Millipore filter,
Fisher Scientific). The final volume was adjusted to 100 ml with sterile distilled deionised water
prior to filter sterilization. For bacterial growth, filter-sterilized glucose was added to the media
at a final concentration of 0.25% (vol/vol).
Trypticase Soy Broth (TSB)
Trypticase Soy Broth (TSB) was prepared by dissolving 30.0 g of Bacto Tryptic Soy Broth
powder (BD Biosciences) in 1.0 litre of distilled deionised water, and sterilized by autoclaving.
Brain Heart Infusion (BHI)
Brain Heart Infusion (BHI) broth and BHI agar were prepared by dissolving 37.0 g of Bacto BHI
or BHI agar (BD Biosciences) in 1.0 litre of distilled deionised water, and sterilized by
autoclaving.
59
APPENDIX B: GAMMA IRRADIATION
Human caries-free teeth, even if extracted for orthodontic reasons, are not free of bacteria. In
order to prepare samples that will be later inoculated with a specific type of microorganism, and
due to infection control concerns regarding the handling of teeth for research purposes, teeth
need to be sterilized by a process that does not affect their natural properties. Gamma irradiation
has been effectively used for sterilization purposes and has proven to be an effective system
(141) but there is the potential for changes in the dentin substrate after its utilization (142). De
Wald (143) in a literature review, concluded that Gamma radiation did not produce structural
changes in dentin as well as Brauer (144) or White et al. (128) that also found that gamma
radiation had no effect on dentin permeability, nor on structural changes of the dentin as
measured by Fourier transform infrared spectroscopy (FTIR) or ultraviolet-visible-near-infrared
(UV NISINIR) spectra.
Doses ranging between 7 kGy and 35 kGy are safe to use without causing alterations in the
dentin surface morphology. Most studies use doses of 25 kGy with an exposure time of 6 hours
which is capable of inactivating most microorganisms and showing no deleterious effect to
dentin (142) or enamel (145).
Consequently, samples were sent to the Gamma Irradiation services of the University of
Toronto’s Department of Environmental Nuclear Science, for processing.
Figure 3: Samples in sterile vial after being gamma irradiated.
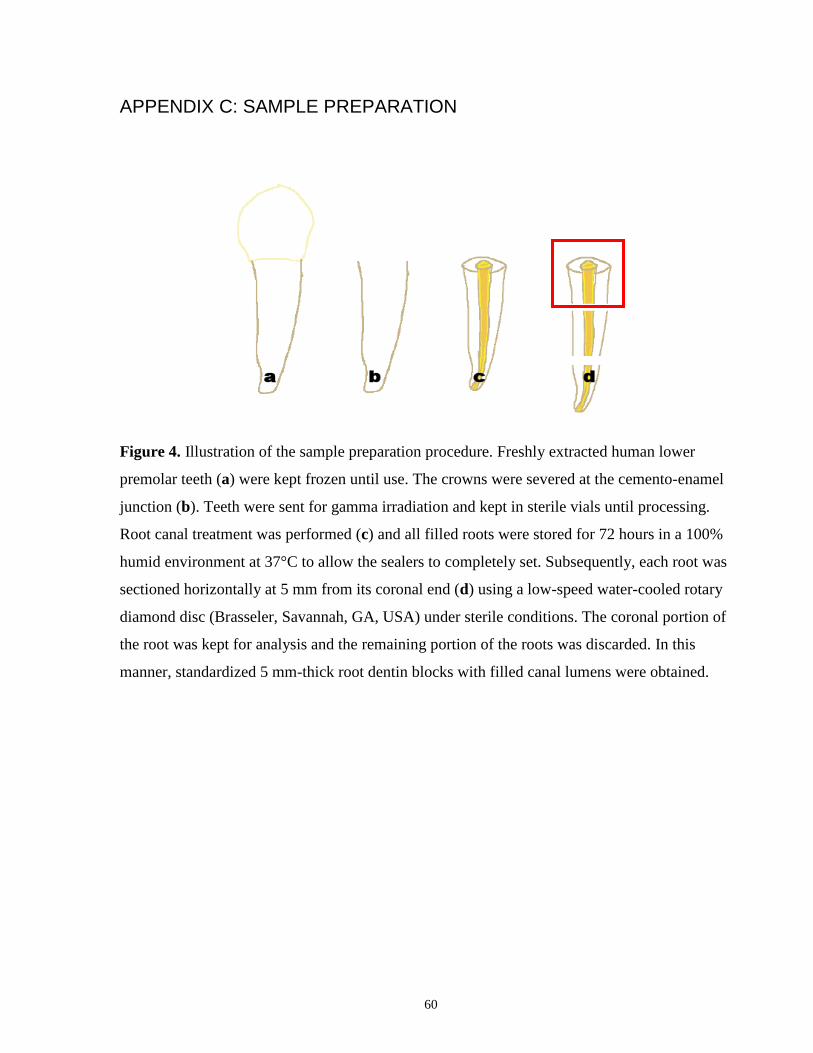
60
APPENDIX C: SAMPLE PREPARATION
Figure 4. Illustration of the sample preparation procedure. Freshly extracted human lower
premolar teeth (a) were kept frozen until use. The crowns were severed at the cemento-enamel
junction (b). Teeth were sent for gamma irradiation and kept in sterile vials until processing.
Root canal treatment was performed (c) and all filled roots were stored for 72 hours in a 100%
humid environment at 37°C to allow the sealers to completely set. Subsequently, each root was
sectioned horizontally at 5 mm from its coronal end (d) using a low-speed water-cooled rotary
diamond disc (Brasseler, Savannah, GA, USA) under sterile conditions. The coronal portion of
the root was kept for analysis and the remaining portion of the roots was discarded. In this
manner, standardized 5 mm-thick root dentin blocks with filled canal lumens were obtained.
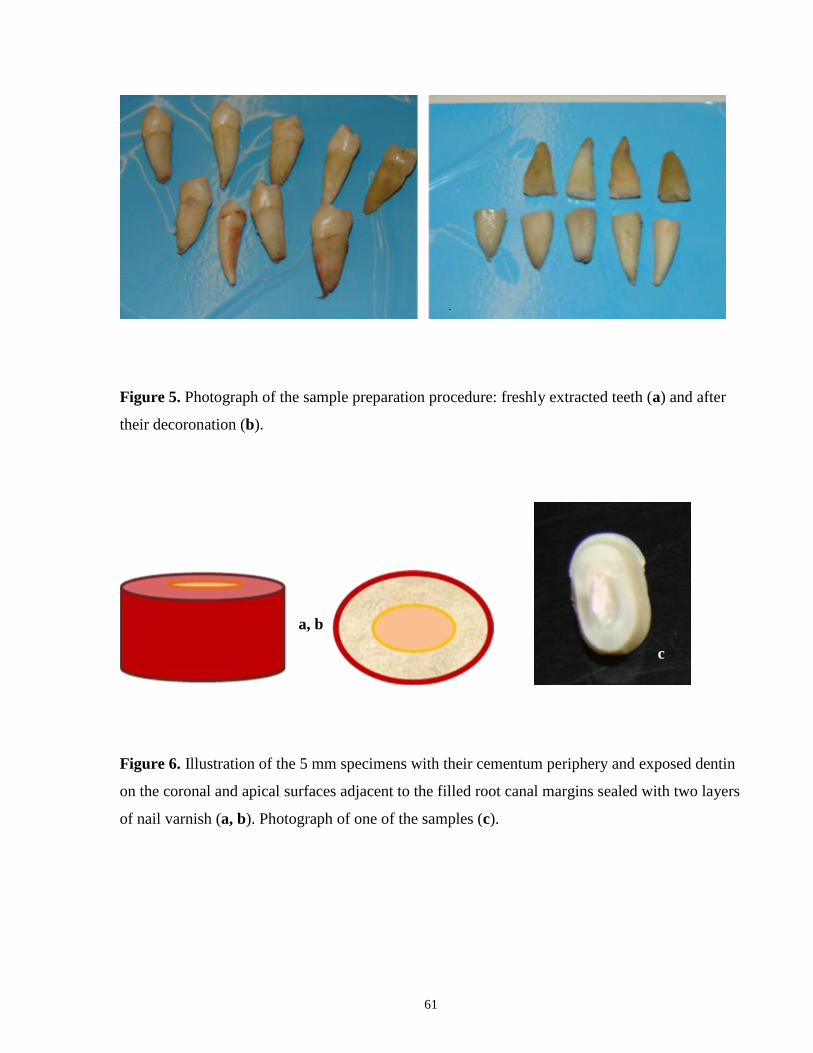
61
Figure 5. Photograph of the sample preparation procedure: freshly extracted teeth (a) and after
their decoronation (b).
Figure 6. Illustration of the 5 mm specimens with their cementum periphery and exposed dentin
on the coronal and apical surfaces adjacent to the filled root canal margins sealed with two layers
of nail varnish (a, b). Photograph of one of the samples (c).
a, b
c
a b
62
APPENDIX D: STERILITY ASSAYS OF SPECIMEN PREPARATION
INTRODUCTION
Pilot studies were run to assess the sterility of the chemostat-based biofilm fermentor (CBBF).
METHOD
The CBBF was run continuously for 7 days inside a laminar flow hood. Visual inspection of the
CBBF vessel and the inflow flask were performed on a daily basis to ensure that there could be
no problems and that biofilms were established and grown under carefully controlled conditions.
RESULTS
Contamination of the CBBF vessel occurred twice during pilot studies. For the first
contamination, we suspected that the problem might be due to backflow of media into the inflow
pump. A drop count mechanism was added to the system to overcome this problem. The second
contamination was most probably due to a problem with the outflow pump. The pump was
replaced and the outflow tubing was set accordingly to maintain the media levelled at 400 cc.
CONCLUSION
After the changes were implemented, the CBBF system was successfully run twice during a 7-
day period without any contamination.
63
APPENDIX E: MICROBIOLOGY TECHNIQUES
AGAR PLATE STOCK CULTURE
The wild-type strain Enterococcus faecalis ATCC 47077 was generously donated by Dr. Celine
Levesque from the Department of Oral Microbiology, Faculty of Dentistry. E. faecalis strain was
routinely cultured on BHI agar at 37°C. Bacteria were stored for up to one week on BHI-agar
plate at 4°C.
PREPARATION OF CULTURES FOR CBBF
The precultures were prepared as follows:
Day 1: Few colonies of E. faecalis grown on the surface of a BHI-agar plate were used to
inoculate 10 mL of TSB broth. The culture was incubated statically overnight at 37°C.
Day 2: The overnight preculture was diluted (1:20) into 30 ml of fresh TSB and incubated under
agitation at 37°C for 18 h.
Day 3: The overnight culture was diluted (1:30) into 400 ml of fresh TSB broth supplemented
with 0.25% sterile glucose inside the CBBF vessel.
SERIAL DILUTIONS
Bacterial viability was assessed by plate counting on BHI-agar. Briefly, serial dilutions (10-1
to
10-7
) were performed with sterile phosphate-buffered saline and 20 µl of diluted cells were spot-
plated in triplicates onto BHI-agar for enumeration. The colonies were counted after 24 h of
incubation at 37°C (Fig. 7). The results are given as colony forming units (CFU) per ml and are
presented at Table 1.
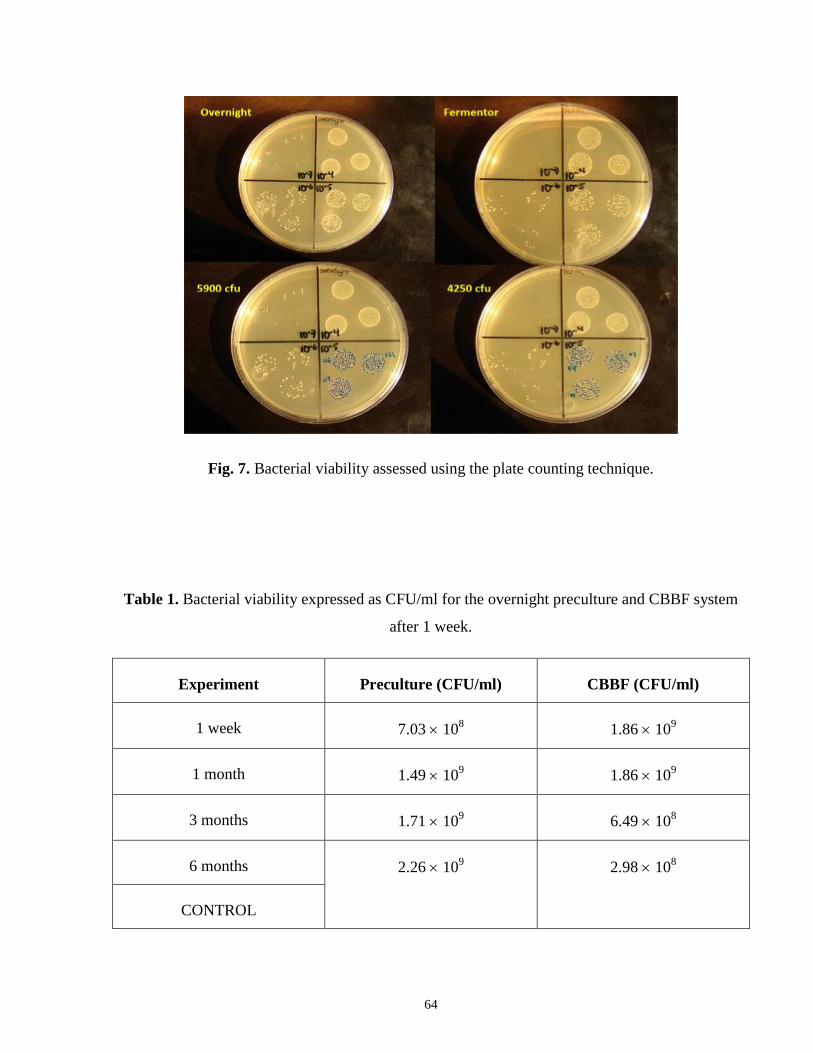
64
Fig. 7. Bacterial viability assessed using the plate counting technique.
Table 1. Bacterial viability expressed as CFU/ml for the overnight preculture and CBBF system
after 1 week.
Experiment Preculture (CFU/ml) CBBF (CFU/ml)
1 week 7.03 108 1.86 10
9
1 month 1.49 109 1.86 10
9
3 months 1.71 109 6.49 10
8
6 months 2.26 109 2.98 10
8
CONTROL
65
GRAM STAINING
Gram staining was performed on biofilm culture after one week to confirm culture purity.
Typical results are shown at Fig. 8.
Fig. 8. Gram stain of E. faecalis cultured into the CBBF after 1 week.
STERILITY CONTROL
Sample preparations were immersed into sterile phosphate-buffered saline (PBS) and kept into
vials at 37°C. To ensure that no contamination occurred during the PBS incubation, 20 µl of
immersing solution was spot-plated in triplicates onto BHI-agar for enumeration (Fig. 3). No
colonies were detected after 24 h of incubation at 37°C confirming the sterility of our
preparations.
Fig. 9. Analysis of immersing solution obtained from the vials.
66
APPENDIX F: CHEMOSTAT-BASED BIOFILM FERMENTOR SET-UP
Fig. 10. Individual components of the chemostat-based biofilm fermentor (CBBF)
Fig. 11. Image of the CBBF set-up within the laminar flowhood.
Prior to use, all components of the system were sterilized prior to each run by autoclaving at
121°C for 45 min (PRIMUS sterilizer Mc Davis; North York, ON, Canada). The system was
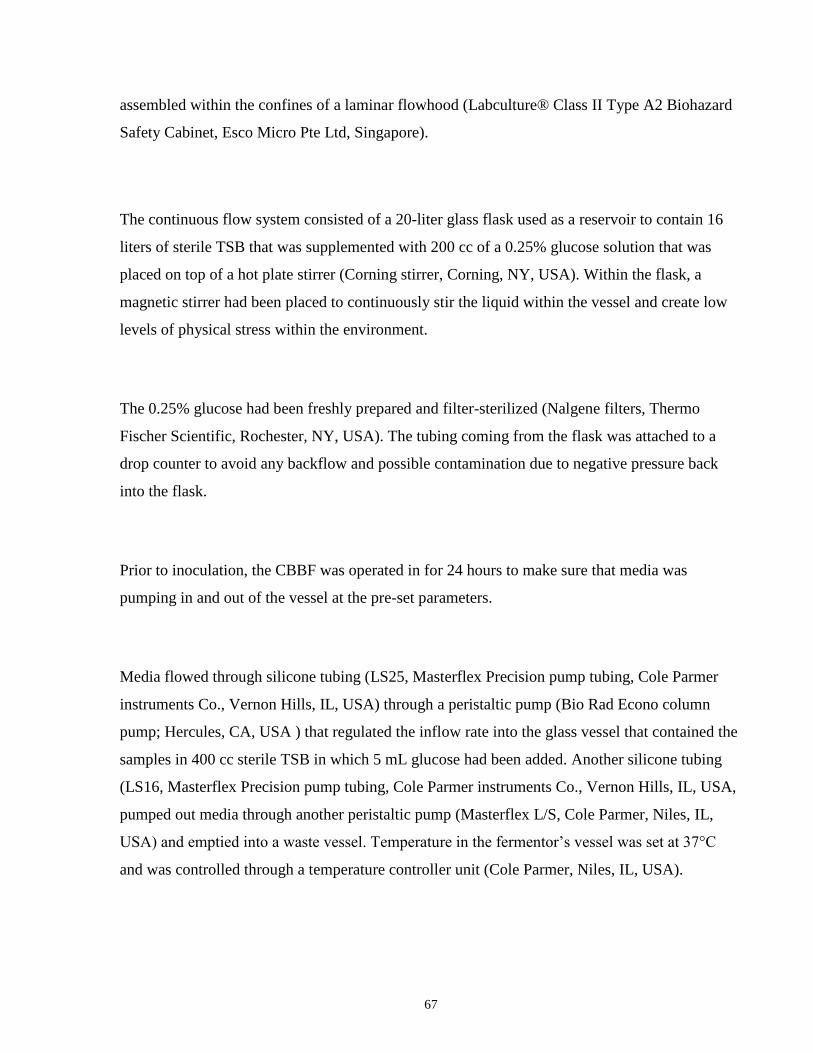
67
assembled within the confines of a laminar flowhood (Labculture® Class II Type A2 Biohazard
Safety Cabinet, Esco Micro Pte Ltd, Singapore).
The continuous flow system consisted of a 20-liter glass flask used as a reservoir to contain 16
liters of sterile TSB that was supplemented with 200 cc of a 0.25% glucose solution that was
placed on top of a hot plate stirrer (Corning stirrer, Corning, NY, USA). Within the flask, a
magnetic stirrer had been placed to continuously stir the liquid within the vessel and create low
levels of physical stress within the environment.
The 0.25% glucose had been freshly prepared and filter-sterilized (Nalgene filters, Thermo
Fischer Scientific, Rochester, NY, USA). The tubing coming from the flask was attached to a
drop counter to avoid any backflow and possible contamination due to negative pressure back
into the flask.
Prior to inoculation, the CBBF was operated in for 24 hours to make sure that media was
pumping in and out of the vessel at the pre-set parameters.
Media flowed through silicone tubing (LS25, Masterflex Precision pump tubing, Cole Parmer
instruments Co., Vernon Hills, IL, USA) through a peristaltic pump (Bio Rad Econo column
pump; Hercules, CA, USA ) that regulated the inflow rate into the glass vessel that contained the
samples in 400 cc sterile TSB in which 5 mL glucose had been added. Another silicone tubing
(LS16, Masterflex Precision pump tubing, Cole Parmer instruments Co., Vernon Hills, IL, USA,
pumped out media through another peristaltic pump (Masterflex L/S, Cole Parmer, Niles, IL,
USA) and emptied into a waste vessel. Temperature in the fermentor’s vessel was set at 37°C
and was controlled through a temperature controller unit (Cole Parmer, Niles, IL, USA).
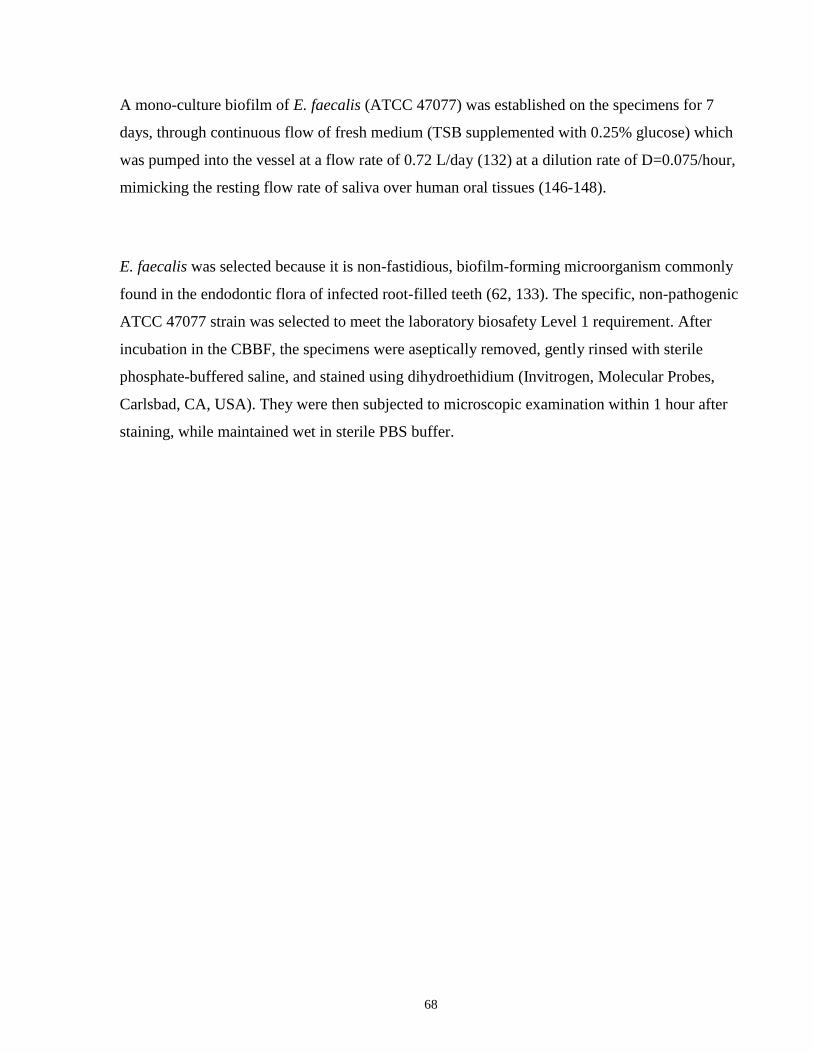
68
A mono-culture biofilm of E. faecalis (ATCC 47077) was established on the specimens for 7
days, through continuous flow of fresh medium (TSB supplemented with 0.25% glucose) which
was pumped into the vessel at a flow rate of 0.72 L/day (132) at a dilution rate of D=0.075/hour,
mimicking the resting flow rate of saliva over human oral tissues (146-148).
E. faecalis was selected because it is non-fastidious, biofilm-forming microorganism commonly
found in the endodontic flora of infected root-filled teeth (62, 133). The specific, non-pathogenic
ATCC 47077 strain was selected to meet the laboratory biosafety Level 1 requirement. After
incubation in the CBBF, the specimens were aseptically removed, gently rinsed with sterile
phosphate-buffered saline, and stained using dihydroethidium (Invitrogen, Molecular Probes,
Carlsbad, CA, USA). They were then subjected to microscopic examination within 1 hour after
staining, while maintained wet in sterile PBS buffer.
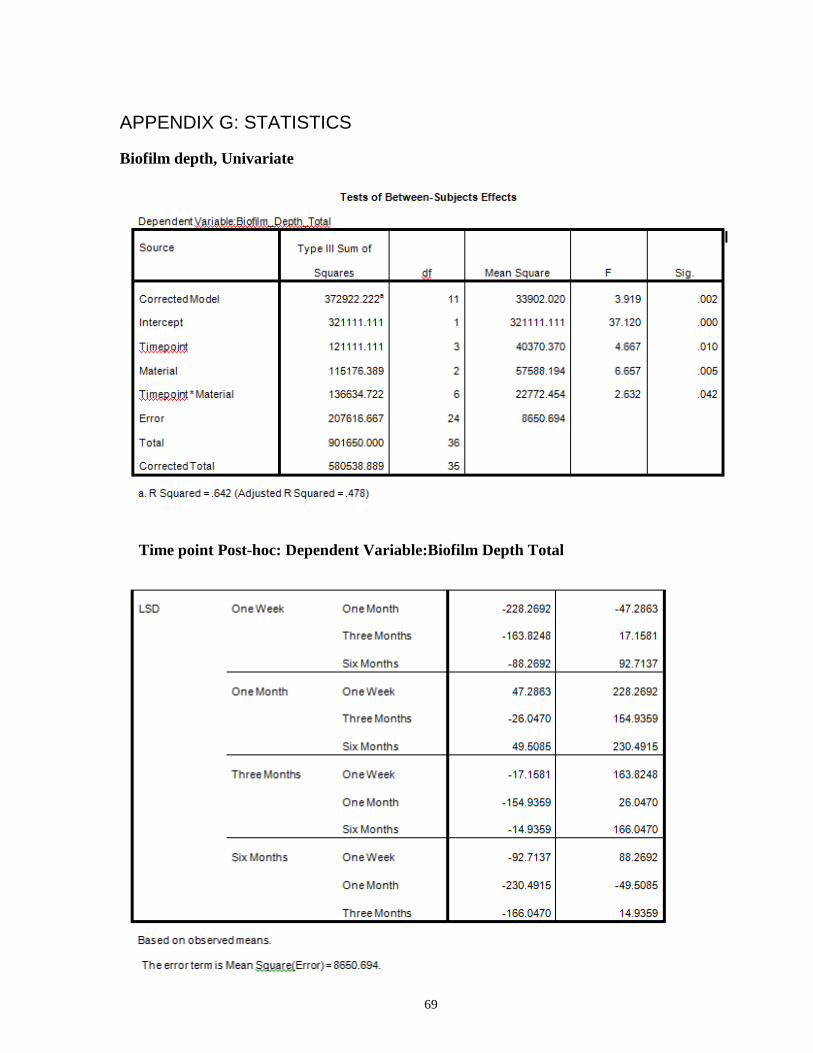
69
APPENDIX G: STATISTICS
Biofilm depth, Univariate
Time point Post-hoc: Dependent Variable:Biofilm Depth Total
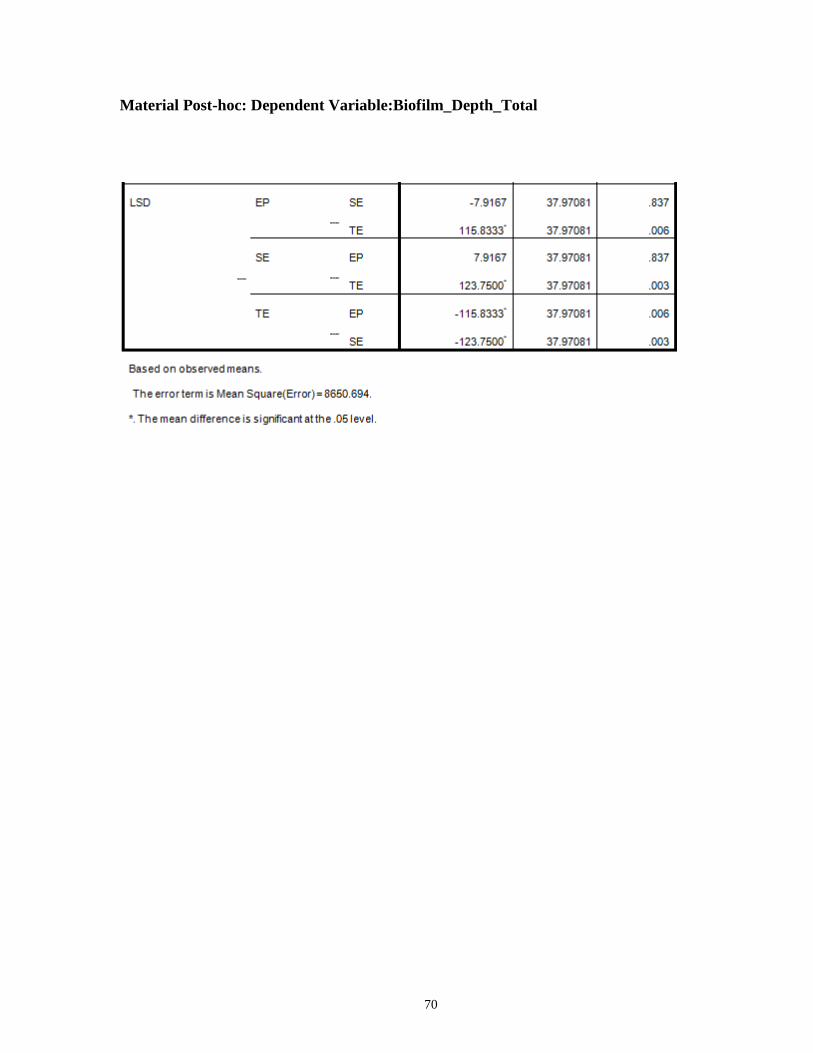
70
Material Post-hoc: Dependent Variable:Biofilm_Depth_Total
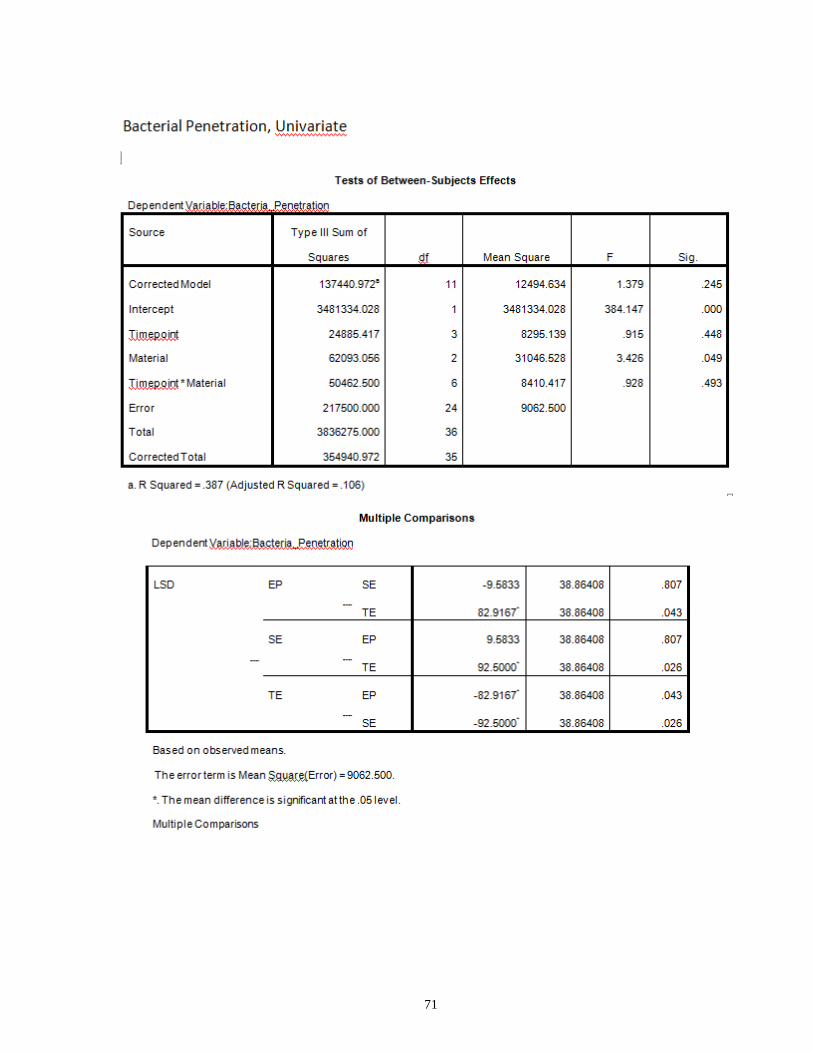
71
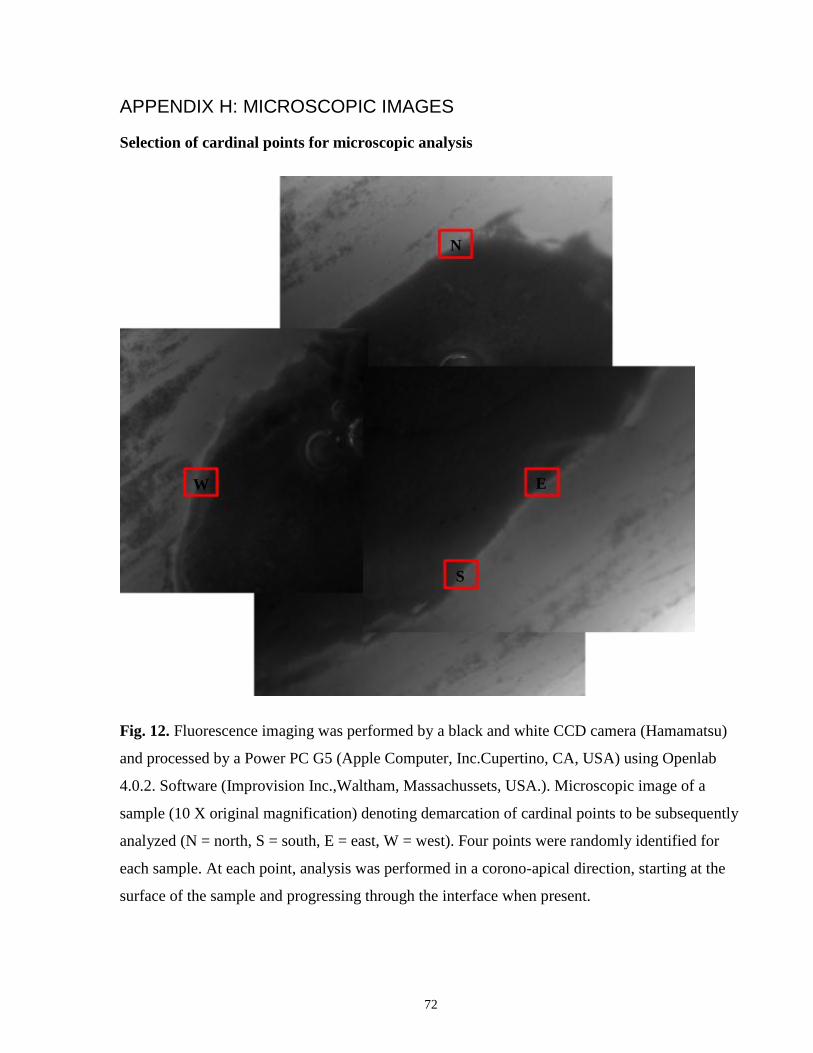
72
APPENDIX H: MICROSCOPIC IMAGES
Selection of cardinal points for microscopic analysis
Fig. 12. Fluorescence imaging was performed by a black and white CCD camera (Hamamatsu)
and processed by a Power PC G5 (Apple Computer, Inc.Cupertino, CA, USA) using Openlab
4.0.2. Software (Improvision Inc.,Waltham, Massachussets, USA.). Microscopic image of a
sample (10 X original magnification) denoting demarcation of cardinal points to be subsequently
analyzed (N = north, S = south, E = east, W = west). Four points were randomly identified for
each sample. At each point, analysis was performed in a corono-apical direction, starting at the
surface of the sample and progressing through the interface when present.
W E
N
S

73
Fig. 13. Selected points to be analyzed, were mapped and processed by a Power PC G5 (Apple
Computer, Inc.Cupertino, CA, USA) using Openlab 4.0.2. Software (Improvision Inc.,Waltham,
Massachussets, USA.). The imaging operations are programmable (using Openlab Automation)
which substantially speeds up repetitive procedures and makes them less invasive by reducing
the irradiation of specimens. Multiple samples and areas of interest can be mapped
simultaneously (in this image, 6 samples have been mapped). Additionally, the software allows
for re-evaluation of an area of interest multiple times, focusing on the exact same analyzed point,
as long as samples are not moved from the stage. Magnified view of the representative four
cardinal points (red square).
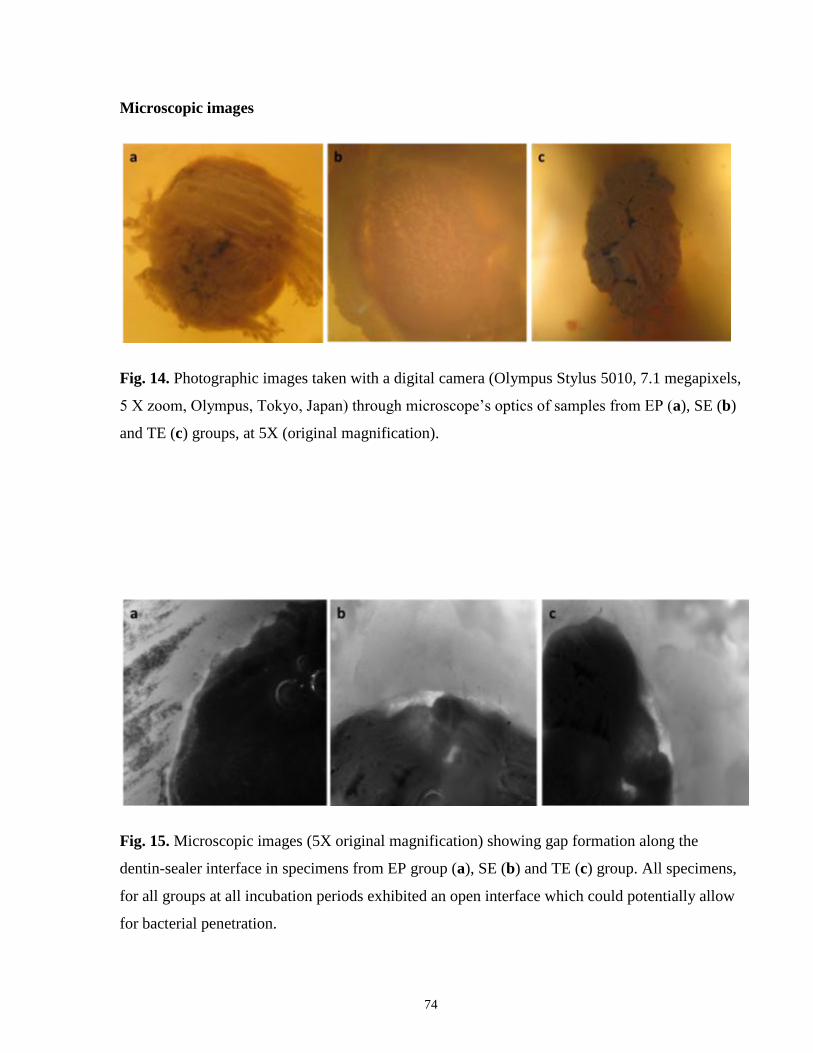
74
Microscopic images
Fig. 14. Photographic images taken with a digital camera (Olympus Stylus 5010, 7.1 megapixels,
5 X zoom, Olympus, Tokyo, Japan) through microscope’s optics of samples from EP (a), SE (b)
and TE (c) groups, at 5X (original magnification).
Fig. 15. Microscopic images (5X original magnification) showing gap formation along the
dentin-sealer interface in specimens from EP group (a), SE (b) and TE (c) group. All specimens,
for all groups at all incubation periods exhibited an open interface which could potentially allow
for bacterial penetration.

75
APPENDIX I: SEM IMAGES
Scanning electron microscopy produces high resolution images of a sample surface which allows
visualization of details which are smaller than 1 µm. Due to its large depth of field, a three-
dimensional appearance is obtained, which is useful for analyzing the surface structure of a
sample.
Specimens were subjected to increasing concentrations of ethanol (30, 50, 70, 90, 95 and 100%)
for dehydration. Specimens were dried using a critical point dryer (Polaron CPD7501 critical
point dryer; Fisons instruments; Structure Probe Inc / SPI Supplies; West Chester, PA, USA).
Samples were sputter coated with platinum in a SEM coating system (Polaron coater SC515;
Fisons instruments; Structure Probe Inc / SPI Supplies; West Chester, PA, USA) and examined
by SEM (Hitachi S-2500; Sapporo, Japan) at 10 kV, Fig. 16.
After SEM analysis, a different and distinct pattern of gap formation was observed for specimens
filled with the different test materials, which held true and consistent for all specimens within a
group at all time points analyzed. Wider gaps were consistently observed for SE specimens,
followed by EP and finally TE specimens revealed the smallest. It can therefore be hypothesized
that the magnitude of the interfacial gap affected bacterial cell penetration, and even more
significantly affect biofilm formation within the interface. .
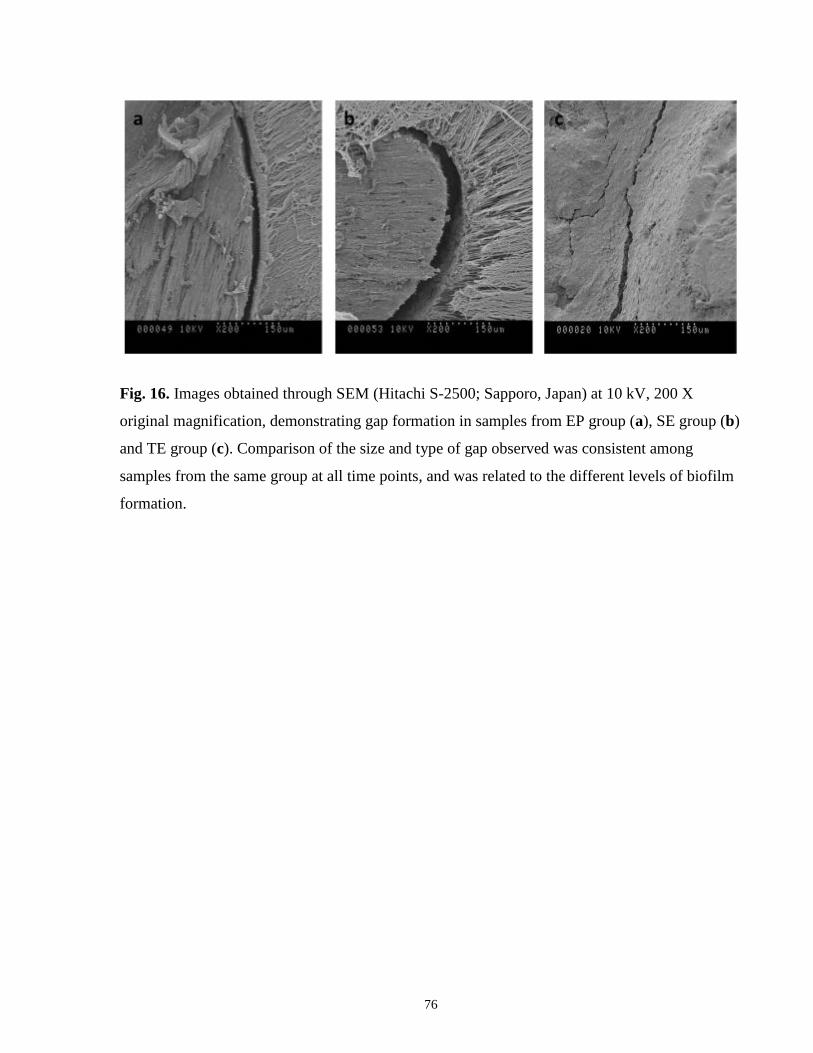
76
Fig. 16. Images obtained through SEM (Hitachi S-2500; Sapporo, Japan) at 10 kV, 200 X
original magnification, demonstrating gap formation in samples from EP group (a), SE group (b)
and TE group (c). Comparison of the size and type of gap observed was consistent among
samples from the same group at all time points, and was related to the different levels of biofilm
formation.
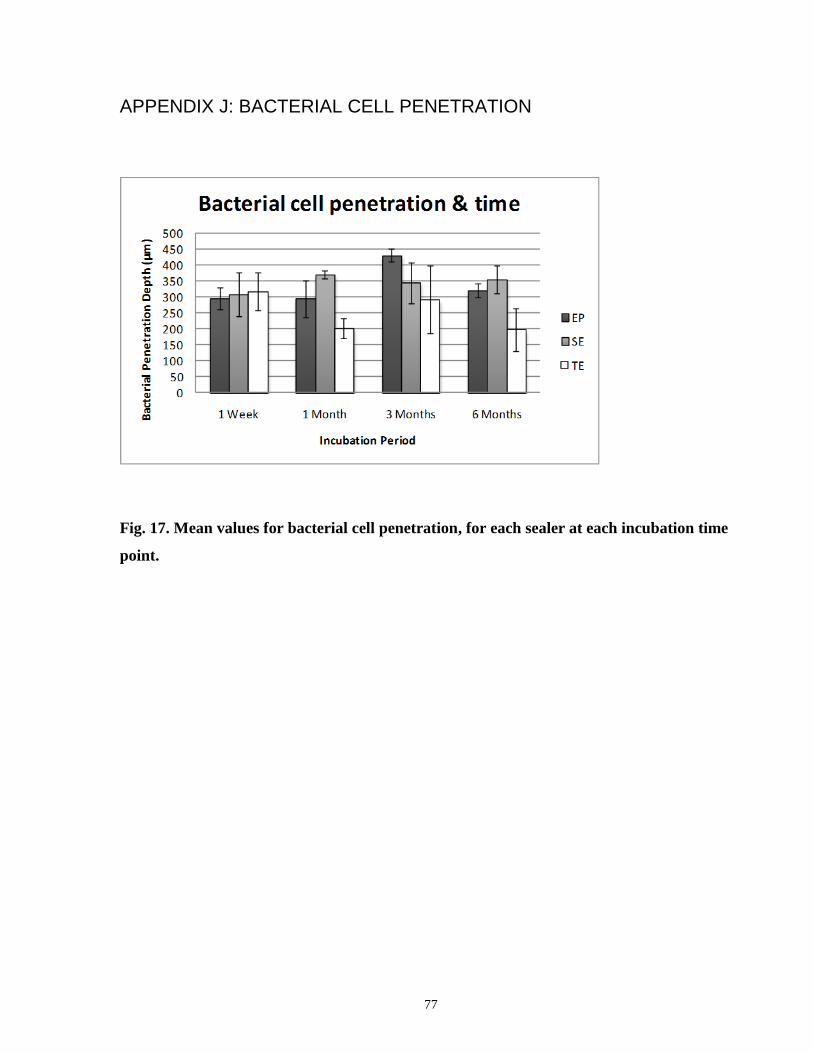
77
APPENDIX J: BACTERIAL CELL PENETRATION
Fig. 17. Mean values for bacterial cell penetration, for each sealer at each incubation time
point.
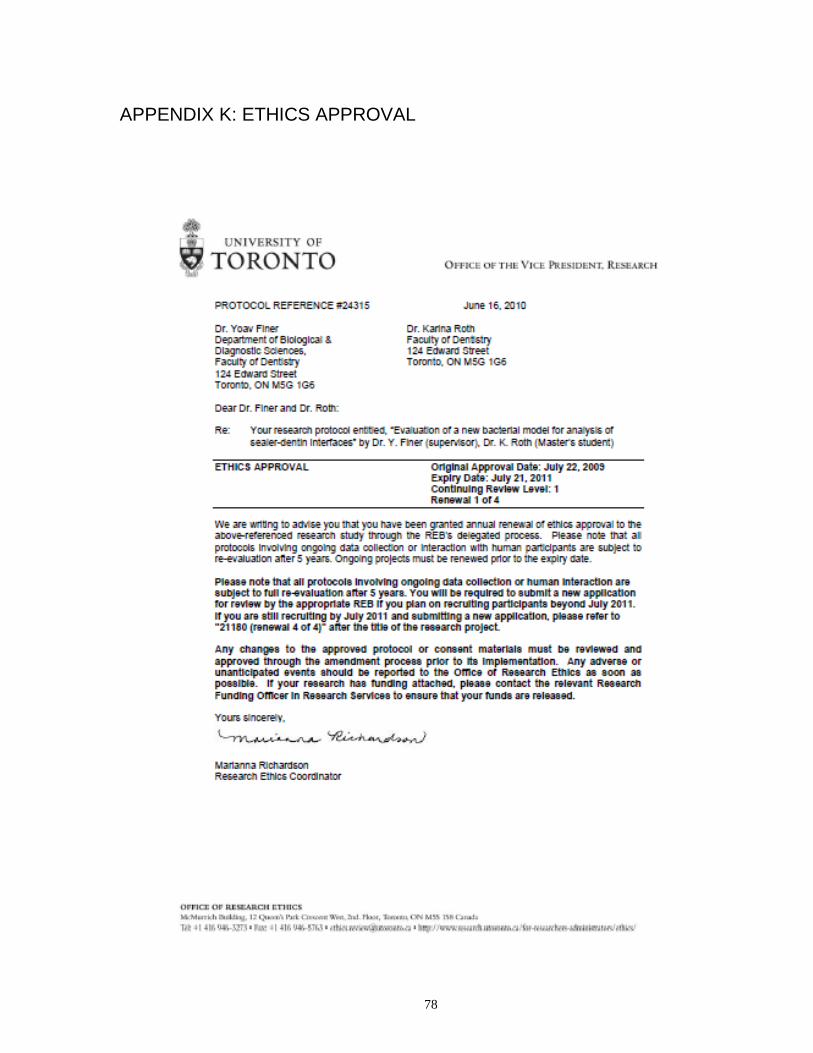
78
APPENDIX K: ETHICS APPROVAL
79
References
1. Nair PN. Apical periodontitis: a dynamic encounter between root canal infection
and host response. Periodontol 2000 1997;13:121-148.
2. Sjogren U, Figdor D, Persson S, Sundqvist G. Influence of infection at the time of
root filling on the outcome of endodontic treatment of teeth with apical periodontitis. Int
Endod J 1997;30(5):297-306.
3. Paquette L, Legner M, Fillery ED, Friedman S. Antibacterial efficacy of
chlorhexidine gluconate intracanal medication in vivo. J Endod 2007;33(7):788-795.
4. Peters LB, Wesselink PR. Periapical healing of endodontically treated teeth in one
and two visits obturated in the presence or absence of detectable microorganisms. Int
Endod J 2002;35(8):660-667.
5. Waltimo T, Trope M, Haapasalo M, Orstavik D. Clinical efficacy of treatment
procedures in endodontic infection control and one year follow-up of periapical healing. J
Endod 2005;31(12):863-866.
6. Gomes BP, Lilley JD, Drucker DB. Variations in the susceptibilities of components
of the endodontic microflora to biomechanical procedures. Int Endod J 1996;29(4):235-241.
7. Siqueira JF, Jr., Rocas IN. Clinical implications and microbiology of bacterial
persistence after treatment procedures. J Endod 2008;34(11):1291-1301 e1293.
8. Grossman L. Antimicrobial effect of root canal cements. J Endod 1980;6(6):594-597.
9. Carratu P, Amato M, Riccitiello F, Rengo S. Evaluation of leakage of bacteria and
endotoxins in teeth treated endodontically by two different techniques. J Endod
2002;28(4):272-275.
10. Shipper G, Orstavik D, Teixeira FB, Trope M. An evaluation of microbial leakage
in roots filled with a thermoplastic synthetic polymer-based root canal filling material
(Resilon). J Endod 2004;30(5):342-347.
11. Cobankara FK, Adanr N, Belli S. Evaluation of the influence of smear layer on the
apical and coronal sealing ability of two sealers. J Endod 2004;30(6):406-409.
12. Murray PE, Hafez AA, Smith AJ, Cox CF. Bacterial microleakage and pulp
inflammation associated with various restorative materials. Dent Mater 2002;18(6):470-
478.
13. Van Meerbeek B, Perdigao J, Lambrechts P, Vanherle G. The clinical performance
of adhesives. J Dent 1998;26(1):1-20.
14. Tay FR, Loushine RJ, Lambrechts P, Weller RN, Pashley DH. Geometric factors
affecting dentin bonding in root canals: a theoretical modeling approach. J Endod
2005;31(8):584-589.
80
15. Lai SC, Mak YF, Cheung GS, Osorio R, Toledano M, Carvalho RM, et al. Reversal
of compromised bonding to oxidized etched dentin. J Dent Res 2001;80(10):1919-1924.
16. Santos JN, Carrilho MR, De Goes MF, Zaia AA, Gomes BP, Souza-Filho FJ, et al.
Effect of chemical irrigants on the bond strength of a self-etching adhesive to pulp chamber
dentin. J Endod 2006;32(11):1088-1090.
17. Ricucci D, Siqueira JF, Jr. Biofilms and apical periodontitis: study of prevalence
and association with clinical and histopathologic findings. J Endod 2010;36(8):1277-1288.
18. Brackett MG, Martin R, Sword J, Oxford C, Rueggeberg FA, Tay FR, et al.
Comparison of seal after obturation techniques using a polydimethylsiloxane-based root
canal sealer. J Endod 2006;32(12):1188-1190.
19. Teixeira CS, Alfredo E, Thome LH, Gariba-Silva R, Silva-Sousa YT, Sousa-Neto
MD. Adhesion of an endodontic sealer to dentin and gutta-percha: shear and push-out
bond strength measurements and SEM analysis. J Appl Oral Sci 2009;17(2):129-135.
20. Schwartz RS, Fransman R. Adhesive dentistry and endodontics: materials, clinical
strategies and procedures for restoration of access cavities: a review. J Endod
2005;31(3):151-165.
21. Tay FR, Loushine RJ, Monticelli F, Weller RN, Breschi L, Ferrari M, et al.
Effectiveness of resin-coated gutta-percha cones and a dual-cured, hydrophilic
methacrylate resin-based sealer in obturating root canals. J Endod 2005;31(9):659-664.
22. Nakabayashi N, Kojima K, Masuhara E. The promotion of adhesion by the
infiltration of monomers into tooth substrates. J Biomed Mater Res 1982;16(3):265-273.
23. Van Meerbeek B, De Munck J, Yoshida Y, Inoue S, Vargas M, Vijay P, et al.
Buonocore memorial lecture. Adhesion to enamel and dentin: current status and future
challenges. Oper Dent 2003;28(3):215-235.
24. De Munck J, Van Landuyt K, Peumans M, Poitevin A, Lambrechts P, Braem M, et
al. A critical review of the durability of adhesion to tooth tissue: methods and results. J
Dent Res 2005;84(2):118-132.
25. Babb BR, Loushine RJ, Bryan TE, Ames JM, Causey MS, Kim J, et al. Bonding of
self-adhesive (self-etching) root canal sealers to radicular dentin. J Endod 2009;35(4):578-
582.
26. Monticelli F, Osorio R, Mazzitelli C, Ferrari M, Toledano M. Limited
decalcification/diffusion of self-adhesive cements into dentin. J Dent Res 2008;87(10):974-
979.
27. Kermanshahi S, Santerre JP, Cvitkovitch DG, Finer Y. Biodegradation of resin-
dentin interfaces increases bacterial microleakage. J Dent Res 2010;89(9):996-1001.
81
28. Pashley DH, Tay FR, Yiu C, Hashimoto M, Breschi L, Carvalho RM, et al. Collagen
degradation by host-derived enzymes during aging. J Dent Res 2004;83(3):216-221.
29. Shokati B, Tam LE, Santerre JP, Finer Y. Effect of salivary esterase on the integrity
and fracture toughness of the dentin-resin interface. J Biomed Mater Res B Appl Biomater
2010;94(1):230-237.
30. Hashimoto M, Ohno H, Endo K, Kaga M, Sano H, Oguchi H. The effect of hybrid
layer thickness on bond strength: demineralized dentin zone of the hybrid layer. Dent
Mater 2000;16(6):406-411.
31. Khalichi P, Cvitkovitch DG, Santerre JP. Effect of composite resin biodegradation
products on oral streptococcal growth. Biomaterials 2004;25(24):5467-5472.
32. Singh J, Khalichi P, Cvitkovitch DG, Santerre JP. Composite resin degradation
products from BisGMA monomer modulate the expression of genes associated with biofilm
formation and other virulence factors in Streptococcus mutans. J Biomed Mater Res A
2009;88(2):551-560.
33. Bergenholtz G. Micro-organisms from necrotic pulp of traumatized teeth. Odontol
Revy 1974;25(4):347-358.
34. Kakehashi S, Stanley HR, Fitzgerald RJ. The Effects of Surgical Exposures of
Dental Pulps in Germ-Free and Conventional Laboratory Rats. Oral Surg Oral Med Oral
Pathol 1965;20:340-349.
35. Sjogren U, Hagglund B, Sundqvist G, Wing K. Factors affecting the long-term
results of endodontic treatment. J Endod 1990;16(10):498-504.
36. Dalton BC, Orstavik D, Phillips C, Pettiette M, Trope M. Bacterial reduction with
nickel-titanium rotary instrumentation. J Endod 1998;24(11):763-767.
37. Shuping GB, Orstavik D, Sigurdsson A, Trope M. Reduction of intracanal bacteria
using nickel-titanium rotary instrumentation and various medications. J Endod
2000;26(12):751-755.
38. Siqueira JF, Jr., Lima KC, Magalhaes FA, Lopes HP, de Uzeda M. Mechanical
reduction of the bacterial population in the root canal by three instrumentation techniques.
J Endod 1999;25(5):332-335.
39. Bystrom A, Sundqvist G. Bacteriologic evaluation of the efficacy of mechanical root
canal instrumentation in endodontic therapy. Scand J Dent Res 1981;89(4):321-328.
40. Friedman S, Torneck CD, Komorowski R, Ouzounian Z, Syrtash P, Kaufman A. In
vivo model for assessing the functional efficacy of endodontic filling materials and
techniques. J Endod 1997;23(9):557-561.
41. Schilder H. Filling root canals in three dimensions. 1967. J Endod 2006;32(4):281-
290.
82
42. Mjor IA, Nordahl I. The density and branching of dentinal tubules in human teeth.
Arch Oral Biol 1996;41(5):401-412.
43. Garberoglio R, Brannstrom M. Scanning electron microscopic investigation of
human dentinal tubules. Arch Oral Biol 1976;21(6):355-362.
44. Carrigan PJ, Morse DR, Furst ML, Sinai IH. A scanning electron microscopic
evaluation of human dentinal tubules according to age and location. J Endod
1984;10(8):359-363.
45. Tronstad L. Ultrastructural observations on human coronal dentin. Scand J Dent
Res 1973;81(2):101-111.
46. Love RM, Jenkinson HF. Invasion of dentinal tubules by oral bacteria. Crit Rev
Oral Biol Med 2002;13(2):171-183.
47. Sen BH, Wesselink PR, Turkun M. The smear layer: a phenomenon in root canal
therapy. Int Endod J 1995;28(3):141-148.
48. Siqueira JF, Jr., De Uzeda M, Fonseca ME. A scanning electron microscopic
evaluation of in vitro dentinal tubules penetration by selected anaerobic bacteria. J Endod
1996;22(6):308-310.
49. Ando N, Hoshino E. Predominant obligate anaerobes invading the deep layers of
root canal dentin. Int Endod J 1990;23(1):20-27.
50. Horiba N, Maekawa Y, Matsumoto T, Nakamura H. A study of the distribution of
endotoxin in the dentinal wall of infected root canals. J Endod 1990;16(7):331-334.
51. Sen BH, Piskin B, Demirci T. Observation of bacteria and fungi in infected root
canals and dentinal tubules by SEM. Endod Dent Traumatol 1995;11(1):6-9.
52. Peters LB, Wesselink PR, Buijs JF, van Winkelhoff AJ. Viable bacteria in root
dentinal tubules of teeth with apical periodontitis. J Endod 2001;27(2):76-81.
53. Akpata ES, Blechman H. Bacterial invasion of pulpal dentin wall in vitro. J Dent
Res 1982;61(2):435-438.
54. Kakoli P, Nandakumar R, Romberg E, Arola D, Fouad AF. The effect of age on
bacterial penetration of radicular dentin. J Endod 2009;35(1):78-81.
55. Nair PN. On the causes of persistent apical periodontitis: a review. Int Endod J
2006;39(4):249-281.
56. Siqueira JF, Jr. Aetiology of root canal treatment failure: why well-treated teeth can
fail. Int Endod J 2001;34(1):1-10.
57. Fouad AF. Endodontic microbiology. 1st edition. ed: Wiley-Blackwell.; 2009.
83
58. Imura N, Pinheiro ET, Gomes BP, Zaia AA, Ferraz CC, Souza-Filho FJ. The
outcome of endodontic treatment: a retrospective study of 2000 cases performed by a
specialist. J Endod 2007;33(11):1278-1282.
59. Gomes BP, Pinheiro ET, Gade-Neto CR, Sousa EL, Ferraz CC, Zaia AA, et al.
Microbiological examination of infected dental root canals. Oral Microbiol Immunol
2004;19(2):71-76.
60. Schirrmeister JF, Liebenow AL, Pelz K, Wittmer A, Serr A, Hellwig E, et al. New
bacterial compositions in root-filled teeth with periradicular lesions. J Endod
2009;35(2):169-174.
61. Chavez De Paz LE, Dahlen G, Molander A, Moller A, Bergenholtz G. Bacteria
recovered from teeth with apical periodontitis after antimicrobial endodontic treatment.
Int Endod J 2003;36(7):500-508.
62. Molander A, Reit C, Dahlen G, Kvist T. Microbiological status of root-filled teeth
with apical periodontitis. Int Endod J 1998;31(1):1-7.
63. Zehnder M, Guggenheim B. The mysterious appearance of enterococci in filled root
canals. Int Endod J 2009;42(4):277-287.
64. Baumgartner G, Zehnder M, Paque F. Enterococcus faecalis type strain leakage
through root canals filled with Gutta-Percha/AH plus or Resilon/Epiphany. J Endod
2007;33(1):45-47.
65. Kaufman B, Spangberg L, Barry J, Fouad AF. Enterococcus spp. in endodontically
treated teeth with and without periradicular lesions. J Endod 2005;31(12):851-856.
66. Chivatxaranukul P, Dashper SG, Messer HH. Dentinal tubule invasion and
adherence by Enterococcus faecalis. Int Endod J 2008;41(10):873-882.
67. Sedgley CM, Lennan SL, Appelbe OK. Survival of Enterococcus faecalis in root
canals ex vivo. Int Endod J 2005;38(10):735-742.
68. Rocas IN, Siqueira JF, Jr., Santos KR. Association of Enterococcus faecalis with
different forms of periradicular diseases. J Endod 2004;30(5):315-320.
69. George S, Kishen A, Song KP. The role of environmental changes on monospecies
biofilm formation on root canal wall by Enterococcus faecalis. J Endod 2005;31(12):867-
872.
70. Costerton JW, Stewart PS, Greenberg EP. Bacterial biofilms: a common cause of
persistent infections. Science 1999;284(5418):1318-1322.
71. Nair PN, Henry S, Cano V, Vera J. Microbial status of apical root canal system of
human mandibular first molars with primary apical periodontitis after "one-visit"
endodontic treatment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2005;99(2):231-252.
84
72. Ricucci D, Martorano M, Bate AL, Pascon EA. Calculus-like deposit on the apical
external root surface of teeth with post-treatment apical periodontitis: report of two cases.
Int Endod J 2005;38(4):262-271.
73. Harn WM, Chen YH, Yuan K, Chung CH, Huang PH. Calculus-like deposit at apex
of tooth with refractory apical periodontitis. Endod Dent Traumatol 1998;14(5):237-240.
74. Takemura N, Noiri Y, Ehara A, Kawahara T, Noguchi N, Ebisu S. Single species
biofilm-forming ability of root canal isolates on gutta-percha points. Eur J Oral Sci
2004;112(6):523-529.
75. Costerton JW, Cheng KJ, Geesey GG, Ladd TI, Nickel JC, Dasgupta M, et al.
Bacterial biofilms in nature and disease. Annu Rev Microbiol 1987;41:435-464.
76. Costerton JW, Lewandowski Z, DeBeer D, Caldwell D, Korber D, James G.
Biofilms, the customized microniche. J Bacteriol 1994;176(8):2137-2142.
77. Gilbert P, Das J, Foley I. Biofilm susceptibility to antimicrobials. Adv Dent Res
1997;11(1):160-167.
78. Mader CL, Baumgartner JC, Peters DD. Scanning electron microscopic
investigation of the smeared layer on root canal walls. J Endod 1984;10(10):477-483.
79. McComb D, Smith DC. A preliminary scanning electron microscopic study of root
canals after endodontic procedures. J Endod 1975;1(7):238-242.
80. Pashley DH, Michelich V, Kehl T. Dentin permeability: effects of smear layer
removal. J Prosthet Dent 1981;46(5):531-537.
81. Hovland EJ, Dumsha TC. Leakage evaluation in vitro of the root canal sealer
cement Sealapex. Int Endod J 1985;18(3):179-182.
82. Saunders WP, Saunders EM. Coronal leakage as a cause of failure in root-canal
therapy: a review. Endod Dent Traumatol 1994;10(3):105-108.
83. Wu MK, Wesselink PR. Endodontic leakage studies reconsidered. Part I.
Methodology, application and relevance. Int Endod J 1993;26(1):37-43.
84. Lee KW, Williams MC, Camps JJ, Pashley DH. Adhesion of endodontic sealers to
dentin and gutta-percha. J Endod 2002;28(10):684-688.
85. McComb D, Smith DC. Comparison of physical properties of polycarboxylate-based
and conventional root canal sealers. J Endod 1976;2(8):228-235.
86. Wennberg A, Orstavik D. Adhesion of root canal sealers to bovine dentine and
gutta-percha. Int Endod J 1990;23(1):13-19.
87. Saleh IM, Ruyter IE, Haapasalo M, Orstavik D. Bacterial penetration along
different root canal filling materials in the presence or absence of smear layer. Int Endod J
2008;41(1):32-40.
85
88. Gettleman BH, Messer HH, ElDeeb ME. Adhesion of sealer cements to dentin with
and without the smear layer. J Endod 1991;17(1):15-20.
89. Eldeniz AU, Erdemir A, Belli S. Shear bond strength of three resin based sealers to
dentin with and without the smear layer. J Endod 2005;31(4):293-296.
90. Zmener O, Pameijer CH, Serrano SA, Vidueira M, Macchi RL. Significance of
moist root canal dentin with the use of methacrylate-based endodontic sealers: an in vitro
coronal dye leakage study. J Endod 2008;34(1):76-79.
91. Kim YK, Grandini S, Ames JM, Gu LS, Kim SK, Pashley DH, et al. Critical review
on methacrylate resin-based root canal sealers. J Endod 2010;36(3):383-399.
92. Spencer P, Ye Q, Park J, Topp EM, Misra A, Marangos O, et al. Adhesive/Dentin
interface: the weak link in the composite restoration. Ann Biomed Eng 2010;38(6):1989-
2003.
93. Kim YK, Mai S, Haycock JR, Kim SK, Loushine RJ, Pashley DH, et al. The self-
etching potential of RealSeal versus RealSeal SE. J Endod 2009;35(9):1264-1269.
94. Ari H, Yasar E, Belli S. Effects of NaOCl on bond strengths of resin cements to root
canal dentin. J Endod 2003;29(4):248-251.
95. Perdigao J, Lopes M, Geraldeli S, Lopes GC, Garcia-Godoy F. Effect of a sodium
hypochlorite gel on dentin bonding. Dent Mater 2000;16(5):311-323.
96. Morris MD, Lee KW, Agee KA, Bouillaguet S, Pashley DH. Effects of sodium
hypochlorite and RC-prep on bond strengths of resin cement to endodontic surfaces. J
Endod 2001;27(12):753-757.
97. Yiu CK, Garcia-Godoy F, Tay FR, Pashley DH, Imazato S, King NM, et al. A
nanoleakage perspective on bonding to oxidized dentin. J Dent Res 2002;81(9):628-632.
98. Wang Y, Spencer P. Continuing etching of an all-in-one adhesive in wet dentin
tubules. J Dent Res 2005;84(4):350-354.
99. Hebling J, Pashley DH, Tjaderhane L, Tay FR. Chlorhexidine arrests subclinical
degradation of dentin hybrid layers in vivo. J Dent Res 2005;84(8):741-746.
100. Breschi L, Mazzoni A, Ruggeri A, Cadenaro M, Di Lenarda R, De Stefano Dorigo E.
Dental adhesion review: aging and stability of the bonded interface. Dent Mater
2008;24(1):90-101.
101. Ito S, Hashimoto M, Wadgaonkar B, Svizero N, Carvalho RM, Yiu C, et al. Effects
of resin hydrophilicity on water sorption and changes in modulus of elasticity. Biomaterials
2005;26(33):6449-6459.
102. Ferracane JL. Elution of leachable components from composites. J Oral Rehabil
1994;21(4):441-452.
86
103. Finer Y, Santerre JP. Influence of silanated filler content on the biodegradation of
bisGMA/TEGDMA dental composite resins. J Biomed Mater Res A 2007;81(1):75-84.
104. Ortengren U, Wellendorf H, Karlsson S, Ruyter IE. Water sorption and solubility of
dental composites and identification of monomers released in an aqueous environment. J
Oral Rehabil 2001;28(12):1106-1115.
105. Ames JM, Loushine RJ, Babb BR, Bryan TE, Lockwood PE, Sui M, et al.
Contemporary methacrylate resin-based root canal sealers exhibit different degrees of ex
vivo cytotoxicity when cured in their self-cured mode. J Endod 2009;35(2):225-228.
106. Buonocore MG. A simple method of increasing the adhesion of acrylic filling
materials to enamel surfaces. J Dent Res 1955;34(6):849-853.
107. Bouillaguet S, Gysi P, Wataha JC, Ciucchi B, Cattani M, Godin C, et al. Bond
strength of composite to dentin using conventional, one-step, and self-etching adhesive
systems. J Dent 2001;29(1):55-61.
108. Ceballos L, Camejo DG, Victoria Fuentes M, Osorio R, Toledano M, Carvalho RM,
et al. Microtensile bond strength of total-etch and self-etching adhesives to caries-affected
dentine. J Dent 2003;31(7):469-477.
109. Paul SJ, Welter DA, Ghazi M, Pashley D. Nanoleakage at the dentin adhesive
interface vs microtensile bond strength. Oper Dent 1999;24(3):181-188.
110. Sano H. Microtensile testing, nanoleakage, and biodegradation of resin-dentin
bonds. J Dent Res 2006;85(1):11-14.
111. Tay FR, Pashley DH. Have dentin adhesives become too hydrophilic? J Can Dent
Assoc 2003;69(11):726-731.
112. Wilcox LR, Diaz-Arnold A. Coronal microleakage of permanent lingual access
restorations in endodontically treated anterior teeth. J Endod 1989;15(12):584-587.
113. Khayat A, Lee SJ, Torabinejad M. Human saliva penetration of coronally unsealed
obturated root canals. J Endod 1993;19(9):458-461.
114. Madison S, Swanson K, Chiles SA. An evaluation of coronal microleakage in
endodontically treated teeth. Part II. Sealer types. J Endod 1987;13(3):109-112.
115. Swanson K, Madison S. An evaluation of coronal microleakage in endodontically
treated teeth. Part I. Time periods. J Endod 1987;13(2):56-59.
116. Stratton RK, Apicella MJ, Mines P. A fluid filtration comparison of gutta-percha
versus Resilon, a new soft resin endodontic obturation system. J Endod 2006;32(7):642-645.
117. Wu MK, Wesselink PR, Boersma J. A 1-year follow-up study on leakage of four
root canal sealers at different thicknesses. Int Endod J 1995;28(4):185-189.
87
118. Alves J, Walton R, Drake D. Coronal leakage: endotoxin penetration from mixed
bacterial communities through obturated, post-prepared root canals. J Endod
1998;24(9):587-591.
119. Trope M, Chow E, Nissan R. In vitro endotoxin penetration of coronally unsealed
endodontically treated teeth. Endod Dent Traumatol 1995;11(2):90-94.
120. Xu Q, Fan MW, Fan B, Cheung GS, Hu HL. A new quantitative method using
glucose for analysis of endodontic leakage. Oral Surg Oral Med Oral Pathol Oral Radiol
Endod 2005;99(1):107-111.
121. Rahimi M, Jainaen A, Parashos P, Messer HH. Bonding of resin-based sealers to
root dentin. J Endod 2009;35(1):121-124.
122. Leonardo MR, Barnett F, Debelian GJ, de Pontes Lima RK, Bezerra da Silva LA.
Root canal adhesive filling in dogs' teeth with or without coronal restoration: a
histopathological evaluation. J Endod 2007;33(11):1299-1303.
123. Shipper G, Teixeira FB, Arnold RR, Trope M. Periapical inflammation after
coronal microbial inoculation of dog roots filled with gutta-percha or resilon. J Endod
2005;31(2):91-96.
124. Pitt Ford TR. Relation between seal of root fillings and tissue response. Oral Surg
Oral Med Oral Pathol 1983;55(3):291-294.
125. Oliver CM, Abbott PV. Correlation between clinical success and apical dye
penetration. Int Endod J 2001;34(8):637-644.
126. Grondahl H, Huumonen S. Radiographic manifestations of periapical inflammatory
lesions. Endodontic Topics 2004;8:55-67.
127. Hirsch E, Wolf U, Heinicke F, Silva MA. Dosimetry of the cone beam computed
tomography Veraviewepocs 3D compared with the 3D Accuitomo in different fields of
view. Dentomaxillofac Radiol 2008;37(5):268-273.
128. White JM, Goodis HE, Marshall SJ, Marshall GW. Sterilization of teeth by gamma
radiation. J Dent Res 1994;73(9):1560-1567.
129. Gogos C, Theodorou V, Economides N, Beltes P, Kolokouris I. Shear bond strength
of AH-26 and Epiphany to composite resin and Resilon. J Endod 2008;34(11):1385-1387.
130. Torabinejad M, Ung B, Kettering JD. In vitro bacterial penetration of coronally
unsealed endodontically treated teeth. J Endod 1990;16(12):566-569.
131. Zapata RO, Bramante CM, de Moraes IG, Bernardineli N, Gasparoto TH, Graeff
MS, et al. Confocal laser scanning microscopy is appropriate to detect viability of
Enterococcus faecalis in infected dentin. J Endod 2008;34(10):1198-1201.
88
132. Mohamed JA, Huang W, Nallapareddy SR, Teng F, Murray BE. Influence of origin
of isolates, especially endocarditis isolates, and various genes on biofilm formation by
Enterococcus faecalis. Infect Immun 2004;72(6):3658-3663.
133. Sundqvist G, Figdor D, Persson S, Sjogren U. Microbiologic analysis of teeth with
failed endodontic treatment and the outcome of conservative re-treatment. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod 1998;85(1):86-93.
134. Teixeira FB, Teixeira EC, Thompson J, Leinfelder KF, Trope M. Dentinal bonding
reaches the root canal system. J Esthet Restor Dent 2004;16(6):348-354; discussion 354.
135. Estrela C, Sydney GB, Figueiredo JA, Estrela CR. A model system to study
antimicrobial strategies in endodontic biofilms. J Appl Oral Sci 2009;17(2):87-91.
136. Khalichi P, Singh J, Cvitkovitch DG, Santerre JP. The influence of triethylene
glycol derived from dental composite resins on the regulation of Streptococcus mutans gene
expression. Biomaterials 2009;30(4):452-459.
137. Hirai VH, da Silva Neto UX, Westphalen VP, Perin CP, Carneiro E, Fariniuk LF.
Comparative analysis of leakage in root canal fillings performed with gutta-percha and
Resilon cones with AH Plus and Epiphany sealers. Oral Surg Oral Med Oral Pathol Oral
Radiol Endod 2010;109(2):e131-135.
138. Nawal RR, Parande M, Sehgal R, Rao NR, Naik A. A comparative evaluation of 3
root canal filling systems. Oral Surg Oral Med Oral Pathol Oral Radiol Endod
2011;111(3):387-393.
139. Hashimoto M. A review--micromorphological evidence of degradation in resin-
dentin bonds and potential preventional solutions. J Biomed Mater Res B Appl Biomater
2010;92(1):268-280.
140. Ferrari M, Mannocci F, Vichi A, Cagidiaco MC, Mjor IA. Bonding to root canal:
structural characteristics of the substrate. Am J Dent 2000;13(5):255-260.
141. Reid BD. Gamma processing technology: an alternative technology for terminal
sterilization of parenterals. PDA J Pharm Sci Technol 1995;49(2):83-89.
142. Sperandio M, Souza JB, Oliveira DT. Effect of gamma radiation on dentin bond
strength and morphology. Braz Dent J 2001;12(3):205-208.
143. DeWald JP. The use of extracted teeth for in vitro bonding studies: a review of
infection control considerations. Dent Mater 1997;13(2):74-81.
144. Brauer DS, Saeki K, Hilton JF, Marshall GW, Marshall SJ. Effect of sterilization by
gamma radiation on nano-mechanical properties of teeth. Dent Mater 2008;24(8):1137-
1140.
89
145. Rodrigues LK, Cury JA, Nobre dos Santos M. The effect of gamma radiation on
enamel hardness and its resistance to demineralization in vitro. J Oral Sci 2004;46(4):215-
220.
146. Guyton A, Hall J. Secretary functions of the alimentary tract. Philadelphia:
Saunders; 1992.
147. Lamb J, Ingram C, Johnston I, Pitman R. Essentials of Physiology. Oxford:
Blackwell Scientific Publications; 1991.
148. Pratten J, Andrews CS, Craig DQ, Wilson M. Structural studies of microcosm
dental plaques grown under different nutritional conditions. FEMS Microbiol Lett
2000;189(2):215-218.
Recommended

















