3/5/2014
1
Proactively Preventing Ventilator-associated Events (VAE)
Suzi M. Burns RN, MSN, RRT, ACNP, CCRN, FAAN, FCCM, FAANP
3/5/2014
2
Suzi M. Burns RN, MSN, RRT, ACNP, CCRN, FAAN, FCCM, FAANP
Professor Emeritus, University of Virginia
Independent consultant
Published author and speaker
AACN Flame of Excellence Award recipient
Copyright © 2014 American Association of Critical-Care Nurses
Webinar Goals
Implement evidence-based VAE prevention strategies right away.
Topics
History of CDC’s ventilator-associated pneumonia (VAP) surveillance definitions and rationale for change
Four new CDC 2013 VAE categories
Evidence-based VAE preventive strategies
Barriers and solutions to implementation
3/5/2014
3
Copyright © 2014 American Association of Critical-Care Nurses
VAP Impact on Patient Outcomes Increased morbidity, mortality, hospital LOS
*Replaced National Nosocomial Infection Surveillance System (NNIS)
National Healthcare Safety Network (NHSN)* reported for 2013:
>3,525 VAPs
Hospital units: 0.0-5.8 per 1,000 ventilator days
Copyright © 2014 American Association of Critical-Care Nurses
History of VAP Surveillance
3/5/2014
4
Copyright © 2014 American Association of Critical-Care Nurses
History of VAP
New surveillance criteria implemented
VAP defined as “PNEU” event within 48 hours of mechanical ventilation
1970 1980 1990 2000 2002
CDC’s NNIS starts surveillance for nosocomial pneumonia
Copyright © 2014 American Association of Critical-Care Nurses
Diagnosing VAP Using 2002 Criteria Determined by:
Subjective clinical signs/symptoms
Radiographic evidence
Laboratory data
Not sensitive or specific compared with histopathological “gold standard”
Copyright © 2014 American Association of Critical-Care Nurses
3/5/2014
5
Copyright © 2014 American Association of Critical-Care Nurses
Consequences of Vague VAP Criteria
Hospitals and even their own units:
Employed divergent and noncomparable approaches to VAP surveillance and reporting
Included some “gaming”
Copyright © 2014 American Association of Critical-Care Nurses
Copyright © 2014 American Association of Critical-Care Nurses
Repercussions for… Clinicians and Researchers Hard to identify effective strategies
to prevent/treat VAP
Public health Healthcare-associated infections at heart
of healthcare policy and prevention initiatives
Hospitals Reimbursement programs linked to
outcomes (Medicare/Medicaid)
Conclusion: Need for accurate, reliable outcome measurement!
3/5/2014
6
Copyright © 2014 American Association of Critical-Care Nurses
A New Approach
Copyright © 2014 American Association of Critical-Care Nurses
National Quality Forum (NQF)
Role: To set standards for healthcare
Focus: Improve healthcare quality
Asked CDC to reconsider VAP criteria
Copyright © 2014 American Association of Critical-Care Nurses
3/5/2014
7
Copyright © 2014 American Association of Critical-Care Nurses
CDC Responds
Convenes leaders
from Critical Care
Societies Collaborative
(AACN, ACCP, ATS,
SCCM) and others from
key organizations.
2010 2011
Purpose: Identify objective approach to surveillance/reporting in mechanically ventilated patients
2012 2013
Copyright © 2014 American Association of Critical-Care Nurses
CDC Workgroup Develops surveillance definition algorithm
Identifies broader range of VAEs
Finds most VAEs due to
Pneumonia
ARDS
Atelectasis
Pulmonary edema
All potentially preventable by nurses!
Magill SS, et al. Am J Crit Care. 2013;22(6):469-473.
3/5/2014
8
Copyright © 2014 American Association of Critical-Care Nurses
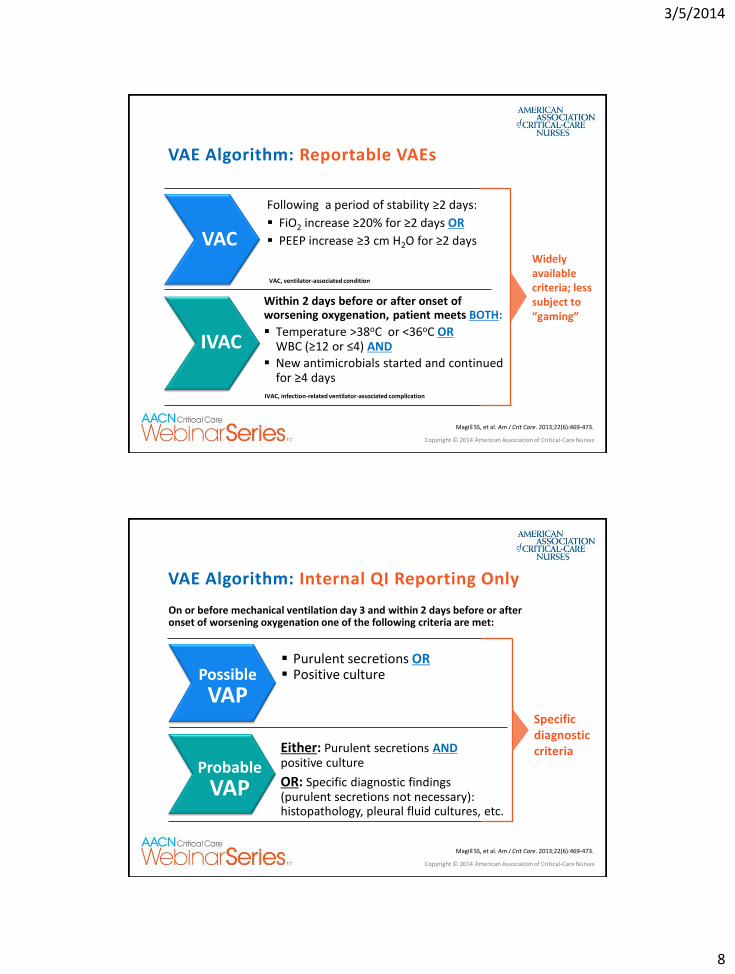
Within 2 days before or after onset of worsening oxygenation, patient meets BOTH:
Temperature >38oC or <36oC OR WBC (≥12 or ≤4) AND
New antimicrobials started and continued for ≥4 days
VAE Algorithm: Reportable VAEs
VAC
Following a period of stability ≥2 days:
FiO2 increase ≥20% for ≥2 days OR
PEEP increase ≥3 cm H2O for ≥2 days
IVAC
Widely available criteria; less subject to “gaming”
VAC, ventilator-associated condition
IVAC, infection-related ventilator-associated complication
Magill SS, et al. Am J Crit Care. 2013;22(6):469-473.
Copyright © 2014 American Association of Critical-Care Nurses
Either: Purulent secretions AND positive culture
OR: Specific diagnostic findings (purulent secretions not necessary): histopathology, pleural fluid cultures, etc.
VAE Algorithm: Internal QI Reporting Only
Possible VAP
Purulent secretions OR Positive culture
Specific diagnostic criteria
Possible
VAP
Probable
VAP
On or before mechanical ventilation day 3 and within 2 days before or after onset of worsening oxygenation one of the following criteria are met:
Magill SS, et al. Am J Crit Care. 2013;22(6):469-473.
3/5/2014
9
Copyright © 2014 American Association of Critical-Care Nurses
Challenges Related to Changing VAP Criteria
Unknowns
How historical rates based on old definition compare with “possible” and “probable” VAP
Accuracy of previously reported hospital rates comparing pre- and post outcomes of interventions
Makes identifying preventive strategies difficult
Copyright © 2014 American Association of Critical-Care Nurses
Copyright © 2014 American Association of Critical-Care Nurses
What is the relationship of VACs to IVAC, Possible and Probable VAP?
Looking at the Science
3/5/2014
10
Copyright © 2014 American Association of Critical-Care Nurses
Muscedere J, et al. J Crit Care. 2008;23:138-47.
Study 1: Developing Evidence-based Guidelines for VAP Prevention
Method: Systematic review of science related to prevention of VAP
Sample: All randomized controlled trials (RCTs) and systematic reviews on VAP prevention in adults, published from 1980 to October 2006
Copyright © 2013 American Association of Critical-Care Nurses
Results: Evidence-based Guidelines for Prevention
Consider
Intubate orally
Change ventilator circuit only if soiled
Change airway humidifiers every 5-7 days as indicated
Use closed suctioning system
Change suctioning systems only as needed
Use subglottic secretion drainage for expected ventilation >72 hrs
Set HOB at 45o when possible
Use oral antiseptic (chlorhexidine)
Recommended
Muscedere J, et al. J Crit Care. 2008;23:138-47.

3/5/2014
11
Copyright © 2014 American Association of Critical-Care Nurses
Sinuff T, et al. Crit Care Med.2013;41:15-23.
Study 2: Implementing VAP Prevention Guidelines: Correlation with Guideline Adherence and VAP Rates
Design: Prospective study: 2007-2009
Sample: 11 community and academic medical center ICUs; 30 adults/site (330 total) for each of 4 time periods Total=1,320 patients
Method: Implementation of 14 VAP evidence-based diagnostic, treatment and prevention guidelines
Copyright © 2014 American Association of Critical-Care Nurses
Copyright © 2014 American Association of Critical-Care Nurses
Results: Increased Adherence to VAP Guidelines Correlates With Decreased Incidence of VAP
Sinuff T, et al. Crit Care Med. 2013;41:15-23.
Change from baseline
Adherence to VAP Guidelines (P=0.007)
VAP Rates (P=0.003)
15.8% 38.3%
3/5/2014
12
Copyright © 2014 American Association of Critical-Care Nurses
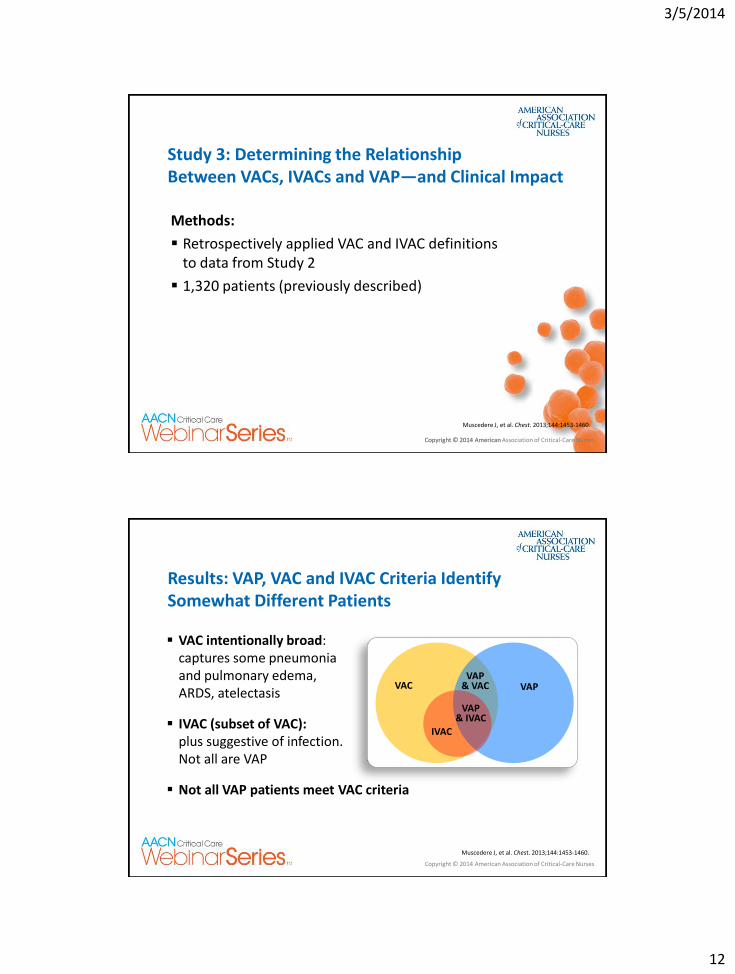
Study 3: Determining the Relationship Between VACs, IVACs and VAP—and Clinical Impact
Methods:
Retrospectively applied VAC and IVAC definitions to data from Study 2
1,320 patients (previously described)
Muscedere J, et al. Chest. 2013;144:1453-1460.
Copyright © 2014 American Association of Critical-Care Nurses
Copyright © 2014 American Association of Critical-Care Nurses
VAC intentionally broad: captures some pneumonia and pulmonary edema, ARDS, atelectasis
IVAC (subset of VAC): plus suggestive of infection. Not all are VAP
Not all VAP patients meet VAC criteria
Results: VAP, VAC and IVAC Criteria Identify Somewhat Different Patients
VAC
IVAC
VAP & IVAC
VAP & VAC VAP
Muscedere J, et al. Chest. 2013;144:1453-1460.
3/5/2014
13
Copyright © 2014 American Association of Critical-Care Nurses
Conclusions
Poor agreement between VAC, IVAC and VAP
Patients with a VAC or IVAC:
Significantly more Ventilator days
Hospital days
Antibiotic days
Higher hospital mortality than those with neither condition
Higher adoption of VAP preventative measures lower VAP and VAC rates
Copyright © 2014 American Association of Critical-Care Nurses
Preventing VAEs

3/5/2014
14
Copyright © 2014 American Association of Critical-Care Nurses
How VACs Occur Particularly IVAC and Possible/Probable VAP
Sterile lower respiratory tract breeched from:
Aspiration of secretions
Colonization of aerodigestive tract
Contaminated equipment or medications
Copyright © 2014 American Association of Critical-Care Nurses
Copyright © 2014 American Association of Critical-Care Nurses
Associated Risk Factors
Prolonged intubation
Enteral feeding
Witnessed aspiration
Paralytic agents/sedation
Underlying illness (immune-suppressed)
Extremes of age Evidence-based approach is needed:
Target key risk factors for lung contamination
3/5/2014
15
Copyright © 2014 American Association of Critical-Care Nurses
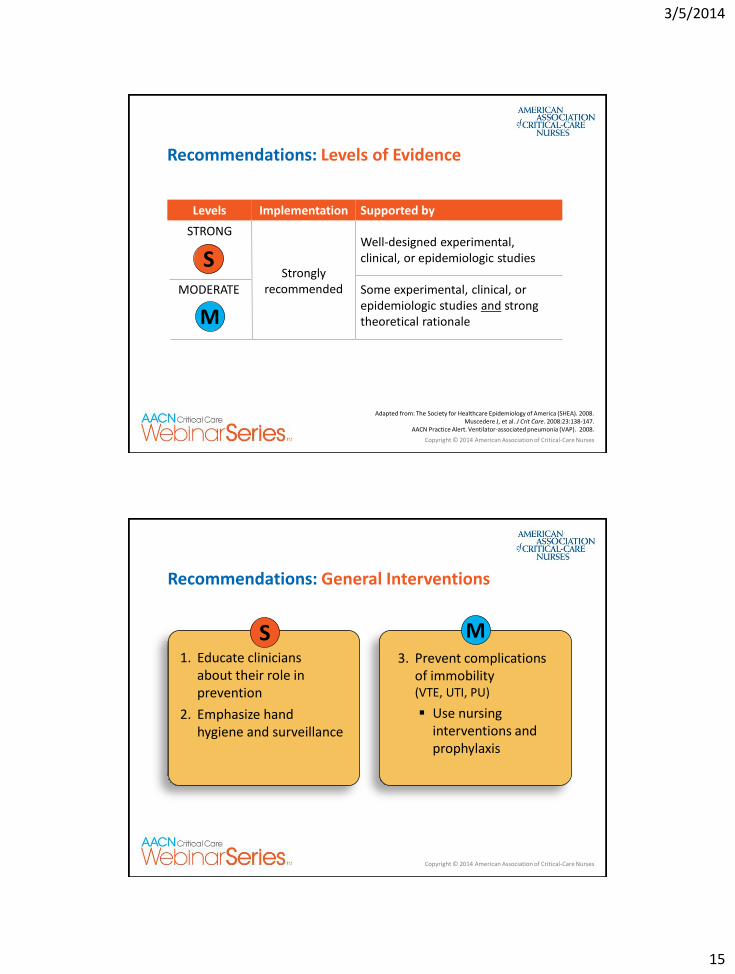
Adapted from: The Society for Healthcare Epidemiology of America (SHEA). 2008. Muscedere J, et al. J Crit Care. 2008:23:138-147.
AACN Practice Alert. Ventilator-associated pneumonia (VAP). 2008.
Recommendations: Levels of Evidence
Levels Implementation Supported by
STRONG
Strongly recommended
Well-designed experimental, clinical, or epidemiologic studies
MODERATE Some experimental, clinical, or epidemiologic studies and strong theoretical rationale
S
M
Copyright © 2014 American Association of Critical-Care Nurses
Recommendations: General Interventions
1. Educate clinicians about their role in prevention
2. Emphasize hand hygiene and surveillance
3. Prevent complications of immobility (VTE, UTI, PU)
Use nursing interventions and prophylaxis
S M
3/5/2014
16
Copyright © 2014 American Association of Critical-Care Nurses
Barriers
Inconsistent
Hand hygiene (better when observed)
Knowledge of VAP prevention
Insufficient attention to “interventional hygiene” (targeting mobility, VAP, BSI, UTI, PU)
McGuckin, et al, nurses fail to:
Adequately understand value of interventional hygiene
Take ownership
Blot SI, et al. Intensive Care Med. 2007;3:1463-1467. Cason CL, et al. Am J Crit Care. 2007:16;28-37.
McGuckin M, et al. Am J Infect Control. 2008;36:59-62.
Copyright © 2014 American Association of Critical-Care Nurses
Copyright © 2014 American Association of Critical-Care Nurses
Solutions
Reinforce education regularly
Provide tools, resources, processes to facilitate interventional hygiene
Develop a culture of accountability
Example: “Intentional Rounds”
3/5/2014
17
Copyright © 2014 American Association of Critical-Care Nurses
Intentional Rounds Promote Culture Change
Don’t tell me—show me at the bedside!
APN selects patient(s)
APN discusses all aspects of care
Focus: Prevention and key nurse sensitive metrics
Very popular and well attended!
Mahanes D, et al. Intensive Crit Care Nurs. 2013;29(5):256-260.
Copyright © 2014 American Association of Critical-Care Nurses
Recommendation 2: Prevent Aspiration
Use cuffed tube and continuous aspiration of subglottic secretions (CASS)
Maintain cuff pressures ~20 cm H2O
Maintain HOB (or backrest elevation) at 30-45o
Prevent gastric overdistension
M
3/5/2014
18
Copyright © 2014 American Association of Critical-Care Nurses
Barriers
CASS tubes considered too expensive; not always available (recommended if >72 hours of ventilation)
HOB elevation rarely maintained
Cuff pressures vary with changes in position
Grap MJ, et al. Am J Crit Care. 1999;8:475–480. van Nieuwenhoven CA, et al. Crit Care Med. 2006;34:396–402.
Ballew C, et al. Am J Crit Care. 2011;20:395-399.
Copyright © 2014 American Association of Critical-Care Nurses
Solutions
Compare costs related to CASS tubes with VAP-related costs
Audit and provide education frequently on:
Use of bed-level indicators and appropriate backrest elevation
Monitor and maintain cuff pressures (evaluate in different positions)
3/5/2014
19
Copyright © 2014 American Association of Critical-Care Nurses
Recommendation 3: Reduce Gastric Colonization
Perform regular oral care (timing/type unresolved)
Orotracheal vs nasal intubation (risk of sinusitis)
S M
Copyright © 2014 American Association of Critical-Care Nurses
Barriers
Oral care takes time
Other aspects of care considered more important
Protocol for intubations may not stress use of oral route.
Other units (ED, etc.) may not know about preference for oral route
Copyright © 2014 American Association of Critical-Care Nurses
3/5/2014
20
Copyright © 2014 American Association of Critical-Care Nurses
Solutions
Oral Care
Educate staff on importance of oral care
Determine consistent approach including time/type (unresolved evidence for frequency)
Make it easy to accomplish and provide reminders
Identify champions
Take ownership of oral care
Copyright © 2014 American Association of Critical-Care Nurses
Solutions (continued)
Orotracheal vs nasal intubations
Educate staff to request oral intubation
Collaborative with other units (ED, anesthesia, etc.) to assure oral intubations
3/5/2014
21
Copyright © 2014 American Association of Critical-Care Nurses
Recommendation 4: Reduce Risk of Contamination of Respiratory Equipment
Wash hands
Change tubing and equipment only when visibly soiled
Use sterile water when rinsing reusable respiratory equipment
Properly store and disinfect
S
Copyright © 2014 American Association of Critical-Care Nurses
Barriers and Solutions
Barrier
Lack of policies governing care and cleaning of equipment
Solution
Collaborate with Respiratory Care to ensure recommendations are implemented and monitored
3/5/2014
22
Copyright © 2014 American Association of Critical-Care Nurses
Recommendation 5: Prevent Complications of Mechanical Ventilation
*View August 2013 Pain and Sedation webinar for additional information
Consider noninvasive ventilation (easy access/protocols to promote use)
Prevent unplanned extubations and reintubations
Minimize sedation; discontinue early
Perform daily “Wake Up and Breathe Trials”
Use protocols for sedation withdrawal and spontaneous breathing trials (SBTs)*
S
Copyright © 2014 American Association of Critical-Care Nurses
Barriers Non-invasive ventilation and unplanned extubation Noninvasive ventilation is:
Often considered too late
Hard to apply effectively in emergencies
Rates of unplanned extubations/reintubations often unknown
Result: lack of prevention strategies to reduce rates
Misconception that physical restraints may prevent unplanned extubation
Copyright © 2014 American Association of Critical-Care Nurses
3/5/2014
23
Copyright © 2014 American Association of Critical-Care Nurses
Solutions Noninvasive ventilation and unplanned extubation
Noninvasive ventilation: develop protocols for indications and uses; educate staff
Instead of physical restraints (which do not prevent unplanned extubation):
Use pharmacologic agents sparingly
Assess for delirium
Do not delay SBTs if indicated
Copyright © 2014 American Association of Critical-Care Nurses
Barriers Limiting sedation
Misperceptions:
Patients prefer to be sedated
Sedation promotes patient comfort
It’s better if patients don’t remember being ventilated
Withdrawing sedation causes psychological stress
Sedation best via infusion to deliver steady state of the drug
Guttormson JL, et al. Crit Care Nurs, 2010;26(1):44-50. Kress JP, et al. Am J Respir Crit Care Med. 2003;168(12):1457-1461.
3/5/2014
24
Copyright © 2014 American Association of Critical-Care Nurses
Solutions Limiting sedation Educate staff about use of sedation, misconceptions,
and potential complications, eg:
Prolonged ventilation
Adverse clinical outcomes (delirium, cognitive dysfunction etc.)
Treat pain first
Start sedation only if clearly indicated (eg, anxiety, paralytic use).
Copyright © 2014 American Association of Critical-Care Nurses
Copyright © 2014 American Association of Critical-Care Nurses
Barriers and Solutions “Wake Up and Breathe Trials”
Barriers
Time consuming
Difficult to ensure they are performed
Solution
Nurses, therapists and physicians must consider optimal timing of trials for all involved
3/5/2014
25
Copyright © 2014 American Association of Critical-Care Nurses
Summary
Copyright © 2014 American Association of Critical-Care Nurses
Summary
New CDC VAE algorithm designed to make surveillance of VAEs (including VAP) more accurate.
Accuracy of definitions will help establish validity of preventive strategies
Strategies associated with lower rates of VAP and VAC include:
Preventing aspiration
Reducing gastric colonization
Reducing risk of contamination of respiratory equipment
Weaning off ventilator ASAP
Copyright © 2014 American Association of Critical-Care Nurses
3/5/2014
26
Copyright © 2014 American Association of Critical-Care Nurses
Prevention of VAEs is possible and nurses can make a difference! Our patients’ lives depend on it!
As Yoda said….
"Do or not do. There is no try!”
Copyright © 2014 American Association of Critical-Care Nurses
AACN Implementation Tools and Resources
Tools and Tactics: Blue Print for Reducing VAEs
A Gap Analysis for Reducing VAEs
AACN Practice AlertsTM: Oral Care for Patients at Risk for VAP Prevention of Aspiration Audit of HOB Elevation in Intubated Patients Assessing Pain in the Critically Ill Adult
SAS and RASS Sedation Assessment Tools
BPS and CPOT Pain Assessment Scales
Nurse-driven Pain and Sedation Protocol
Wake Up and Breathe Protocol
Early Progressive Mobility Protocol
Designed to help you apply these practices in your environment
Find these tools on the VAE webinar information page at www.aacn.org.

3/5/2014
27
Copyright © 2014 American Association of Critical-Care Nurses
Prevent Ventilator Associated Events Now— Improve Patient Outcomes
1. Download the Implementation Tools. Find them on the VAE webinar information page at www.aacn.org.
2. Discuss the tools and recommended practices with your colleagues.
3. Implement practices that are suitable for your unit.
4. Join the Webinar Series Learn Network online discussion forum to continue the conversation.
Recommended

















