Prevention and Treatment of DVT and PE (VTE)
L. Bernardo Menajovsky, MD, MS. Associate Professor of Medicine Director, Anticoagulation Clinics
Texas A&M Health Sciences Center College of Medicine Scott & White Memorial Hospital and Clinic
Temple, Texas, USA
Need for recommendations - guidelines
• Most practitioners need to identify the useful and pertinent information for practice
When it comes to anticoagulation management…
ACCP guidelines 2012 AT9
However…
There are several others…
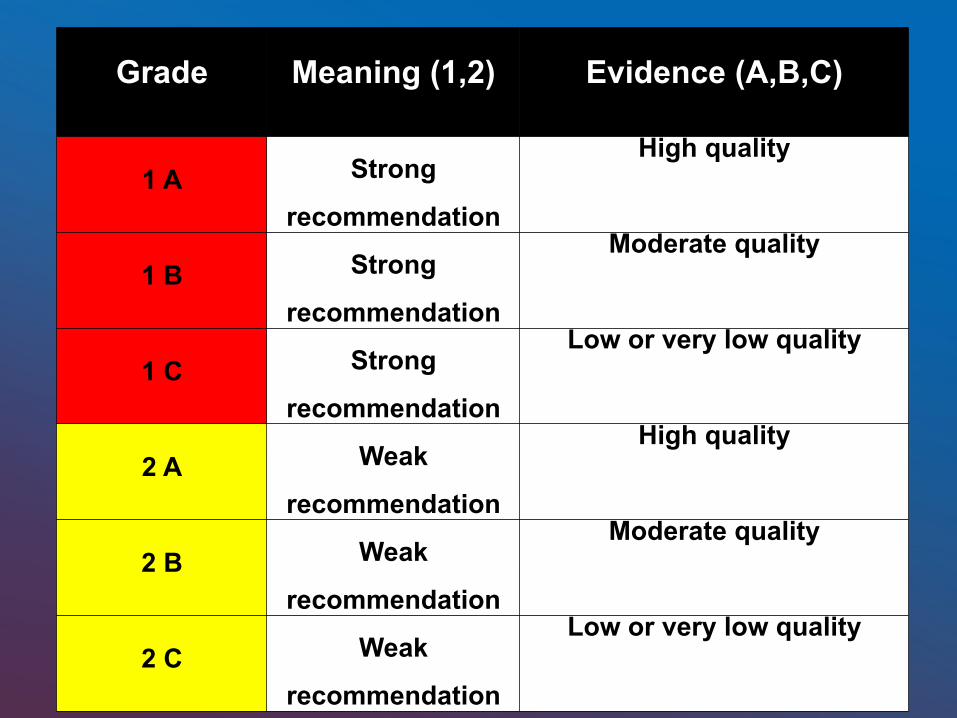
Grade
Meaning (1,2)
Evidence (A,B,C)
1 A Strong
recommendation
High quality
1 B Strong
recommendation
Moderate quality
1 C Strong
recommendation
Low or very low quality
2 A Weak
recommendation
High quality
2 B Weak
recommendation
Moderate quality
2 C Weak
recommendation
Low or very low quality
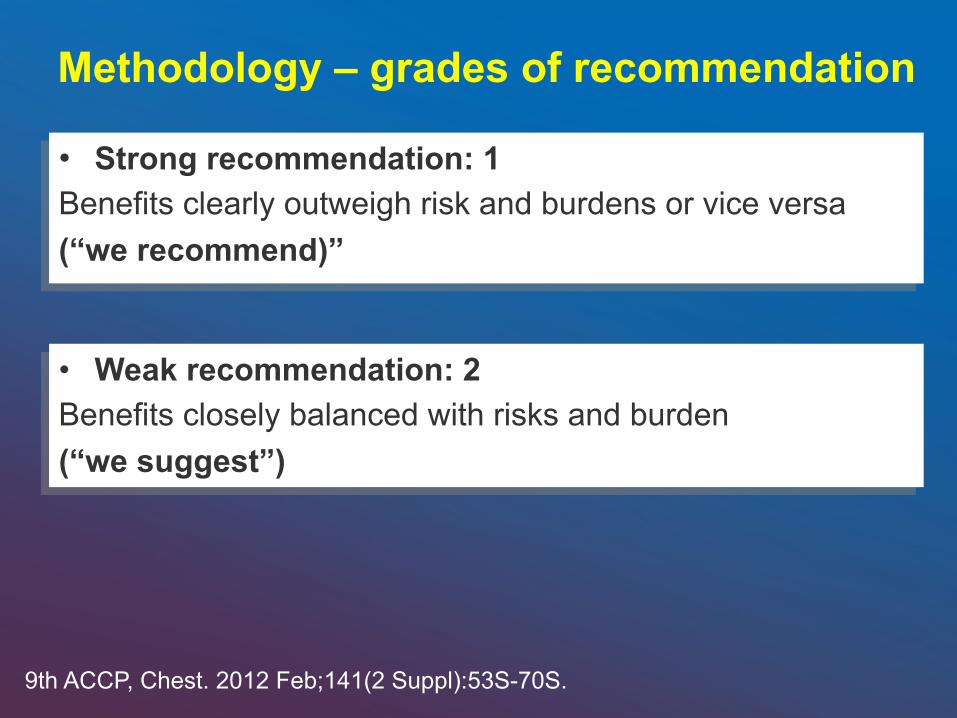
• Strong recommendation: 1 Benefits clearly outweigh risk and burdens or vice versa (“we recommend)”
Methodology – grades of recommendation
• Weak recommendation: 2 Benefits closely balanced with risks and burden (“we suggest”)
9th ACCP, Chest. 2012 Feb;141(2 Suppl):53S-70S.

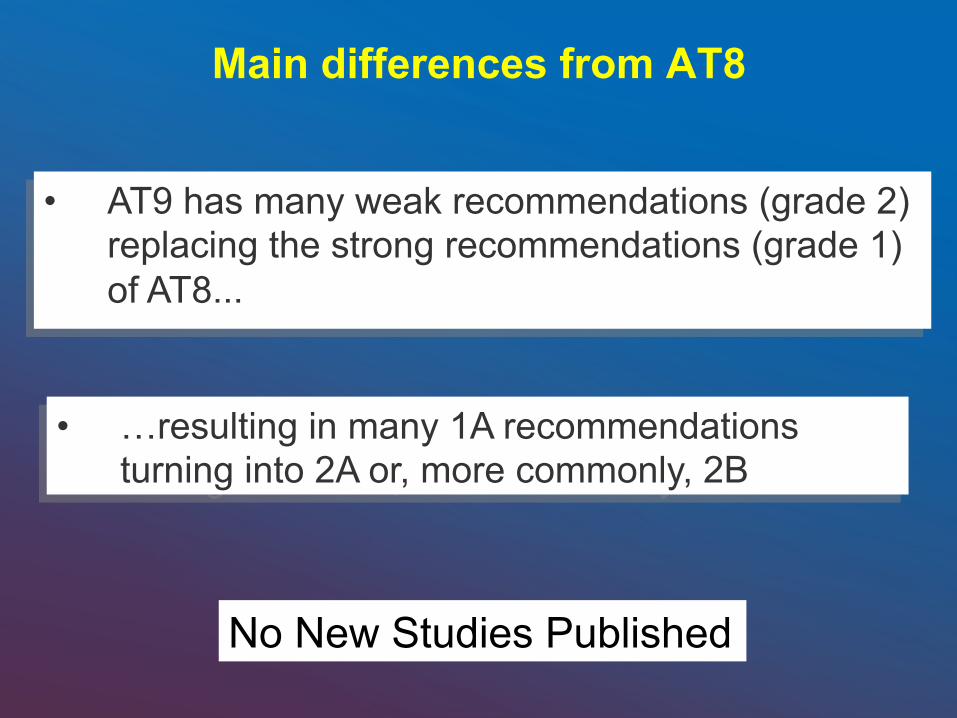
• AT9 has many weak recommendations (grade 2) replacing the strong recommendations (grade 1) of AT8...
Main differences from AT8
• …resulting in many 1A recommendations turning into 2A or, more commonly, 2B
No New Studies Published
Methodology for AT9 • More rigorous evaluation of studies with standardized
methodology, reviewing the risk of bias, imprecision and inconsistency of results of a RCT
• Attempt to exclusion of financial and intellectual conflicts of interest • Authors involved:
• Editor: Methodologists • Clinicians with few experience on the subject • Panelists: the experts (no voting)
• Caution in interpretation of single studies and recommendations
9th ACCP, Chest. 2012 Feb;141(2 Suppl):53S-70S.
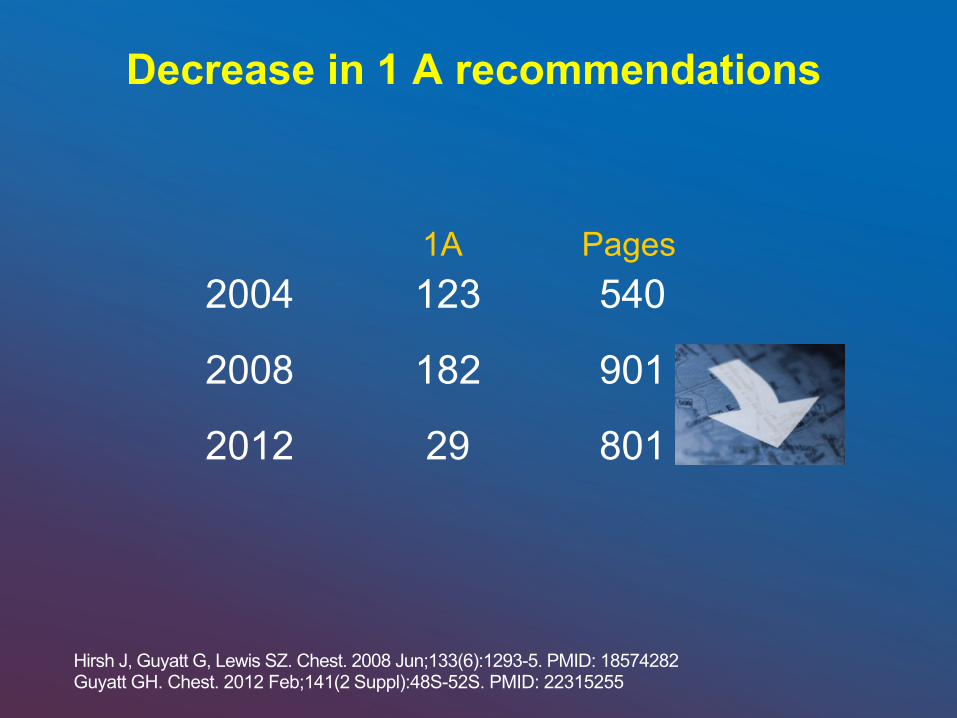
Decrease in 1 A recommendations
2004 123 540 2008 182 901 2012 29 801
1A Pages
Hirsh J, Guyatt G, Lewis SZ. Chest. 2008 Jun;133(6):1293-5. PMID: 18574282 Guyatt GH. Chest. 2012 Feb;141(2 Suppl):48S-52S. PMID: 22315255
• Apply recommendations to particular clinical scenarios
and check whether these recommendations fit them
• It is always useful to read the small prints!
Recommendations AT9
Big Change
• Hard Outcomes = Clinically significant VTE • Soft Outcomes = Venographic or US VTE
12
Facts
• 50% clinically significant DVT – Asymptomatic
• 60-70% of Fatal PE – Asymptomatic DVT
Heit JA, et al. Arch Intern Med. 1999;159:445.
Application of Guidelines
Real Life Cases
Case Study #1
27-year-old woman, who began having left leg pain 6 days ago, woke up in the morning with the pain. Since the pain did not go away, she then went to the ED. The patient states that she has felt otherwise well. She denies any swelling of the leg or warmth, but she does complain of tenderness to palpation.
Case Study #1 (cont…)
• PMH: Non-contributory. • FH: Father prostate cancer. No clotting disorders • PSH: Repair of septated uterus in 2003. • SH: No smoking. Occ alcohol. No illicit drug use. • ALLERGIES: allergic to penicillin. • ROS: Just back from a non-stop 10 hr. car trip. • MEDS: OCPs since age 17.
16
Case Study #1 (PE)
• VS: BP 123/83, HR 88, RR 18, O2 sat on RA 97%. Temp 101.0.
• GEN: moderate distress (pain). • HEENT; NECK; CV; LUNGS; ABD; all normal. • EXTREMITIES: Mod tenderness to palp in left
calf. Leg is warm, 1+ edema and erythema, positive Hommans sign. 2+ pedal pulses.
• The patient did not ambulate, but states that she has been walking with a limp because of the pain.
17
Case Study #1 (Labs)
• CBC: WBC 10.3, Hgb 13.1, Hct 38.4, plat 153. • CMP, and LFTs within normal limits. • INR 1.2. • Serum pregnancy test is pending.
18
Q1: What is your diagnosis?
1. DVT vs. Cellulitis. 2. Cellulitis vs. DVT. 3. Other
19
DVTvs.Cellulitis.
Cellulitisvs.D
VT.
Other
33%33%33%
:10
Q2: What is your next step?
1. Doppler US lower extremity veins.
2. High sensitivity D- dimer.
3. Start treatment immediately.
4. Hypercoagulable panel.
5. 2 and 4
20
DopplerUSlowerextremi..
HighsensitivityD‐dimer.
Starttreatm
entim
media...
Hypercoagulablepanel.
2and4
20% 20%20%20%20%
:15
Q3: Potential contributing factors for this patient’s condition are (except)?
1. Use of OCPs 2. Long dist travel. 3. 1 and 2. 4. Age 5. None: All are
contributing factors.
23
UseofOCPs
Longdisttravel.
1and2. Ag
e
None:Allarecontributin...
20% 20%20%20%20%
:10
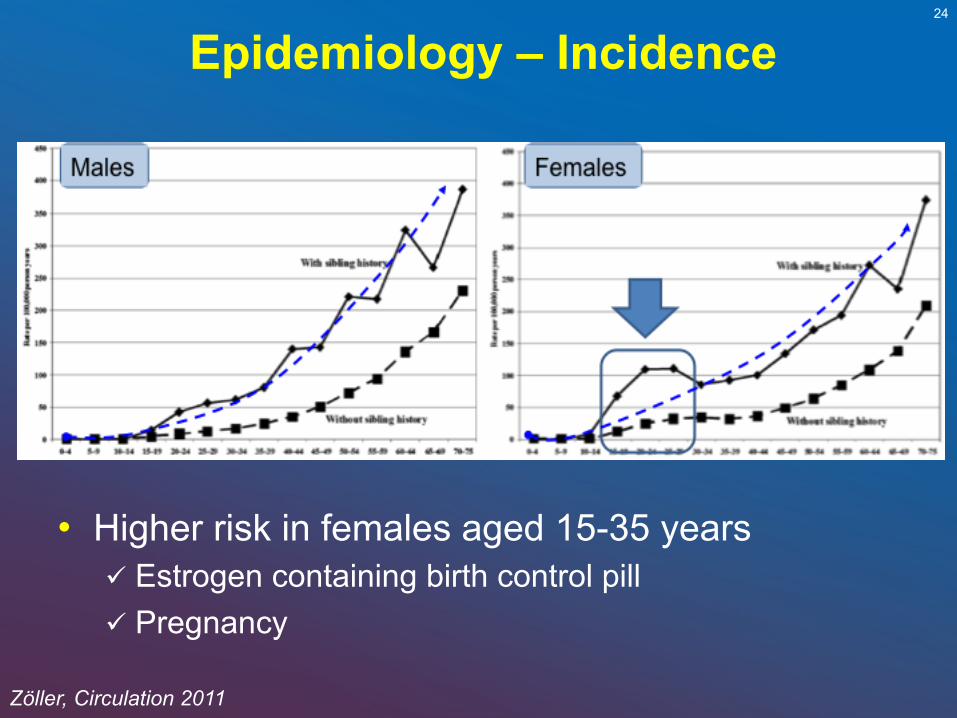
Epidemiology – Incidence 24
Zöller, Circulation 2011
• Higher risk in females aged 15-35 years Estrogen containing birth control pill Pregnancy
Epidemiology of VTE and HT
• 99% of cases occur during the first 2 years • 90% within the first 6 months.
Zöller, Circulation 2011
Long distance travel and VTE
• Evidence is poor • Events are unusual • The majority of patients have other major risk
factors • Only air travel longer than 6 hours in economy
class has been studied • Not a single study on land travel.
Case 1 (cont…)
• All tests you order are pending and you decide to start systemic anticoagulation.
27
Q4: In addition you order the following:
1. Stop OCPs (particularly estrogen based) immediately and never use them again.
2. Avoid traveling for at least one year.
3. Graduated compression stockings, 40 mmHg at level of ankle
4. Bed rest for at least one week.
5. 1 and 2
28
StopO
CPs(particularly...
Avoidtravelingforatlea..
Graduatedcompression...
Bedrestforatleastone...
1and2
0% 0%0%0%0%
:20
Estrogen-related VTE – Management
• Attitude towards contraception Stop the estrogen-containing pill
- No rush (anticoagulant therapy) - Refer to the physician in charge of her contraception - Estrogens should be stopped ideally 6 weeks prior to
anticoagulant discontinuation
Which contraception after a VTE? - Mechanical - Progestin-only pill or levonorgestrel-releasing intra-uterine
device (Mirena®) appear inoffensive, although no RCT is available to support this attitude. Avoid injectable progesterone
- Never resume an estrogen-containing contraceptive
29
Conard, Contraception 2004
Estrogen-related VTE - Prevention
• Avoid their use in women with other VTE risk factors Age > 35 years Obese Family hx of VTE, particularly if first degree relatives
with hormone-related thrombosis Known thrombophilia (but no evidence to support
prior testing) Current smokers Hx of diabetes, hypertension, dyslipidemia
30
Case 2 • 42 y/o white man comes to the ED with a 1 day
h/o pain and swelling of the left upper extremity. • The patient states that he was helping his
brother-in-law moving to his brand new 2nd story apartment over the weekend.
• PMH: unremarkable. • PSH: Appendectomy as a child. • FHx: Parents alive and well; one sister (32) in
good health except for trouble getting pregnant. • SHx: Accountant; smokes and drinks
occasionally; works out 5 times a week.
Case 2 (PE)
• Alert, moderate distress from pain on left arm. • HEENT; Neck; CV; Lungs; Abdomen all normal. • Left arm swollen and tender with prominence of
superficial venous circulation. • Pulses and sensation normal.
32
Case 2 (Dx tests)
• Labs: All normal.
• Doppler US LUE: Occlusive thrombus on axillary, brachial and basilic veins.
33
Q1: What is your next step?
1. Start anticoag immediately with a LMWH and Warfarin the same day.
2. Hypercoagulable panel. 3. No anticoagulation; arm
elevation and warm compresses + NSAIDs
4. Consult IR for venography and thrombolysis.
34
Startanticoagimm
ediat...
Hypercoagulablepanel.
Noanticoagulation;arm...
ConsultIRforvenograp..
0% 0%0%0%
:20
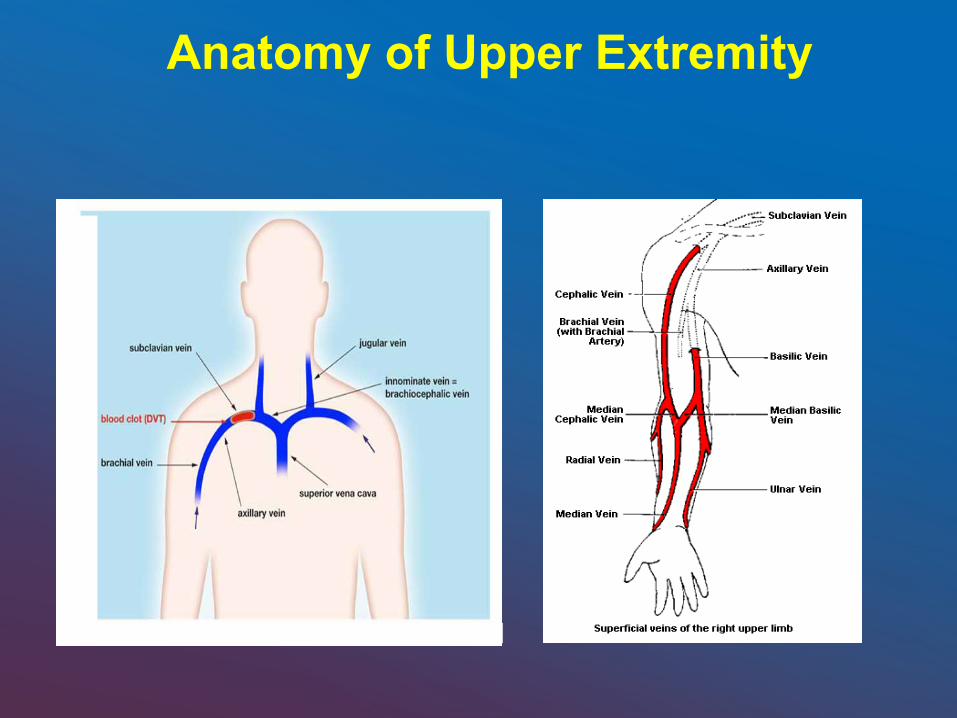
Anatomy of Upper Extremity
Types of UEDVT
• Primary Unprovoked or without thrombophilia-idiopathic Effort related– Paget-Schrötter syndrome Thoracic outlet syndrome (TOS) Incidence
- 2 per 100,000 person years - 30% of all UEDVTs
Flinterman LE. J Thromb Haemost. 2008;6:1262-1266
Paget-Schrötter Syndrome • Effort induced thrombosis
Rapid onset of DVT after strenuous activity Intimal microtrauma to vessel wall after exertion Activation of coagulation system
• Occurs in young, healthy adults; males more often than female
• Should be treated as an emergency • Considered venous manifestation of TOS
Flinterman LE. J Thromb Haemost. 2008;6:1262-1266
Thoracic Outlet Syndrome
• 3-10% of TOS cases related to vasculature; venous or arterial
• Compression of thoracic outlet veins by clavicle and first rib Rapid occlusion of vein Typically subclavian vein
• 60% of patients with primary UEDVT have the TOS
Watson HG. J Thromb Haemost. 2008;6:1267-1268

Treatment Recommendations- Paget-Schrötter Syndrome
• Course of action Venography Thrombolysis Anticoagulation Surgery
Flinterman LE. J Thromb Haemost. 2008;6:1262-1266
Treatment Recommendations- Paget-Schrötter Syndrome
• Surgery Lysis of adhesions around subclavian vein Resection of part of clavicle and/or first rib Scalene muscle resection Subclavian vein patching Bypass procedures
Flinterman LE. J Thromb Haemost. 2008;6:1262-1266
Case 3
• 52 y/o white man with h/o COPD admitted for exacerbation and IV antibiotics. Right upper extremity PICC placed due to poor IV access.
• On hospital day # 3, RUE swollen, red and tender.
• PE: VS normal; Pox 96% on RA ; Lungs with decrease breath sounds, no wheezing.
• Right arm is slightly swollen and tender. No erythema, good pulses.
• Doppler US: Occlusive clot on Axillary, brachial, basilic, and cephalic veins.
41
Q1: What is your next step? 1. Start anticoagulation
immediately with a LMWH and Warfarin the same day. Leave PICC in place.
2. Request a hypercoagulable panel.
3. Remove PICC. No anticoagulation; arm elevation and warm compresses
4. Consult IR for venography and thrombolysis
42
Startanticoagulationi...
Requestahypercoagulab..
RemovePICC.Noanticoa...
ConsultIRforvenograph...
25% 25%25%25%
:20
Types of UEDVT
• Secondary Provoked by central venous catheters Pacemakers Cancer IV drug abuse Coagulation abnormalities
- Protein C/S deficiency - Factor V Leiden gene mutation - Hyperhomocysteinemia - Antiphospholipid antibody syndrome
Flinterman LE. J Thromb Haemost. 2008;6:1262-1266
Malignancy
• Related to placement of CVCs 18 fold increase risk of developing UEDVT compared
to patients without active malignancy.
• Hypercoagulability of malignancy • Tumor mass compression • Comprises 24% of UEDVT cases • Types
Lymphoma Lung cancer
Flinterman LE. J Thromb Haemost. 2008;6:1262-1266
Diagnosis
• Doppler Ultrasound Disadvantages
- False negative - Clavicle may shadow segment of subclavian vein
Use venography if Doppler is negative and strong clinical suspicion of UEDVT
Gaffar M. Hospital Physician. 2005:29-34
Diagnosis
• Venography Gold standard Contrast dye injected into basilic vein Defects in intraluminal filling indicate thrombus Limited use due to complications and invasive nature
Gaffar M. Hospital Physician. 2005:29-34
Diagnosis
• Magnetic Resonance Angiography Higher resolution imaging of thoracic veins compared
to Doppler Blood flow information and collateral vessel
visualization better Strong correlation to results of venography
- Is noninvasive and accurate - May use if venography is contraindicated
Gaffar M. Hospital Physician. 2005:29-34
Differential Diagnosis
• Hematomas • Muscle contusions or tears • Cellulitis • Lymphedema • Gangrene • All may present with pain and swelling in upper
extremity
Gaffar M. Hospital Physician. 2005:29-34
Complications
• Pulmonary embolism Occurs in up to 30% of patients Occurs more frequently if CVC in place Less common than in patients with LEDVT
Gaffar M. Hospital Physician. 2005:29-34
Complications
• Post thrombotic syndrome Occurs in up to 40% of patients Results from chronic venous insufficiency from clot Characteristics
- Edema - Pain - Venous ulcers - Skin pigmentation changes
Treatment/prevention
Gaffar M. Hospital Physician. 2005:29-34
Treatment Recommendations
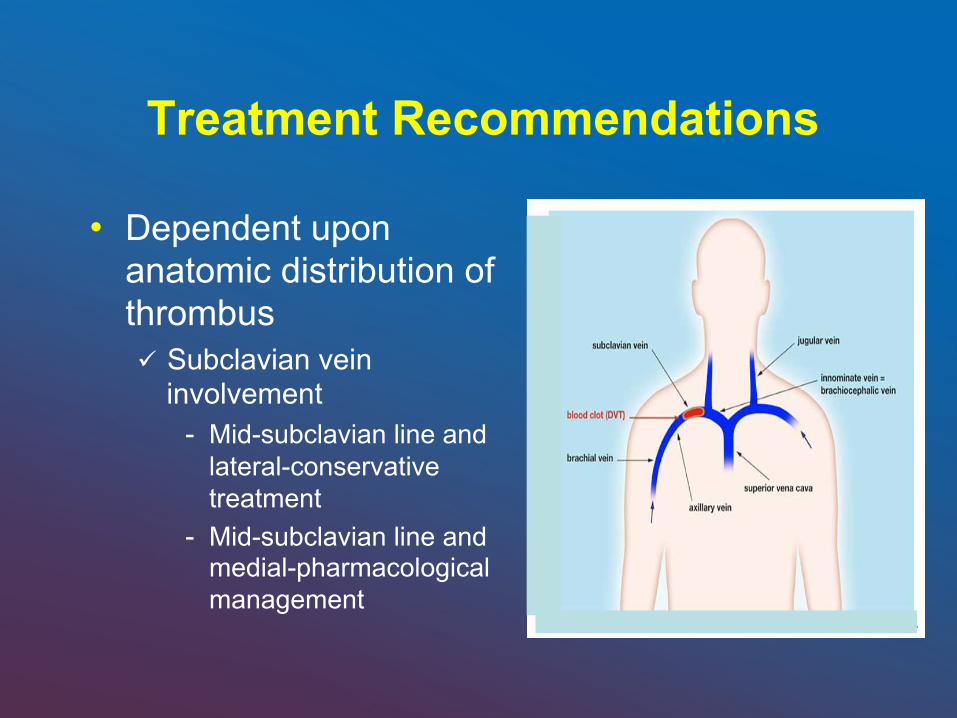
• Dependent upon anatomic distribution of thrombus Subclavian vein
involvement - Mid-subclavian line and
lateral-conservative treatment
- Mid-subclavian line and medial-pharmacological management
Treatment Recommendations-Lateral to Mid-Subclavian Line
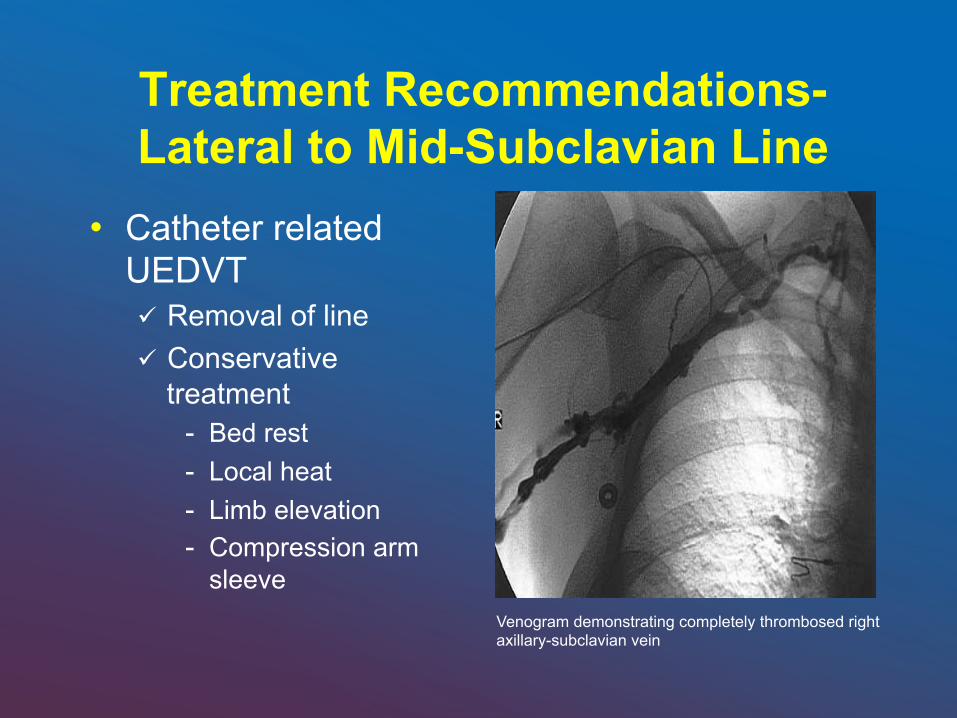
• Catheter related UEDVT Removal of line Conservative
treatment - Bed rest - Local heat - Limb elevation - Compression arm
sleeve Venogram demonstrating completely thrombosed right axillary-subclavian vein
Treatment Recommendations-Lateral to Mid-Subclavian Line
• Catheter related UEDVT Removal of line not possible
- Anticoagulate patient for duration of line involvement - Repeat imaging after line removed
Treatment Recommendations-Medial to Mid-Subclavian Line
• Catheter Related UEDVT Removal of line if possible
- Anticoagulate for total of 12 weeks Removal of line not possible
- Anticoagulate patient for duration of line involvement - Begin 12 weeks of anticoagulation once line is removed
Case 4
• 73 year old man scheduled for elective right total knee replacement surgery
• History of Hypertension and DM type 2 • Creatinine clearance: 35 ml/min • BMI 35 • Med: metoprolol 50mg, HCTZ 12.5 mg, Lantus 10
55
Q1: What VTE prophylaxis would you recommend?
1. LMWH S/Q 2. Heparin (UFH): 5,000 U
S/Q Q8hs 3. Heparin (UFH): 5,000 U
S/Q Q12 4. Fondaparinux 2.5 mg. S/
Q daily. 5. Dabigatran 75 mg PO
every 12 hs 6. Rivaroxaban 10 mg PO
daily 7. ASA 325 mg. PO daily
56
LMWH
S/Q
Heparin(UFH):5,000US..
Heparin(UFH):5,000US..
Fondaparinux2.5mg.S/...
Dabigatran75mgPOeve..
Rivaroxaban10m
gPOdaily
ASA325mg.POdaily
14% 14% 14%14%14%14%14%
:25
Q8hr dosing schedule 0700 1500 2300
Methods • Compare:
Patients that were prescribed Enoxaparin once daily to Patients that were prescribed with UFH twice daily or three times daily.
• Patients enrolled were required to have a hospitalization period > 4 days. • Followed patients for the duration of their hospitalization. • Adherence = Number of Doses Administered Number of doses Scheduled for Administration • We identified all doses that were omitted or late. • We measure the time interval between:
Successive administered doses Time interval between scheduled administration time and dose administration
time.
Fanikos, J. et.al AmJMed Volume 123, Issue 6 , Pages 536-541, June 2010
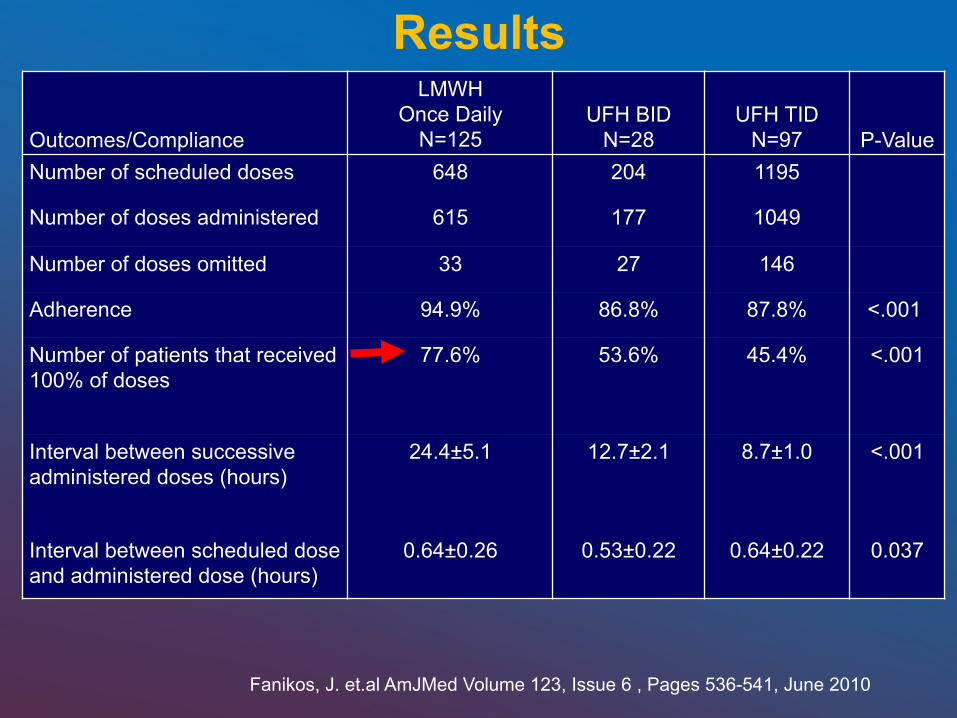
Results
Outcomes/Compliance
LMWH Once Daily
N=125 UFH BID
N=28 UFH TID
N=97 P-Value Number of scheduled doses 648 204 1195
Number of doses administered 615 177 1049
Number of doses omitted 33 27 146
Adherence 94.9% 86.8% 87.8% <.001
Number of patients that received 100% of doses
77.6% 53.6% 45.4% <.001
Interval between successive administered doses (hours)
24.4±5.1 12.7±2.1 8.7±1.0 <.001
Interval between scheduled dose and administered dose (hours)
0.64±0.26 0.53±0.22 0.64±0.22 0.037
Fanikos, J. et.al AmJMed Volume 123, Issue 6 , Pages 536-541, June 2010
Prevention of VTE in surgical patients What´s new in the 2012 9th ACCP guidelines?
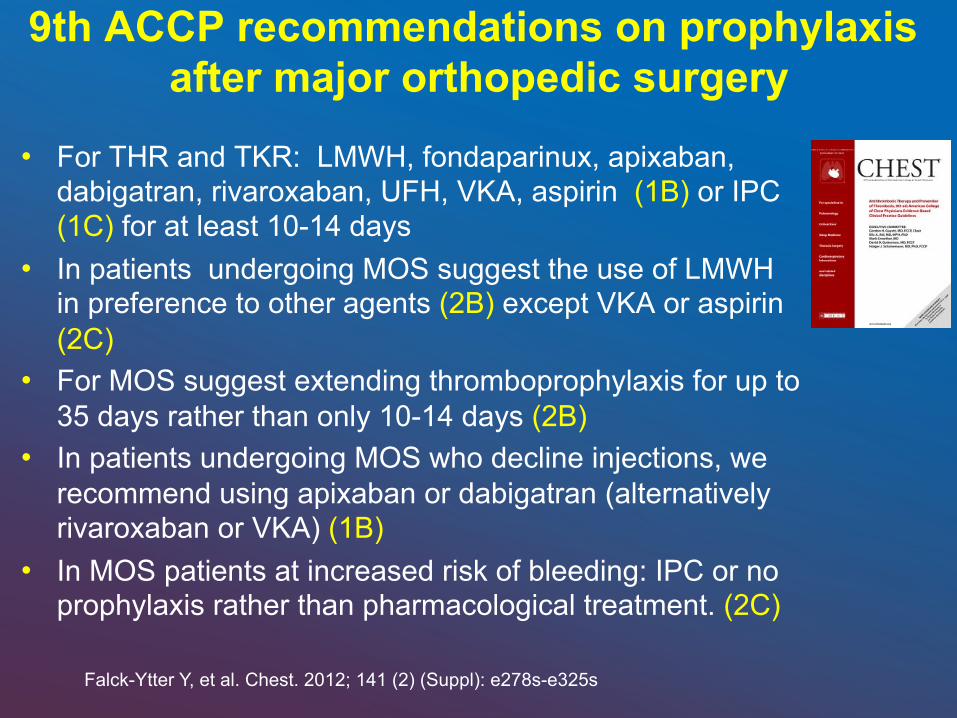
9th ACCP recommendations on prophylaxis after major orthopedic surgery
• For THR and TKR: LMWH, fondaparinux, apixaban, dabigatran, rivaroxaban, UFH, VKA, aspirin (1B) or IPC (1C) for at least 10-14 days
• In patients undergoing MOS suggest the use of LMWH in preference to other agents (2B) except VKA or aspirin (2C)
• For MOS suggest extending thromboprophylaxis for up to 35 days rather than only 10-14 days (2B)
• In patients undergoing MOS who decline injections, we recommend using apixaban or dabigatran (alternatively rivaroxaban or VKA) (1B)
• In MOS patients at increased risk of bleeding: IPC or no prophylaxis rather than pharmacological treatment. (2C)
Falck-Ytter Y, et al. Chest. 2012; 141 (2) (Suppl): e278s-e325s
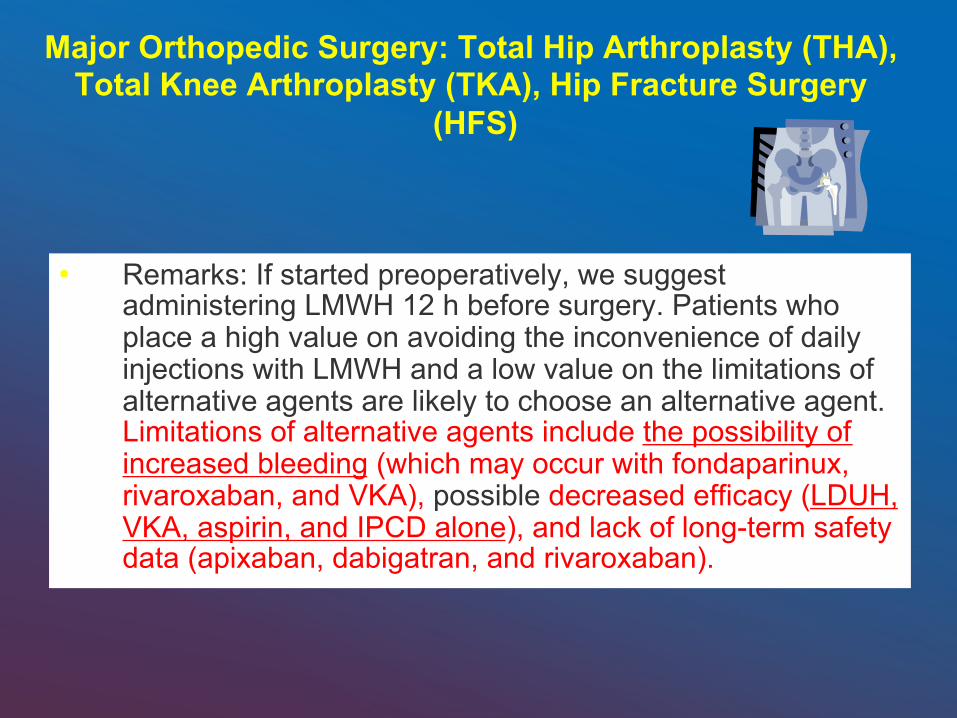
• Remarks: If started preoperatively, we suggest administering LMWH 12 h before surgery. Patients who place a high value on avoiding the inconvenience of daily injections with LMWH and a low value on the limitations of alternative agents are likely to choose an alternative agent. Limitations of alternative agents include the possibility of increased bleeding (which may occur with fondaparinux, rivaroxaban, and VKA), possible decreased efficacy (LDUH, VKA, aspirin, and IPCD alone), and lack of long-term safety data (apixaban, dabigatran, and rivaroxaban).
Major Orthopedic Surgery: Total Hip Arthroplasty (THA), Total Knee Arthroplasty (TKA), Hip Fracture Surgery
(HFS)
Bleeding and anti-coagulation: to what extent?
The decision to prophylax: The balance of benefits and harms
• Major orthopedic surgery patients are at high-risk for post-operative venous thromboembolism (VTE)1
• Risk of major bleeding associated with pharmacological prophylaxis is a concern for orthopedic surgeons2,3
1. Geerts WH, et al. Chest 2008;133:381-453. 2. Schulman S, et al. Chest. 2008;133:257S-298S.
3. Ng JH, Crowther MA. Semin Hematol. 2006;43:S77-S83.
Symptomatic thromboembolic
events
Bleeding
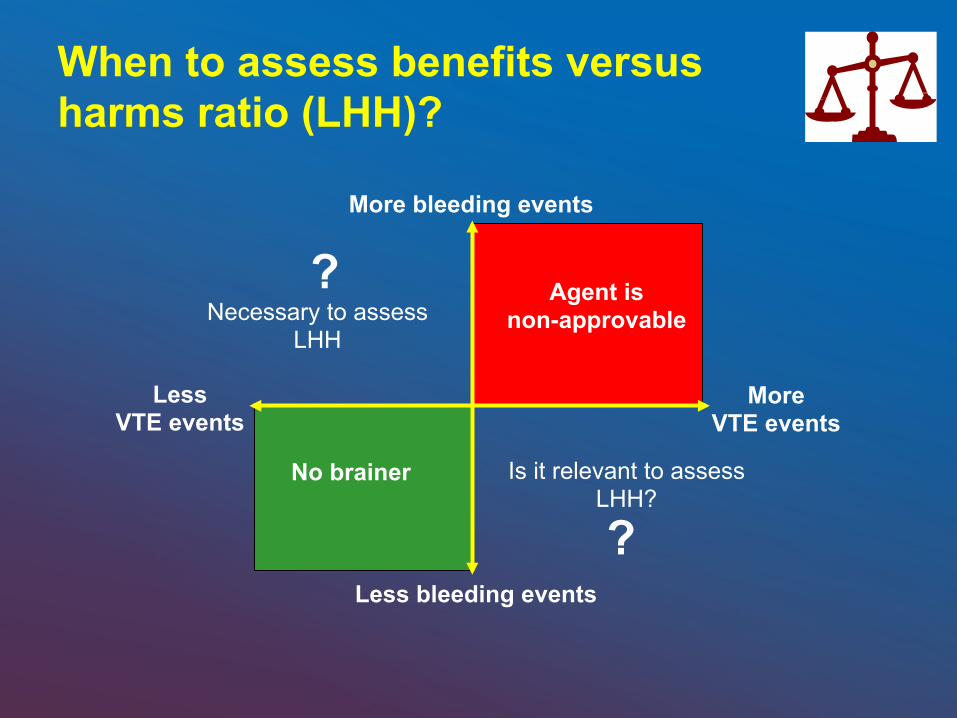
More VTE events
Less VTE events
More bleeding events
Less bleeding events
Agent is non-approvable Necessary to assess
LHH
No brainer Is it relevant to assess LHH?
When to assess benefits versus harms ratio (LHH)?
?
?
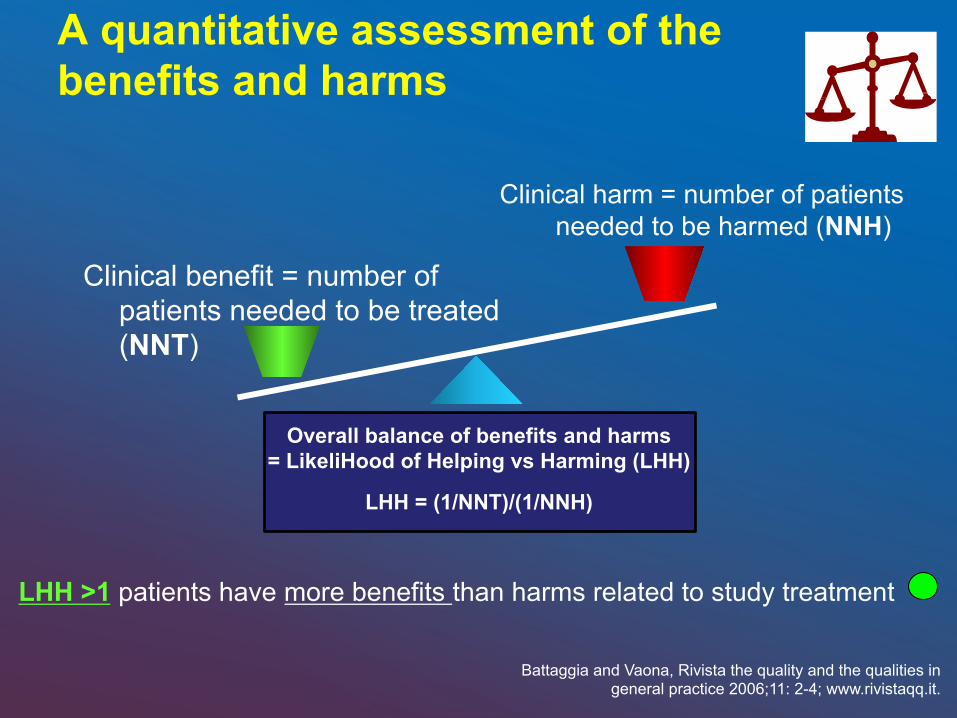
A quantitative assessment of the benefits and harms
Clinical benefit = number of patients needed to be treated (NNT)
Clinical harm = number of patients needed to be harmed (NNH)
LHH >1 patients have more benefits than harms related to study treatment
Battaggia and Vaona, Rivista the quality and the qualities in general practice 2006;11: 2-4; www.rivistaqq.it.
Overall balance of benefits and harms = LikeliHood of Helping vs Harming (LHH)
LHH = (1/NNT)/(1/NNH)
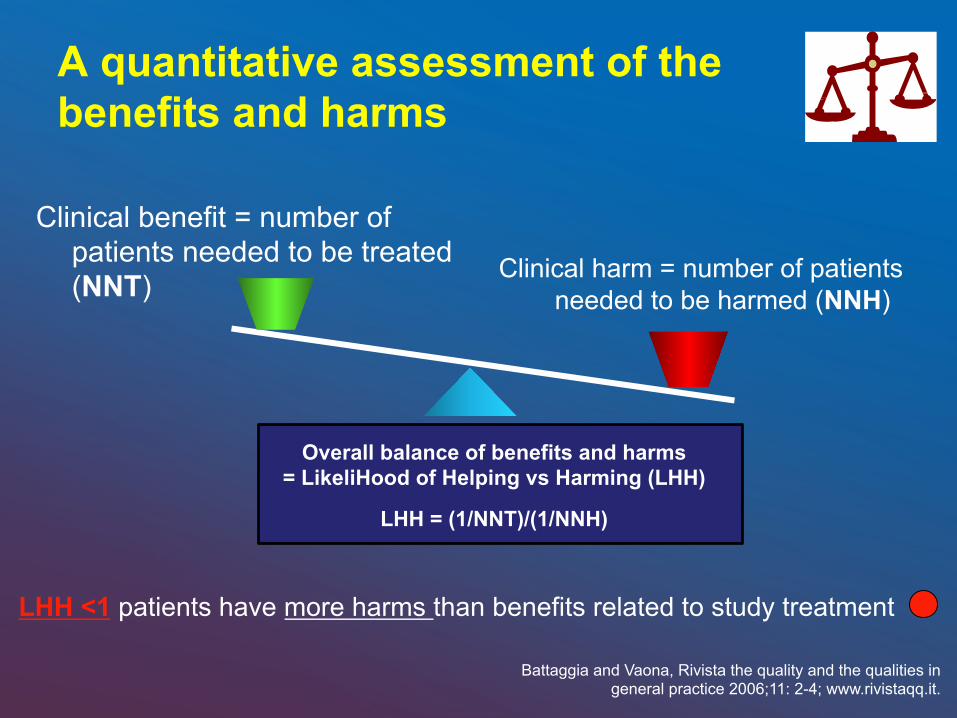
A quantitative assessment of the benefits and harms
Clinical benefit = number of patients needed to be treated (NNT) Clinical harm = number of patients
needed to be harmed (NNH)
LHH <1 patients have more harms than benefits related to study treatment
Battaggia and Vaona, Rivista the quality and the qualities in general practice 2006;11: 2-4; www.rivistaqq.it.
Overall balance of benefits and harms = LikeliHood of Helping vs Harming (LHH)
LHH = (1/NNT)/(1/NNH)
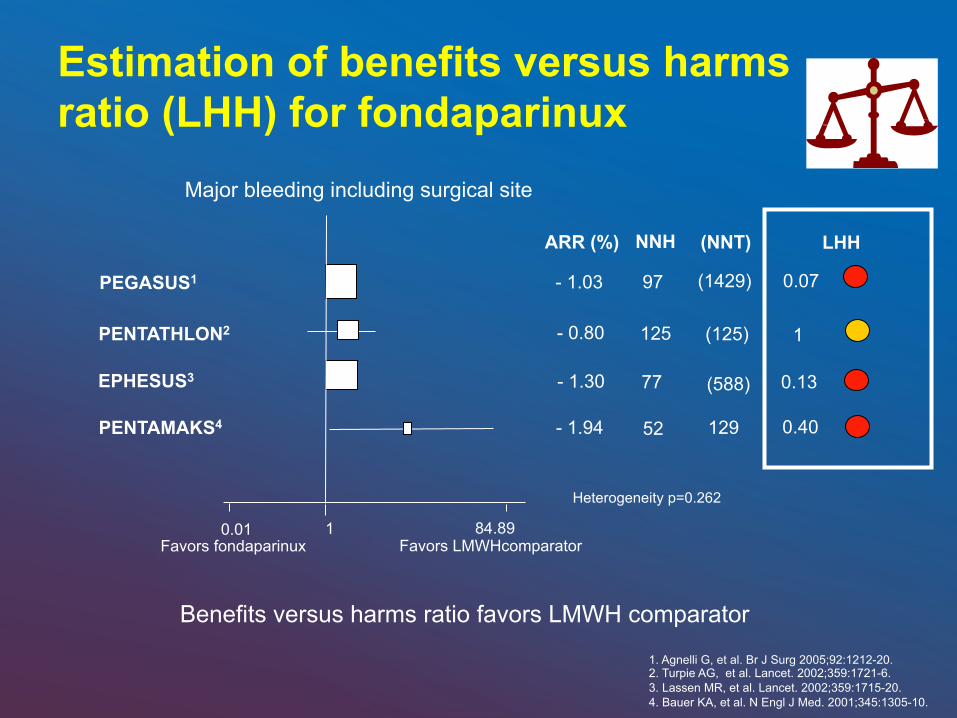
Estimation of benefits versus harms ratio (LHH) for fondaparinux
PEGASUS1
PENTATHLON2
EPHESUS3
PENTAMAKS4
NNH
97
125
Heterogeneity p=0.262
52
ARR (%)
- 1.03
- 0.80
- 1.30 77
- 1.94
Favors LMWHcomparator Favors fondaparinux
1. Agnelli G, et al. Br J Surg 2005;92:1212-20. 2. Turpie AG, et al. Lancet. 2002;359:1721-6. 3. Lassen MR, et al. Lancet. 2002;359:1715-20. 4. Bauer KA, et al. N Engl J Med. 2001;345:1305-10.
Major bleeding including surgical site
0.01 1 84.89
Benefits versus harms ratio favors LMWH comparator
(NNT)
(1429)
(125)
129
(588)
0.07
1
0.40
0.13
LHH
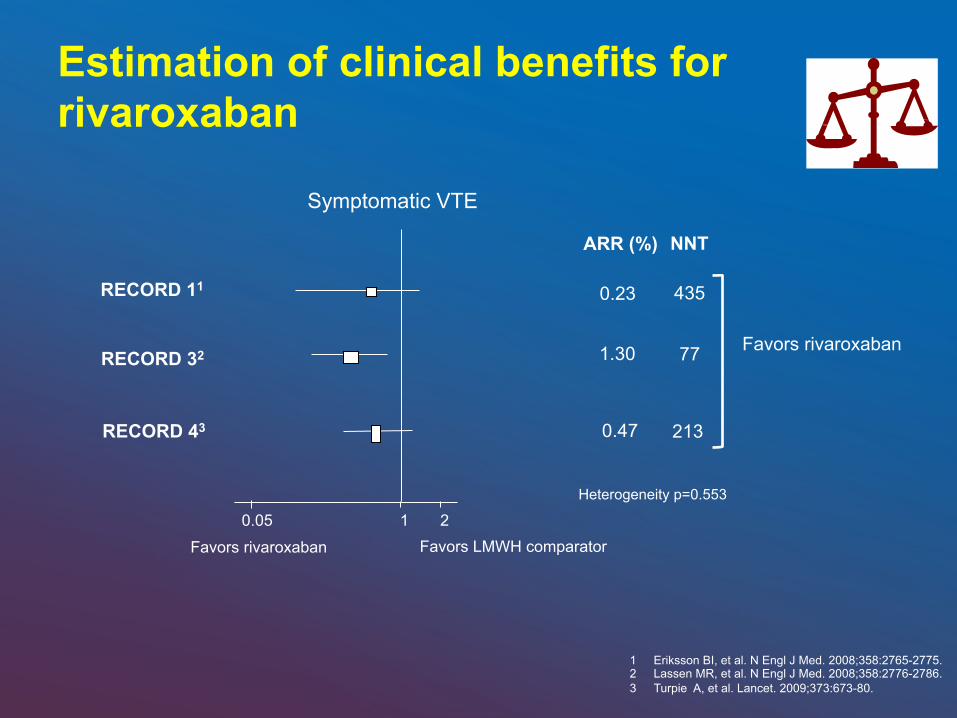
Estimation of clinical benefits for rivaroxaban
RECORD 11
RECORD 32
RECORD 43
NNT
435
77
213
Symptomatic VTE
Favors rivaroxaban
Favors rivaroxaban Favors LMWH comparator
Heterogeneity p=0.553
1 Eriksson BI, et al. N Engl J Med. 2008;358:2765-2775. 2 Lassen MR, et al. N Engl J Med. 2008;358:2776-2786. 3 Turpie A, et al. Lancet. 2009;373:673-80.
ARR (%)
0.23
1.30
0.47
1 2 0.05
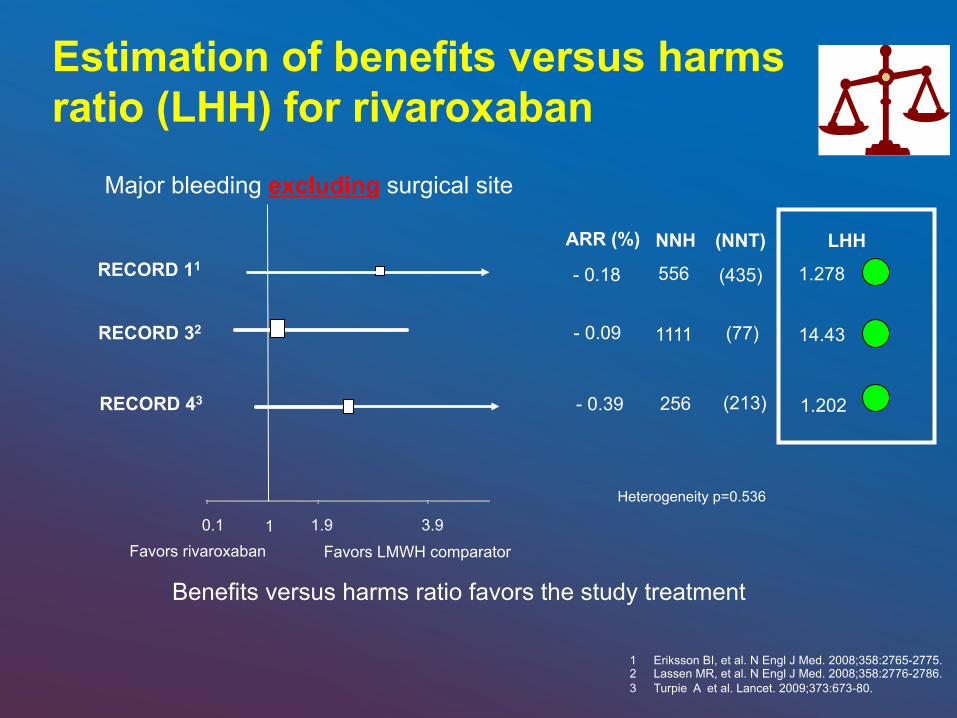
Estimation of benefits versus harms ratio (LHH) for rivaroxaban
0.1 1.9 3.9 1
RECORD 11
RECORD 32
RECORD 43
ARR (%)
- 0.18
- 0.09
- 0.39
NNH
556
256
1111
Heterogeneity p=0.536
Major bleeding excluding surgical site
Favors LMWH comparator Favors rivaroxaban
1 Eriksson BI, et al. N Engl J Med. 2008;358:2765-2775. 2 Lassen MR, et al. N Engl J Med. 2008;358:2776-2786. 3 Turpie A et al. Lancet. 2009;373:673-80.
Benefits versus harms ratio favors the study treatment
(NNT)
(435)
(77)
(213)
LHH
1.278
1.202
14.43
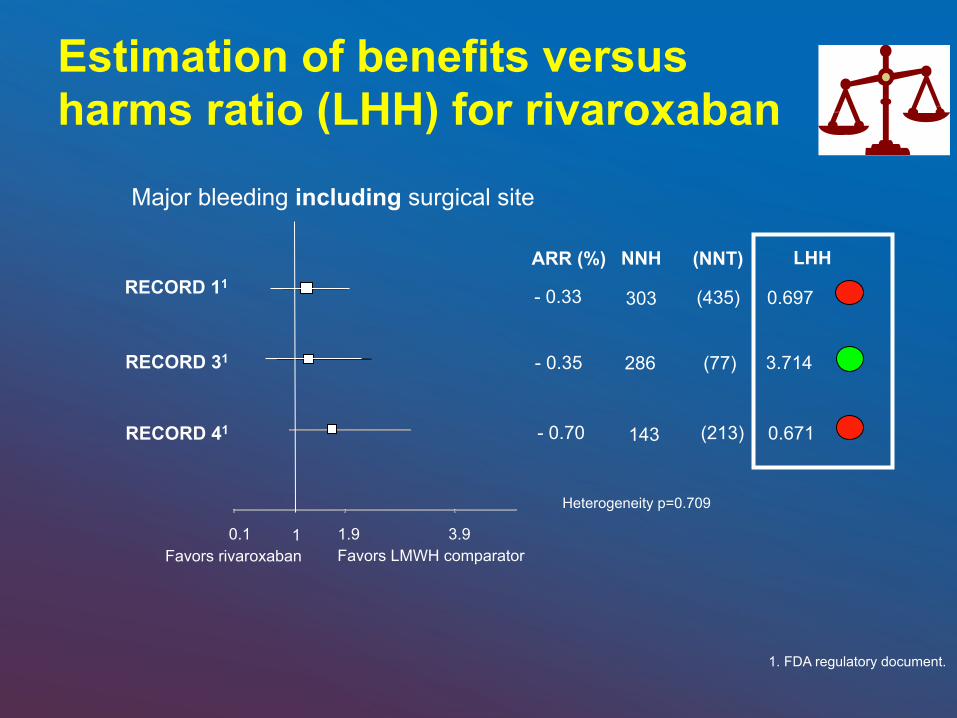
0.1 1.9 3.9 1
RECORD 11
RECORD 31
RECORD 41
Major bleeding including surgical site
Favors LMWH comparator Favors rivaroxaban
Estimation of benefits versus harms ratio (LHH) for rivaroxaban
1. FDA regulatory document.
ARR (%)
- 0.33
- 0.35
- 0.70
NNH
Heterogeneity p=0.709
303
286
143
(NNT)
(435)
(77)
(213)
LHH
0.697
3.714
0.671
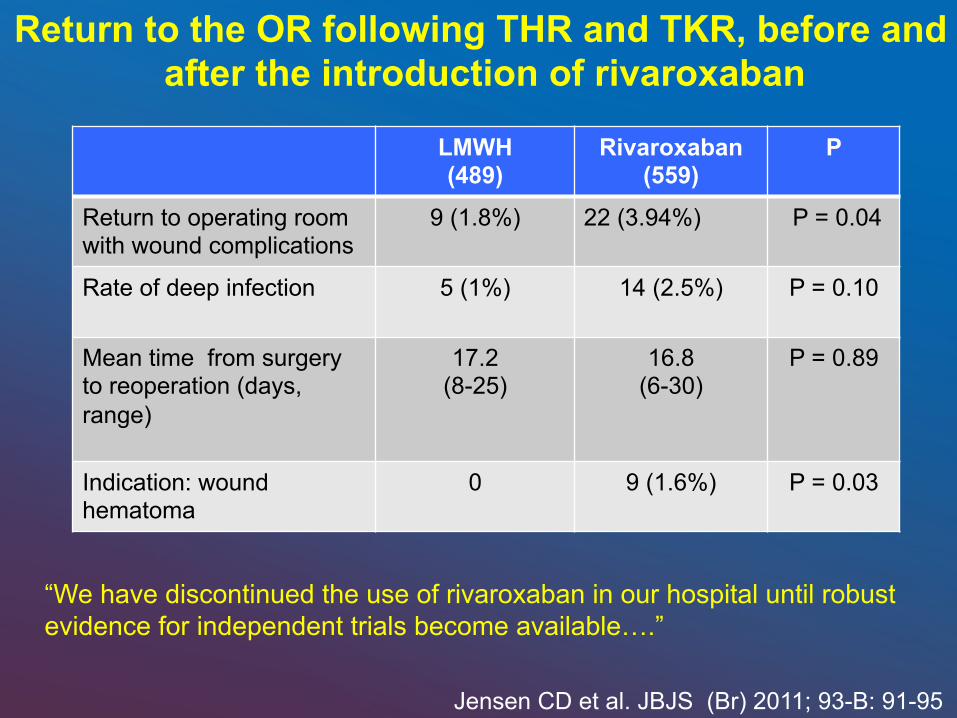
LMWH (489)
Rivaroxaban (559)
P
Return to operating room with wound complications
9 (1.8%) 22 (3.94%) P = 0.04
Rate of deep infection 5 (1%) 14 (2.5%) P = 0.10
Mean time from surgery to reoperation (days, range)
17.2 (8-25)
16.8 (6-30)
P = 0.89
Indication: wound hematoma
0 9 (1.6%) P = 0.03
Return to the OR following THR and TKR, before and after the introduction of rivaroxaban
Jensen CD et al. JBJS (Br) 2011; 93-B: 91-95
“We have discontinued the use of rivaroxaban in our hospital until robust evidence for independent trials become available….”
1. Ansell J et al. Chest. 2004;126:204S-233S. 2. Hirsh J et al. J Am Coll Cardiol. 2003;41:1633-1652. 3. Rothberg MB et al. Ann Intern Med. 2005;143:241-250.
Balancing Risks and Benefits of Prophylactic Anticoagulation Therapy
Q2: For how long?
1. Until discharge from hospital
2. 10 – 14 days. 3. 28 – 35 days. 4. Until ambulation is
achieved.
75
Untildischargefrom
hosp...
10–14days.
28–35days.
Untilambulationisachi...
25% 25%25%25%
:20
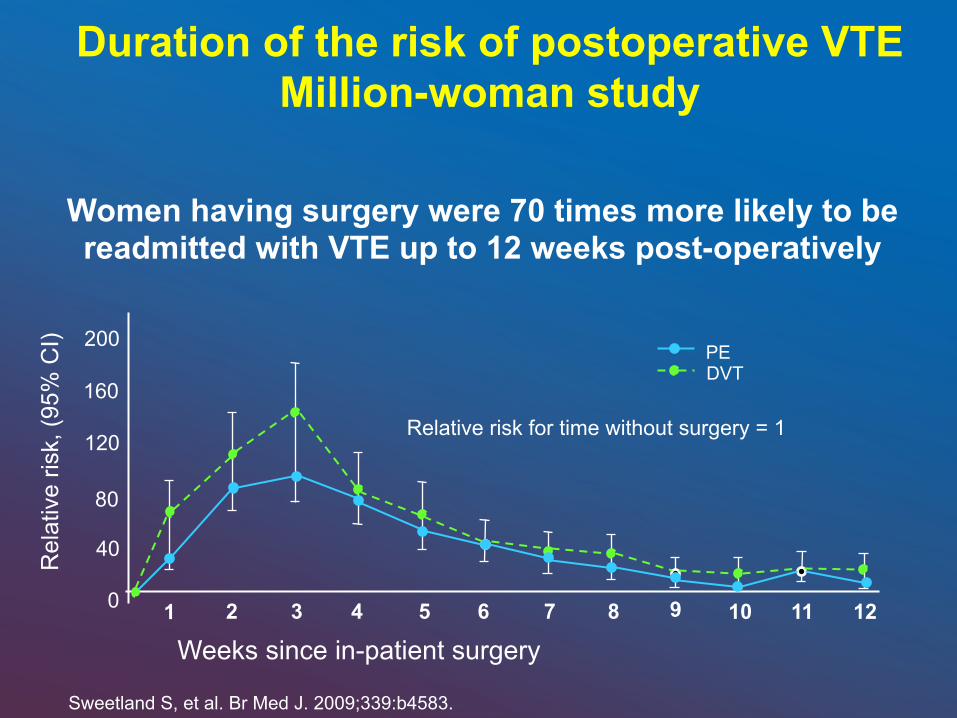
Duration of the risk of postoperative VTE Million-woman study
Sweetland S, et al. Br Med J. 2009;339:b4583.
Rel
ativ
e ris
k, (9
5% C
I)
1 2 3 4 5 6 7 0 8 9 10
40
80
120
160
200
11 12
Weeks since in-patient surgery
PE DVT
Relative risk for time without surgery = 1
Women having surgery were 70 times more likely to be readmitted with VTE up to 12 weeks post-operatively
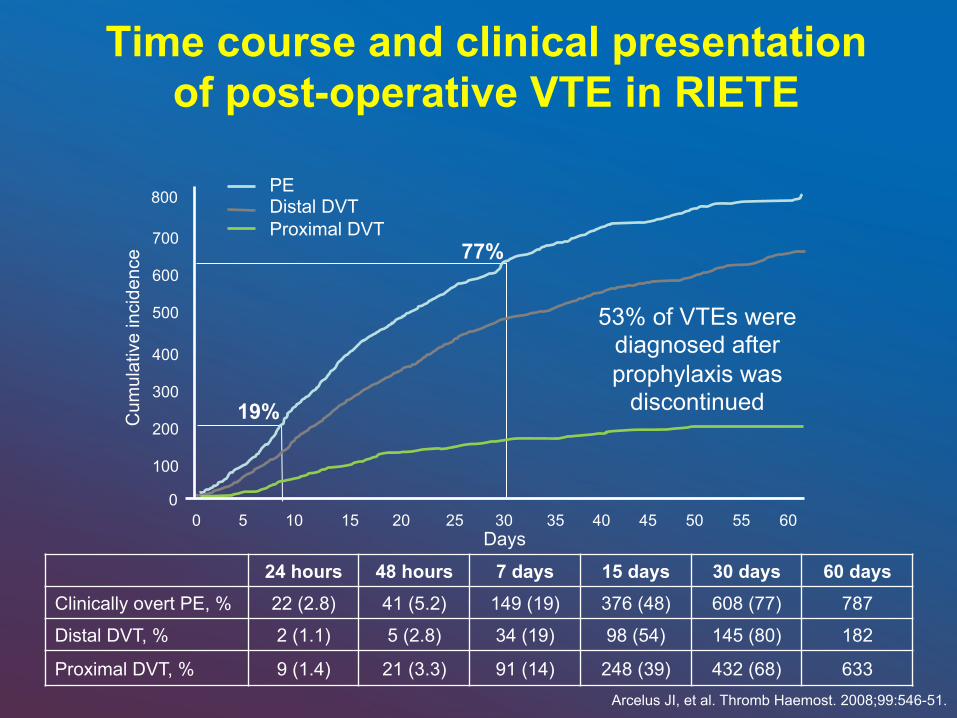
Time course and clinical presentation of post-operative VTE in RIETE
Arcelus JI, et al. Thromb Haemost. 2008;99:546-51.
19%
77%
53% of VTEs were diagnosed after prophylaxis was
discontinued
PE Distal DVT Proximal DVT
24 hours 48 hours 7 days 15 days 30 days 60 days Clinically overt PE, % 22 (2.8) 41 (5.2) 149 (19) 376 (48) 608 (77) 787
Distal DVT, % 2 (1.1) 5 (2.8) 34 (19) 98 (54) 145 (80) 182
Proximal DVT, % 9 (1.4) 21 (3.3) 91 (14) 248 (39) 432 (68) 633
Days
Cum
ulat
ive
inci
denc
e
5 10 15 20 25 30 35 40 0
45 50 55 60 0
100
200
300
400
500
600
700
800
• For patients undergoing major orthopedic surgery, we suggest extending thromboprophylaxis in the outpatient period for up to 35 days from the day of surgery rather than for only 10 to 14 days (Grade 2B)
Major Orthopedic Surgery: Total Hip Arthroplasty (THA), Total Knee Arthroplasty (TKA), Hip Fracture Surgery
(HFS)
Back to the Basics
79
Treatment DVT LMWH Vs UFH Meta-analyses
• Authors Leizorovicz et al ‘94 Lensing et al ‘95 Siragusa et al ‘96 Gould et al ‘99 Dolovich et al ’00 van den Belt ‘00
• Outcomes More or as effective < Major bleeding < Thrombocytopenia
Concerns With LMWH Use
• Obesity • Renal insufficiency • Pregnancy • Adverse effects
osteoporosis HIT
HIT = heparin-induced thrombocytopenia
UFH
• Therapeutic levels -- First 24 hours. • Otherwise, risk of recurrent VTE -- 15 X
Hull, et al. NEJM 1986; 315, 1109-13 Brandjes DPM et al. NEJM 1992; 327, 1485-90

Treat for at least 5 days with UFH or LMWH, overlapping
oral anticoagulation

Duration of Treatment
General Aspects
• Short-term treatment associated with 15-50% frequency of extension of thrombus or recurrent disease.
• Minimum duration 3 months. • Treatment with VKA is the preferred approach
for long-term treatment.
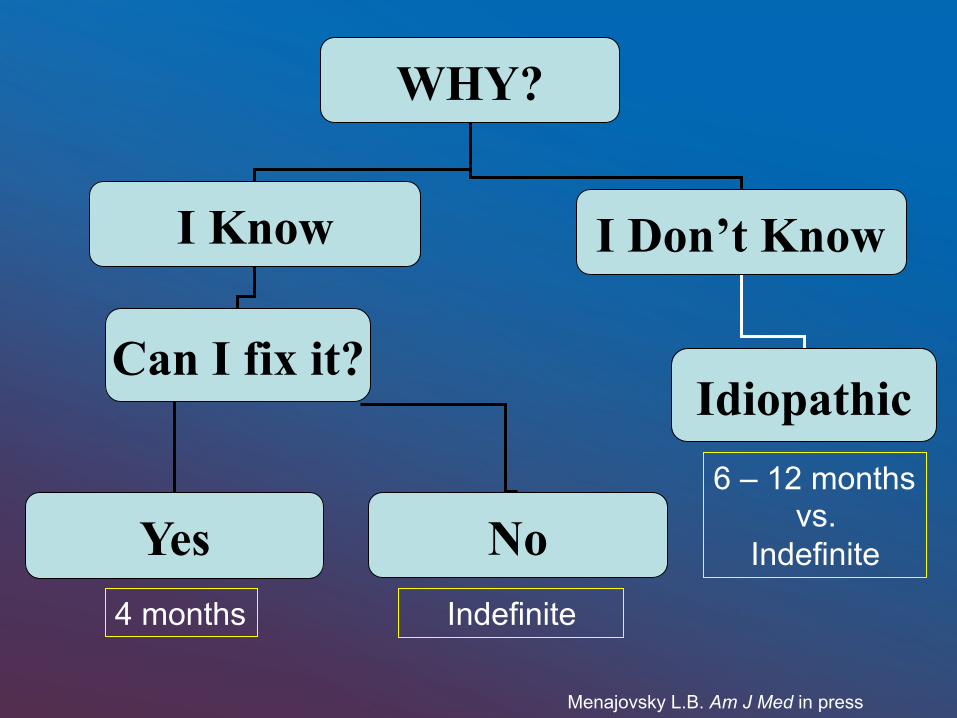
WHY?
I Know I Don’t Know
Can I fix it?
Yes No
Idiopathic
4 months Indefinite
6 – 12 months vs.
Indefinite
Menajovsky L.B. Am J Med in press
Conclusions
• Treat acutely with Heparin or LMWH • Advantages of LMWH • Either way: Treat for at least 5 days,
overlapping oral anticoagulation • Thrombolytic therapy and
Thrombectomy for selected patients • Careful discharge planning
Consequences of VTE
• Recurrent VTE • Post-thrombotic syndrome (PTS)1
Presence of leg symptoms (pain, cramps, heaviness, pruritus, and paresthesia) and signs (pretibial edema, skin induration, hyperpigmentation, new venous ectasia, redness and pain during calf compression)
• Mortality2
1. Prandoni P et al. Haematologica. 1997;82:423-428. 2. Pengo V et al. N Engl J Med. 2004;350:2257-2264.




Thank you!
Recommended