Preventing Surgical Site Infections in the Diabetic Cardiac Surgical Patient
Paula Pintar BSN, RN
Alverno College – MSN Student
Tutorial Project Spring 2010

Navigation of Tutorial
This button will return you to the Tutorial menu screen.
This button will return you to the previous slide.
This button will advance you to the next slide.
Click on any underlined word for additional information
Tutorial MenuLearning
Objectives
Tying It AllTogether
Surgical Site Infection
What is it?
Why are SurgicalSite Infections a
Problem?
SignificanceOf
Diabetes Mellitus
Stages of SurgicalWound Healing
Age & Wound Healing
Inflammation &
Wound Healing
Genetics&
Wound Healing
Key Risks With
Wound Healing
Activation of Stress Response
And Surgery
Case StudyPart 2
“Bundle”Elements &
Nsg. Interventions
Best PracticeStandards“Bundle”
Case StudyPart 1
References
Click on the button you would like to view more information about.

Learning Objectives
The Learner Will: Identify criteria used for classifying a surgical site infection (SSI). Identify why Surgical Site infections are a problem. Review of Diabetes Mellitus and the genetic link of incidence. Identify what risk factors can put Diabetic patients at a higher risk to
developing a Surgical Site infection. Review the three main stages of wound healing: Inflammation, Proliferation,
Remodeling. Be able to correlate the factors of Age, Inflammation, and the Generalized
Stress Response in the diabetic patient; relate how these factors impact the stages of wound healing.
Review Best Practice Standards and Nursing interventions for a Surgical Site infection prevention plan.
Apply Nursing indicators to a case study. Understand how applying “best practice guidelines” will support positive
outcomes for the patient, family, staff, health system, and community.

Surgical Site Infection (SSI)What Is It? Clinical and laboratory signs of infection at the surgical site
within: 30 days of the surgery or Within 1 year if an implant was used (heart valve/joint) Criteria for Defining a Surgical Site Infection (SSI)
Documented at various tissue levels: Superficial (skin/subcutaneous) Deep (soft tissue/muscle) Deep/organ space (organ space)
Caused by: Endogenous bacteria – patients’ own skin flora Exogenous bacteria – environmental bacteria or surgical
material Source: 1
SSI As Defined by the CDC
Superficial Infection within 30 days after procedure Involves the skin and subcutaneous tissue (and meets one of the following
criteria) Has purulent drainage Organisms cultured from fluid or tissue Displays at least 1 of the following pain, local swelling, redness, and
incision is opened by surgeon Diagnosis of superficial incision SSI by the surgeon or attending MD
Source:1
SSI As Defined by the CDC Deep Incisional SSI
Occurs within 30 days of procedure 1 year if implant Involves deep soft tissue ( fascial and muscle layers)
And patient displays at least one of the following Purulent drainage Spontaneously dehisces or opened by the surgeon and the
patient has at least one of the following: Fever, pain, abscess, or diagnosis by MD
Source: 1
SSI As Defined by the CDC Organ space
Occurs with in 30 days 1 year if implant used Includes any part of the body excluding skin, fascia, or muscle layer.
Must meet the following criteria Purulent drainage from a drain that is place through a stab
wound Isolated organisms from an aseptic culture Abscess Diagnosis by MD
Source: 1

Lets Review What are the 3 tissue levels of a Surgical Site
Infection?
Primary Scar
Organ Space
Deep
Superficial
Acute

Surgical Site InfectionWhy Is It A Problem?
According to the Institute for Healthcare Improvement (IHI) 38% of all Healthcare Associated Infections are SSI’s 2 – 5% of patients operated on will develop an SSI Developing an SSI will extend the hospital stay by 5 to 7 days One SSI will increase cost by $2,734 - $26,019 (estimated on 1985
dollars) Estimated national costs of 130 million to 845 million dollars spent a year
on SSI’s.
Source: 1
What Does this Mean at a Local Level?
Higher cost related to longer stays Decreased patient turnover translates into less income for healthcare facility Healthcare facility develops a reputation of poor patient outcomes. Decreased reimbursement by The Centers for Medicare and Medicaid
(CMS) as of October 1, 2008 stopped reimbursement for hospital acquired infections
Source: 16
Microsoft clipart
What Does this Mean at a Local Level? Negative Outcomes Linked to SSI’s Trend is toward public reporting of infection rates for healthcare
facilities. This will impact consumer decisions as to where they will go to have
procedures performed. Consumers have greater access to information - Intranet Milwaukee has number of facilities with duplicative resources. Patients
may begin shopping around for facility with lowest infection rates.
Source: 16Microsoft Clipart

Lets Review According to the Institute for Healthcare Improvement
(IHI) 38% of all Healthcare Associated Infections are SSI’s.
Developing an SSI will extend the hospital stay by 5 to 7 days.
Increased reimbursement by The Centers for Medicare and Medicaid (CMS) as of October 1, 2008 started for hospital acquired infections.
Trend is toward public reporting of infection rates for healthcare facilities.
True False
True False
True False
True False

Now With The Problem Identified…
Lets take a closer look at a patient population (diabetes mellitus), and apply nursing indicators and medical knowledge to decrease and prevent the development of Surgical Site Infections.
Microsoft Clipart
Significance of Diabetes Mellitus
Diabetes mellitus affects approximately 2.8 million people in the United States
The disease is a metabolic process that results from a lack of insulin secretion or action.
Insulin is a hormone that is secreted by the beta cells in the pancreas.
This hormone then allows the cells in our body to absorb the glucose and convert it into energy to maintain metabolic processes.
There are two main types of diabetes mellitus that the majority of diabetics are classified into.
Microsoft Clipart
Source: 6

Diabetes Mellitus & Genetic Link
Type 1: This is characterized by an complete lack of insulin
secretion and elevated blood sugar, related to destroyed pancreatic beta cells (6)
Usually occurs at an early age (childhood) 5 to 10% of the diabetic population have this type
of diabetes (~ 1 million people) (6)
These individuals have been associated with an autoimmune link to the disease. (4)
This autoimmune response is the cause of beta cell destruction (4)
The other factor identified is an exposure to an environmental mediator, such as having an infection. (6)
Microsoft Clipart
Source: 4, 6
Diabetes Mellitus & Age Link
Type 2 : This is characterized by having insulin resistance Approximately 90 to 95% of diabetics present with this
type (~19 million people) 18 -20% of persons 65 and older have diabetes 40% have the disease or precursor to disease Obesity and older individuals is commonly associated
with Type 2 There is multiple hypothesis as to the causal agents of
this form. Due to the variability of the causal agents, it is difficult
to predict or identify specific factors that lead to disease. It is known that autoimmune destruction of the beta cells,
as in Type 1 does not occur.
Microsoft Clipart
Source: 6

Diabetes Mellitus & Link to Developing an SSI
Studies correlating elevated levels of hemoglobin A1C 6.5 (HgA1C) and uncontrolled blood sugars in the postoperative period have had a higher incidence of postoperative wound infections. Blood glucose levels >200mg/dL in immediate postoperative period
and up to 48 hours post operatively are a key link to SSI development.
Phagocyte activity is altered by the elevated blood glucose levels.
Source: 6

Lets Review What is the key reference data used to
monitor blood sugar stability over time?
Correct In Correct
Hgb A1C
Blood pressure
Urine glucose
Amylase
Finger stick glucose
C reactive protein
K level

Review of the Surgical Wound Healing Process
There are 3 main stages of wound healing 1. Inflammation 2. Proliferation 3. Remodeling
Within each stage there is a complex system of cellular functions that occur. (5)
Factors that can impede good wound healing are: Poor diet/uncontrolled blood sugars Compromised blood flow Disruption of inflammatory response Infection Effects of age (14)
Microsoft Clipart
Source: 5,14
Surgical Wound Healing Stages
Stage 1 Inflammatory (acute) Incision – initial vasoconstriction followed by platelet
aggregation to damaged endothelium (14)
Followed by a dilation of capillaries Around 24 hours macrophages enter the area and remain
there to clean up cellular debris and stimulate the healing process (5)
Microsoft Clipart
Source: 5,15

Surgical Wound Healing Stages
Stage 2 – Proliferation 24-48 hours after wound occurrence the
fibroblast and vascular endothelial cells begin formation (5)
This is a fragile period for the wound due to new capillary growth (14)
Then formation of new dermal layers begins (14)
Microsoft ClipartMicrosoft Clipart
Source: 5,15
Review of Surgical Wound
Stage 3 – Remodeling Occurs post wound by about week 3 Formation of a scar develops During this process the healing wound experiences a
decrease in vascularization with the continuing development of scar tissue.
Source: 14

Lets Review
Click on stage definition
Debris removal
New capillary growth
Wound stabilization
Inflammation
Proliferation
Remodeling
Stage Definition Stages of Wound Healing

Age & Wound Healing
Immunosenescence or age-related changes impact the immune system, putting these individuals at a higher risk for infection.
By age 50 the thymus gland has decreased in size. The function of the helper T cells deteriorates Which in turn prolongs the inflammation phase of
wound healing. During cardiopulmonary bypass blood cells are
“bypassed” in normal circulation. This activates the cytokine response and activation of the phagocyte cells.
Microsoft Clipart
Stages of Wound Healing Inflammation
ProliferationRemodeling
Source:12

Inflammation & Wound Healing
The key mediators in inflammation are Cytokines & Chemokines These proteins activate the macrophages and lymphocytes. Other contributing risk factors are high blood pressure, altered platelet
function, systemic inflammation noted by elevated C-reactive protein. There is a thickening of the blood vessel walls that supply nerves. This
causes a decreased blood supply to tissues. Elevated blood glucose levels cause damage to small blood vessels. In
time this causes defects in the cell structure at the microcirculation level.
Stages of Wound Healing Inflammation
ProliferationRemodeling
Source: 14
Genetics & Wound Healing Diabetes has the genetic disease link that
contributes to poor wound healing. Hyperglycemia will affect phagocyte function by
lessening the chemotaxic and phagocytic action of the neutrophils.
Source: 14 Microsoft Clipart

A Closer Look at the Generalized Stress Response (GSR), DM and SSI
During periods of stress such as surgery and anesthesia
There is an increase release of growth hormones With this response there is a mobilization of fatty
acids from the adipose tissue. This decreases the cellular utilization of glucose
causing a rise in blood glucose levels During periods of stress, diabetic patients react
with a variety of metabolic processes despite optimal insulin management
Microsoft Clipart
Source: 7

Review of the GSR
GSR – also known as “fight or flight response” It is the sympathetic nervous system release of
Catecholamine's: epinephrine adrenalin
The elderly individual has a slower response to epinephrine and it takes them longer to recover from its effects.
Excretion of these catecholamine's is also slower. Lets take a closer look at what happens to blood
sugar in response to stress response. (next slide)
Source: 15
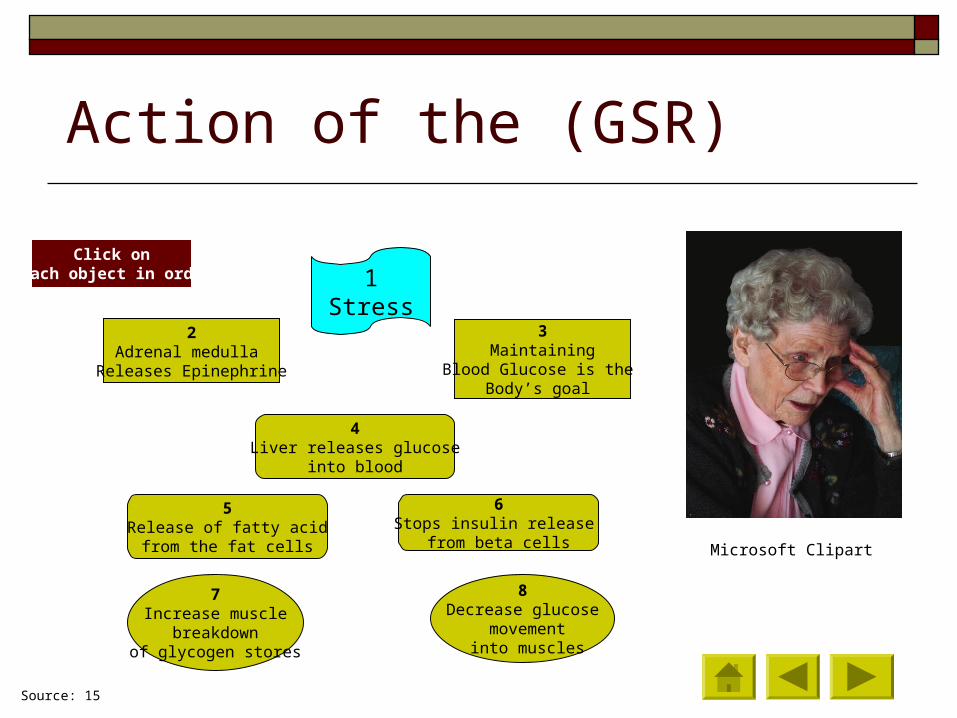
Action of the (GSR)
Microsoft Clipart
1Stress
2Adrenal medulla
Releases Epinephrine
3Maintaining
Blood Glucose is the Body’s goal
4Liver releases glucose
into blood
5Release of fatty acid
from the fat cells
6Stops insulin release
from beta cells
7Increase muscle
breakdown of glycogen stores
8Decrease glucose
movement into muscles
Click on each object in order
Source: 15
Generalized Stress Response & DM The Diabetic patient experiencing stress will have
added risk to SSI development Sporadic, transient increases of cortisol can affect
blood sugar control There is an increased secretion of cortisol in response to stress, (it can
cause damage to brain neurons over time) if the levels become too high.
This is a Positive feedback system – an example of this is when an elderly person secretes cortisol in response to stress. Repeated exposure to the neurons causes the damaged. Therefore the neurons can no longer sense the level and the hypothalamus continues to secrete the hormone.
Source: 15
To view graphic of Positive Feedback System, click HERE

Graphic of Generalized Stress Response Positive Feedback
System
Over time and repeatedstress response
activation leads todamage of neurons
Neurons in hypothalamus unable to sense
elevated cortisol level.Cont. to release CRH
Hypothalamusmeasures cortisol.In times of stress,
releases CRH
Source: 15
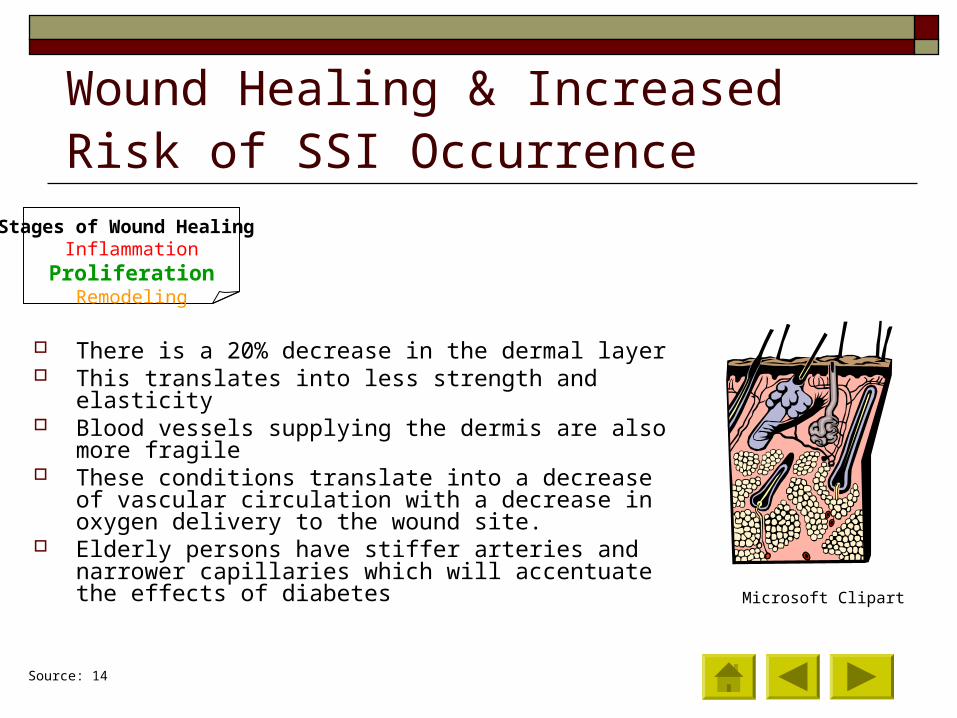
Wound Healing & Increased Risk of SSI Occurrence
There is a 20% decrease in the dermal layer This translates into less strength and elasticity Blood vessels supplying the dermis are also more fragile These conditions translate into a decrease of vascular
circulation with a decrease in oxygen delivery to the wound site.
Elderly persons have stiffer arteries and narrower capillaries which will accentuate the effects of diabetes
Microsoft Clipart
Source: 14
Stages of Wound Healing Inflammation Proliferation
Remodeling

A Closer Look at the Who, What, and Why Of SSI Development
Early detection of infection is difficult as aged (65 or older) individuals present with atypical signs and symptoms: lack of elevated white blood cell count and temperature
Persons with diabetes mellitus have neuropathic and peripheral vascular disease which will impact circulation to the wound site.
Age is a predisposing factor resulting in decreased function of systems with an increased susceptibility to stressors.
Stages of Wound HealingInflammationProliferationRemodeling
Source:13

Case Study – Part 1 Lets apply this knowledge to a case study: 65 year old Caucasian, widowed female who is overweight (101 kg.) has a
sedentary life style and lives alone. She has had poor medical care due to lack of financial resources. She thinks she recalls a doctor telling her in the past that she may have
diabetes or “something.” The patient is now in the Cardiovascular Surgical Intensive care unit
following surgery of a 4 vessel myocardial revascularization.
Microsoft Clipart
Case Study – Part 1 Post operative day #1 Patient presents with the
following: Elevated blood glucose for the last 4 assessments: 190,
200,207,195 Fatigue and difficult to arouse Low blood pressure :100/60 Sinus tachycardia: 120 bpm Urine output: 25-30cc/hr Low grade temperature: 99.1 blood temp Slight elevated white blood cell count: 11,000 Elevated C-reactive protein (CRP) level: 2 Decreased bilateral pedal pulses: + 1 Cool bilateral lower leg extremities: new on
assessment
Microsoft Clipart
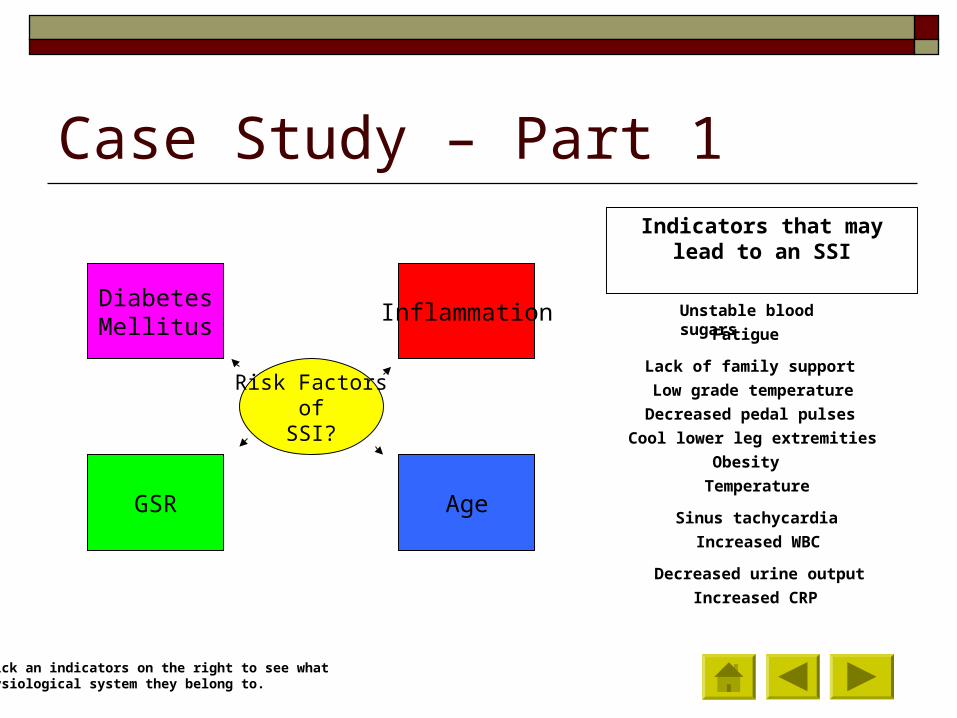
Case Study – Part 1
DiabetesMellitus
GSR Age
Risk Factors of
SSI?
Inflammation
Indicators that may lead to an SSI
Unstable blood sugars
Fatigue
Lack of family support
Low grade temperature
Decreased pedal pulses
Cool lower leg extremities
Obesity
Sinus tachycardia
Temperature
Decreased urine output
Increased WBC
Increased CRP
Click an indicators on the right to see what Physiological system they belong to.
Best Practice Standards – “Bundle” Elements
A “Bundle” is a group of researched based best practice interventions.
It is shown that when bundle elements are implemented together patient outcomes improve.
Source: 2
Best Practice Standards – “Bundle” Elements
Strict adherence to hand hygiene www.cdc.gov/handhygiene/Patient_Admission_Video.html Treat all remote infections to the elective surgical site prior surgery Do not shave hair at surgical site, but use clippers. This will cause less
microabraisions to the skin. Control serum blood sugar levels, avoid hyperglycemic states. Recommend stopping tobacco use Antiseptic showers prior surgical procedure Use appropriate surgical skin prep Surgical team hand & forearm antisepsis Administration of appropriate antimicrobial prophylaxis drug at the correct
time, and dose prior surgical incision (30min.)
Source: 2

Bundle Elements & Nursing Interventions
Pre-surgical baths have shown to decrease skin flora and multi-drug resistant bacteria (MDRO's) such as Methicillin resistant Staphaureus, vancomycin resistant Enterococci that may lead to surgical site infections.
Most SSI’s are caused by the patients own bacterial flora 20% Staphylococcus aureus 14% Coagulase negative staphylococcus 12% Enterococci
Source: 2
Bundle Elements & Nursing Interventions
Glucose control intra-operative and postoperative (target less than 200 mg/dL)
Unstable blood sugars affect the neutrophils ability to provide adequately functioning phagocytes
Maintaining the postoperative dressing for 24-48 hours
This is a critical time period when wound site is gaining stability in cellular repair and revascularization.
Source: 10

Bundle Elements & Nursing Interventions Appropriate surgical antimicrobial
prophylaxis given at: The appropriate time – 30 minutes prior cut time Provides a therapeutic blood & tissue level of antibiotic at
time of surgery Appropriate dosage – weight based. Repeat dose if
surgery extends past the ½ life of the drug Appropriate agent – for gram negative and gram positive
organisms Discontinue antibiotic 24 hours post surgery – assists in
decreasing resistance. Doses past 24 hour time frame of wound closure have not proven beneficial.
Source: 1, 3
Bundle Elements & Nursing Interventions
Clipping surgical site in place of shaving
Eliminates micro abrasions to the skin that provides an entry portal for microorganisms
Microsoft Clipart
Source: 2

Bundle Elements & Nursing Interventions
Maintain normothermia (greater that 36.0 Celsius) pre, intra, and postoperatively
Decreases vasoconstriction in blood vessels. Normothermia will promote the blood flow
and oxygen delivery to the cells Fosters immune function preservation If normothermia maintained produces less
overall stress to diabetic patient
Microsoft Clipart
Source: 9
Let’s Review Bundle elements produce better
patient outcomes.
Application of bundle practices are researched based.
Using appropriate antibiotic therapy is a key bundle
component.
True False
True
True
False
False

What’s New?...Not Much!
Decreased emphasis and incentive for drug manufactures to develop new generations of antimicrobials to treat infections.
More deaths related to Methicillin-resistant Staphylococcus aureus (MRSA) in U.S. facilities than from HIV/AIDS & Tuberculosis combined.
Only 83 antibacterial in clinical trials – very small number in late stage testing
Only 5 pharmaceutical companies still support antibacterial programs.
Source: 3

Antibiotic Manufacturing Strategies
Infectious Disease Society of America (ISDA) is working on a plan in cooperation with the pharmaceutical industry and academia to create and sustain research and a long term plan. Incorporate big pharmacies, and small entities Create incentives for pharmaceutical companies to participate in
antibiotic research and development.
Source: 3

Case Study – Part 2
Lets apply this knowledge to our case study: Post operative surgical day #3 Assessment findings: Blood Sugar range 185-220 over last 48hours Temp. 99.1-100.9(oral ranges) WBC 11,000 CRP level 3 Sternal incision warm, red, small opening at bottom draining
creamy white fluid Wound culture showing Moderate PMS’s & Moderate colonies of
Staphylococcus aureus Fatigues easily Stable SBP, Sinus tachycardia (105-110bpm), U.O. 30cc/hr
Microsoft Clipart

Case Study – Part 2
1. Diabetes affect 2.8 million people in the United States. Identify three case study laboratory results that may be indicators of an SSI.
Temperature, WBC, CRP, U.O., Positive wound culture, Fatigue
2. What assessment finding is a response to activation of the Generalized Stress Response?
Increased Heart Rate, Warm draining wound, Positive wound culture
3. During cardiovascular revascularization surgery, what process causes a cytokine response?
The process of “bypass”, anesthesia, maintaining normothermia
4. In reference to question 3, what stage of wound healing is critical to a diabetic with uncontrolled blood sugars?
Inflammation, Proliferation, Remodeling
5. How is the proliferation stage of wound healing affected by diabetes?
Microcirculation, cellular regeneration , decrease in metabolic needs
6. What three nursing interventions can be initiated to help decrease the risk of patients developing an SSI?
Hand Hygiene, Blood glucose control, Maintaining normothermia, quick ventilator weaning, frequent turning of patient

Tying It All Together Surgical Site Infections affect patients, families, hospital
systems, and communities. They add to personal pain and suffering, mortality and financial
burdens. Research has identified that using the “Bundle” method of
preventive measures is more effective in preventing SSI’s than when elements are applied inconsistently and individually.
Diabetics are at a higher surgical risk due to the inflammation correlation process of their disease.

Tying It All Together Nursing Interventions Key “take away” – Astute assessments and documentation of
subtle indicators Hand hygiene before all patient cares, tight control of
blood sugars, slight elevated WBC, mental status changes, low grade temps, maintain surgical wound dressing in place for 24 – 48 hours.

References1. Barnard, B. (2003). Best practices prevention of surgical site infections. Infection Control Today, 1-6.
Retrieved February 23, 2010 from http://www.infectioncontroltoday.com/articles/341bpract.html
2. Beaver, M. (2008). CABG wound are best practices are elusive. Infection Control Today, 1-4. Retrieved February 23, 2010 from http://www.infectioncontroltoday.com/articles/cabg-wound-care-best.html
3. Boucher, H.W., Talbot, G.H., Bradley, J.S., Edwards, J.E., Gilbert, D., Reice, L.B., etal. (2009). Bad bugs, no drugs: no ESKAPE! An update from the infectious diseases society of america, 48, 1-12. Infectious Disease Society of Americal
4. Connection diabetes and inflammation. Science Daily, 1-2. Retrieved March 22, 2010, from http://www.sciencedaily.com/released/2007/07/070722105802.htm
5. De la Torre, J. & Chambers, J.A. (2008). Wound healing, chronic wounds. Plastic Surgery, 1-5. Retrieved March 21, 2010, from the Medsape database.
6. Diagnosis and classification of diabetes mellitus. American Diabetes Association, 1-11. Retrieved March 15, 2010, from http://care.diabetesjournals.org/content/33/supplement_l/s62.full
7. Engelic, G., Wright, D.G., Hartshorn, K.L. (2001). Acquired disorders of phagocyte function complicating medical and surgical illness. Clinical Infectious Diseases, 33, 2040-8.
8. http://en.wikipedia.org/wiki/Diabetes
9. Kurz, A. Sesslelr, D.I., Lenhardt, R. (1996). Perioperative normothermia to reduce the incidence of surgical wound infection and shorten hospitalization. New England Journal of Medicine, 334, 1309-1216. Retrieved March 26, 2010, from http://www.endo.gr/cgi/content/full/334/19/1209
References10. Mercandetti, M. & Cohen, A.J. (2008) Wound healing, healing and repair. Plastic Surgery, 1-5.
Retrieved March 26, 2010, from Medscape database.11. Microsoft clipart online.12. Porth, C.M. & Matfin, G. (2009). Pathophsiology concepts of altered health states. In. H. Surrena, et al
(Ed.), Concepts of altered health in order adults (pp.36-55). Philadelphia, PA:Wolters Kluwer Health/Lippincott Williams & Wilkins.
13. Porth, C.M. & Matfin, G. (2009). Pathophsiology concepts of altered health states. In. H. Surrena, et al (Ed.), Diabetes mellitus and the metabolic syndrome (pp. 1047-1077). Philadelphia, PA:Wolters Kluwer Health/Lippincott Williams & Wilkins.
14. Porth, C.M. & Matfin, G. (2009). Pathophsiology concepts of altered health states. In. H. Surrena, et al (Ed.), Inflammation, tissue repair, and wound healing (377-399). Philadelphia, PA:Wolters Kluwer Health/Lippincott Williams & Wilkins.
15. Porth, C.M. & Matfin, G. (2009). Pathophsiology concepts of altered health states. In. H. Surrena, et al (Ed.), Stress and adaptation (198-238). Philadelphia, PA:Wolters Kluwer Health/Lippincott Williams & Wilkins.
16. Stone, P.W., (2009). Changes in medicare reimbursement for hospital-acquired conditions including infections. Association for Professionals in Infection Control and Epidemiology, 37, 12!-18A.
17. Swenson, B.R., Hedrick, T.L., Mezger, R., Bonartt, H., Ruett, T.L., Sqwyefr, R.G. (2009). Effects of preoperative skin preparation on postoperative wound infection rates: a prospective study of 3 skin prparitn protocols. Infection Control and Hospital Epidemiology, 30, 964-971.

The End
Thank you for your attention and participation!
Recommended