~~
0 1991 S. Karger AG, Basel Vox Sang 1991;61:3&36 0042-9007/91/0611-000 $2.75/0
Prevalence of Anti-HCV Antibodies Confirmed by Recombinant Immunoblot in Different Population Subsets in The Netherlands
C. L. Van der Poela, H . W Reesinka*b, E. P. Mauser-Bunschoten', R. H. Kaufmannd, A. Leentvaar-Kuypers", R. A . E M . Chamuleau', W Schaasbergb, E. Bakkerb, P. J . Exel-Oehlersb, I . Theobaldsb, J . J . P. Van Boven a,
A. Camerong, P. N . Lelieb 'Red Cross Blood Bank, Amsterdam; bCentral Laboratory of the Netherlands Red Cross Blood Transfusion Service, Amsterdam; 'Van Creveld Clinic, Bilthoven; dDialysis Group The Netherlands, Leyenburg Hospital, The Hague; 'Municipal Health Service, Amsterdam: 'Academic Medical Centre, University of Amsterdam; BRed Cross Blood Transfusion Service, Paramaribo, Surinam
Key Words. Hepatitis C virus - Anti-HCV RIBA . Blood donors
Abstract. The prevalence of antibodies to hepatitis C virus (anti-HCV) was studied in various population subsets in the Netherlands with anti-HCV ClOO enzyme linked immunosorbent assay (ELISA), and confirmed with recombinant immunoblot assay (RIBA). Anti-HCV ClOO ELISA positivity and RIBA positivity were found in 39 (0.7%) and 5 (0.1%) of 5,434 blood donors from Amsterdam; 25 (5%) and 2 (0.4%) of 481 blood donors from Surinam (South America); 19 (9%) and 2 (1%) of 213 multitransfused patients; 28 (4%) and 15 (2%) of 633 hemodialysis patients; 179 (80%) and 150 (67%) of 225 hemophiliaA and B patients; 8 (80%) and 4 (40%) of 10 intravenous drug abusers; 18 (15%) and 2 (2%) of 119 anti-HIV-positive homosexual men; 2 (2%) and none of 106 anti-HIV-negative homosexual men; 6 (32%) and 3 (16%) of 19 patients with acute hepatitis non-A, non-B (NANBH); 13 (65%) and 8 (40%) of 20 patients with chronic NANBH and/or cryptogenic cirrhosis; and 4 (40%) and 1(10%) of 10 patients with idiopathic autoimmune chronic hepatitis. Among blood donors, a positive correlation between a history of jaundice after the age of 18years and the presence of RIBA-confirmed anti-HCV antibodies was found. Among both blood donors and hemodialysis patients, a positive correlation of RIBA-confirmed anti-HCV positivity with elevated alanine aminotransferase levels, but not with the presence of anti-hepatitis B core antibodies was found. In the Netherlands, HCV antibodies are low endemic among blood donors, as well as among blood donors from Surinam, and are more frequently observed in patients with NANBH and individuals at risk of blood-borne virus infections. It is concluded that 8-13% of the ClOO ELISA-positive individuals in low-risk populations are RIBA-confirmed positive, as compared to 5680% of individuals at increased risk.
Introduction
Posttransfusion hepatitis non-A, non-B (IT-NABH) re- mains one of the major complications of blood transfusion. In Europe and in the USA, approximately 2-14% of recip- ients of blood products develop PT-NANBH [l]. Especially the long-term consequences of PT-NANBH such as chronic hepatitis, liver cirrhosis and the association with hepatocel- lular carcinoma are of concern [l-31.
Researchers at Chiron Corporation in Emeryville, Cal- if., USA, have expressed in Escherichia coli a cDNA clone (clone 5-1-1) from serum of a proven NANBH infectious chimpanzee, yielding a recombinant protein that binds spe-
cifically to antibodies in sera of patients with chronic NANBH [4]. A single-stranded RNA virus has been de- fined, that was designated hepatitis C virus (HCV). Using overlapping cDNA clones, the 5-1-1 clone has also been expressed as part of a larger recombinant fusion protein (C100-3) expressed in yeast, with which a prototype ra- dioimmunoassay (RIA) and later a commercially available anti-HCV enzyme-linked immunoassay (ClOO ELISA) for detection of anti-HCV antibodies were developed [5-71. The specificity of the anti-HCV ClOO ELISA as a screening test in blood donors for the prevention of PT-NANBH in recipients was described as 93% 181. In addition, the ClOO ELISA was shown to be of equal [8] or higher (9, 101

Prevalence of Anti-HCV in the Netherlands 31
sensitivity than alanine aminotransferase (ALT) surrogate testing in preventing PT-NANBH in recipients. However, by screening large numbers of blood donors, false-positive ClOO ELISA results occur, and approximately 80% of the ClOO ELISA-positive blood donors are not associated with PT-NANBH in the recipient [8,11]. In the absence of con- firmatory assays, cofactors of anti-HCV-positive blood do- nors (raised ALT level, high ClOO ELISA optical density to cutoff ratio, and persistence of the anti-HCV reactivity during follow-up) were shown to be helpful in predicting HCV infectivity [8].
More recently, a recombinant immunoblot assay (RI- BA) employing both the ClOO (expressed in E. Coli) and 5-1-1 (expressed in yeast) antigens, was developed to con- firm anti-HCV antibody reactivity. By employing virtually the same antigens as the ELISA, the RIBA cannot be regarded as an independent confirmation test. Neverthe- less, in a sample size of 5,150 transfused blood products, the combination of antibody positivity, both in ClOO ELISA and in RIBA, was very specifically associated with PT- NANBH in the recipients [12]. This finding was supported by another prospective study of Ebeling et al. [13]. The sensitivity of the ClOO ELISA plus RIBA combination for the detection of infectious HCV carriers, however, ap- peared to be limited as compared to ELISA alone [12].
HCV-specific nucleotide sequences have been amplified by cDNA polymerase chain reaction (PCR) from sera of anti-HCV-positive NANBH patients [ll, 141, but this test is not yet suited for large-scale confirmatory testing.
The aim of this study was to establish the prevalence of RIBA-confirmed anti-HCV antibodies in Dutch blood do- nors, as well as in blood donors from Surinam; in the Netherlands an important subset of the population consists of natives of Surinam (South America), a former Dutch colony. In addition, the prevalence of anti-HCV was estab- lished in patients with acute and chronic hepatitis, recip- ients of blood and blood products, and in individuals at increased risk of blood-borne virus infections.
Subjects and Methods
Subjects and Patients Blood donors. From a prospective study on PT-NANBH, conduct-
ed in 1984-86 [8, 151, stored frozen (-20 to -30°C) serum samples of 4,900 blood donations from 4,123 blood donors were available for anti-HCV testing. Since some donors were represented by more than one donation sample, form each donor only the anti-HCV test results and the historical data, i.e. donor history of jaundice, presence of antibodies to hepatitis B core antigen (anti-HBc), and ALT levels, of the first available donation during the 1984-86 PT-NANBH study [15] were included in the present study.
Fresh unfrozen serum samples, obtained in June 1989 from 1,311 consecutive blood donors to the Amsterdam Blood Bank, were tested for anti-HCV, anti-HBc and ALT (see ‘Techniques’). Stored serum samples of 481 blood donors from Surinam were tested for anti-HCV.
Hepatitis Patients. Stored serum samples from 71 hepatitis patients (ALTr2.5 x upper limit of normal), obtained during the acute phase of illness, were available for anti-HCV testing. In addition, anonymous standardized forms were available, describing risk factors for viral hepatitis, and results of previously performed tests: ALT, hepatitis B surface antigen (HBsAg), IgM antibodies to hepatitis A virus (HAV), IgM antibodies to cytomegalovirus (CMV) and IgM antibodies to Ep- stein-Barr virus (EBV). Acute hepatitis A or B was diagnosed when IgM anti-HAV or HBsAg were present. Acute NANBH was diagnosed when HBsAg, IgM anti-HAV, IgM anti-EBV, or IgM anti-CMV were absent.
Serum samples from 20 patients with previously diagnosed chronic NANBH andor cryptogenic cirrhosis, and from 10 patients previously diagnosed with idiopathic autoimmune chronic hepatitis (AIH), were available for anti-HCV testing. Diagnosis of AIH was based on exclu- sion of HBV or CMV infection, alcohol abuse, drug-induced hepatitis, Wilson’s disease and a,-antitrypsin deficiency, and on the presence of hyperglobulinemia, antinuclear antibodies and a favorable response to corticosteroid therapy. The diagnosis in all 30 chronic hepatitis patients had been confirmed by liver biopsy.
Recipients of Blood or Blood products. Stored serum samples of 213 multi-transfused patients (mainly hemato-oncology patients), and fresh serum samples of 633 hemodialysis patients were tested for anti- HCV. In addition, from the hemodialysis patients, anonymous standar- dized forms including latest results of previously performed ALT tests (including local values for the upper limit of normal) and anti-HBc tests were available.
Stored serum samples from 225 hemophilia (A and B) patients, who received treatment with clotting factor preparations, were available for anti-HCV testing.
Individuals at Risk of Blood-Borne Virus Infections. Stored serum samples of 10 intravenous drug abusers, 119 anti-HIV-positive and 106 anti-HIV-negative homosexual men were tested for anti-HCV.
None of the serum samples had been heat treated, and all study protocols were approved of by an ethics committee.
Techniques Anti-HCV Testing. All sera were tested at 1:lO dilution with the
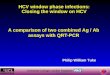
anti-HCV ClOO ELISA, according to the manufacturer’s instructions (Ortho Diagnostics, Raritan, N.J., USA). Cl00 ELISA optical densitiy (OD) reading results were considered reactive when equal to or higher than the cutoff. ClOO ELISA initially reactive samples were retested in duplicate, and were considered positive when in total 2 of 3 test deter- minations were reactive. Of the 1,311 blood donors, the initial anti- HCV ClOO ELISA ratios (OD reading, divided by the cutoff value) were calculated in order to compare the Cl00 ELISA results. ClOO ELISA ratios were plotted in a histogram, indicating on the X axis the cutoff value at ClOO ELISA ratio = 1 (fig. 1).
All anti-HCV ClOO ELISA-positive samples were retested with RIBA (Ortho) according to the manufacturer’s instructions. Sera reac- ting with both the 5-1-1 and the ClOO antigens were regarded as RIBA positive, those reacting with just one were RIBA indeterminate, and sera that reacted with neither antigen were RIBA negative [12,13]. In

Van der Poel et al. 32
Fig. 1. Distribution of ALT and anti-HCV test results of 1,311 blood donors. The cutoff for ALT is mean log + 2 SD, the cutoff for anti- HCV is according to the manufacturer’s instructions.
addition, to exclude reactivity to human superoxide dysmutase (SOD), employed in the manufacturing of the anti-HCV ClOO ELISA, as a cause for false-positive anti-HCV ClOO ELISA reactivity, SOD is repre- sented on the RIBA strip as a separate antigen. Sera that reacted with SOD and one or more viral antigens were regarded as indeterminate, sera that reacted with SOD only were regarded as RIBA negative.
Additional ALT and Anti-HBc Testing. The fresh serum samples from 1,311 blood donors (obtained in 1989) were also tested for ALT with an Abbott W single-channel blood chemistry analyzer at 37”C, with the cutoff defined at 2 standard deviations above the mean log [16] (fig. l), and for anti-HBc antibodies with a RIA (Corab, Abbott, Chi- cago, Ill., USA), according to the manufacturer’s instructions; initially anti-HBc reactive samples were retested once and were considered positive when repeatedly reactive.
Statistical Methods Statistical methods included Yates’ corrected x’ test, and 2-tailed
Fisher’s exact test.
Results
Blood Donors (table 1) Of stored sera, collected in 1984-1986 from 4,123 blood
donors, 30 (0.7%) were anti-HCV ClOO ELISA positive, and 4 (0.1%) of these were also positive with RIBA. Of the 4,123 blood donors, 159 (3.9%) had an ALT > 2 SD + mean log. Of 159 blood donors with ALT I 2 SD + mean log, 3 (1.9%), and of 3,964 blood donors with ALT 2 2SD + mean log, 1(0.03%) were ClOO ELISA plus RIBA positive (p<O.OOl x’). Of 4,123 blood donors, 67 (1.6%) were anti- HBc positive, but none of these anti-HBc positive blood donors were anti-HCV ClOO ELISA positive. Of 3,909 of 4,123 (94.8%) blood donors, it was known whether the donor had a history of jaundice, and 220 of 3,909 (5.6%) blood donors were associated with a history of jaundice before 18years of age, and 61 (1.6%) with a history of jaundice after the age of 18. Blood donors with a history of jaundice after the age of 18 years were significantly (pC0.05, x’) more often anti-HCV ClOO ELISA plus RIBA positive than blood donors without a history of jaundice (table 2).
Of 1,311 fresh sera from blood donors collected in 1989,9 (0.7%) were anti-HCV ClOO ELISA positive, and 1 (0.1%) of these was also positive with RIBA. Of the 1,311 blood donors, 41 (3.1%) had an ALT 2 2 SD above the mean log, and 23 (1.8%) were anti-HBc positive. In this subset, all 41 blood donors with an elevated ALT level, and all 23 blood donors with anti-HBc, were anti-HCV ClOO ELISA nega- tive. The distributions of the anti-HCV ClOO ELISA ratios and of the ALT test results of these 1,311 donors are shown in figure 1.
Of 481 stored sera of blood donors from Surinam, 25 (5%) were anti-HCV ClOO ELISA positive, and 2 (0.4%) of these were also positive with RIBA.
The prevalence of RIBA-confirmed anti-HCV antibod- ies in blood donors from Surinam was not significantly different by x’ from the prevalence in Amsterdan blood donors, either in the subset of 1984-86 or in the subset of 1989.
Patients with Hepatitis Of 26 patients with acute hepatitis A, 11 were intrave-
nous drug abusers, 9 of whom were anti-HCV ClOO ELISA positive, and 8 (72.7%) of these were also positive with RIBA. The remaining 15 patients with acute hepatitis A were all anti-HCV ClOO ELISA negative.
Of 26 patients with acute hepatitis B, 5 were intravenous drug abusers, 4 of whom were anti-HCV ClOO ELISA posi- tive, and 2 (40%) of these were also positive with RIBA.

Prevalence of Anti-HCV in the Netherlands 33
Table 1. Prevalence of RIBA-confirmed anti-HCV antibodies in various population subsets in the Netherlands
Population studied n ELISA positive RIBA result on ELISA-positive samples RIBA positive of ELISA positive
n % positive indeterminate negative %
n % n % n %
Blood donors Amsterdam (1984-1986) 4,123 30 0.7 4 0.1 8 0.2 18 0.4 13 Blood donors Amsterdam (1989) 1,311 9 0.7 1 0.1 4 0.3 4 0.3 11 Blood donors from Surinam 481 25 5.2 2 0.4 2 0.4 21 4.4 8 Multitransfused patients 213 19 0.9 2 0.9 3 1.4 14 6.6 11 Hemodialysis patients 633 28 4.4 15 2.4 9 1.4 4 0.6 54 Hemophilia (A or B) patients 225 179 79.6 150 66.6 21 9.3 8 3.6 84 Intravenous drug abusers 10 8 80 4 4 0 0 4 40 50 Anti-HIV-positive homosexual men 119 18 15.1 2 1.7 0 16 13.4 11 Anti-HIV-negative homosexual men 106 2 1.9 0 0 2 1.9 Acute NANBH 19 6 31.6 3' 15.8 1 5.3 2 10.5 50 Chronic NANBH andor cryptogenic cirrhosis 20 13 65 8 4 0 5 25 0 62 AIH 10 4 40 1 10 1 10 2 20 25
2 of 3 RIBA-positive samples were from intravenous drug abusers.
Table 2. Donor history of jaundice as a cofactor for anti-HCV negative. Of the total number of 19 patients with acute NANBH, 3 (15.7%) were anti-HCV ClOO ELISA plus RIBA positivity (n = 3,909)
RIBA positive (table 1). Of 20 patients with chronic HANBH andor cryptogenic
cirrhosis, 13 (65%) were anti-HCV C l O O ELISA positive
Donor history n ELISA + VE ELISA + VE and RIBA + VE
n % n % and 8 (40%) of these were also positive with RIBA. The biomies of these 20 Datients showed cirrhosis andor chron- ic active hepatitis i n i l cases (6 of 11 ClOO ELISA plus RIBA positive), and chronic persistent hepatitis in 9 cases (2 of 9 ClOO ELISA plus RIBA positive; not significant, Fisher's
1.64
No jaundice 3,628 22 0.61 2 Jaundice <18years 220 4 1.82 0 Jaundice 318years 61 2 3.28 1 Total 3,909 28 0.72 3 0.08
0.06 1 * exact). Of 10 patients with AIH, 4 (40%) were anti-HCV ClOO ELISA positive, and 1 (10%) of these was also positive with RIBA (table 1).
*p<O.O5 (x2 ) ; *VE=positive.
The remaining 21 patients with acute hepatitis B were all anti-HCV ClOO ELISA negative. Of the total number of 52 patients with acute hepatitis A or B, 16 (31%) were in- travenous drug abusers; 10 (62.5%) of whom were anti- HCV ClOO ELISA plus RIBA positive.
Of 19 patients with acute NANBH, 6 were intravenous drug abusers, 4 of whom were anti-HCV ClOO ELISA posi- tive, and 2 (33%) of these were also positive with RIBA. None of the remaining 13 patients with acute NANBH were intravenous drug abusers or received blood product trans- fusions, and 2 of these were anti-HCV ClOO ELISA posi- tive, one of which was RIBA positive and one was RIBA
Recipients of Blood or Blood Products Of 213 stored serum samples of multitransfused pa-
tients, 19 (9%) were anti-HCV ClOO ELISA positive, and 2 (0.9%) of these were also positive with RIBA.
Of 633 hemodialysis patients, 28 (4%) were anti-HCV ClOO ELISA positive, and 15 (2.4%) of these were also positive with RIBA (table 1). ALT values, including local upper limit of normal (ULN) were known in 533 hemodia- lysis patients, 19 (4%) of whom had an ALT L 1.5 x ULN. Of 19 hemodialysis patients with ALT 2 l S x U L N , 3 (15.8%), and of 514 hemodialysis patients with ALT C 1.5 x ULN, 12 (2.3%) were ClOO ELISA plus RIBA posi- tive (p<0.01x2). The anti-HBc status was reported in 83

34 Van der Poel et al.
hemodialysis patients, 32 (39%) of whom were anti-HBc positive. Of 32 anti-HBc-positive hemodialysis patients, 1 (3.1%), and none of 51 anti-HBc-negative patients were ClOO ELISA plus RIBA positive (not significant, x’).
Of 225 patients with hemophilia A or B, 179 (79.5%) were anti-HCV ClOO ELISA positive, and 150 (66.6%) of these were also positive with RIBA (table 1).
Individuals at Risk of HIV Infection Of 10 intravenous drug abusers, 8 (80%) were anti-HCV
ClOO ELISA positive, and 4 (40%) of these were also posi- tive with RIBA. Of 119 anti-HIV-positive homosexual men, 18 (15%) were anti-HCV ClOO ELISA positive, and 2 (1.7%) of these were also positive with RIBA. Of 106 anti- HIV-negative homosexual men, 2 (2%) were anti-HCV ClOO ELISA positive, all of whom were RIBA negative. The difference in prevalence of ClOO ELISA plus RIBA positivity in anti-HIV-positive and anti-HIV-negative ho- mosexual men was not significant (x’) (table 1).
Discussion
Our study shows that in the Netherlands, anti-HCV antibodies are prevalent in low- as well as in high-risk populations for blood-borne virus infections.
Bearing in mind that the combination of both RIBA and ClOO ELISA positivity is of limited sensitivity [El, the here presented prevalences of RIBA-confirmed anti-HCV anti- bodies may underestimate the true prevalences of HCV infection. Stored sera from Amsterdam blood donors, col- lected in 1984-86, as well as fresh sera collected in 1989, showed a similar prevalence of anti-HCV ClOO ELISA (0.7%) and RIBA (0.1%) positivity. It therefore seems un- likely that storage of the serum samples significantly influ- enced the anti-HCV antibody test results.
We have described that the presence of elevated ALT levels in anti-HCV ClOO ELISA-positive blood products is predictive of infectious HCV carriership [8]. In conjunc- tion with these findings, a positive correlation of RIBA- confirmed anti-HCV positivity with elevated ALT levels was found in the subsets of blood donors from 1984-86 and in the subset of hemodialysis patients. The lack of this correlation in the subset of 1,311 blood donors from 1989 can be ascribed to the relatively smaller sample size. Anti- HBc positivity did not correlate with the presence of RIBA-confirmed anti-HCV, which is consistent with the reported lack of significance of anti-HBc testing for the prevention of PT-NANBH in the Netherlands [15]. Blood donors with a history of jaundice after 18 years of age were
significantly more often anti-HCV ClOO ELISA plus RIBA positive than donors without such a history. However, since only 1.6% of the blood donors with a history of jaundice after 18 years of age were RIBA-confirmed anti- HCV positive, rejection of blood donors with a history of jaundice will not be very cost effective in preventing HCV transmission to recipients.
In epidemiological studies of European blood donors, the anti-HCV ClOO ELISA prevalence shifts from 0 .247% in Northern Europe to 0.8-1.4% in the Mediterranean area [17-191. In subtropical countries, a higher prevalence can therefore be expected. In the present study, the prevalence of RIBA-confirmed anti-HCV antibodies in blood donors from Surinam tended to be higher than in Amsterdam blood donors; however, the difference was not significant.
In our study, 15% of the NANBH patients were found anti-HCV ELISA plus RIBA positive in the acute phase of illness, and 40% in the chronic phase. Our ClOO ELISA results in these subsets of 32 and 65% respectively, accord with the ELISA results of others [5, 6, 9, 20, 211. It is not clear why the prevalence of anti-HCV in the acute phase is that low. It is known that antibodies to the ClOO antigen can develop as late as 12 months after infection by blood trans- fusion [5, 91. Also, the ClOO antigen represents only ap- proximately 12% of the HCV genome [4, 51, and it is con- ceivable that by employment of other immunogenic HCV antigens more patients are found anti-HCV positive. The finding that a proportion of patients, diagnosed with AIH, are anti-HCV ELISA positive, was also observed by others [6, 221. Since the diagnosis of AIH is usually made by exclusion of other causes of hepatitis, combined with the presence of autoimmune phenomena, overlap with cases of HCV infection remains possible. Discrimination between HCV infection and autoimmune disease is of clinical im- portance, since a proportion of the HCV patients respond well to treatment with interferons [23, 241.
Recipients of blood products are at increased risk of HCV infection. Retrospectively studied patients who re- ceived multiple transfusions, and prospectively followed open heart surgery patients [12] were found anti-HCV ClOO ELISA plus RIBA positive in 1% of the cases. The high risk of NANBH in hemophilia patients, which was known be- fore anti-HCV testing became available [3], is now clearly established. Our prevalence rate of 80% for anti-HCV ClOO ELISA positivity in hemophiliacs is in conjunction with other studies [6,20,25,26], and we show that 67% of these patients are confirmed anti-HCV positive by RIBA. Adequately virus-inactivated clotting factor preparations are fortunately now available to hemophilia patients [25]. Hemodialysis patients were found anti-HCV ClOO ELISA

Prevalence of Anti-HCV in the Netherlands 35
positive in 4% of the cases, and in total 2.4% were also RIBA confirmed. This accords with anti-HCV ClOO ELISA prevalences of 1 4 % in the United Kingdom and in Germa- ny [20,27]. In Spain, an anti-HCV ClOO ELISA prevalence of 20% was observed in hemodialysis patients, and 90% of the anti-HCV ELISA-positive patients received blood transfusions [6]. Whether hemodialysis patients in the Netherlands acquire HCV by the hemodialysis procedures as such, or whether the main risk is constituted by blood transfusions, is under further study.
The blood-borne character of HCV infection is further supported by the high prevalence of RIBA-confirmed anti- HCV (40%) antibodies among intravenous drug abusers, apparently caused by needle sharing [6,27].
Sexual transmission of NANBH virus has also been re- ported [28], but seem less efficient than sexual transmission of HIV or HBV [6]. In anti-HIV-negative homosexual men, the prevalence appears to be low, which was also observed by others [27]. A higher prevalence in anti-HIV- positive homosexual men (26% with ClOO ELISA) was also reported [27] and may indeed reflect an increased risk of sexual transmission of HCV in this group, but could also be caused by interaction of HIV and HCV, rendering these individuals more susceptible to HCV infection [29]. How- ever, in our study populations the prevalence of RIBA- confirmed anti-HCV in anti-HIV-positive and anti-HIV- negative homosexual men was not significantly different.
Finally, as described elsewhere, mother-to-infant trans- mission of HCV does not seem to play an important role [30]. An unanswered question therefore remains how indi- viduals, without a history of parenteral blood contact, ac- quire HCV infection.
The predictive value of the ClOO ELISA increases with a higher prevalence of HCV infection in a given population. We conclude that 8-13% of the ClOO ELISA-positive indi- viduals in low-risk populations (blood donors) are RIBA- confirmed positive, as compared to 5680% of individuals at increased risk (hemodialysis patients, hemophiliacs, in- travenous drug abusers and NANBH patients).
Acknowledgements
We thank Ortho Diagnostics for anti-HCV tests, members of the Dialysis Group The Netherlands, and further Dr. P. L. M. Jansen, Dr. D. J. van Leeuwen, Dr. J.C. Roos, Dr. J. H. Ten Veen, Dr. P. Stevens, Dr. A. Van der Putten, Dr. P. van Munster, Dr. L. W. Statius van Eps, and Dr. R.N.I. Pietersz for their contributions to the serum panel, Prof. Dr. W. G. Van Aken and Prof. Dr. R. A. Coutinho for comments on the manuscrtipt, and Miss A. Roukens and Mr. F. Feijen for the preparation of the typescript.
~
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
17
18
19
20
References
Reesink HW, Van der Poel CL: Blood transfusion and hepatitis: Still a threat? Blut 1989;58:1-6. Alter HJ: Chronic consequences of non-A, non-B hepatitis; in Seeff LB, Lewis JH (eds): Current Perspectives in Hepatology. New York, Plenum Medical, 1989, pp 83-89. Hay CRM, Preston FE, Triger DR, et al: Progressive liver disease in haemophilia, an understated problem? Lancet 1985;i: 1495-1498. Choo Q-L, Kuo G, Weiner AJ, et al: Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science 1989;244:359-362. Kuo G, Choo Q-L, Alter HJ, et al: An assay for circulating antibod- ies to a major etiologic virus of human non-A, non-B hepatitis. Science 1989;244:362-364. Esteban JI, Estaban R, Viladomiu L, et al: Hepatitis C virus anti- bodies among risk groups in Spain. Lancet 1989;ii:294-296. Van der Poel CL, Reesink HW, Lelie PN;et al: Anti-hepatitis C antibodies and non-A, non-B post-transfusion hepatitis in The Netherlands. Lancet 1989;33:297-298. Van der Poel CL, Reesink HW, Schaasberg W, et al: Infectivity of blood seropositive for hepatitis C virus antibodies. Lancet 1990;335:558-560. Alter HJ, Purcell RH, Shih JW, et al: Detection of antibody to hepatitis C virus in prospectively followed transfusion recipients with acute and chronic non-A, non-B hepatitis. New Engl J Med
Estaban JI, Gonzales A, Hernandez JM, et al: Evaluation of anti- bodies to hepatitis C virus in a study of transfusion-associated hepa- titis. New Engl J Med 1990;323:1107-1112. Garson JA, Tedder RS, Briggs M, et al: Detection of hepatitis C viral sequences in blood donations by ‘nested’ polymerase chain reaction and prediction of infectivity. Lancet 1990;335: 1419-1422. Van der Poel CL, Reesink HW, Lelie PN, et al: Anti-HCV and transaminase testing of blood donors. Lancet 1990;336: 187-188. Ebeling F, Naukkarinen R, Leikola J: Recombinant immunoblot assay for hepatitis C antibody as predictor of infectivity. Lancet
Weiner AJ, Kuo G, Bradley DW, et al: Detection of hepatitis C viral sequences in non-A, non-B hepatitis. Lancet 1990;335: 1-3. Reesink HW, Leentvaar-Kuypers A, Van der Poel CL, et al: Non-A, non-B posttransfusion hepatitis in open heart surgery pa- tients in The Netherlands: Preliminary results of a prospective study; in Zuckerman AJ (ed): Viral Hepatitis and Liver Disease. Liss, 1988, New York, pp 558-560. Steane EA: Recommendations on surrogate testing for non-A, non-B hepatitis. American Association of Blood Banks, 1987,
Janot C, CourouCe AM, Maniez M: Antibodies to hepatitis C virus in French blood donors. Lancet 1989;ii:796-797. Kuhnl P, Seidl S, Stangel W, et al: Antibody to hepatitis C virus in German blood donors. Lancet 1989;ii:324. Sirchia G, Bellobuono A, Giovanetti A, et al: Antibodies to hepati- tis C virus in Italian blood donors. Lancet 1989;ii:797. Roggendorf M, Deinhardt F, Rasshofer R, et al: Antibodies to hepatitis C virus. Lancet 1989;ii:324-325.
1989;321:1491-1500.
1990;335 :982-983.
pp 2-3.
21 Colombo M, Kuo G, Choo Q-L, et al: Prevalence of antibodies to hepatitis C virus in Italian patients with hepatocellular carcinoma. Lancet 1989;ii: 1006-1008.

36 Van der Poel et al.
22
23
24
25
26
27
28
Lenzi M, Ballardini G, Fusconi M, et al: q p e 2 autoimmune hepa- titis and hepatitis C virus infection. Lancet 1990;335:258-259. Di Bisceglie AM, Martin P, Kassianides C, et al: Recombinant interferon alfa therapy for chronic hepatitis C. New Engl J Med 1989;321:1506-1510. Davis GL, Balart LA, Schiff ER, et al: Treatment of chronic hepati- tisC with recombinant interferon alfa. New Engl J Med
Noel L, Guerois C, Maisonneuve P, et al: Antibodies to hepatitis C virus in haemophilia. Lancet 1989;ii:560. Ludlam CA, Chapman D, Cohen B, et al: Antibodies to hepatitis C virus in haemophilia. Lancet 1989;ii:560-561. Mortimer PP, Cohen BJ, Litton PA, et al: Hepatitis C virus anti- body. Lancet 1989;ii:798. Alter MJ, Coleman PJ, Alexander WJ, et al: Importance of hetero- sexual activity in the transmission of hepatitis B and non-A, non-B hepatitis. JAMA 1989;262: 1201-1205.
1989;321:1502-1506.
29 Giovanni M, Tagger A, Ribero ML, et al: Maternal-infant trans- mission of hepatitis C virus and HIV infections: A possible interac- tion. Lancet 1990;335:1166.
30 Reesink HW, Wong VCW, Ip HMH, et al: Mother-to-infant trans- mission and hepatitis C virus. Lancet 1990;335: 1216-1217.
Received: June 19,1990 Revised manuscript received: December 19,1990 Accepted: December 28,1990
C.L. van der Poel, MD Red Cross Blood Bank Amsterdam PO Box 9137 NL-1006 AC Amsterdam (The Netherlands)
Recommended