Dysfunctional Uterine BleedingDysfunctional Uterine Bleeding
Prof.DR.Dr.H.M.Thamrin Tanjung, Sp.OG(K)j g p ( )Dr.Muhammad Rusda, Sp.OG
Dept. of Obstetric & GynecologySchool of Medicine University of Sumatera Utara
Dysfunctional Uterine Bleedingy g
MOST COMMON MENSTRUAL DISORDER
CAN AFFECT ANY WOMEN FROM MENARCHEE TO MENOPAUSEMENARCHEE TO MENOPAUSE
OFTEN THE FIRST CLINICAL DIAGNOSIS FOR ANY EXCESSIVE MENSTRUAL BLEEDINGANY EXCESSIVE MENSTRUAL BLEEDING
DIAGNOSIS HAS TO BE CONFIRMED BY A PROCESS OF EXCLUSION OF PATHOLOGICAL CAUSES
Dysfunctional Uterine Bleedingy g
EXACT PATHOPHYSIOLOGY STILL NOT KNOWN
BASIS OF EXCESSIVE BLEEDING ISBASIS OF EXCESSIVE BLEEDING IS MOSTLY AN ENDOCRINE ABNORMALITY: -OESTROGEN PROGESTERONE IMBALANCEOESTROGEN - PROGESTERONE IMBALANCE (mostly estrogen dominance)
ALTERED PROSTAGLANDIN SYNTHESISALTERED PROSTAGLANDIN SYNTHESIS INFAVOUR OF E2 THAN E2α
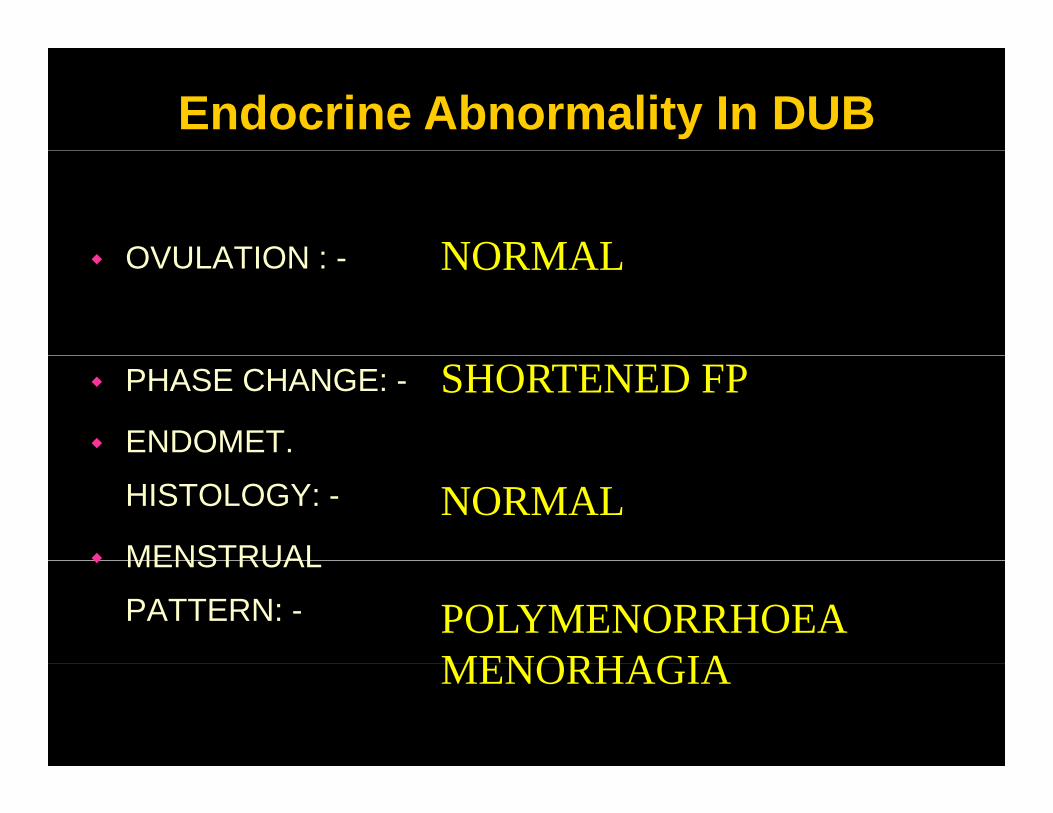
Endocrine Abnormality In DUB
NORMALOVULATION : NORMAL OVULATION : -
SHORTENED FPPHASE CHANGE: -
ENDOMET.
NORMALHISTOLOGY: -
MENSTRUAL
POLYMENORRHOEA MENORHAGIA
MENSTRUAL
PATTERN: -
MENORHAGIA
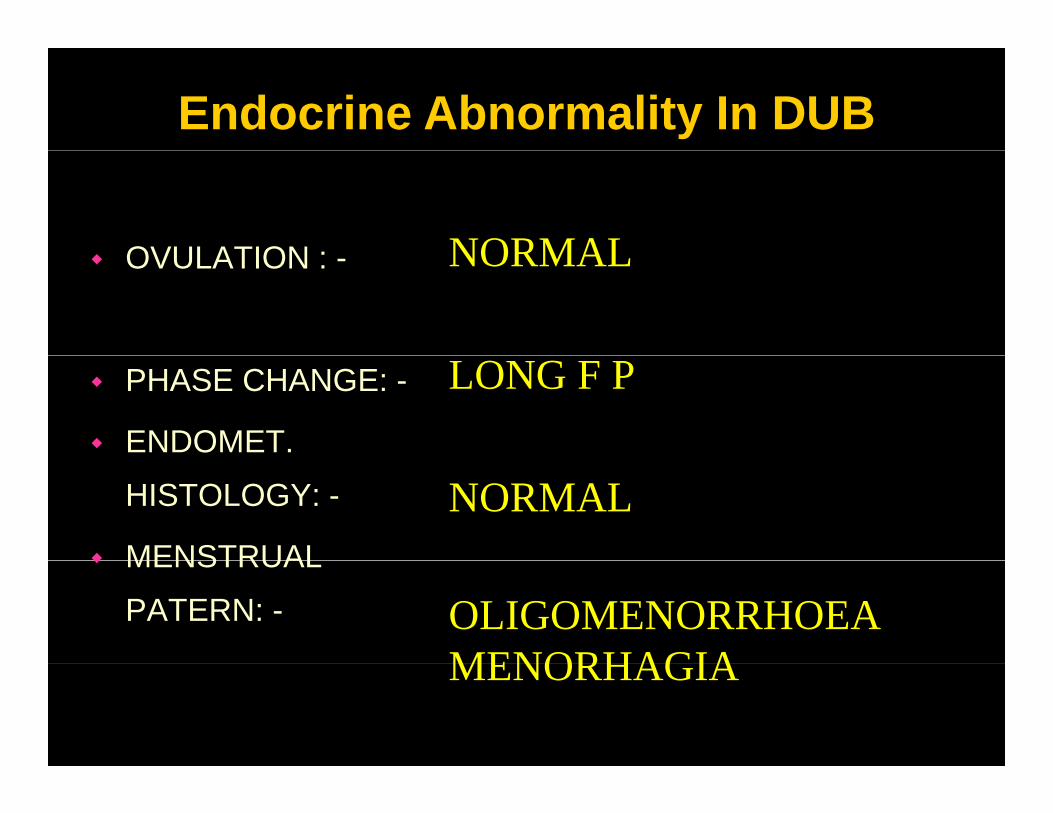
Endocrine Abnormality In DUB
NORMALOVULATION : NORMAL OVULATION : -
LONG F PPHASE CHANGE: -
ENDOMET.
NORMALHISTOLOGY: -
MENSTRUAL
OLIGOMENORRHOEA MENORHAGIA
MENSTRUAL
PATERN: -
MENORHAGIA
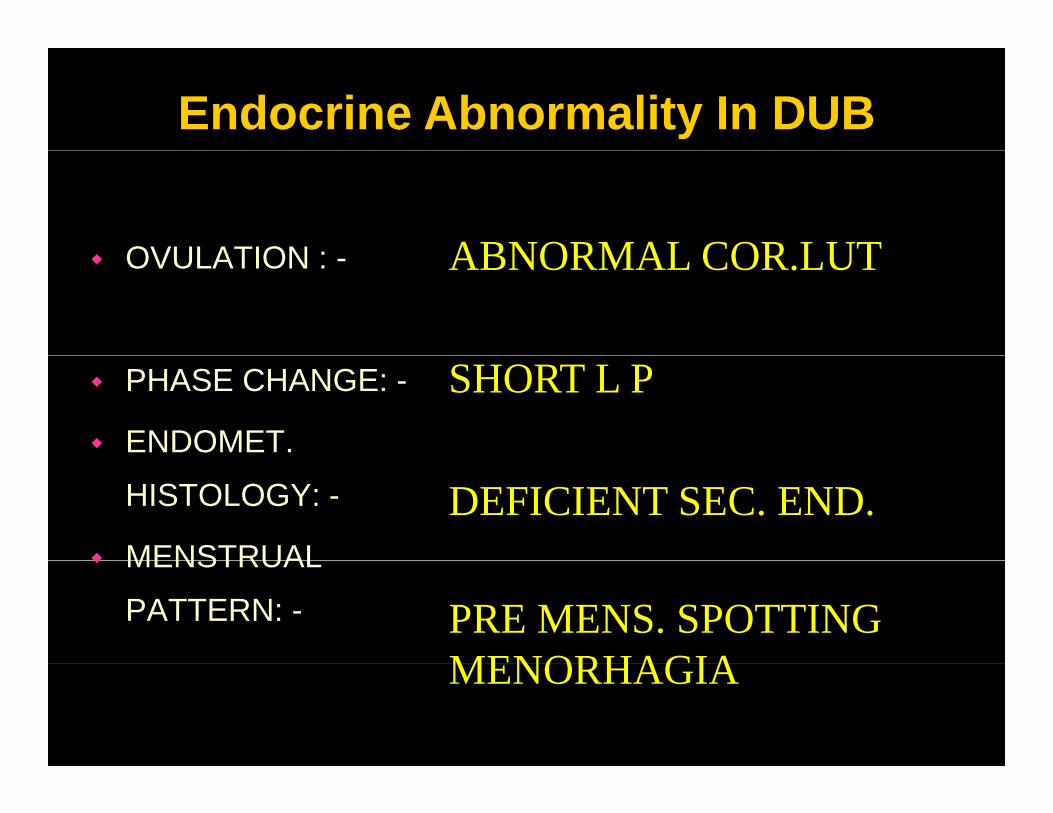
Endocrine Abnormality In DUB
ABNORMAL COR LUTOVULATION : ABNORMAL COR.LUTOVULATION : -
SHORT L PPHASE CHANGE: -
ENDOMET.
DEFICIENT SEC. END.HISTOLOGY: -
MENSTRUAL
PRE MENS. SPOTTING MENORHAGIA
MENSTRUAL
PATTERN: -
MENORHAGIA
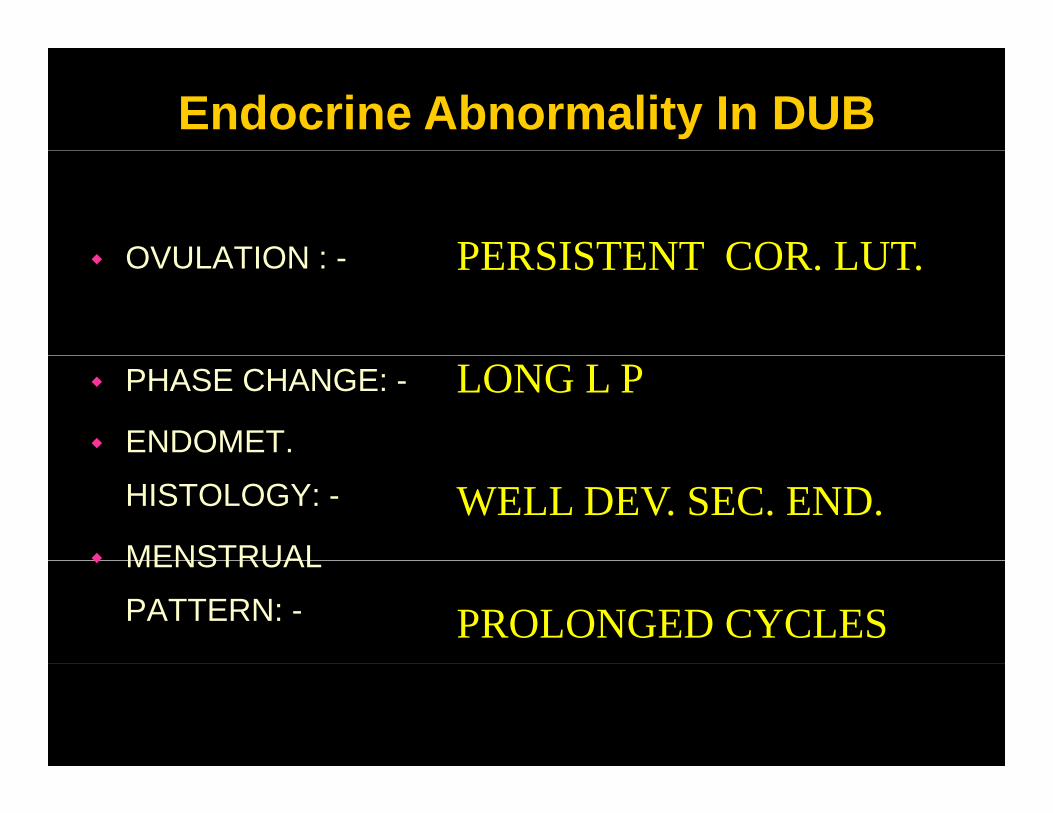
Endocrine Abnormality In DUB
PERSISTENT COR LUTOVULATION : PERSISTENT COR. LUT.OVULATION : -
LONG L PPHASE CHANGE: -
ENDOMET.
WELL DEV. SEC. END.HISTOLOGY: -
MENSTRUAL
PROLONGED CYCLES
MENSTRUAL
PATTERN: -
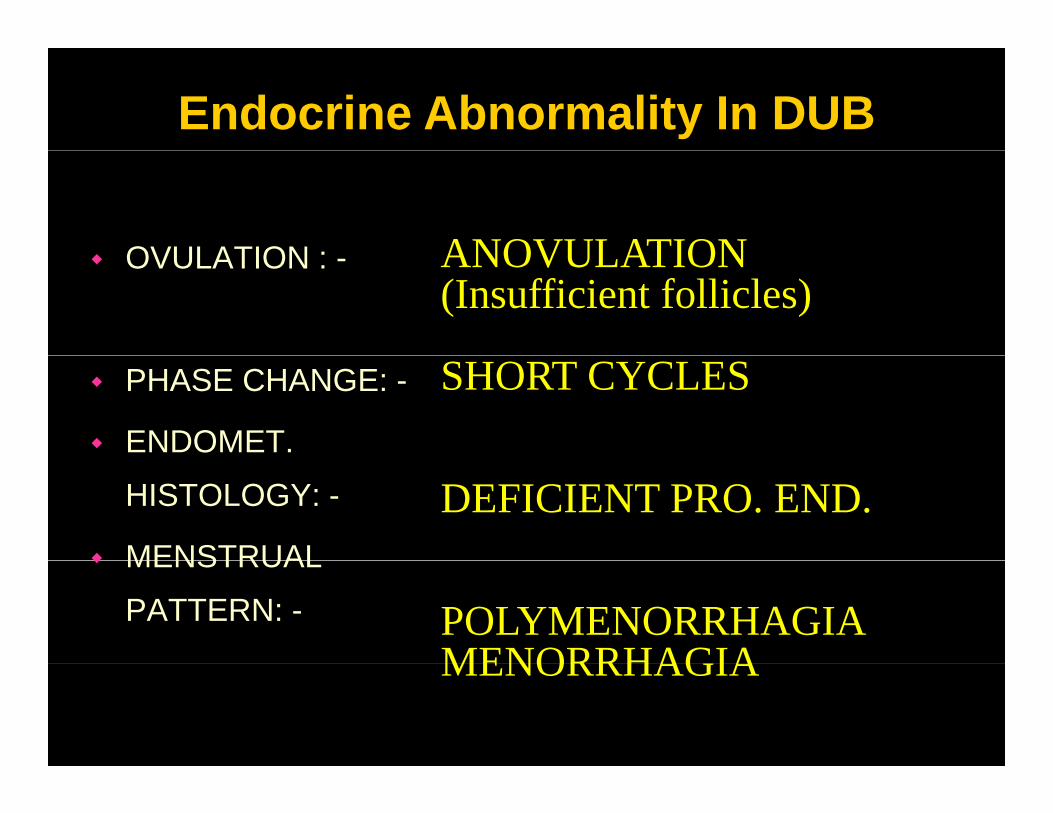
Endocrine Abnormality In DUB
ANOVULATIONOVULATION : ANOVULATION(Insufficient follicles)
OVULATION : -
SHORT CYCLESPHASE CHANGE: -
ENDOMET.
DEFICIENT PRO. END.HISTOLOGY: -
MENSTRUAL
POLYMENORRHAGIA MENORRHAGIA
MENSTRUAL
PATTERN: -
MENORRHAGIA
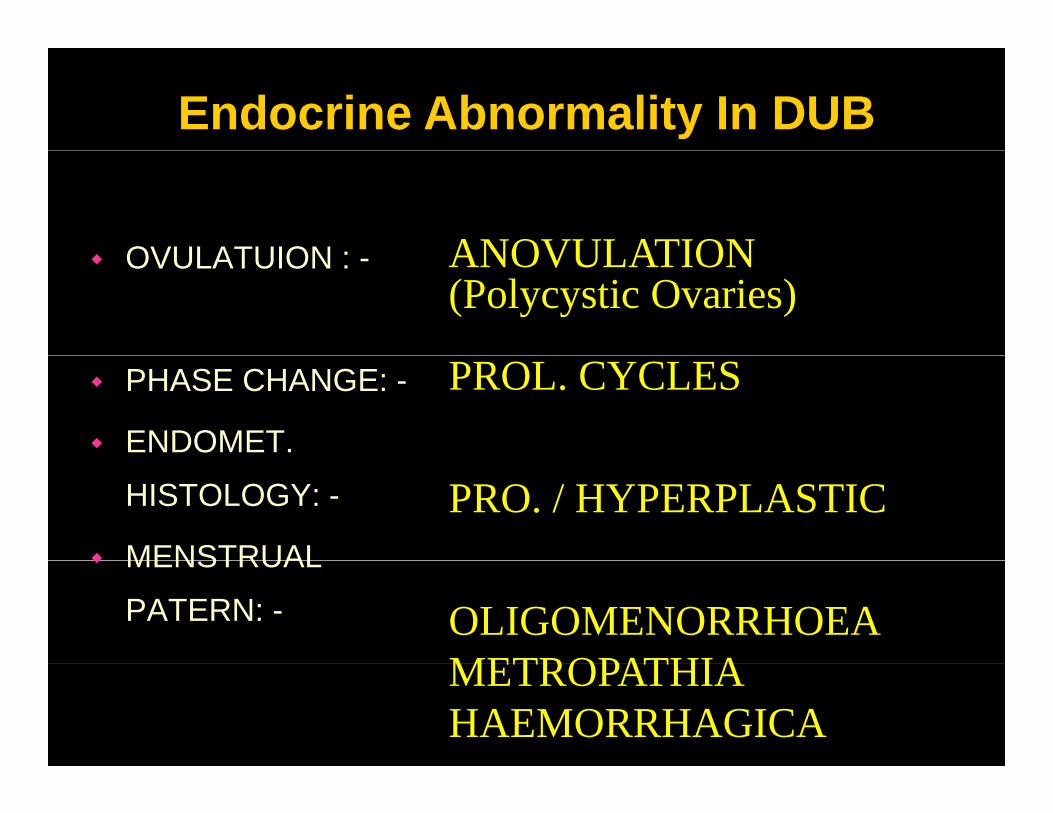
Endocrine Abnormality In DUB
OVULATUION : ANOVULATIONOVULATUION : - ANOVULATION(Polycystic Ovaries)
PHASE CHANGE: -
ENDOMET.
PROL. CYCLES
HISTOLOGY: -
MENSTRUAL
PRO. / HYPERPLASTICMENSTRUAL
PATERN: - OLIGOMENORRHOEAMETROPATHIAMETROPATHIA HAEMORRHAGICA
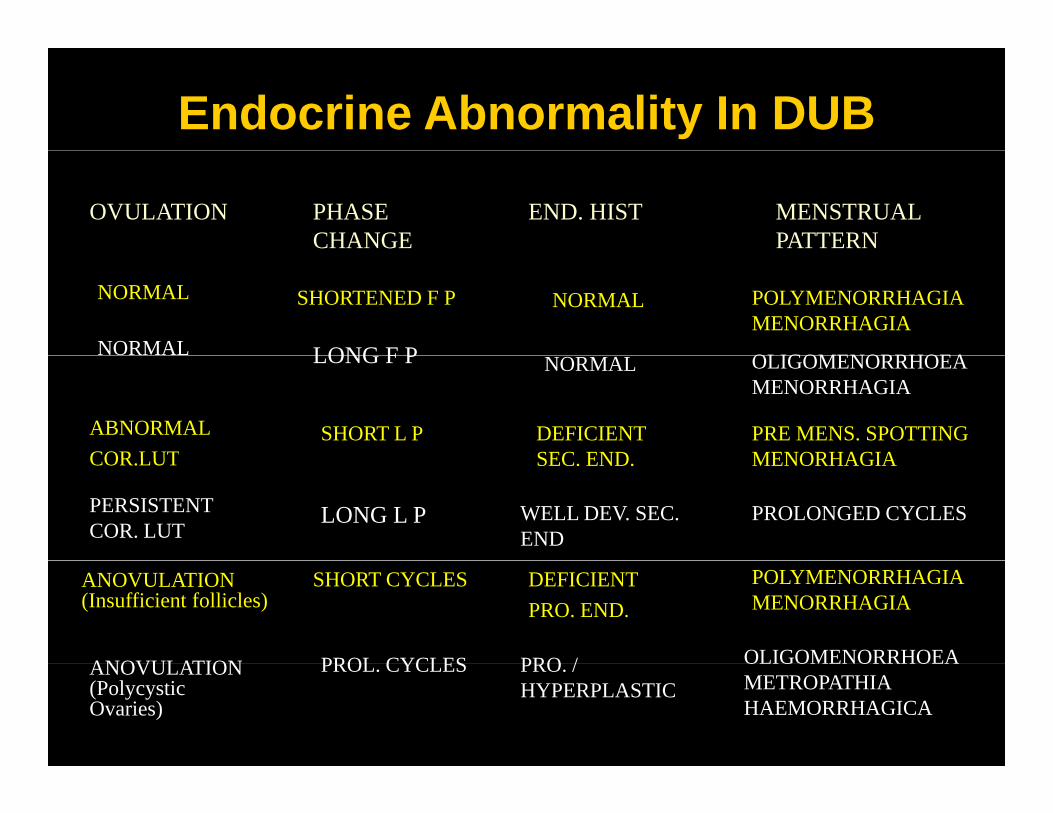
Endocrine Abnormality In DUB
OVULATION PHASE CHANGE
END. HIST MENSTRUAL PATTERN
NORMALNORMAL
NORMAL
SHORTENED F P
LONG F P
POLYMENORRHAGIAMENORRHAGIA
OLIGOMENORRHOEA
ABNORMAL COR LUT
SHORT L P DEFICIENT SEC END
PRE MENS. SPOTTING MENORHAGIA
NORMALLONG F P OLIGOMENORRHOEA MENORRHAGIA
PERSISTENT COR. LUT
LONG L P WELL DEV. SEC. END
PROLONGED CYCLES
COR.LUT SEC. END. MENORHAGIA
ANOVULATION PROL CYCLES PRO / OLIGOMENORRHOEA
ANOVULATION(Insufficient follicles)
DEFICIENT PRO. END.
SHORT CYCLES POLYMENORRHAGIAMENORRHAGIA
ANOVULATION(Polycystic Ovaries)
PROL. CYCLES PRO. / HYPERPLASTIC
OLIGOMENORRHOEAMETROPATHIA HAEMORRHAGICA
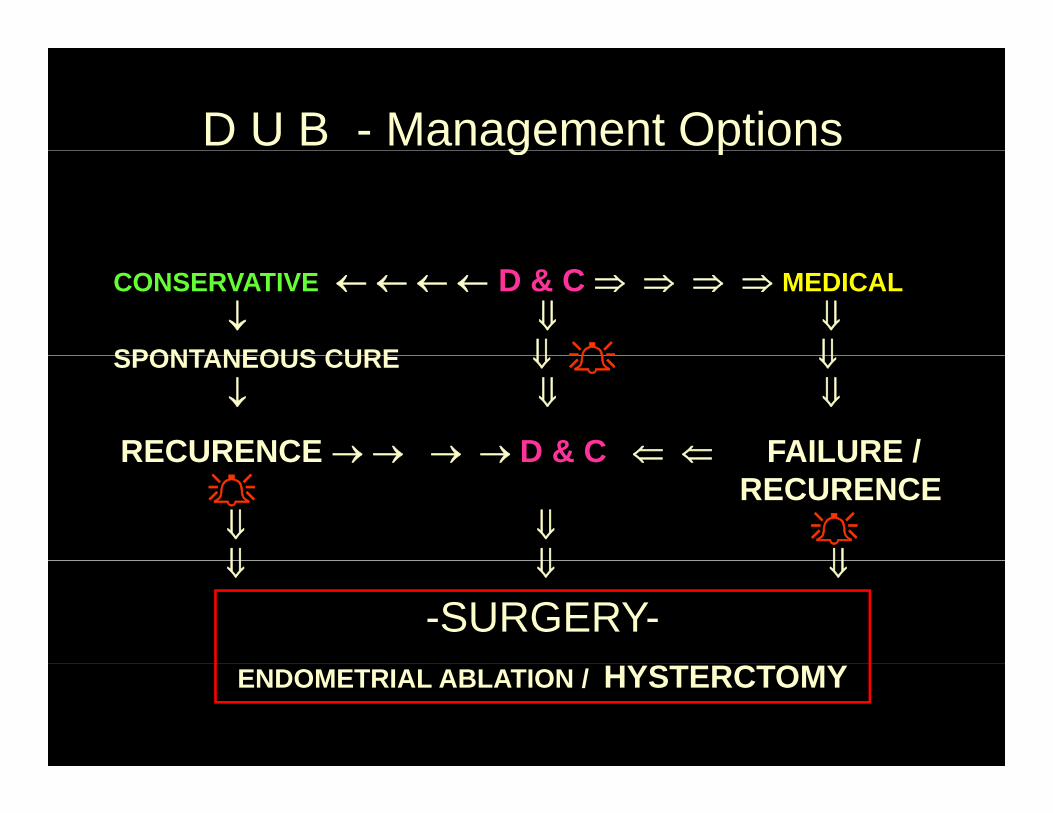
D U B - Management Optionsg p
CONSERVATIVE ← ← ← ← D & C ⇒ ⇒ ⇒ ⇒ MEDICAL↓ ⇓ ⇓
SPONTANEOUS CURE ⇓ ⇓SPONTANEOUS CURE ⇓ ⇓↓ ⇓ ⇓
RECURENCE → → → → D & C ⇐ ⇐ FAILURE /RECURENCE → → → → D & C ⇐ ⇐ FAILURE /RECURENCE
⇓ ⇓⇓ ⇓ ⇓⇓ ⇓ ⇓
-SURGERY-ENDOMETRIAL ABLATION / HYSTERCTOMY
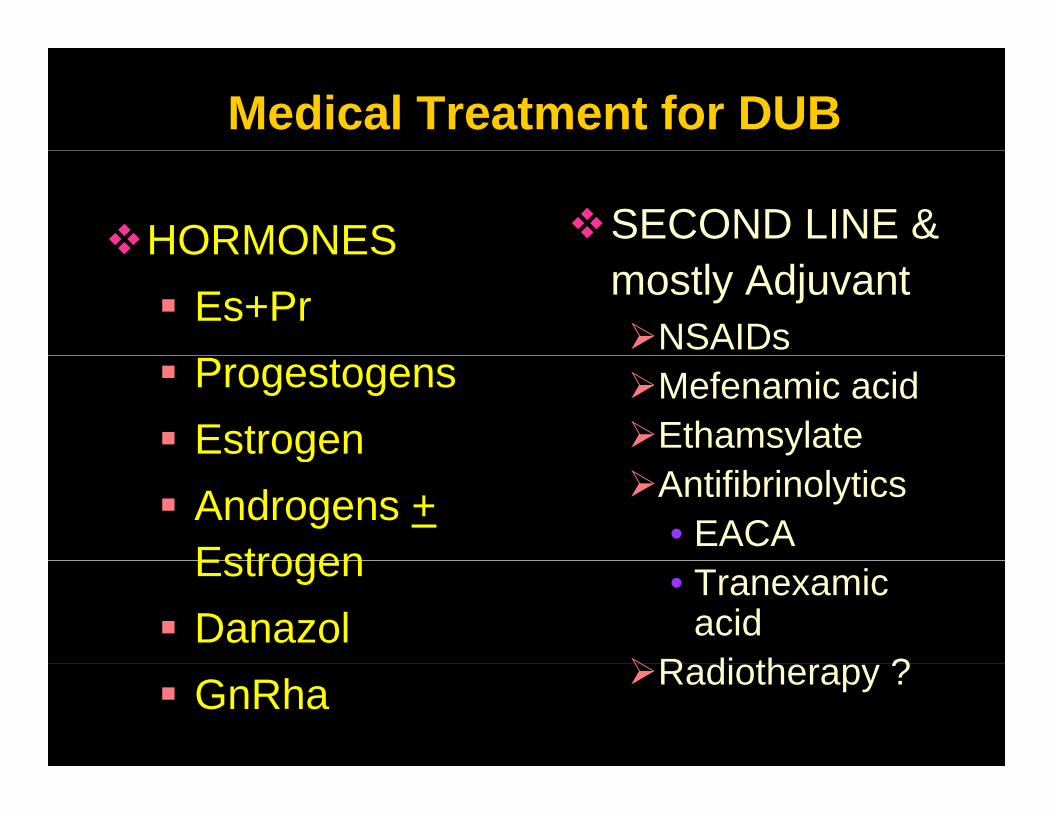
Medical Treatment for DUB
HORMONES SECOND LINE & HORMONES Es+Pr mostly Adjuvant
NSAIDsProgestogensEstrogen
Mefenamic acidEthamsylateg
Androgens +Estrogen
Antifibrinolytics• EACA
EstrogenDanazol
• Tranexamic acid
R di th ?GnRha Radiotherapy ?
Medical Treatment for DUBProblems: -
Treatment has to be indivisualisedNot suitable for all ages gResponse is erratic and unpredictableSIDE EFFECTS - Discontinuation andSIDE EFFECTS Discontinuation and noncomplianceFailures are commonFailures are common Cost effectiveness ? Surgery is often resorted toSurgery is often resorted to
Surgical Treatment of DUB
ENDOMETRIAL ABLATION: -
HYSTEROSCOPIC METHODS: -
• TCRE – Tran Cervical Resection Of
Endometrium
• ELA – Endrometrial Laser Ablation
• HTEA – Hydrothermal Endrometrial Ablation
Surgical Treatment of DUB
ENDOMETRIAL ABLATION: -
• RFEA – Radio Frequency Endometrial Ablation
NON HYSTREOSCOPIC METHODS: -q y
• TBEA – Thermal Balloon Endometrial Ablation• VSEA – Vestablate System Endometrial Ablationy• MWEA – Microwave Endometrial Ablation • ERA – Endometrial Resection and Ablation With a
Specialised Tissue Aspiration Resectoscope (STAR)• TUMA – Total Uterine Mucosa Ablation by a Calibrated
Uterine Resection Tool (CURT)
Surgical Treatment of DUB
HYSTERECTOMY: -
• VAGINAL HYSTERECTOMY• LAPAROSCOPICALLY ASSISTED V H• Lap Hys.- Total / SubtotalLap Hys. Total / Subtotal • Abdominal / MINILAP Hysterectomy- Total /
SubtotalSubtotal
Surgical Treatment of DUB
Curettage • HYSTERECTOMYProblems: -
CurettageMostly diagnosticNever gives a cure
HYSTERECTOMY• Invasive procedure• Not suitable at allNever gives a cure
Endometrial resection / ablation
• Not suitable at all ages
• Not without risksresection / ablationArray of methodsRecurrence is
• Not without risks• Costly• First option in 40+Recurrence is
commonAmenorrhoea gives
• First option in 40+ • DUB is the most common indicationcure common indication
Need of the Hour for the Treatment of DUBDUB
The ideal therapy should be a designer drugThe ideal therapy should be a designer drugwhich can block the action of Estrogen on
the Endometrium but not its beneficialthe Endometrium but not its beneficial actions on other tissues
“Selective Ostrogen Receptor Modulators”“D i O t ”“Designer Oestrogens”
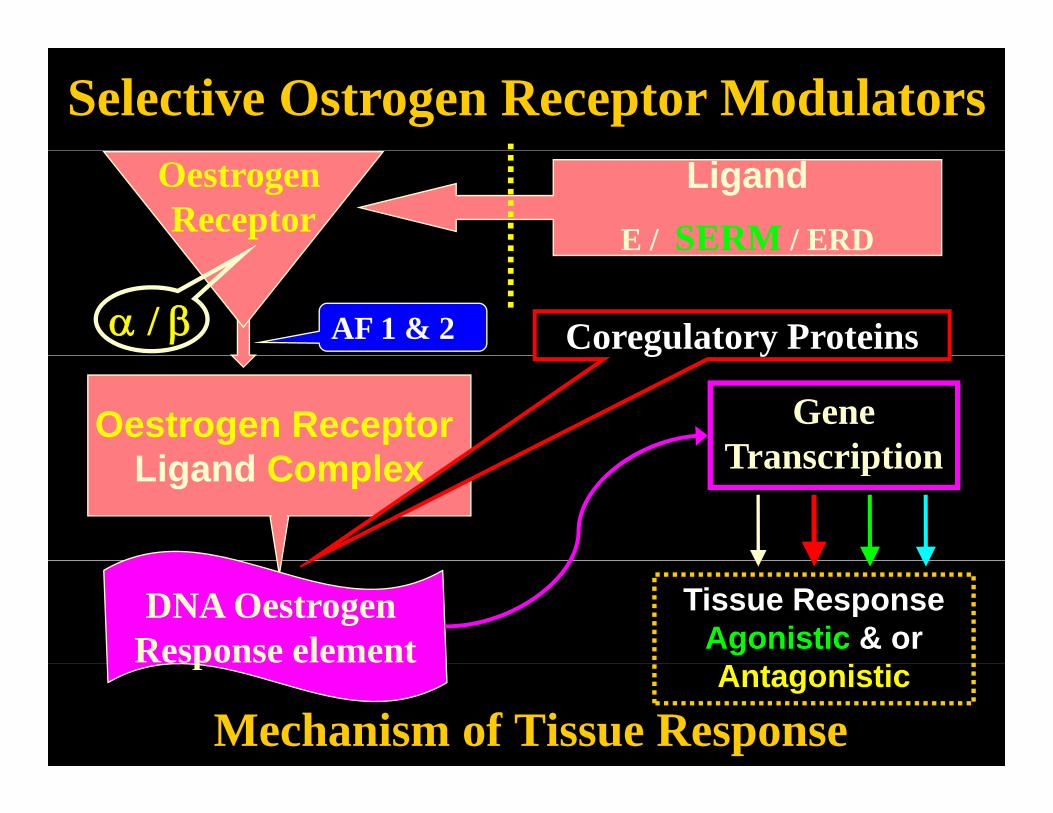
Selective Ostrogen Receptor ModulatorsOestrogen Receptor
LigandE / SERM / ERD
Coregulatory Proteinsα / β AF 1 & 2
Oestrogen Receptor Li d C l
Gene Transcription
g y
Ligand Complex Transcription
DNA Oestrogen Response element
Tissue Response Agonistic & or
Mechanism of Tissue Response
pAntagonistic

Selective Ostrogen Receptor Modulators
E tDesigned to act in
Estrogens
SERMs
specific ways at each of the oestrogen receptor
SERMs sites in different tissues
3 ORMELOXIFENE3.ORMELOXIFENE
2.Raloxifene
iDroloxifeneToremifene
Anti Estrogens 1.TamoxifeneDroloxifene
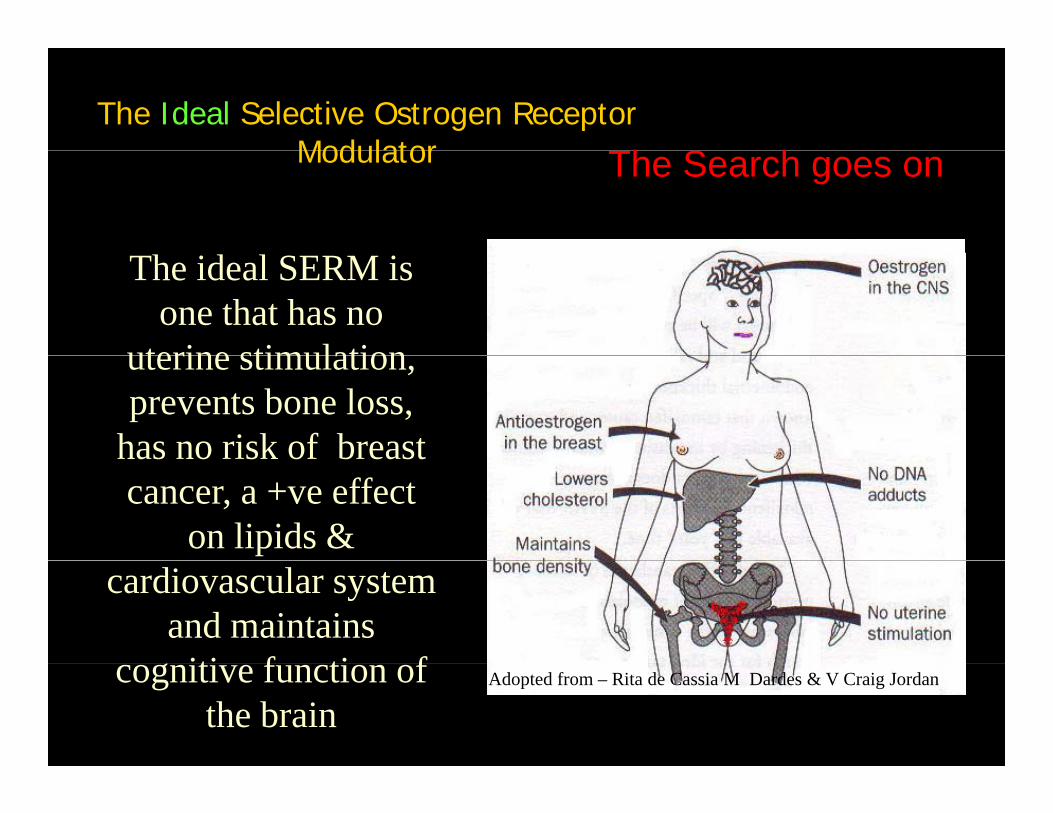
The Ideal Selective Ostrogen Receptor Modulator Th S hModulator The Search goes on
The ideal SERM is one that has no
uterine stimulationuterine stimulation, prevents bone loss,
has no risk of breasthas no risk of breast cancer, a +ve effect
on lipids & cardiovascular system
and maintains iti f ti fcognitive function of the brain
Adopted from – Rita de Cassia M Dardes & V Craig Jordan
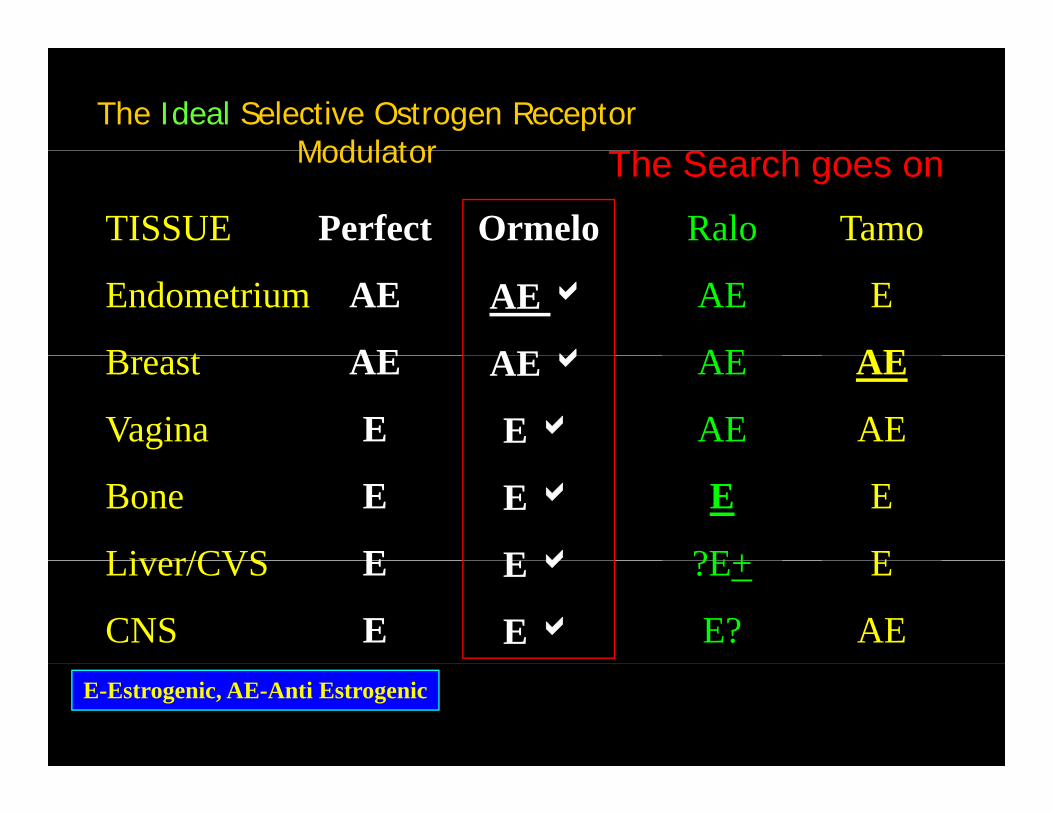
The Ideal Selective Ostrogen Receptor Modulator Th S hModulator The Search goes on
TISSUE Perfect Tamo Ralo Ormelo
Endometrium
B t
AE
AE
E
AE
AE
AE
AE a
AEaBreast
Vagina
AE
E
AE
AE
AE
AE
AE a
E a
Bone
Liver/CVS
E
E
E
E
E
?E+
E a
EaLiver/CVS
CNS
E
E
E
AE
?E+
E?
E a
E aE-Estrogenic, AE-Anti Estrogenic
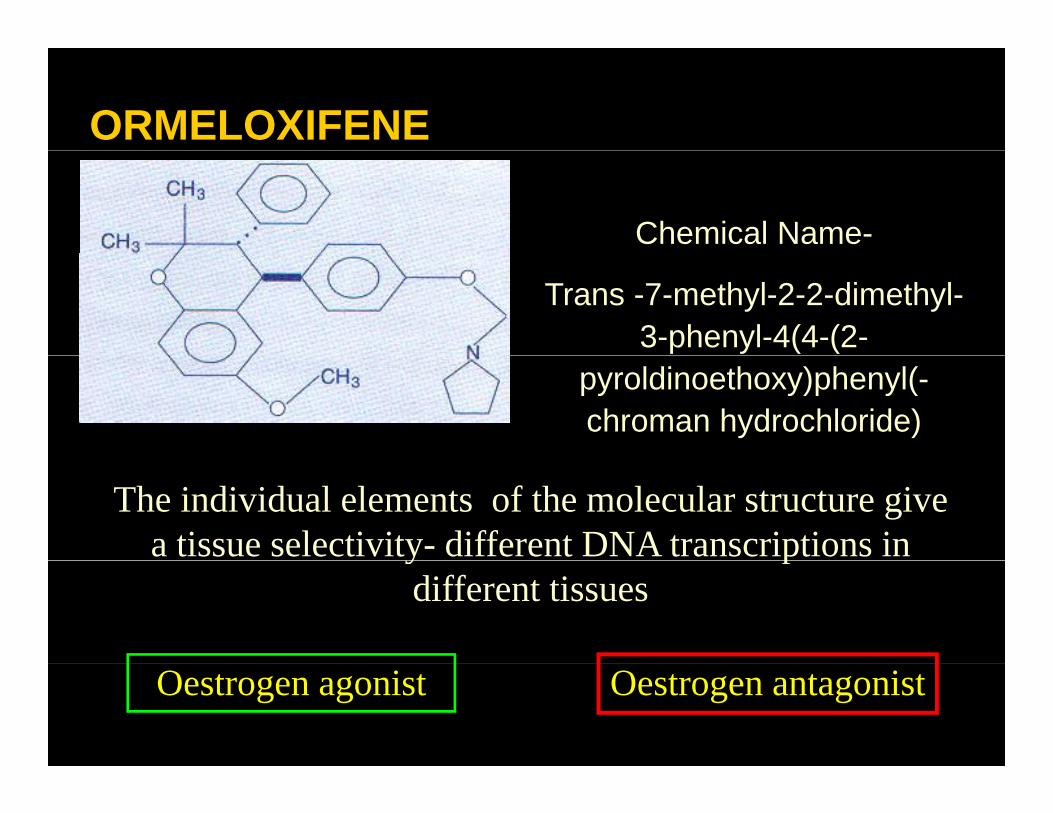
ORMELOXIFENE
Chemical Name-
Trans -7-methyl-2-2-dimethyl-3-phenyl-4(4-(2-
pyroldinoethoxy)phenyl(-chroman hydrochloride)
The individual elements of the molecular structure give a tissue selectivity- different DNA transcriptions in y p
different tissues
Oestrogen agonist Oestrogen antagonist
ORMELOXIFENEAn optimally designed SERM with Varied Tissue
Responsep
It blocks the cytosol receptors by its competitive binding affinity over Estradiolbinding affinity over Estradiol.
It not only causes a slow build up of the receptors, y p p ,but also causes their prolonged retention.
Its action lasts long after the drug is withdrawnwithdrawn.
ORMELOXIFENEAn optimally designed SERM with Varied Tissue
Responsep
Estrogen Antagonist in UTERUS & BREAST.
Mild Estrogenic action on Vagina, Bone mineral g g ,density, CNS and Serum Lipids.
No action on Hypothalamic Pituitary Ovarian function, Thyroid or Adrenal. No Progestational, , y g ,
Androgenic or Antiandrogenic properties
ORMELOXIFENEAn optimally designed SERM with Varied Tissue
Responsep
INDICATED for the treatment of Dysfunctional Uterine BleedingDysfunctional Uterine Bleeding
at ANY AGE.
Offers additional advantage of relief of PMS i i lin peirmenopausal women.
Not suitable for women desiring pregnancy because of its contraceptive property.
ORMELOXIFENEAn optimally designed SERM with Varied Tissue
Responsep
Women desiring contraception should use a barrier contraceptive for first two months
ORMELOXIFENEHas an excellent safety profile,very well tolerated & practically without any undesirable side effects& practically without any undesirable side effectsFew contraindications-• H/O Liver dysfunction or clinical jaundice• PCOD• Cervical Dysplasia, Chronic Cervicitis• H/O Hypersensitivity to the drug• Nursing mothers(6months).• Allergic conditionsg• Chronic illness renal disease & TB
ORMELOXIFENEHas an excellent safety profile,very well tolerated & practically without any undesirable side effects
Precaution-
& practically without any undesirable side effects
• Menstrual cycles may be delayed in some users.users.• Is of no concern if tablets have been taken
regularlyregularly.
• However if it exceeds 15days rule out pregnancypregnancy.
ORMELOXIFENEHas an excellent safety profile,very well tolerated & practically without any undesirable side effects
Easy to administer-
& practically without any undesirable side effects
yTwo 60mg tablets twice a week ( for
l S d & W d d ) f 12example, Sunday & Wednesday) for 12 weeks followed by one tablet of 60mg twice a week for another 12 weeks
ORMELOXIFENEAn optimally designed SERM with Varied Tissue
Responsep
Future possibility of use for-Fib•Fibromyoma,
•Adenomyosis•Endometriosis•Breast cancer (prevention & treatment)•Breast cancer (prevention & treatment)
•Osteoporosis (prevention & treatment)
•Menopause management.
ORMELOXIFENE
SummaryDysfunctional Uterine Bleeding is a very common disorder at all ages from menarche to menopause.
Though its pathophysioology is still unclear, Estrogen-Progesterone imbalance is usually the basis of bleeding.
Available medical treatment modalities are far from satisfactory.
Ormeloxifene, the latest Selective Estrogen Receptor Modulator, is closest to the perfect SERM, having the desired antirestrogenic and estrogenic action in differentdesired antirestrogenic and estrogenic action in different tissues.
ORMELOXIFENE
SummaryIt has a very good safety profile and well tolerated, being practically devoid of sidetolerated, being practically devoid of side effects.
It is easy to administer and cost effective.
However extensive large scale clinicalHowever extensive large scale clinical trials are needed to establish its effectiveness and safety

Recommended