Preventing Postoperative Preventing Postoperative Cognitive Decline Cognitive Decline
in the Elderlyin the Elderly
Alex Bekker, M.D., Ph.DAlex Bekker, M.D., Ph.DProfessor and ChairProfessor and Chair
Department of AnesthesiologyDepartment of AnesthesiologyRutgers New Jersey Medical SchoolRutgers New Jersey Medical School
"My brain, that's my second favorite organ"
Subtle Perioperative Brain InjurySubtle Perioperative Brain Injury
Emergence DeliriumEmergence Delirium
Postoperative DeliriumPostoperative Delirium
Postoperative Cognitive DeclinePostoperative Cognitive Decline
Postoperative DeliriumPostoperative Delirium
An acute brain disorder An acute brain disorder that has a fluctuating that has a fluctuating course and course and characterized by characterized by disturbance of disturbance of attention, memory, attention, memory, orientation, and orientation, and perceptionperception
Incidence (in elderly) Incidence (in elderly) Noncardiac surgery: Noncardiac surgery: 10%-40%10%-40%Cardiac surgery: 20%-Cardiac surgery: 20%-70% 70%
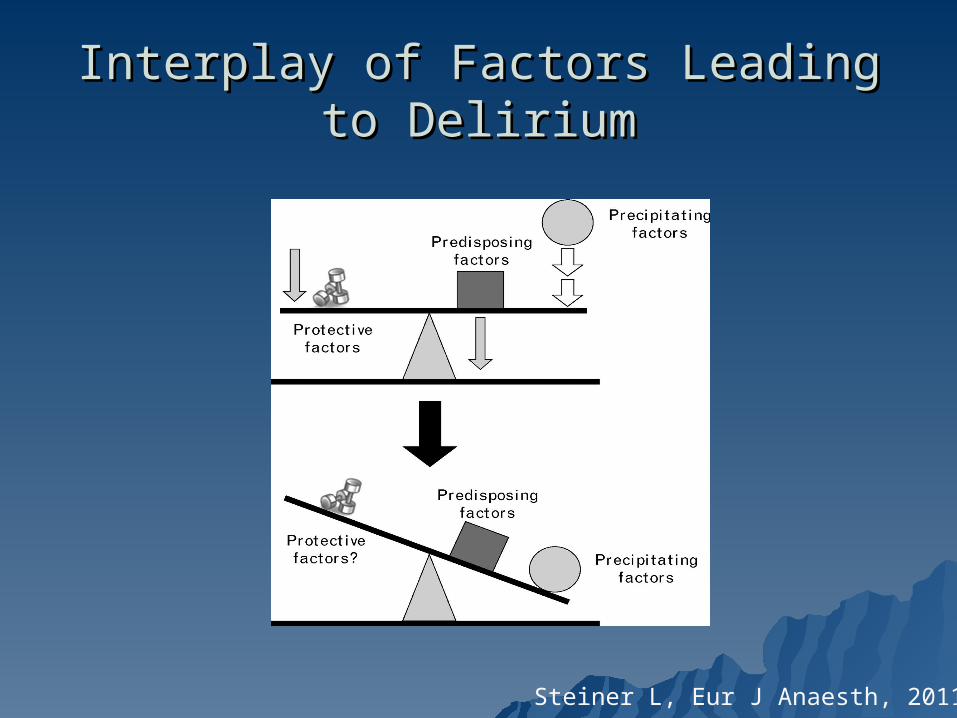
Interplay of Factors Leading to DeliriumInterplay of Factors Leading to Delirium
Steiner L, Eur J Anaesth, 2011
Predisposing FactorsPredisposing Factors
AgeAge Functional impairmentFunctional impairment Cognitive impairmentCognitive impairment Medical co-morbidityMedical co-morbidity DrugsDrugs Genetic factors (sigma 4 allele of Genetic factors (sigma 4 allele of
apolipoprotein E4)apolipoprotein E4)
Precipitating FactorsPrecipitating Factors
Admission to ICUAdmission to ICU DrugsDrugs Concomitant illnessConcomitant illness Primary neurologic diseasePrimary neurologic disease PainPain Use of physical restraintsUse of physical restraints Prolonged sleep deprivationProlonged sleep deprivation
Can Delirium be Prevented in the Can Delirium be Prevented in the Postoperative Period?Postoperative Period?
Pharmacological preventionPharmacological prevention Non-pharmacologic multicomponent Non-pharmacologic multicomponent
strategiesstrategies– Good nursing careGood nursing care– Regular orientationRegular orientation– Early mobilizationEarly mobilization– Reduce modifiable risk factorsReduce modifiable risk factors
Inouye S, JAMA, 1998
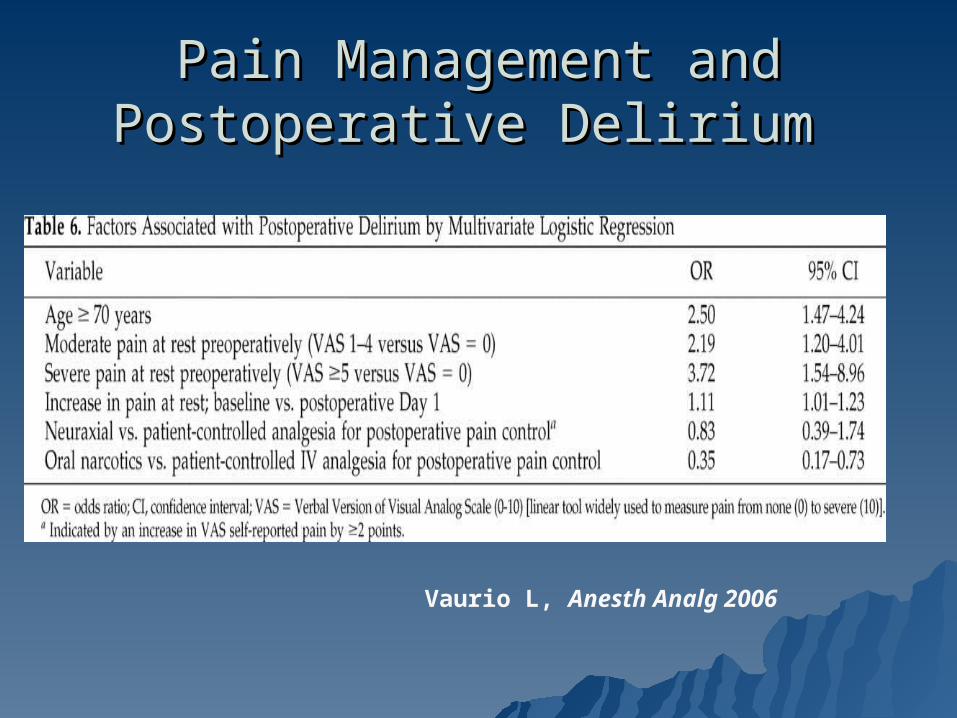
Pain Management and Pain Management and Postoperative Delirium Postoperative Delirium
Vaurio L, Anesth Analg 2006
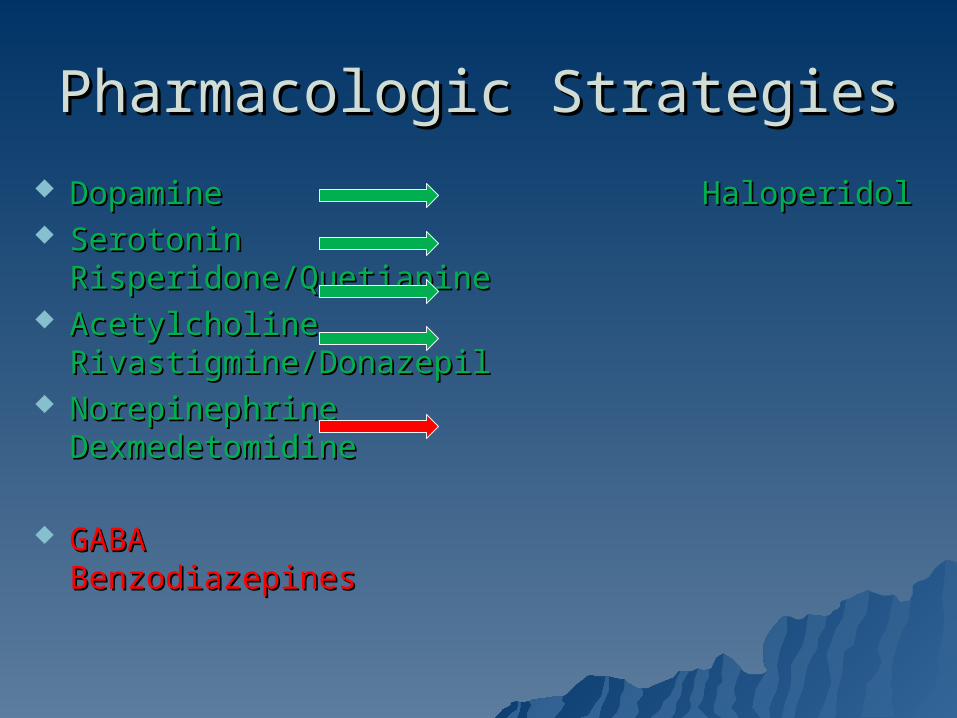
Pharmacologic StrategiesPharmacologic Strategies
Dopamine HaloperidolDopamine Haloperidol Serotonin Risperidone/QuetiapineSerotonin Risperidone/Quetiapine Acetylcholine Rivastigmine/DonazepilAcetylcholine Rivastigmine/Donazepil Norepinephrine DexmedetomidineNorepinephrine Dexmedetomidine
GABA BenzodiazepinesGABA Benzodiazepines
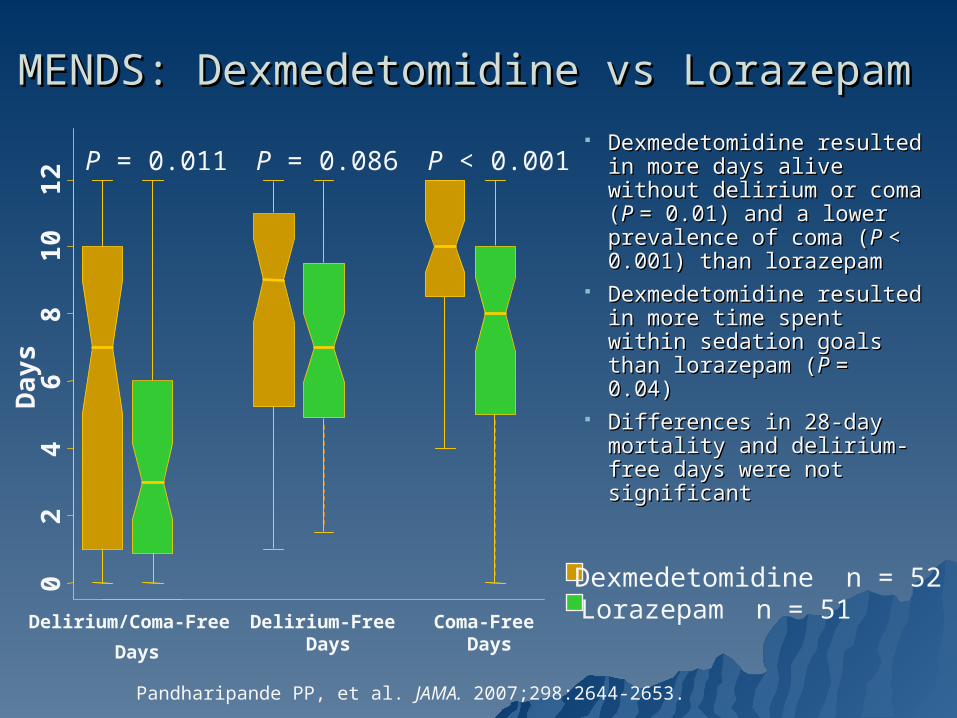
MENDS: Dexmedetomidine vs Lorazepam MENDS: Dexmedetomidine vs Lorazepam
Pandharipande PP, et al. JAMA. 2007;298:2644-2653.
Dexmedetomidine resulted Dexmedetomidine resulted in more days alive without in more days alive without delirium or coma (delirium or coma (P P = = 0.01) and a lower 0.01) and a lower prevalence of coma (prevalence of coma (P P < < 0.001) than lorazepam0.001) than lorazepam
Dexmedetomidine resulted Dexmedetomidine resulted in more time spent within in more time spent within sedation goals than sedation goals than lorazepam (lorazepam (P P = 0.04)= 0.04)
Differences in 28-day Differences in 28-day mortality and delirium-free mortality and delirium-free days were not significantdays were not significant
Days
Lorazepam n = 51Dexmedetomidine n = 520
24
68
10
12 P = 0.011
Delirium/Coma-Free
Days
Delirium-Free Days
P = 0.086 P < 0.001
Coma-Free Days
Midazolam
Dexmedetomidine
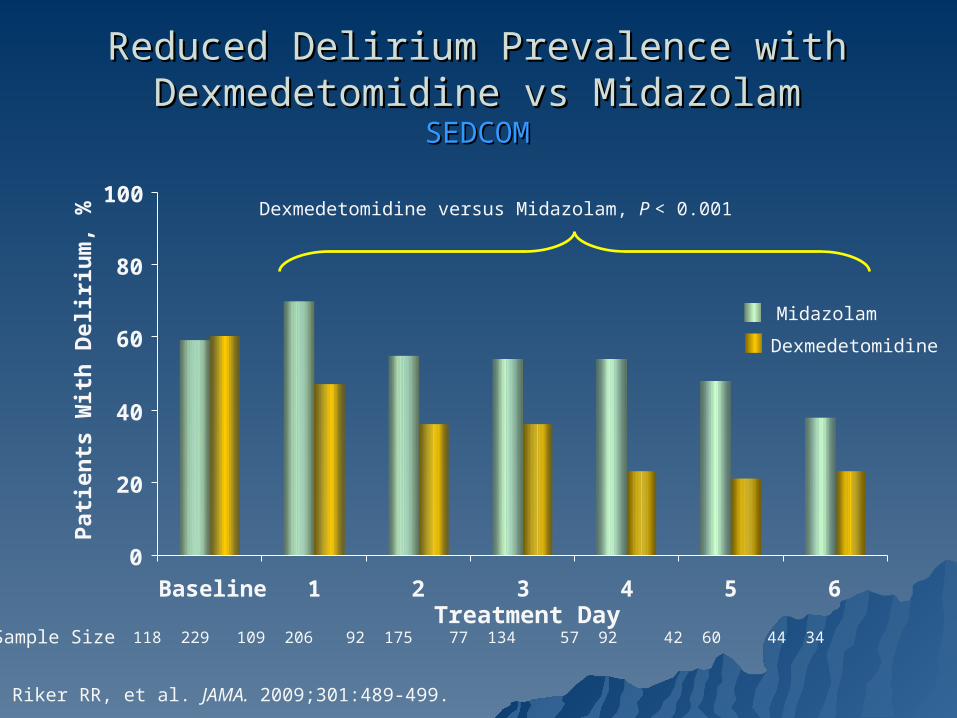
Dexmedetomidine versus Midazolam, P < 0.001
Reduced Delirium Prevalence with Dexmedetomidine Reduced Delirium Prevalence with Dexmedetomidine vs Midazolamvs Midazolam
SEDCOMSEDCOM
Sample Size 118 229 109 206 92 175 77 134 57 92 42 60 44 34Treatment Day
0
20
40
60
80
100
Baseline 1 2 3 4 5 6
Pati
en
ts W
ith
Deliri
um
, %
Riker RR, et al. JAMA. 2009;301:489-499.
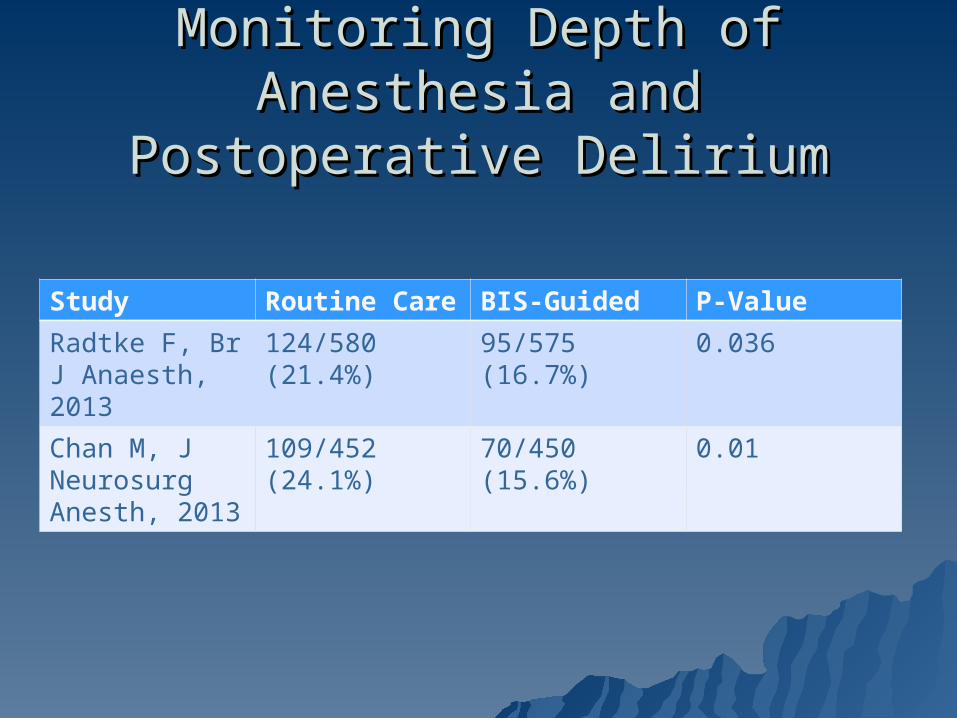
Monitoring Depth of Anesthesia Monitoring Depth of Anesthesia and Postoperative Deliriumand Postoperative Delirium
Study Routine Care BIS-Guided P-Value
Radtke F, Br J Anaesth, 2013
124/580 (21.4%)
95/575 (16.7%)
0.036
Chan M, J Neurosurg Anesth, 2013
109/452 (24.1%)
70/450 (15.6%)
0.01
Delirium PreventionDelirium Prevention Multicomponent targeted intervention strategyMulticomponent targeted intervention strategy
Optimizing medical conditionOptimizing medical condition
Continue antidepressant treatmentContinue antidepressant treatment
Postoperative pain control Postoperative pain control
Avoid benzodiazepinesAvoid benzodiazepines
Dexmedetomidine Dexmedetomidine
Use of brain function monitors (?)Use of brain function monitors (?)
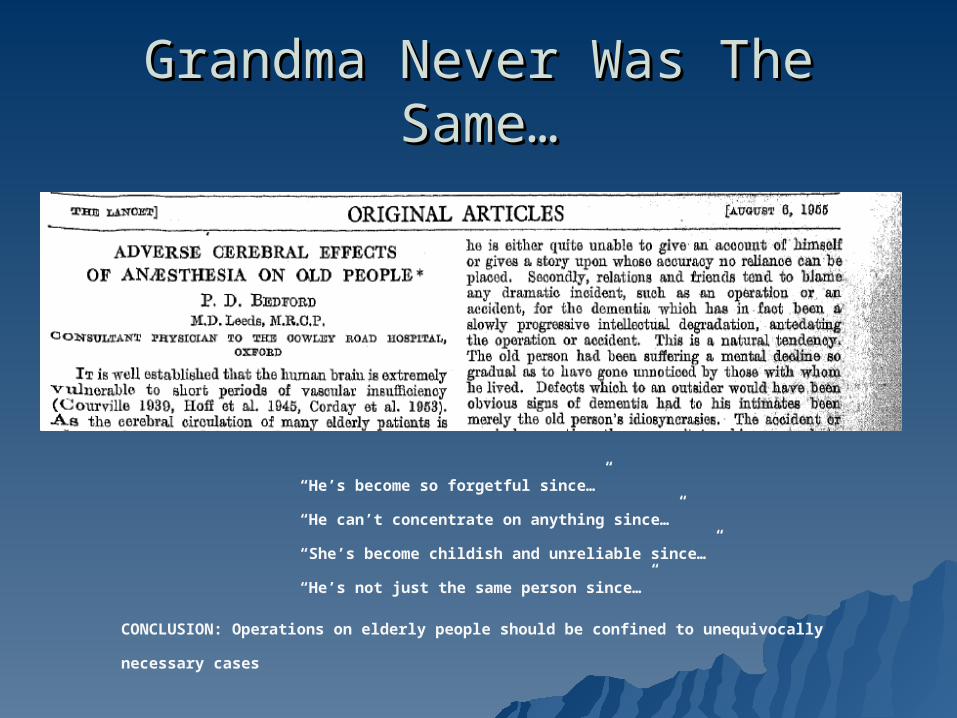
Grandma Never Was The Same…Grandma Never Was The Same…
“He’s become so forgetful since…”
“He can’t concentrate on anything since…”
“She’s become childish and unreliable since…”
“He’s not just the same person since…”
CONCLUSION: Operations on elderly people should be confined to unequivocally necessary cases
Postoperative Cognitive Postoperative Cognitive Dysfunction (POCD):Dysfunction (POCD):
An impairment of functioning An impairment of functioning in several cognitive in several cognitive domains: memory, domains: memory, executive functioning, executive functioning, attention, and attention, and comprehensioncomprehension
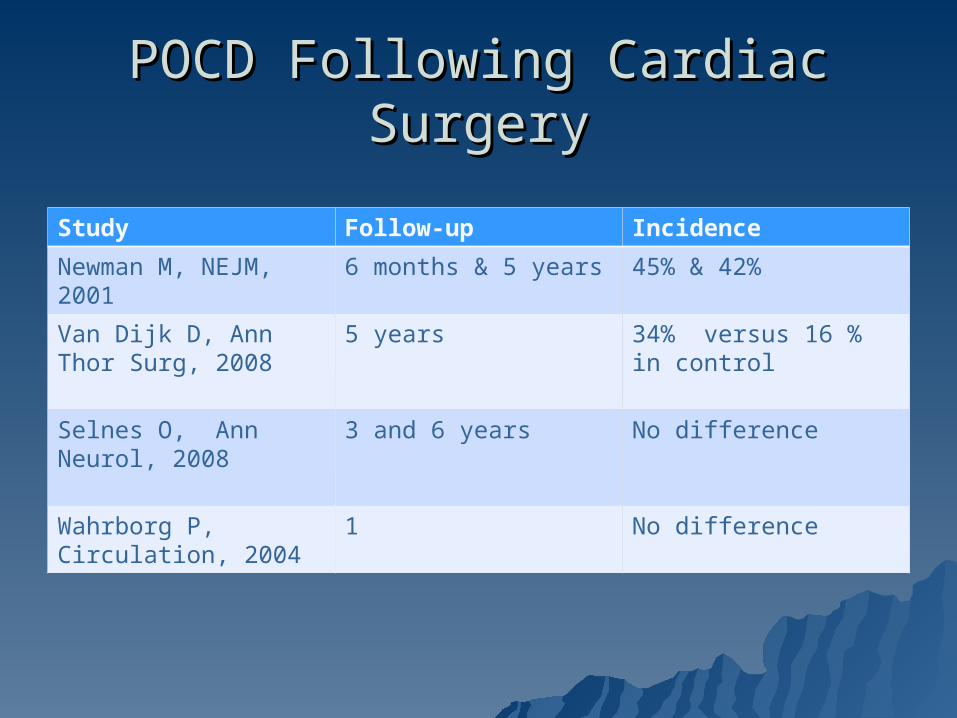
POCD Following Cardiac SurgeryPOCD Following Cardiac Surgery
Study Follow-up Incidence
Newman M, NEJM, 2001
6 months & 5 years 45% & 42%
Van Dijk D, Ann Thor Surg, 2008
5 years 34% versus 16 % in control
Selnes O, Ann Neurol, 2008
3 and 6 years No difference
Wahrborg P, Circulation, 2004
1 No difference
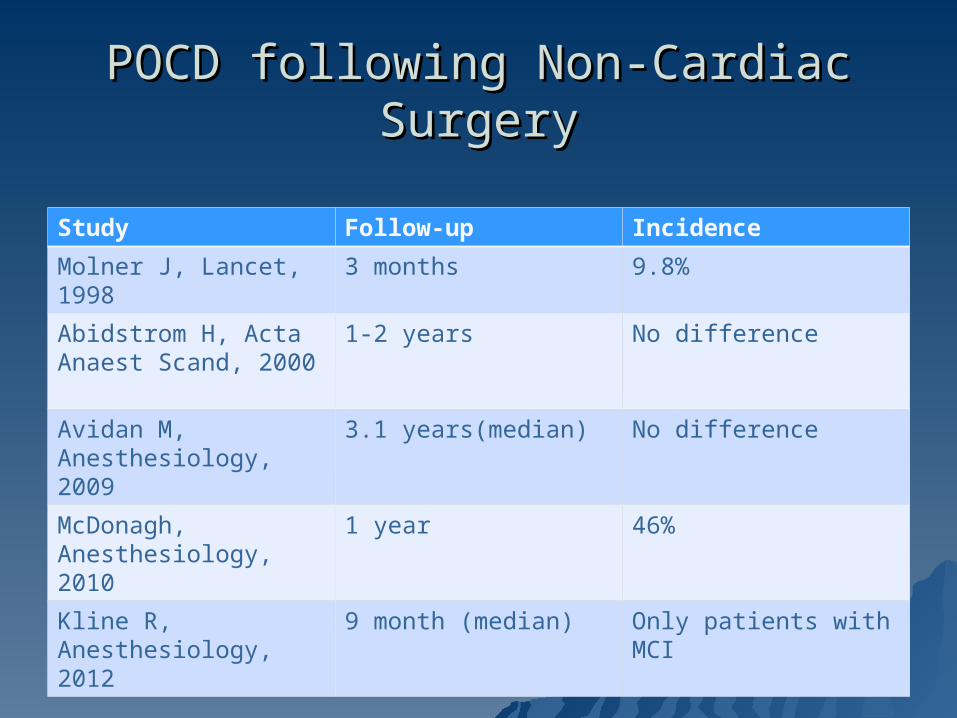
POCD following Non-Cardiac SurgeryPOCD following Non-Cardiac Surgery
Study Follow-up Incidence
Molner J, Lancet, 1998 3 months 9.8%
Abidstrom H, Acta Anaest Scand, 2000
1-2 years No difference
Avidan M, Anesthesiology, 2009
3.1 years(median) No difference
McDonagh, Anesthesiology, 2010
1 year 46%
Kline R, Anesthesiology, 2012
9 month (median) Only patients with MCI
Methodological Challenges Methodological Challenges
Definition of POCDDefinition of POCD What tests should we use?What tests should we use? ControlsControls Learning effectLearning effect Cognitive trajectoryCognitive trajectory
There are no laboratory test or imaging study which can be used to predict or diagnose POCD
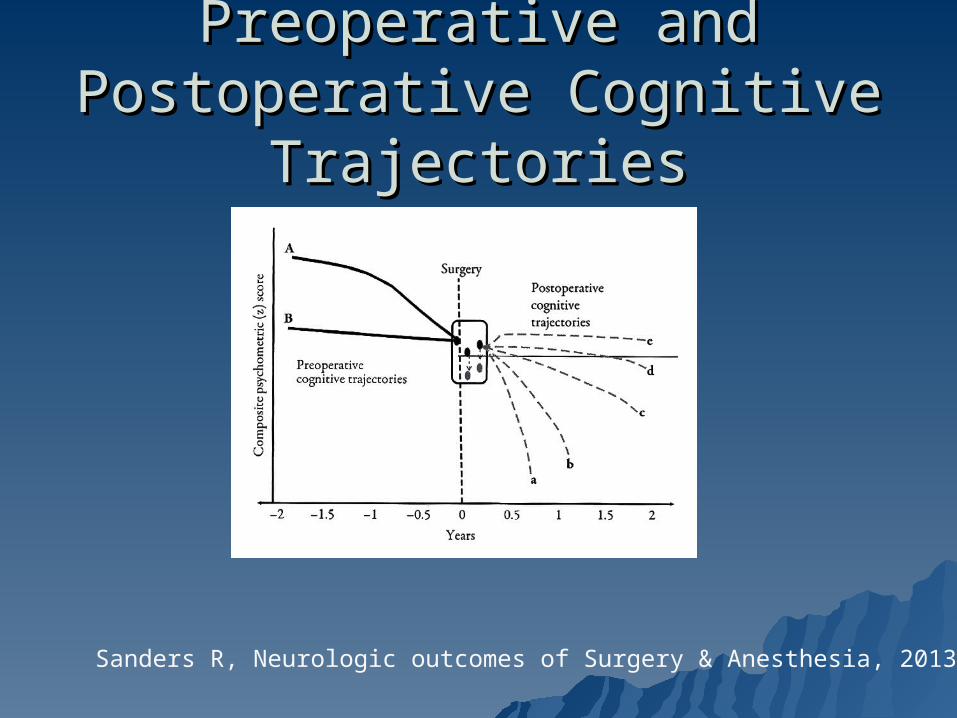
Preoperative and Postoperative Preoperative and Postoperative Cognitive TrajectoriesCognitive Trajectories
Sanders R, Neurologic outcomes of Surgery & Anesthesia, 2013
Predisposing Factors : POCDPredisposing Factors : POCD
AgeAge
Preoperative cognitionPreoperative cognition
Type of surgeryType of surgery
Vascular risk factorsVascular risk factors
Apolipoprotein E genotype (?)Apolipoprotein E genotype (?)
Possible causes of POCD Possible causes of POCD Related to SurgeryRelated to Surgery
Altered cerebral perfusionAltered cerebral perfusion AnestheticsAnesthetics Cerebral microemboliCerebral microemboli InflammationInflammation
– Surgery relatedSurgery related– Patient relatedPatient related
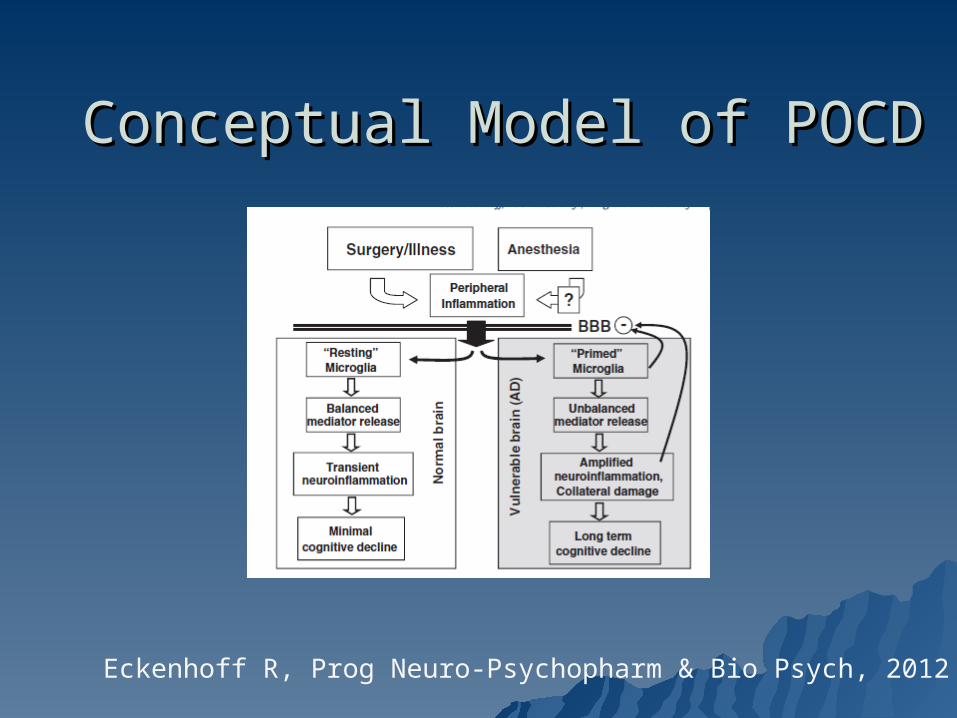
Conceptual Model of POCDConceptual Model of POCD
Eckenhoff R, Prog Neuro-Psychopharm & Bio Psych, 2012
MCI: DiagnosisMCI: Diagnosis
MCI is diagnosed when there is:MCI is diagnosed when there is:
– Evidence of memory impairmentEvidence of memory impairment– Preservation of general cognitive and Preservation of general cognitive and
functional abilitiesfunctional abilities– Absence of diagnosed dementiaAbsence of diagnosed dementia
Morris J, Arch Neurol, 2001
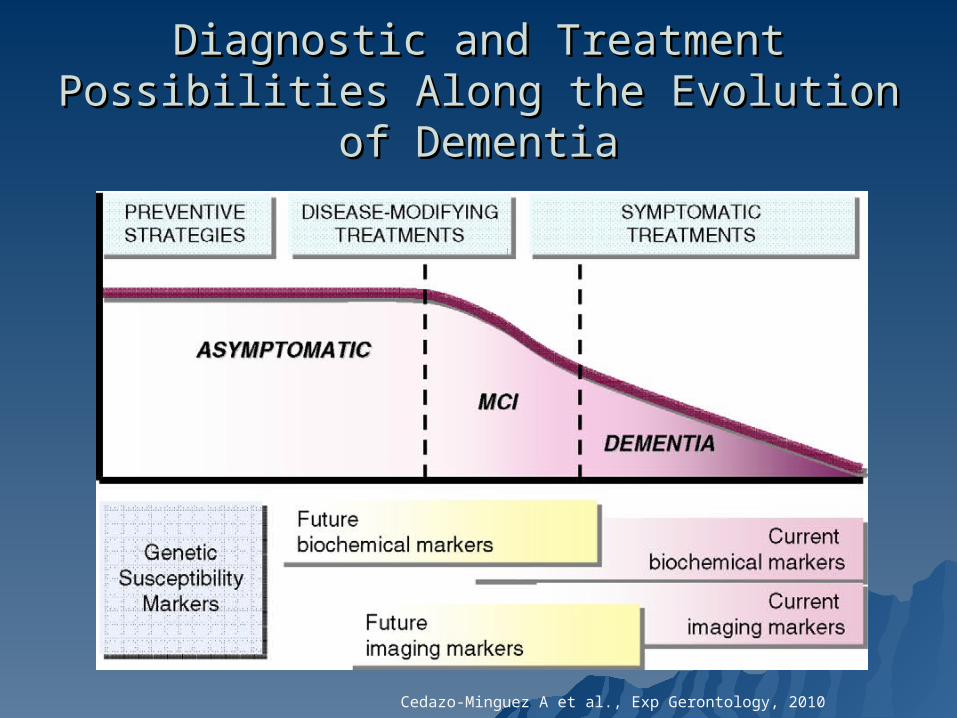
Diagnostic and Treatment Possibilities Along Diagnostic and Treatment Possibilities Along the Evolution of Dementiathe Evolution of Dementia
Cedazo-Minguez A et al., Exp Gerontology, 2010
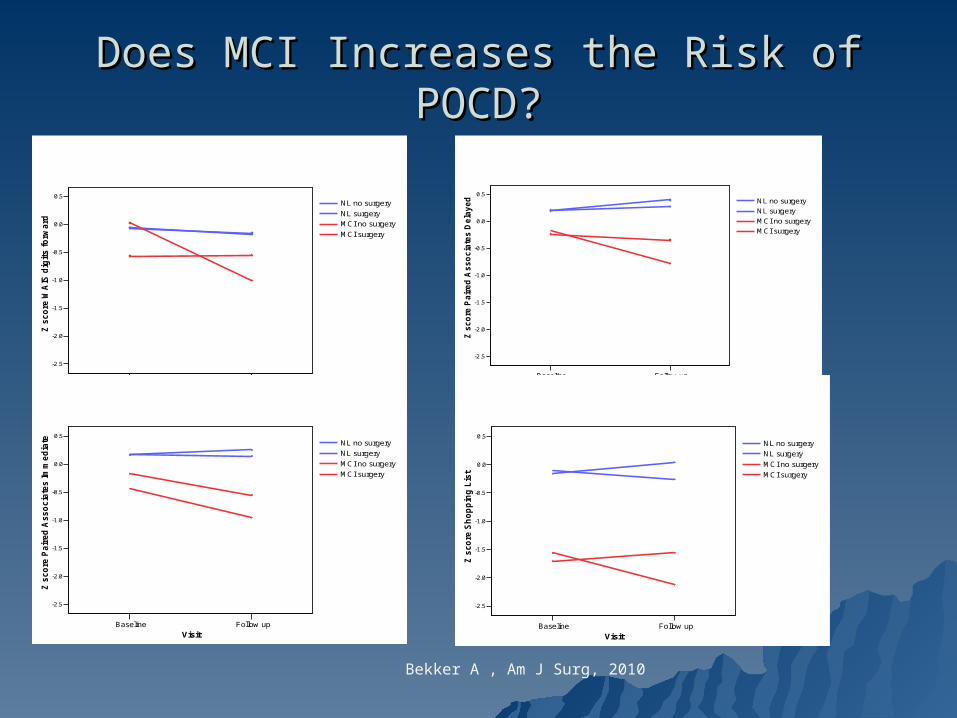
Does MCI Increases the Risk of POCD?Does MCI Increases the Risk of POCD?
Baseline Follow-up
Visit
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
Z s
co
re W
AIS
dig
its
fo
rwa
rd
NL no surgery
NL surgery
MCI no surgery
MCI surgery
Baseline Follow up
Visit
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
Z s
co
re P
air
ed
As
so
cia
tes
De
lay
ed
NL no surgery
NL surgery
MCI no surgery
MCI surgery
Baseline Follow up
Visit
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
Z s
co
re P
air
ed
Asso
cia
tes Im
med
iate
NL no surgery
NL surgery
MCI no surgery
MCI surgery
Baseline Follow up
Visit
-2.5
-2.0
-1.5
-1.0
-0.5
0.0
0.5
Z s
co
re S
ho
pp
ing
Lis
t
NL no surgery
NL surgery
MCI no surgery
MCI surgery
Bekker A , Am J Surg, 2010
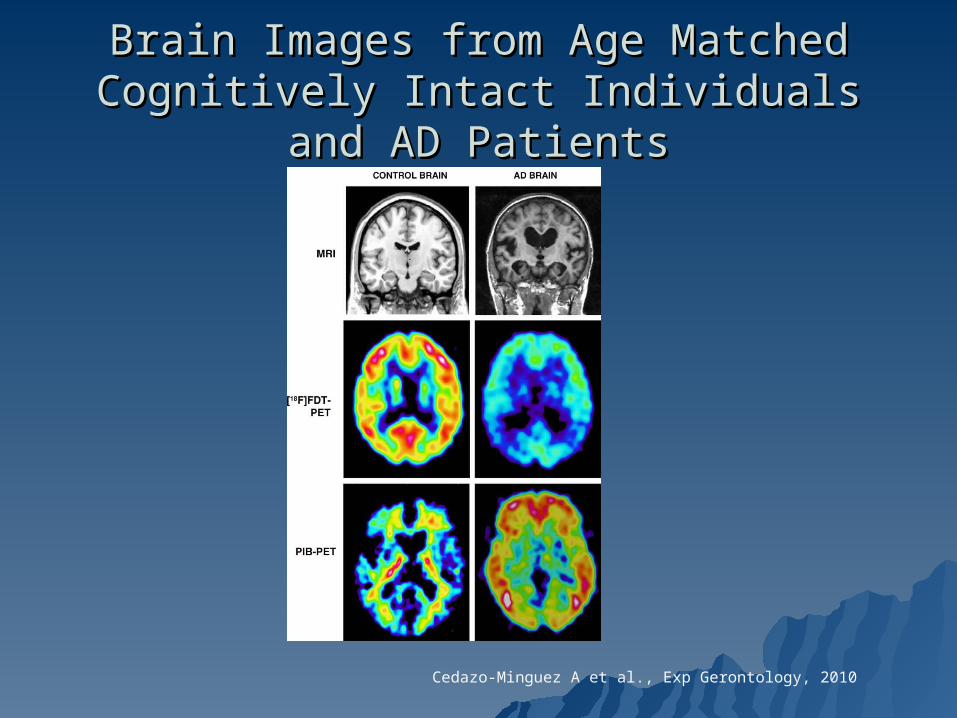
Brain Images from Age Matched Cognitively Brain Images from Age Matched Cognitively Intact Individuals and AD PatientsIntact Individuals and AD Patients
Cedazo-Minguez A et al., Exp Gerontology, 2010
Study Design: Longitudinal Study Design: Longitudinal Examination of Structural MRI Examination of Structural MRI
From ADNI DatabaseFrom ADNI Database Apply MRI to study perioperative cortical Apply MRI to study perioperative cortical
volume change in surgical subjects volume change in surgical subjects
Examine hippocampus, gray matter, white Examine hippocampus, gray matter, white matter and lateral ventricle. matter and lateral ventricle.
Examine composite cognitive scoreExamine composite cognitive score
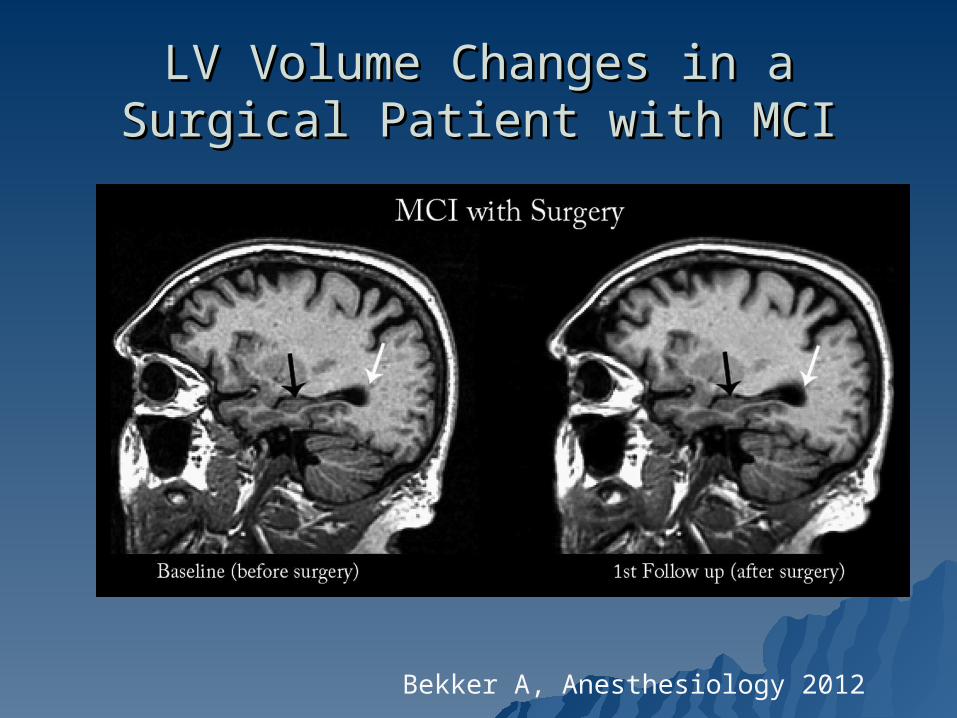
LV Volume Changes in a Surgical LV Volume Changes in a Surgical Patient with MCIPatient with MCI
Bekker A, Anesthesiology 2012
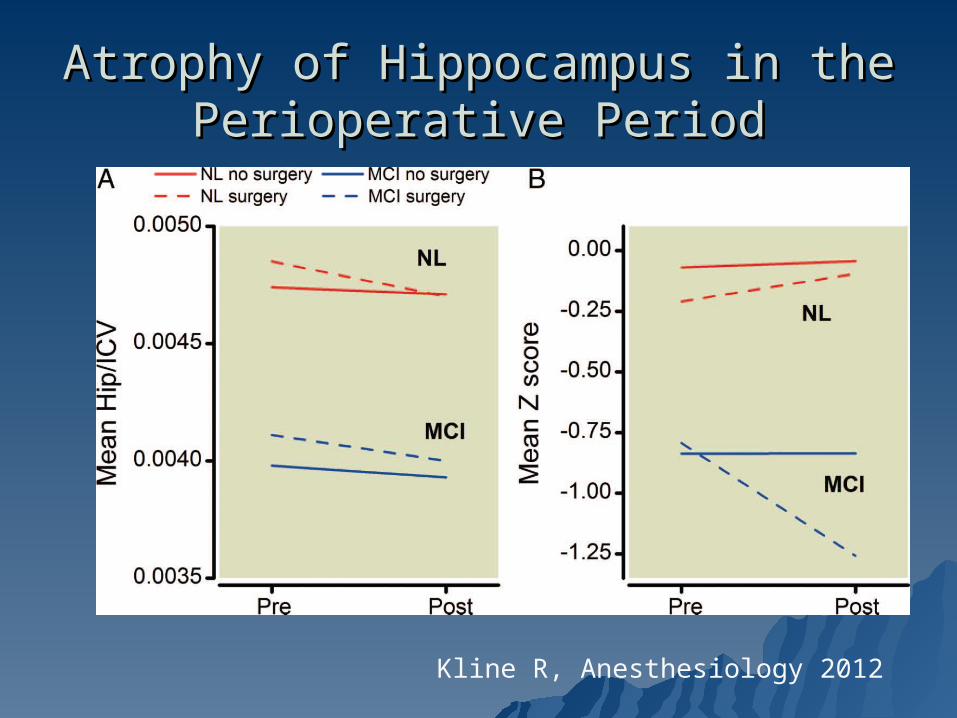
Atrophy of Hippocampus in the Atrophy of Hippocampus in the Perioperative PeriodPerioperative Period
Kline R, Anesthesiology 2012
POCD: Concluding RemarksPOCD: Concluding Remarks
Standardization of diagnostic criteria Standardization of diagnostic criteria NeuroinflammationNeuroinflammation Low intraoperative cerebral Low intraoperative cerebral
oxygenationoxygenation Patient-related factors:Patient-related factors:
– AgeAge– Pre-existing cognitive impairmentPre-existing cognitive impairment– Cognitive reserveCognitive reserve– Priming of the immune systemPriming of the immune system
Low Tech Prescriptions for Low Tech Prescriptions for LongevityLongevity
““Swim, dance a little, go to Paris every Swim, dance a little, go to Paris every August and live within walking distance of August and live within walking distance of two hospitals”two hospitals”
Horatio Lure, at 80Horatio Lure, at 80
““Stay busy, get plenty of exercise and don’t Stay busy, get plenty of exercise and don’t drink too much.drink too much.
Then again, don’t drink too little”Then again, don’t drink too little”Herman ”Jack Rabbit” Smith-Johannsen, at Herman ”Jack Rabbit” Smith-Johannsen, at
103103
““The secret to longevity is to keep breathing” The secret to longevity is to keep breathing” My observationMy observation
Recommended