Selecting Outcome Metrics for Your Outpatient Practice:
An ICF-Based Approach
Presenters:
David Berbrayer, MD,
Amy Houtrow, MD, PhD, MPH;
Armando Miciano, MD;
M. Elizabeth Sandel, MD (Director);
Deepthi Saxena, MD
2014 AAPMR Annual Assembly, San Diego CA, 2014 Nov 15
Learning objectives:1. Define foundational concepts of the ICF that serve as a guide for the choice of PM&R outcome metrics2. Understand variety of resources available for selection of outcome metrics for PM&R patient populations3. Incorporate outcome measurement into outpatient practices for a variety of patient populations to enhance physiatric care using core sets of measures
Selecting Outcome Metrics for Your Outpatient Practice: An ICF-Based Approach
Outcome Core Set – Chronic Low Back Pain
Section Presenter: Armando Miciano, MDNevada Rehabilitation Institute
Las Vegas, NV
2014 AAPMR Annual Assembly, San Diego CA, 2014 Nov 15
Medical Director Spring Mountain Rehab, Las Vegas NV
Practitioner – Nevada Rehabilitation Institute, Las Vegas NV
Disclosures
1. David Berbrayer MD (Performance Metrics Committee member)
2. Edwin Capulong MD3. Kush Goyal MD4. Martin Grabois MD (Co-leader)5. Armando Miciano MD (Clinical Practice
Guideline Committee member)6. Joshua Scheidler MD7. Deborah Venesy MD (Co-leader)
Acknowledgments – CLBP QTB Subject Matter Experts:
Most common assessment: ◦ Evaluation of underlying impairment & pathology
Specialists performing evaluations for MSK disorders will be best served when they can:
◦ Assess the individual's functional status ◦ Incorporate that information into their decision
regarding the individual's current limitations and prognosis
In addition to the evaluation of the underlying impairment and pathology. [1]
INTRODUCTION
[1] Greenough CG. Eur Spine J. 2006.
Many of the factors contributing to the evaluation of functional status are necessarily subjective ◦ e.g. pain, physical functioning, and affective status
Nonetheless, the literature suggests that inclusion of functional assessment into the [MSK] disability determination using a patient-centered approach may provide the factors that are most potent with respect to patient prognosis and care planning. [1]
Functional Status
[1] Linn RT, Granger CV, et al. Phys Med Rehabil Clin N Am. 2001.
DEFINITION: The field of developing, evaluating &
applying measurement instruments
Undergone considerable progress in MSK medicine [1].
How should clinicians measure “Patient-centered Outcomes?”
INTRODUCTION – Performance Metrics
[1] Mooney V, et al. Spine J. 2010 May;10(5):433-40.
How is recovery from low back pain measured?
A systematic review of the literature
BACKGROUND: ◦ No accepted definition of what recovery involves or
guidance as to how it should be measured. OBJECTIVE:
◦ To appraise the LBP literature (last 10 years) to review the methods used to measure recovery.
RESEARCH DESIGN: ◦ All prospective studies of subjects with non-specific
LBP that measured recovery as an outcome
INTRODUCTION – Progress in Performance Metrics
Kamper SJ, et al. Eur Spine J. 2011.
How is recovery from low back pain measured? A systematic review of the literature
RESULTS:
◦ 82 included studies used 66 different measures of recovery ◦ 17 measures used pain as a proxy for recovery, ◦ 7 used disability or function ◦ 17 based on a combination of two or more constructs. ◦ 9 single-item recovery rating scales ◦ 11 studies used a global change scale that included an anchor
of ‘completely recovered’ ◦ 3 measures used return to work as the recovery criterion◦ 2 used time to insurance claim closure ◦ 7 used physical performance
INTRODUCTION – Progress in Performance Metrics
Kamper SJ, et al. Eur Spine J. 2011.
How is recovery from low back pain measured? A systematic review of the literature
CONCLUSIONS:
◦ Almost every study that measured recovery from LBP in the last 10 years did so differently
Lack of consistency makes interpretation &
comparison of the LBP literature problematic.
◦ That the failure to use a standardized measure of recovery is due to the absence of an established definition
INTRODUCTION – Which PRO to use?
Kamper SJ, et al. Eur Spine J. 2011.
Despite progress in PERFORMANCE METRICS, the appreciation of the complex interrelationship between:
◦ Physical ◦ Psychological ◦ Social effects
of MSK disorders is incompletely explored in clinical practice. [1]
Another Challenge
[1] Mayer T, et al. Spine J. 2003 May-Jun;3(3 Suppl):28S-36S. Review.
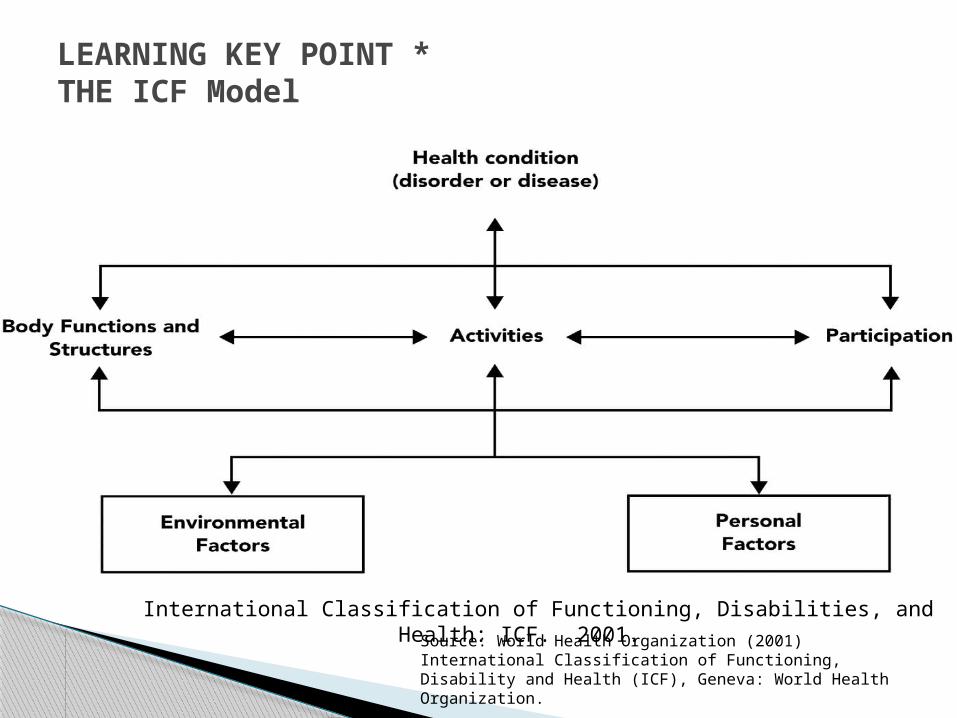
LEARNING KEY POINT *THE ICF Model
International Classification of Functioning, Disabilities, and Health: ICF. 2001. Source: World Health Organization (2001) International Classification of
Functioning, Disability and Health (ICF), Geneva: World Health Organization.
Impairments: problems in body function or structure such as
significant deviation or loss
Activity limitations: difficulties an individual may have in executing
activities.
Participation restrictions:problems an individual may experience in
involvement in life situations.
Rondelli, RD. PM&R. 2009.
Review articles Knowledge Now articles
Clinical practice guidelines
Core constructs specific for the health condition
Assessment instruments
Quality metrics Patient education materials
Checklists
Tools in the Quality Toolbox (QTB)
1. Chapman JR, Norvell DC, et al. Evaluating common outcomes for measuring treatment success for chronic low back pain. Spine (Phila Pa 1976). 2011 Oct 1; 36(21 Suppl):S54-68.
2. Cleland J, Gillani R, Bienen EJ, Sadosky A. Assessing dimensionality and responsiveness of outcomes measures for patients with low back pain. Pain Pract. 2011 Jan-Feb; 11(1):57-69.
3. DeVine J, Norvell DC, et al. Evaluating the correlation and responsiveness of patient-
reported pain with function and quality-of-life outcomes after spine surgery. Spine (Phila Pa 1976). 2011 Oct 1;36(21 Suppl):S69-74.
4. Deyo RA, Dworkin SF, et al. Report of the NIH Task Force on research standards for chronic low back pain. Pain Med. 2014 Aug; 15(8):1249-67.
5. Freiberger E, et al. Performance-based physical function in older community-dwelling persons: a systematic review of instruments. Age Ageing 2012; 41: 712–721.
6. Ghogawala Z, Resnick DK, et al. Guideline update for the performance of fusion procedures for degenerative disease of the lumbar spine. Part 2: assessment of functional outcome following lumbar fusion. J Neurosurg Spine. 2014 Jul; 21(1):7-13.
7. McCormick JD1, Werner BC, Shimer AL. Patient-reported outcome measures in spine surgery. J Am Acad Orthop Surg. 2013 Feb;21(2):99-107.
8. Schoenfeld AJ, Bono CM. Measuring spine fracture outcomes: common scales and checklists. Injury. 2011 Mar;42(3):265-70.
QTB: Review Articles
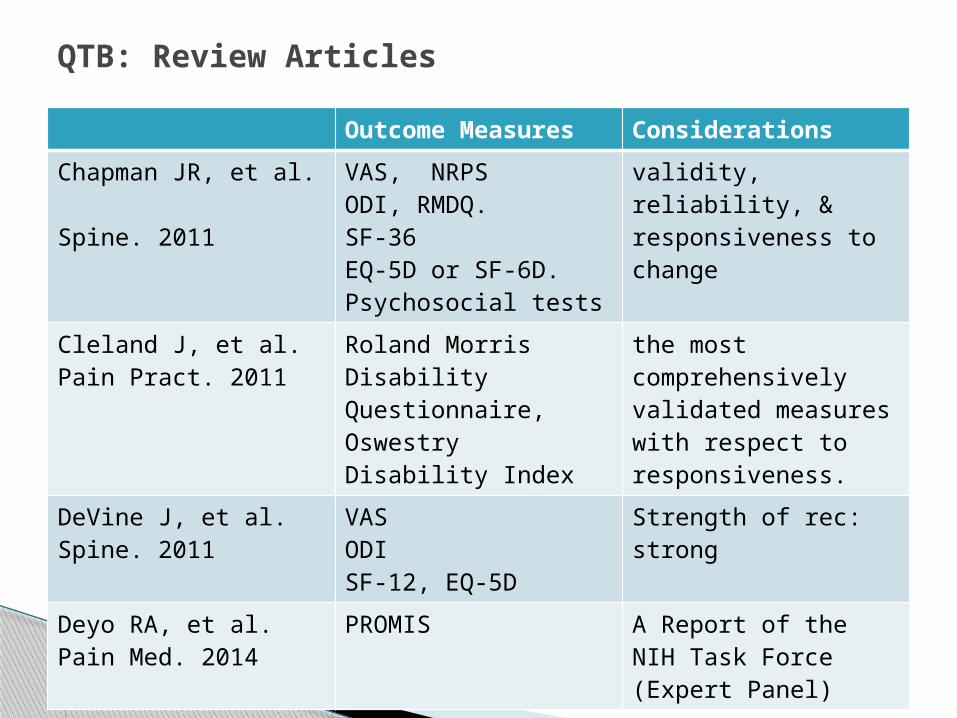
Outcome Measures Considerations
Chapman JR, et al. Spine. 2011
VAS, NRPSODI, RMDQ.SF-36EQ-5D or SF-6D.Psychosocial tests
validity, reliability, & responsiveness to change
Cleland J, et al.Pain Pract. 2011
Roland Morris Disability Questionnaire, Oswestry Disability Index
the most comprehensively validated measures with respect to responsiveness.
DeVine J, et al. Spine. 2011
VASODISF-12, EQ-5D
Strength of rec: strong
Deyo RA, et al. Pain Med. 2014
PROMIS A Report of the NIH Task Force (Expert Panel)
QTB: Review Articles
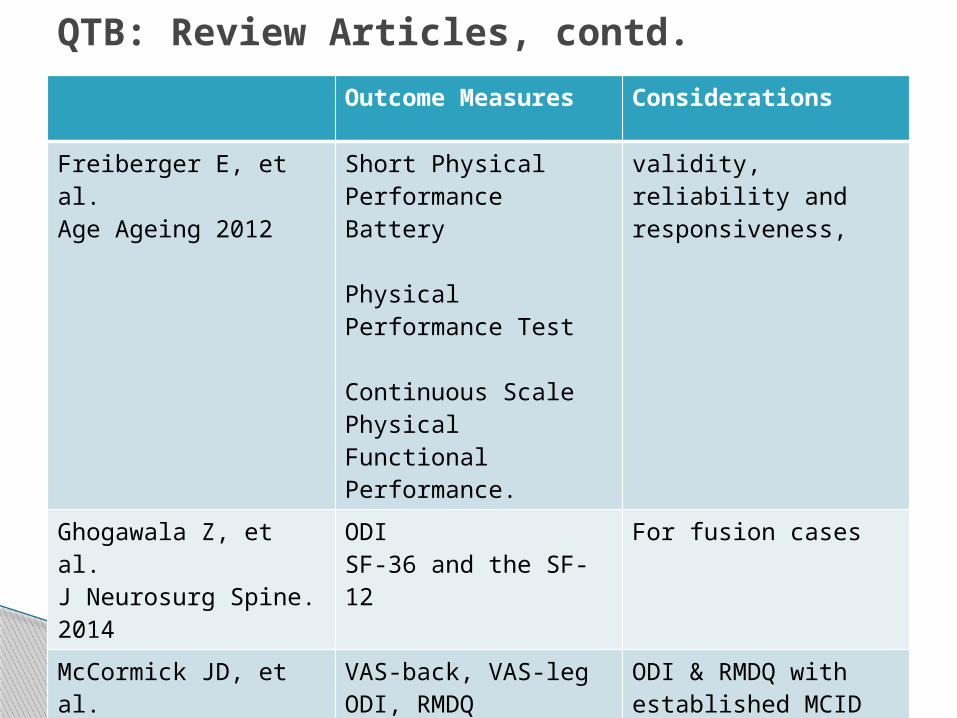
Outcome Measures Considerations
Freiberger E, et al. Age Ageing 2012
Short Physical Performance Battery
Physical Performance Test
Continuous Scale Physical Functional Performance.
validity, reliability and responsiveness,
Ghogawala Z, et al. J Neurosurg Spine. 2014
ODISF-36 and the SF-12
For fusion cases
McCormick JD, et al. J Am Acad Orthop Surg. 2013
VAS-back, VAS-legODI, RMDQEQ-5D, SF
ODI & RMDQ with established MCID
Schoenfeld AJ, et al. Injury. 2011
VASODI, RMDQSF-36
QTB: Review Articles, contd.
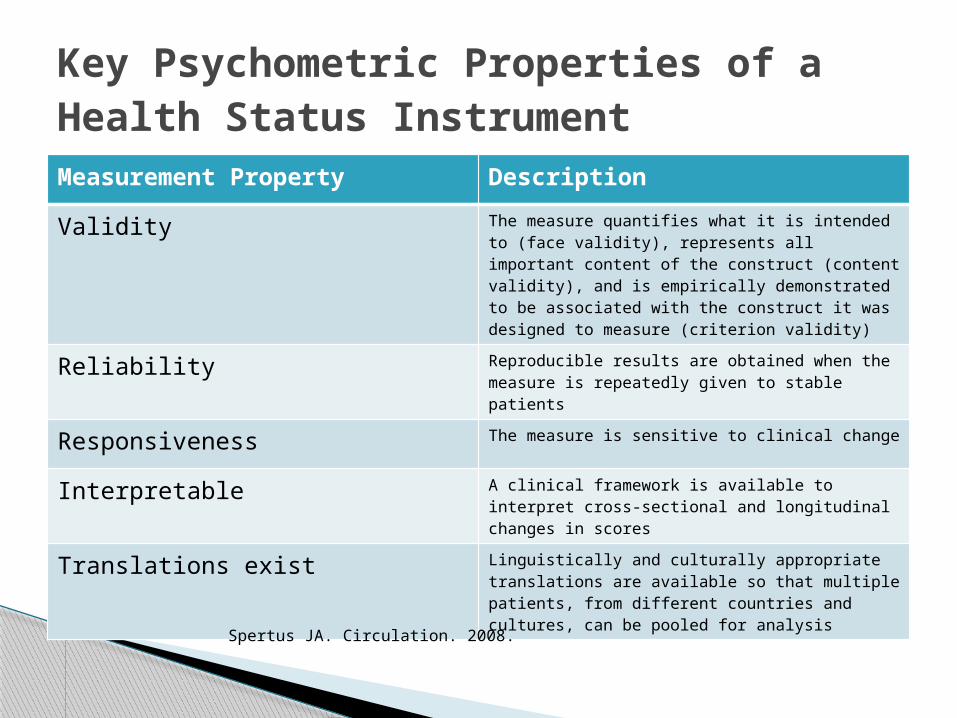
Measurement Property Description
Validity The measure quantifies what it is intended to (face validity), represents all important content of the construct (content validity), and is empirically demonstrated to be associated with the construct it was designed to measure (criterion validity)
Reliability Reproducible results are obtained when the measure is repeatedly given to stable patients
Responsiveness The measure is sensitive to clinical change
Interpretable A clinical framework is available to interpret cross-sectional and longitudinal changes in scores
Translations exist Linguistically and culturally appropriate translations are available so that multiple patients, from different countries and cultures, can be pooled for analysis
Key Psychometric Properties of a Health Status Instrument
Spertus JA. Circulation. 2008.
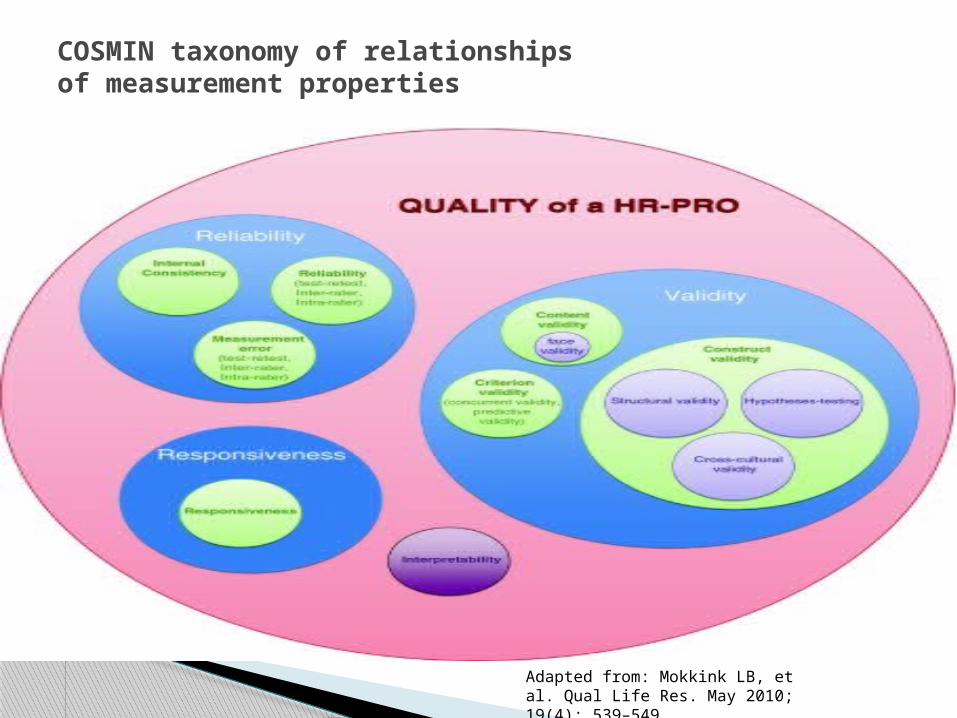
COSMIN taxonomy of relationships of measurement properties
Adapted from: Mokkink LB, et al. Qual Life Res. May 2010; 19(4): 539–549.
1. Carayannopoulos A. Discogenic Lumbar Pain. In: PMR Knowledge NOW [Internet]. 2011 Nov 10 [modified 2013 Jan 24]. c2014 AAPMR. Accessed 10/22/14 at: http://me.aapmr.org/kn/article.html?id=176
2. Everett CR, Ramirez C, Perkowski M. Lumbar Disc disorders. In: PMR Knowledge NOW [Internet]. 2013 Sep 20. c2014 AAPMR. Accessed 10/22/14 at: http://me.aapmr.org/kn/article.html?id=133
3. Nance PW, Chen H. Lumbar stenosis. In: PMR Knowledge NOW [Internet]. 2012 Jul 20 [modified 2013 Jan 23]. c2014 AAPMR. Accessed 10/22/14 at: http://me.aapmr.org/kn/article.html?id=137
4. Spires MC. Inflammatory Arthritides. In: PMR Knowledge NOW [Internet]. 2011 Nov 10 [modified 2012 Dec 27]. c2014 AAPMR. Accessed 10/22/14 at: http://me.aapmr.org/kn/article.html?id=82
QTB: PMR Knowledge NOW *
* Selected ones with discussion on Functional Assessment tools
1. North American Spine Society (NASS). Clinical Guidelines for Multidisciplinary Spine Care Diagnosis and Treatment of Lumbar Disc Herniation with Radiculopathy. c2012 NASS. Accessed 10/22/14 at: https://www.spine.org/Documents/ResearchClinicalCare/Guidelines/LumbarDiscHerniation.pdf
2. North American Spine Society (NASS). Clinical Guidelines for Multidisciplinary Spine Care Diagnosis and Treatment of Degenerative Lumbar Spinal Stenosis. c2011 NASS. Accessed 10/22/14 at: https://www.spine.org/Documents/ResearchClinicalCare/Guidelines/LumbarStenosis.pdf
3. North American Spine Society (NASS). Clinical Guidelines for Multidisciplinary Spine Care Diagnosis and Treatment of Degenerative Lumbar Spondylolisthesis. c2008 NASS. Accessed 10/22/14 at: https://www.spine.org/Documents/ResearchClinicalCare/Guidelines/Spondylolisthesis.pdf
4. American Academy of Orthopedic Surgeons (AAOS). Treatment of Symptomatic Osteoporotic Spinal Compression Fractures. 2010. Accessed 10/22/14 at: http://www.aaos.org/research/guidelines/SCFguideline.pdf
QTB: Clinical Practice Guidelines
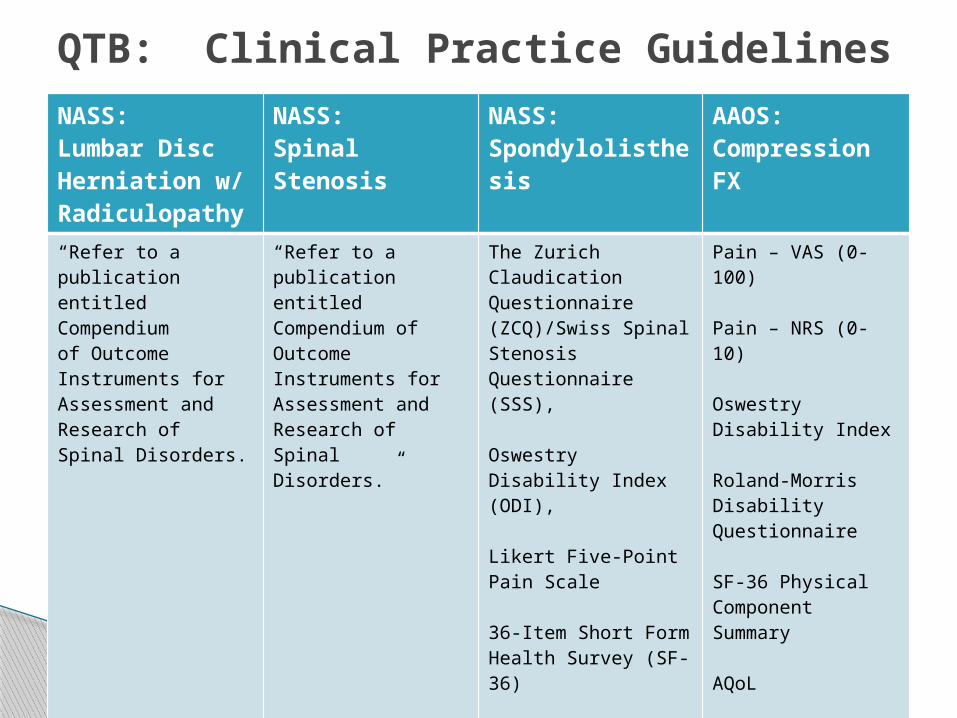
NASS: Lumbar Disc Herniation w/ Radiculopathy
NASS:Spinal Stenosis
NASS:Spondylolisthesis
AAOS:Compression FX
“Refer to a publication entitled Compendiumof Outcome Instruments for Assessment and Research of Spinal Disorders.
“Refer to a publication entitled Compendium of Outcome Instruments for Assessment and Research ofSpinal Disorders.”
The Zurich Claudication Questionnaire (ZCQ)/Swiss Spinal Stenosis Questionnaire (SSS), Oswestry Disability Index (ODI),
Likert Five-Point Pain Scale
36-Item Short Form Health Survey (SF-36)
Pain – VAS (0-100)
Pain – NRS (0-10)
Oswestry Disability Index
Roland-Morris Disability Questionnaire
SF-36 Physical Component Summary
AQoL
EQ-5D
QTB: Clinical Practice Guidelines
1. Symptom quality2. Pain-related impairment 3. Life satisfaction4. Global health status5. Work productivity
Constructs for core sets (for choice of assessment instruments)
[1] Bombardier C. Spine (Phila Pa 1976). 2000.
PRO = Patient-Reported Outcomes – from the “patient”
PBA = Performance Based Assessment - medical search term used also as
outcome measures - clinician-derived objective tests
QTB: Assessment InstrumentsPRO vs. PBA
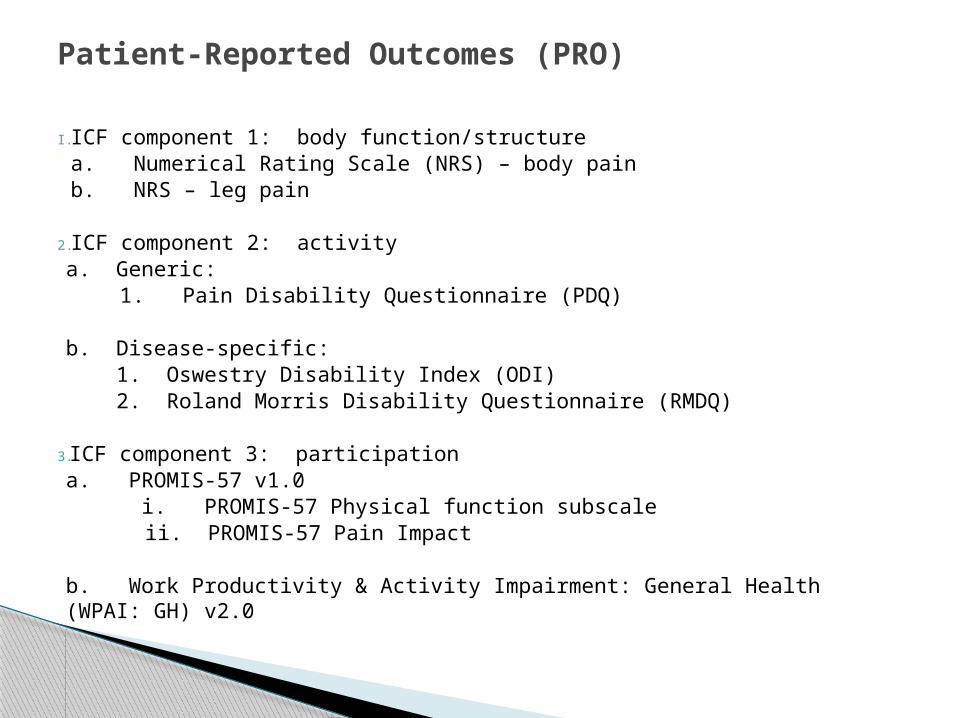
I. ICF component 1: body function/structurea. Numerical Rating Scale (NRS) – body painb. NRS – leg pain
2. ICF component 2: activitya. Generic:
1. Pain Disability Questionnaire (PDQ)
b. Disease-specific: 1. Oswestry Disability Index (ODI) 2. Roland Morris Disability Questionnaire (RMDQ)
3. ICF component 3: participationa. PROMIS-57 v1.0 i. PROMIS-57 Physical function subscale
ii. PROMIS-57 Pain Impact
b. Work Productivity & Activity Impairment: General Health (WPAI: GH) v2.0
Patient-Reported Outcomes (PRO)
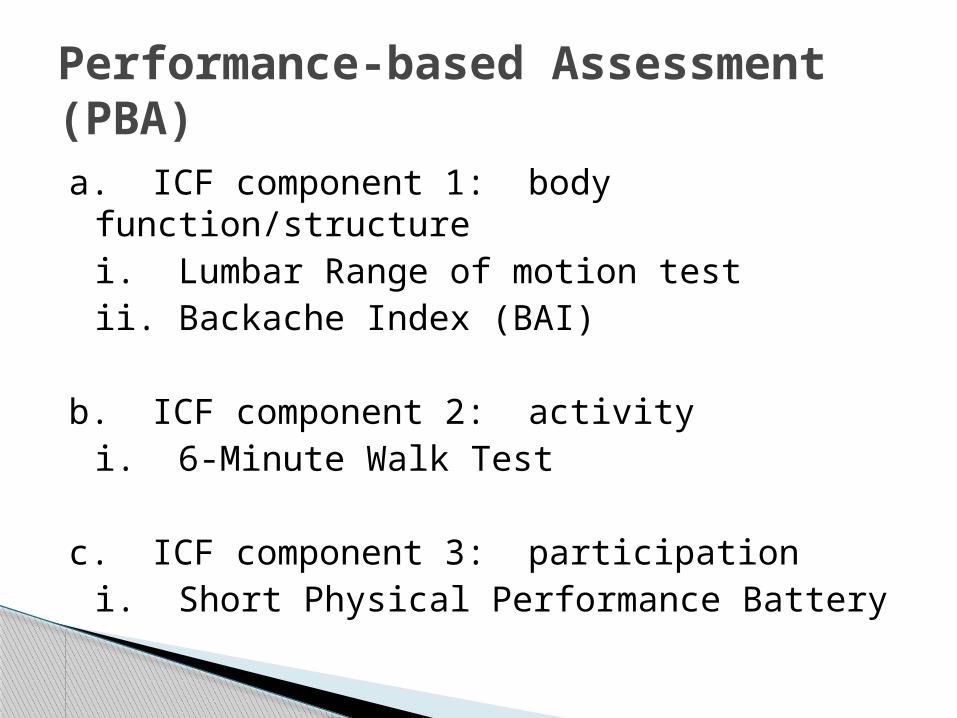
a. ICF component 1: body function/structurei. Lumbar Range of motion testii. Backache Index (BAI)
b. ICF component 2: activityi. 6-Minute Walk Test
c. ICF component 3: participationi. Short Physical Performance Battery
Performance-based Assessment (PBA)
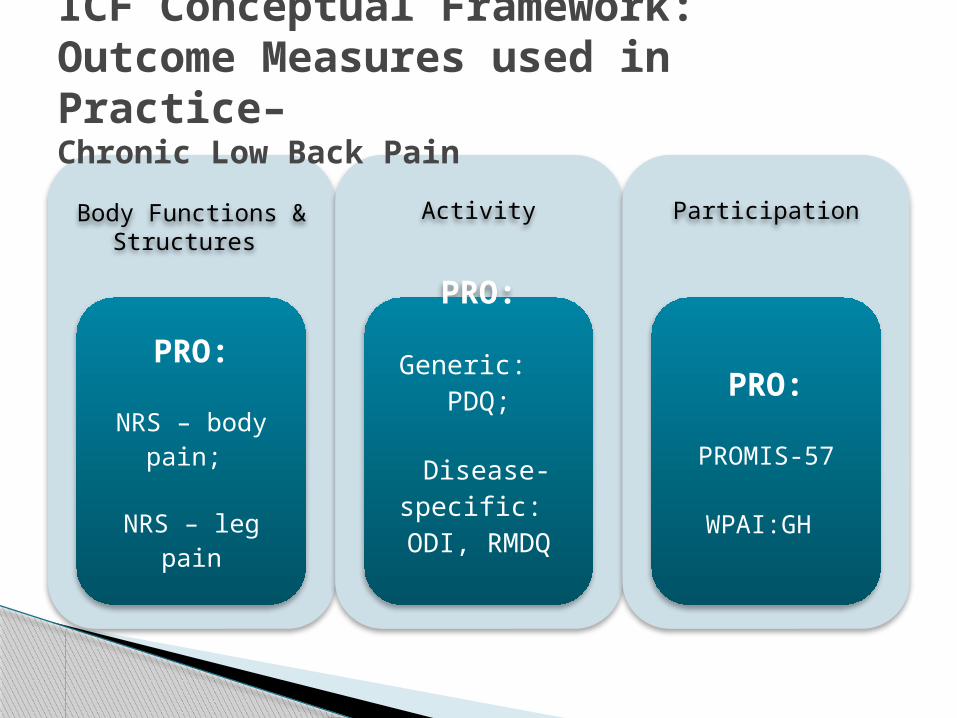
Body Functions & Structures
PRO:
NRS – body pain;
NRS – leg pain
Activity
PRO:
Generic: PDQ;
Disease-specific:
ODI, RMDQ
Participation
PRO:
PROMIS-57
WPAI:GH
ICF Conceptual Framework: Outcome Measures used in Practice– Chronic Low Back Pain
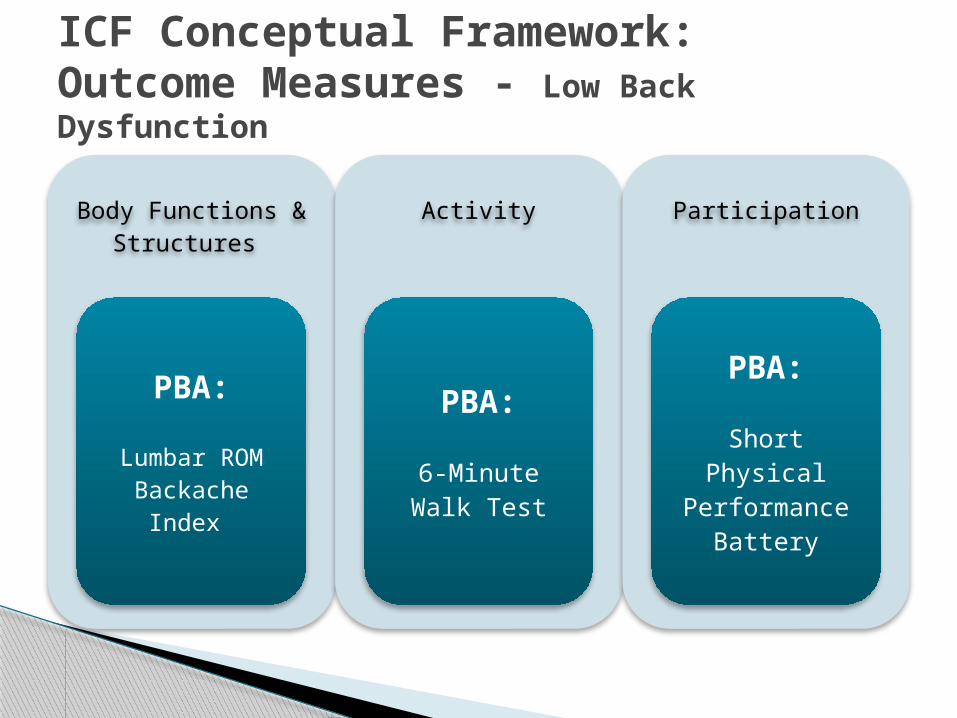
Body Functions & Structures
PBA:
Lumbar ROMBackache
Index
Activity
PBA:
6-Minute Walk Test
Participation
PBA:
Short Physical Performance
Battery
ICF Conceptual Framework: Outcome Measures - Low Back Dysfunction
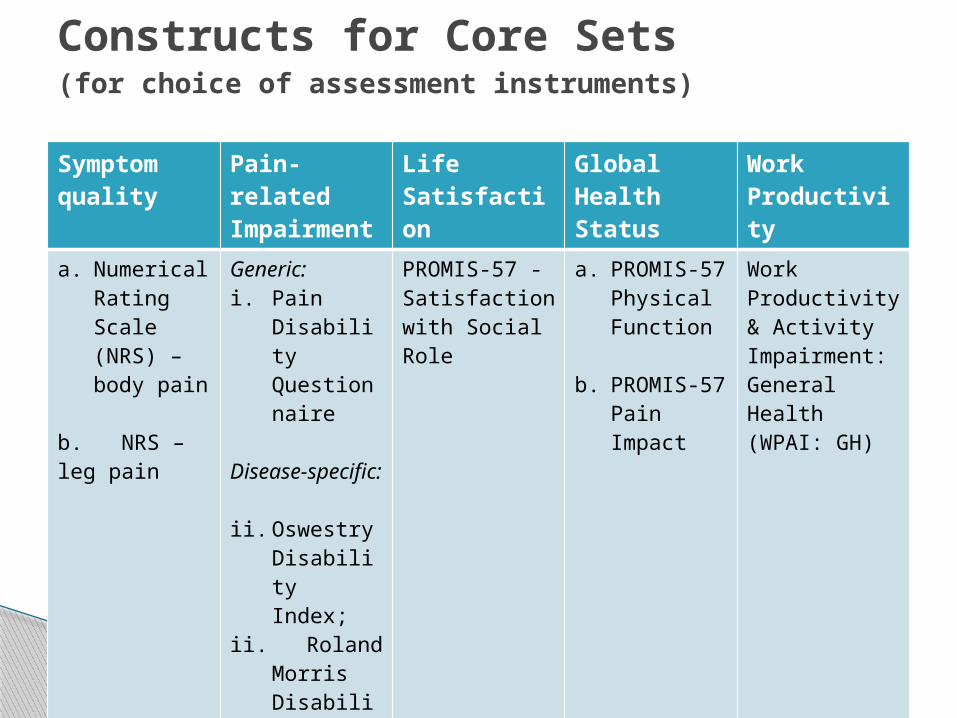
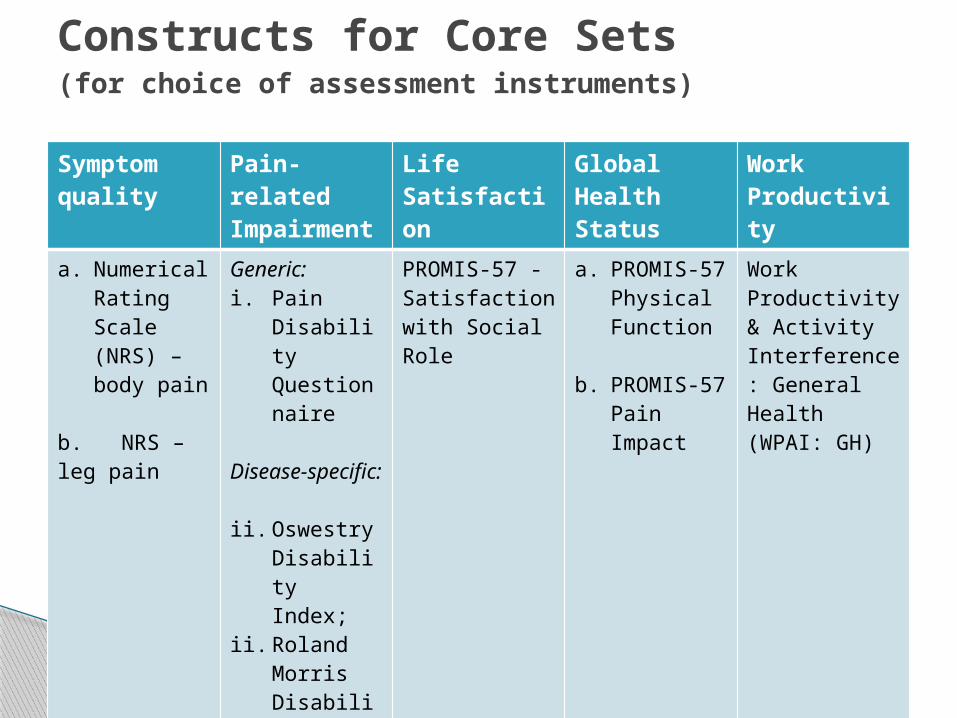
Symptom quality
Pain-related Impairment
Life Satisfaction
Global Health Status
Work Productivity
a. Numerical Rating Scale (NRS) – body pain
b. NRS – leg pain
Generic: i. Pain
Disability Questionnaire
Disease-specific: ii. Oswestry
Disability Index;
ii. Roland Morris Disability Questionnaire
PROMIS-57 - Satisfaction with Social Role
a. PROMIS-57 Physical Function
b. PROMIS-57 Pain Impact
Work Productivity & Activity Impairment: General Health (WPAI: GH)
Constructs for Core Sets (for choice of assessment instruments)
Definition: ◦ the smallest clinical change that is important to
patients, and recognizes the fact that there are some treatment-induced statistically significant improvements that are too small to matter to patients.
Also as Minimal clinical important difference (MCID)
Minimal clinically important improvement (MCII)
Accessed 05/25/14 at: http://www.aaos.org/research/guidelines/SCFguideline.pdf
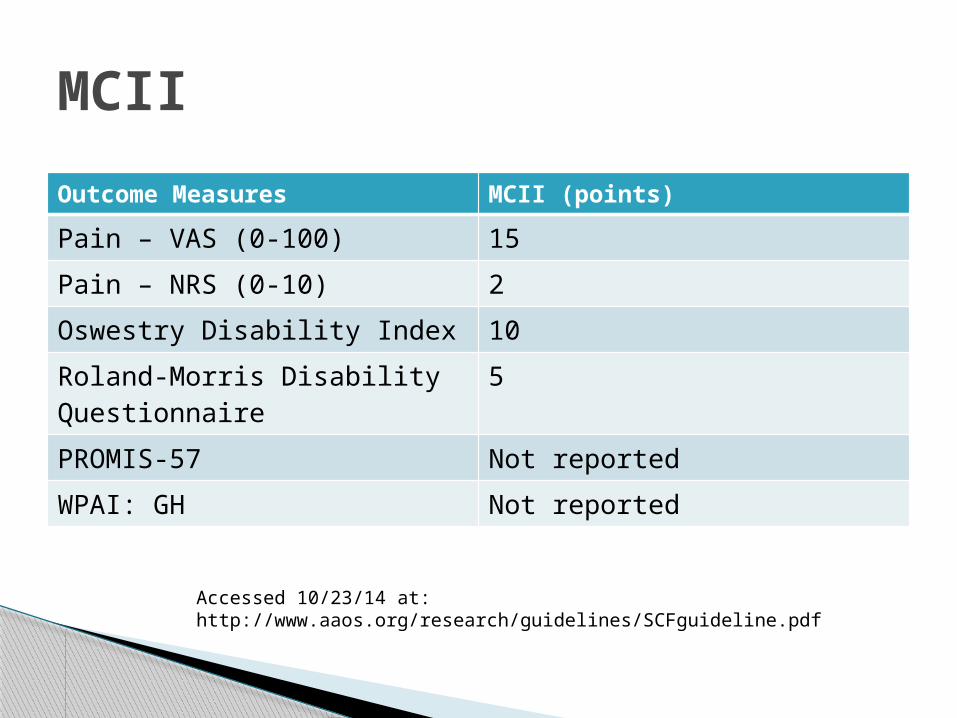
Outcome Measures MCII (points)
Pain – VAS (0-100) 15
Pain – NRS (0-10) 2
Oswestry Disability Index 10
Roland-Morris Disability Questionnaire
5
PROMIS-57 Not reported
WPAI: GH Not reported
MCII
Accessed 10/23/14 at: http://www.aaos.org/research/guidelines/SCFguideline.pdf
To qualify for the 2014 PQRS incentive payment, Physiatrists must report on at least 9 individual measures covering 3 National Quality Strategy (NQS) domains for at least 50 percent of your Medicare Part B FFS patients seen during the reporting period.
Alternatively, you can report at least 1 measures group on a 20-patient sample, a majority of which (at least 11 out of 20) must be Medicare Part B FFS patients.
QTB: Quality Metrics
Accessed 10/23/14 at: http://www.aapmr.org/research/PQRS/Pages/default.aspx
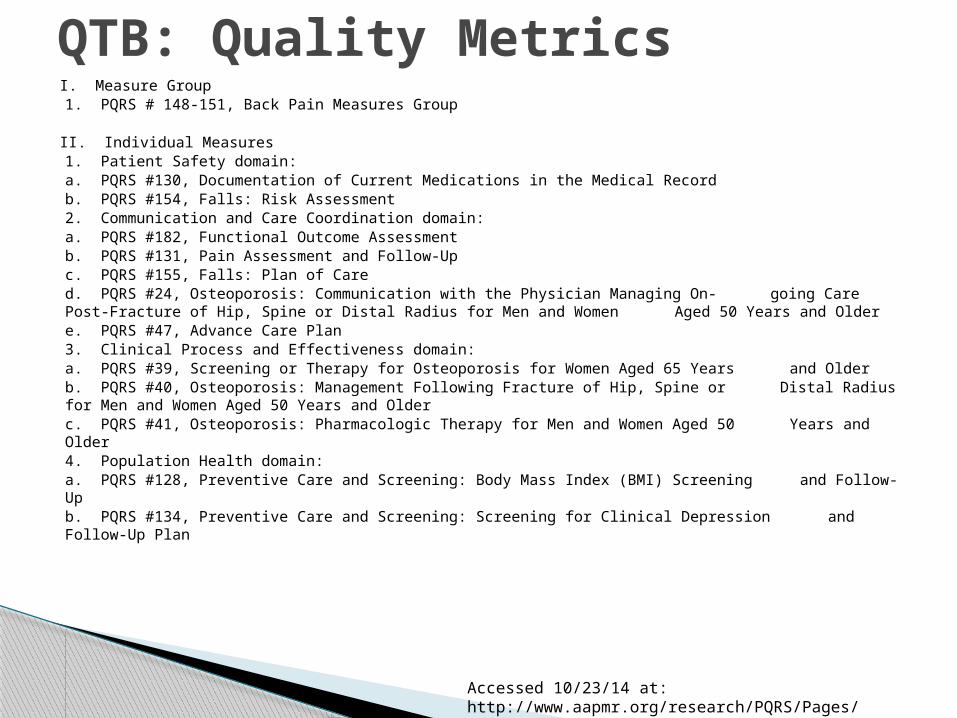
I. Measure Group 1. PQRS # 148-151, Back Pain Measures Group
II. Individual Measures 1. Patient Safety domain:
a. PQRS #130, Documentation of Current Medications in the Medical Recordb. PQRS #154, Falls: Risk Assessment
2. Communication and Care Coordination domain:a. PQRS #182, Functional Outcome Assessmentb. PQRS #131, Pain Assessment and Follow-Upc. PQRS #155, Falls: Plan of Cared. PQRS #24, Osteoporosis: Communication with the Physician Managing On- going Care
Post-Fracture of Hip, Spine or Distal Radius for Men and Women Aged 50 Years and Oldere. PQRS #47, Advance Care Plan
3. Clinical Process and Effectiveness domain:a. PQRS #39, Screening or Therapy for Osteoporosis for Women Aged 65 Years and Olderb. PQRS #40, Osteoporosis: Management Following Fracture of Hip, Spine or Distal
Radius for Men and Women Aged 50 Years and Olderc. PQRS #41, Osteoporosis: Pharmacologic Therapy for Men and Women Aged 50 Years
and Older4. Population Health domain:
a. PQRS #128, Preventive Care and Screening: Body Mass Index (BMI) Screening and Follow-Up
b. PQRS #134, Preventive Care and Screening: Screening for Clinical Depression and Follow-Up Plan
QTB: Quality Metrics
Accessed 10/23/14 at: http://www.aapmr.org/research/PQRS/Pages/default.aspx
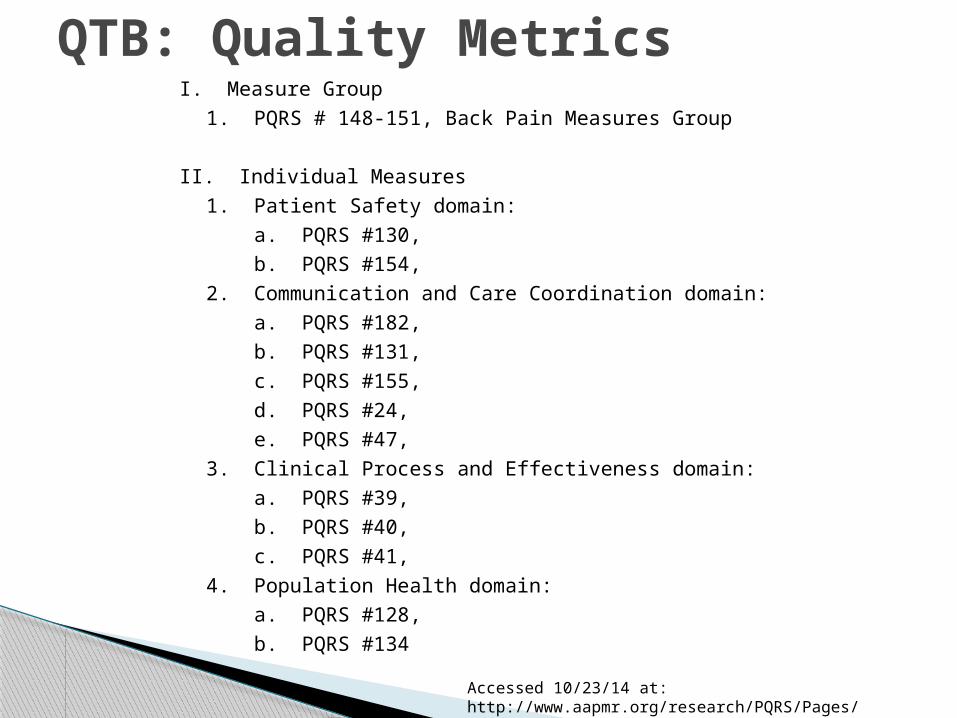
I. Measure Group
1. PQRS # 148-151, Back Pain Measures Group
II. Individual Measures
1. Patient Safety domain:
a. PQRS #130,
b. PQRS #154,
2. Communication and Care Coordination domain:
a. PQRS #182,
b. PQRS #131,
c. PQRS #155,
d. PQRS #24,
e. PQRS #47,
3. Clinical Process and Effectiveness domain:
a. PQRS #39,
b. PQRS #40,
c. PQRS #41,
4. Population Health domain:
a. PQRS #128,
b. PQRS #134
QTB: Quality Metrics
Accessed 10/23/14 at: http://www.aapmr.org/research/PQRS/Pages/default.aspx
Learning objectives:1. Define foundational concepts of the ICF that serve as a guide for the choice of PM&R outcome metrics2. Understand variety of resources available for selection of outcome metrics for PM&R patient populations3. Incorporate outcome measurement into outpatient practices for a variety of patient populations to enhance physiatric care using core sets of measures
What we learned today:
Symptom quality
Pain-related Impairment
Life Satisfaction
Global Health Status
Work Productivity
a. Numerical Rating Scale (NRS) – body pain
b. NRS – leg pain
Generic: i. Pain
Disability Questionnaire
Disease-specific: ii. Oswestry
Disability Index;
ii. Roland Morris Disability Questionnaire
PROMIS-57 - Satisfaction with Social Role
a. PROMIS-57 Physical Function
b. PROMIS-57 Pain Impact
Work Productivity & Activity Interference: General Health (WPAI: GH)
Constructs for Core Sets (for choice of assessment instruments)
Numerical Rating Scale (NRS) – body pain; and,NRS – leg pain
Pain Disability Questionnaire (PDQ)
Oswestry Disability Index (ODI) or Roland-Morris Disability Questionnaire (RMDQ)
PROMIS-57 v1.0
Work Productivity & Activity Impairment: General Health (WPAI: GH) v2.0
Summary: Recommended PRO for practical use
Contact Info:
Armando Miciano, M.D. Nevada Rehabilitation Institute, Las Vegas NV
www.springmountainrehab.com 702-869-4401
Thank You.
Recommended

















