Shock
Presenter :Dr . Mostafa Shokati
Post Doctoral (PDF) in cardiac critical care

What is shock?
Syndrome characterized by decreased tissue perfusion and impaired cellular metabolism
Imbalance in supply/demand for O2 and nutrients
Inadequate cellular oxygenation ◦ Oxygen delivery equation
◦ DO2 = CaO2 x Q
◦ CaO2 = (1.34 x Hgb x SaO2) + (0.003 x PaO2)
◦ Q = HR x SV

Pathophysiology of Shock
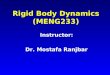
Classification of shock
◦Low blood flow
◦Cardiogenic
◦Hypovolemic
◦Maldistribution of blood flow
◦Septic
◦Anaphylactic
◦Neurogenic

Low Blood FlowCardiogenic Shock
Definition
◦ Systolic or diastolic dysfunction
◦ Compromised cardiac output (CO)
Precipitating causes
◦ Myocardial infarction
◦ Cardiomyopathy
◦ Blunt cardiac injury
◦ Severe systemic or pulmonary hypertension
◦ Cardiac tamponade (Obstructive)
◦ Myocardial depression from metabolic problems

Early manifestations
◦ Tachycardia
◦ Hypotension
◦ Narrowed pulse pressure
◦ ↑ Myocardial O2 consumption
Physical examination
◦ Tachypnea, pulmonary congestion
◦ Pallor; cool, clammy skin
◦ Decreased capillary refill time
◦ Anxiety, confusion, agitation
↑ in pulmonary artery wedge pressure
Decreased renal perfusion and UO
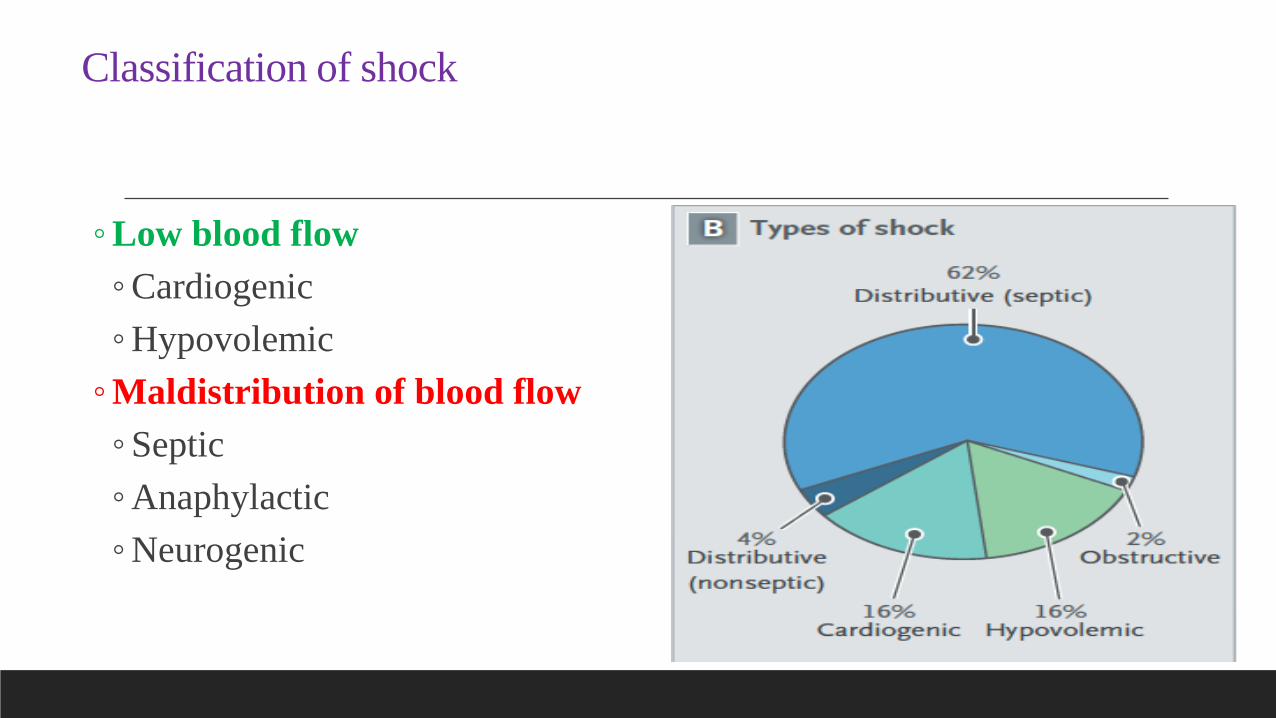
Hypovolemic Shock
Absolute hypovolemia: Loss of intravascular fluid volume
◦ Hemorrhage
◦ GI loss (e.g., vomiting, diarrhea)
◦ Fistula drainage
◦ Diabetes insipidus
◦ Hyperglycemia
◦ Diuresis
Relative hypovolemia
◦ Results when fluid volume moves out of the vascular
space into extravascular space
◦ Termed third spacing

Hypovolemic Shock (Cont’d))
Clinical manifestations
Anxiety
Tachypnea
Increase in CO, heart rate
Decrease in stroke volume, PAWP, UO
If loss is >30%, blood volume is replaced

Maldistribution of Blood FlowNeurogenic Shock
Hemodynamic phenomenon that can occur
within 30 minutes of a spinal cord injury
at the fifth thoracic (T5) vertebra or above
and
can last up to 6 weeks
Results in massive vasodilation leading to
pooling of blood in vessels

Neurogenic Shock (Cont’d)
Clinical manifestations
◦ Hypotension
◦ Bradycardia
◦ Temperature dysregulation (resulting in heat loss)
◦ Dry skin
◦ Poikilothermia (taking on the temperature of the
environment)

Anaphylactic Shock
Acute, life-threatening hypersensitivity
reaction
◦Massive vasodilation
◦Release of mediators
◦ ↑ Capillary permeability

Anaphylactic Shock (Cont’d)Clinical manifestations
◦ Anxiety, confusion, dizziness
◦ Tachycardia, tachypnea, hypotension
◦ Wheezing, stridor
◦ Sense of impending doom
◦ Chest pain
◦ Swelling of the lips and tongue, angioedema
◦ Wheezing, stridor
◦ Flushing, pruritus, urticaria
◦ Respiratory distress and circulatory failure

Septic Shock
Sepsis: Systemic inflammatory response to documented or suspected infection
Severe sepsis = Sepsis + Organ dysfunction
Septic shock = Presence of sepsis with hypotension despite fluid resuscitation + Presence of
tissue perfusion abnormalities
Mortality rates as high as 50%
Primary causative organisms
◦ Gram-negative and gram-positive bacteria
◦ Endotoxin stimulates inflammatory response
◦ Septic shock = Presence of sepsis with hypotension despite fluid resuscitation + Presence of tissue perfusion abnormalities

Pathophysiology of Septic Shock
Copyright © 2010, 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.

Clinical manifestations◦ ↑ Coagulation and inflammation
◦ ↓ Fibrinolysis
◦ Formation of microthrombi
◦ Obstruction of microvasculature
◦ Hyperdynamic state: Increased CO and decreased SVR
◦ Tachypnea/hyperventilation
◦ Temperature dysregulation
◦ ↓ Urine output
◦ Altered neurologic status
◦ GI dysfunction
◦ Respiratory failure is common


Stages of ShockInitial Stage
Usually not clinically apparent
Metabolism changes from aerobic to anaerobic
◦Lactic acid accumulates and must be removed by blood and
broken down by liver
◦Process requires unavailable O2

Compensatory Stage (Nonprogressive)
Clinically apparent
◦ Neural
◦ Hormonal
◦ Biochemical compensatory mechanisms
Attempts are aimed at overcoming consequences of anaerobic metabolism and
maintaining homeostasis
If deficit not corrected, patient enters progressive stage

Baroreceptors in carotid and aortic bodies activate SNS in response to ↓ BP
◦ Vasoconstriction while blood to vital organs maintained
↓ Blood to kidneys activates renin–angiotensin system
◦ ↑ Venous return to heart, CO, BP
If perfusion deficit corrected, patient recovers with no residual sequelae

Progressive Stage (intermediate)
Begins when compensatory mechanisms fail
Aggressive interventions to prevent multiple organ dysfunction syndrome
Hallmarks of ↓ cellular perfusion and altered capillary permeability:
◦ Leakage of protein into interstitial space
◦ ↑ Systemic interstitial edema
Anasarca (severe generalized edema)
◦ Fluid leakage affects solid organs and peripheral tissues
◦ ↓ Blood flow to pulmonary capillaries
Movement of fluid from pulmonary vasculature to interstitium
◦ Pulmonary edema
◦ Bronchoconstriction
◦ ↓ Residual capacity
Progressive Stage Cont’d)
Fluid moves into alveoli
◦ Edema
◦ Decreased surfactant
◦ Worsening V/Q mismatch
◦ Tachypnea
◦ Crackles
◦ Increased work of breathing
CO begins to fall
◦ Decreased peripheral perfusion
◦ Hypotension
◦ Weak peripheral pulses
◦ Ischemia of distal extremities

Progressive Stage (Cont’d)
Myocardial dysfunction results in
◦ Dysrhythmias
◦ Ischemia
◦ Myocardial infarction
◦ End result: Complete deterioration of cardiovascular system
Mucosal barrier of GI system becomes ischemic
◦ Ulcers
◦ Bleeding
◦ Risk of translocation of bacteria
◦ Decreased ability to absorb nutrients
◦ Acute tubular necrosis/acute renal failure
Progressive Stage Cont’d)
Liver fails to metabolize drugs and wastes
◦ Jaundice
◦Elevated enzymes
◦Loss of immune function
◦Risk for DIC and significant bleeding

Progressive (intermediate)Stage of Shock
Copyright © 2010, 2007, 2004, 2000, Mosby, Inc., an affiliate of Elsevier Inc. All Rights Reserved.

Refractory Stage (Irreversible)
Exacerbation of anaerobic metabolism
Accumulation of lactic acid
↑ Capillary permeability
Profound hypotension and hypoxemia
Tachycardia worsens
Decreased coronary blood flow
Cerebral ischemia
Failure of one organ system affects others Recovery unlikely

Diagnostic Studies
Thorough history and physical examination
No single study to determine shock
◦ Blood studies
◦ Elevation of lactate
◦ Base deficit
◦ 12-lead ECG
◦ Chest x-ray
◦ Hemodynamic monitoring

treatment
Overall goal:
1.increase O2 delivery
2.decrease demand

Collaborative CareSuccessful management includes :
◦ Identification of patients at risk for shock
◦ Integration of the patient’s history, physical examination, and clinical findings to establish a diagnosis
◦ Interventions to control or eliminate the cause of the decreased perfusion
◦ Protection of target and distal organs from dysfunction
◦ Provision of multisystem supportive care
General management strategies
◦ Ensure patent airway
◦ Maximize oxygen delivery
Cornerstone of therapy for septic, hypovolemic, and anaphylactic shock = volume expansion
◦ Isotonic crystalloids (e.g., normal saline) for initial resuscitation of shock

Collaborative Care (Cont’d)
Volume expansion
◦ If the patient does not respond to 2 to 3 L of crystalloids, blood administration and
central venous monitoring may be instituted
◦ Complications of fluid resuscitation
◦ Hypothermia
◦ Coagulopathy
Primary goal of drug therapy = correction of decreased tissue perfusion
◦ Vasopressor drugs (epinephrine)
◦ Achieve/maintain MAP >60 to 65 mm Hg
◦ Reserved for patients unresponsive to other therapies

Collaborative Care (Cont’d)
Nutrition is vital to decreasing morbidity from shock
◦ Initiate enteral nutrition within the first 24 hours
◦ Initiate parenteral nutrition if enteral feedings contraindicated or
fail to meet at least 80% of the caloric requirements
◦Monitor protein, nitrogen balance, BUN, glucose, electrolytes

Other treatment
1. correction of acid- bace balance
2.steroids- Hydrocortisone
3.Antibiotics
4.Nasal O2/Ventilatory support
5.CVP line
6.Control of pain
7.ICU-Critical care management

Collaborative CareCardiogenic Shock
Restore blood flow to the myocardium by restoring the balance between O2 supply
and demand
Thrombolytic therapy
Angioplasty with stenting
Emergency revascularization
Valve replacement
Hemodynamic monitoring
Drug therapy (diuretics to reduce preload)
Circulatory assist devices (e.g., intra-aortic balloon pump, ventricular assist device)

Collaborative CareHypovolemic Shock
Management focuses on :
stopping the loss of fluid and restoring the circulating volume
Fluid replacement is calculated using a 3:1 rule (3 ml of isotonic crystalloid for
every 1 ml of estimated blood loss)
Collaborative CareSeptic Shock
Fluid replacement (e.g., 6 to 10 L of isotonic crystalloids and 2 to 4 L of colloids) to restore perfusion
◦ Hemodynamic monitoring
Vasopressor drug therapy; vasopressin for patients refractory to vasopressor therapy
Intravenous corticosteroids for patients who require vasopressor therapy, despite fluid resuscitation, to
maintain adequate BP
Antibiotics after obtaining cultures (blood, wound exudate, urine, stool, sputum)
Drotrecogin alfa (Xigris)
◦ Major side effect: Bleeding
Glucose levels <10 mg/dl
Stress ulcer prophylaxis with histamine (H2)-receptor blockers
Deep vein thrombosis prophylaxis with low-dose unfractionated heparin or low-molecular-weight heparin

Collaborative CareNeurogenic Shock
In spinal cord injury: Spinal stability
◦Treatment of the hypotension and bradycardia with vasopressors
and atropine
◦Fluids used cautiously as hypotension is generally not related to
fluid loss
◦Monitor for hypothermia

Collaborative CareAnaphylactic Shock
Epinephrine, diphenhydramine
Maintaining a patent airway
◦ Nebulized bronchodilators
◦ Endotracheal intubation or cricothyroidotomy may be necessary
Aggressive fluid replacement
Intravenous corticosteroids if significant hypotension persists after 1 to 2 hours
of aggressive therapy

Nursing Assessment
ABCs: Airway, breathing, and circulation
Focused assessment of tissue perfusion
◦ Vital signs
◦ Peripheral pulses
◦ Level of consciousness
◦ Capillary refill
◦ Skin (e.g., temperature, color, moisture)
◦ Urine output
Brief history
◦Events leading to shock
◦Onset and duration of symptoms
Details of care received before hospitalization
Allergies
Vaccinations

Nursing Diagnoses
Ineffective tissue perfusion: Renal, cerebral,
cardiopulmonary, gastrointestinal, hepatic, and peripheral
Fear
Potential complication: Organ ischemia/dysfunction

Planning
Goals for patient
◦Assurance of adequate tissue perfusion
◦Restoration of normal or baseline BP
◦Return/recovery of organ function
◦Avoidance of complications from prolonged states of
hypoperfusion
Nursing Implementation
Health Promotion
◦ Identify patients at risk (elderly patients, those with debilitating illnesses or
who are immunocompromised, surgical or accidental trauma patients)
◦ Planning to prevent shock
(monitoring fluid balance to prevent hypovolemic shock, maintenance of
handwashing to prevent spread of infection)

Nursing Implementation (Cont’d)
Acute Interventions
◦ Monitor the patient’s ongoing physical and emotional status to detect subtle
changes in the patient’s condition
◦ Plan and implement nursing interventions and therapy
◦ Evaluate the patient’s response to therapy
◦ Provide emotional support to the patient and family
◦ Collaborate with other members of the health team when warranted

Nursing Implementation (Cont’d)
Neurologic status: Orientation and level of consciousness
Cardiac status
◦Continuous ECG
◦VS, capillary refill
◦Hemodynamic parameters: central venous pressure, PA pressures,
CO, PAWP
◦Heart sounds: Murmurs, S3, S4
◦

Nursing Implementation (Cont’d)
Respiratory status
◦Respiratory rate and rhythm
◦Breath sounds
◦Continuous pulse oximetry
◦Arterial blood gases
◦Most patients will be intubated and mechanically ventilated

Nursing Implementation (Cont’d)
Urine output
Tympanic or pulmonary arterial temperature
Skin: Temperature, pallor, flushing, cyanosis, diaphoresis,
piloerection
Bowel sounds

Nursing Implementation (Cont’d)
Nasogastric drainage/stools for occult blood
I&O, fluid and electrolyte balance
Oral care/hygiene based on O2 requirements
Passive/active range of motion

Nursing Implementation (Cont’d)
Assess level of anxiety and fear
◦Medication PRN
◦Talk to patient
◦Visit from clergy
◦Family involvement
◦Comfort measures
◦Privacy
◦Call light within reach

Evaluation
Normal or baseline, ECG, BP, CVP, and PAWP
Normal temperature
Warm, dry skin
Urinary output >0.5 ml/kg/hr
Normal RR and SaO2 ≥90%
Verbalization of fears, anxiety

Thanks for your attention
Recommended