ESMO Preceptorship Programme
Presentation of three challenging clinical cases and Faculty discussion
Andrés Cervantes/Dirk Arnold
Colorectal Cancer – Valencia – 12,13 May 2017

ESMO PRECEPTORSHIP PROGRAM
Disclosures
Consulting and advisory services, speaking or writing engagements,
public presenations:
Servier, Merck Serono, Amgen, Roche, Lilly, Bayer, Novartiis, Takeda, Beigene
Direct research support to the responsible project lead:
Servier, Roche, Genentech, Bayer, Janssen, Merck Serono, Medimmune

2
• 62 year old male
• No previous diseases or comorbidities
• Constipation and rectal bleeding
• False diarrhea and tenesmus
• No weight loss
• PS 1
CLINICAL CASE

3
• No peripheral lymph nodes
• No hepatomegaly
• No ascites
• No pleural effusion
• DRE: Fixed tumor at 3 cm from the anal
verge involving 3/4 of the circumference
Physical examination

4
• Rigid rectoscopy: a fixed tumor at 3 cm from the
anal verge obstructing ¾ of the circumference
• Biopsy: poorly differentiated invasive
adenocarcinoma of the rectum
• Colonoscopy: Tumor at 5 cm. Flexible colonoscopy
able to surpass the rectal mass reaching the cecum.
No synchronous polyps.
Diagnostic tests-1

5
• CBC: no anemia
• Biochemistry: within normal range. No liver
alterations.
• CEA: 12.9 ng/ml
• Thorax CT scan: No lung mets
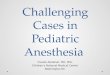
• Abdomino-pelvic CT-scan: 9 liver
metastatic nodes involving both liver lobes
Diagnostic tests-2
6
Abdominal CT-scan

7
• MRI Staging
• MDT discussion
• Preoperative chemoradiation if indicated
• TME Surgical resection
• Pathology assessment and estimation of risk
• Postoperative chemotherapy if indicated
Current approach to localized rectal cancer
8
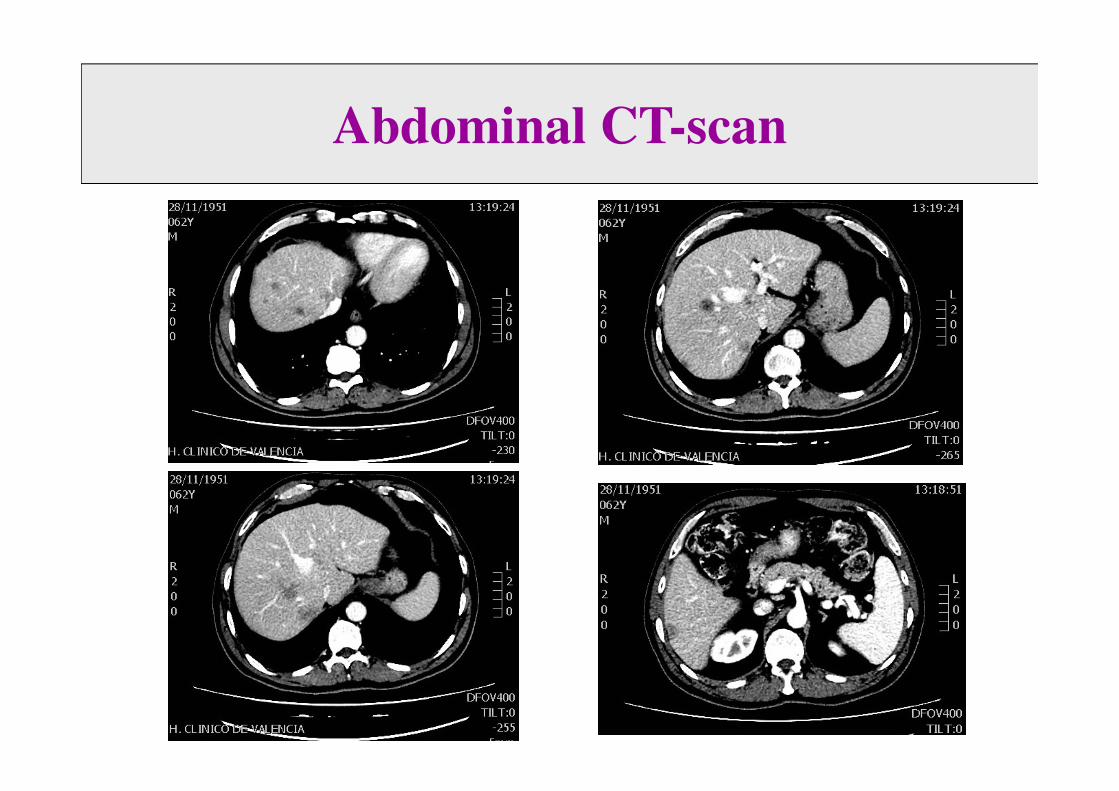
Magnetic resonance imaging
9
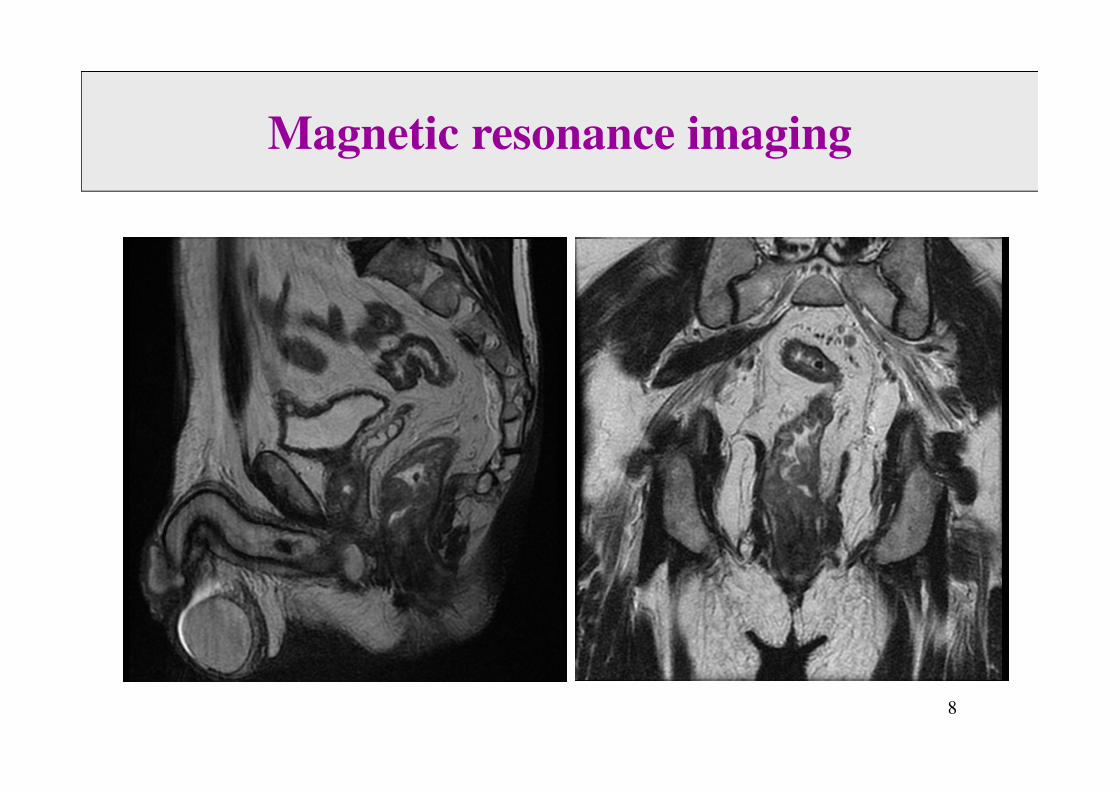
Magnetic resonance imaging

10
• Bulky rectal tumor below the levators and located at 1 cm from the anal verge
• Several nodes with suspected neoplastic involvementand tumor involving the mesorectal fascia
• Invasion by tumor of mesorectal fascia at the anterior and lateral left side
• Left puborectal muscle involved
• No prostatic involvement, but very close to Denonvilliers fascia
• No extramural vascular invasion
• No lateral pelvic nodes (extramesorectal)
Magnetic resonance imaging report
11
• Symptomatic locally advanced rectal cancer
• 62-year old male
• Extensive and unresectable liver only
metastatic disease
• All RAS and BRAF wild-type
• Fit patient without comorbidities
• Do not miss any opportunities
SUMMARY

12
1. Chemoradiation followed by CT
2. Chemotherapy + anti-EGFRs only
3. 5x5 Radiation followed by Chemo
4. TME up front plus Chemo
5. Liver resection plus chemoradiation
Your treatment plan:

13
• Chemoradiation followed by CT
• Chemotherapy + anti-EGFRs only
• 5x5 Radiation followed by Chemo
• TME up front plus Chemo
• Liver resection plus chemoradiation
Your treatment plan:

14
• MRI Staging
• MDT discussion
• Preoperative chemoradiation or 5x5
radiation if indicated
• TME Surgical resection
• Pathology assessment and estimation of risk
• Postoperative chemotherapy if indicated
Current approach to localized rectal cancer

15
• Radiation 5x5 Gy was given for
symptomatic purposes
• Chemotherapy was started two weeks later
within a randomized phase II trial with
FOLFOX-Bev +/- experimental agent
• Assessment of response was considered 8
weeks after starting FOLFOX-Bev
Treatment plan

16
Assessment of primary tumor by
Magnetic Resonance Imaging
• Asymptomatic
• Disappearance of all previous symptoms
• DRE: no mucosal damage
• Rigid rectoscopy: Normal appearance
with no residual ulcer or scar
• Endoscopic ultrasonography: no
disruption of bowel layers
17
Assessment of primary tumor

18
Assessment of liver mets by
CT-scan
19
1. Liver surgery followed by TME
2. TME followed by liver surgery
3. Liver surgery and surveillance for the
primary rectal tumor
4. No further therapy and reintroduce
treatment upon progression
Your treatment plan:

20
• Liver surgery followed by TME
• TME followed by liver surgery
• Liver surgery and surveillance for the
primary rectal tumor
• No further therapy and reintroduce
treatment upon progression
Your treatment plan:

21
• Liver surgery was planned after 8 courses of
FOLFOX-Bev plus 4 courses FULV-Bev
• A right hepatectomy after right hepatic
artery embolization was performed 6 weeks
after the last dose of Bevacizumab
• Surveillance and follow up for the primary
rectal tumor
• No postoperative ChT was considered
Treatment plan

22
• Hospitalized for 7 days
• No liver damage: steatosis, steatonecrosis or
sinusoidal occlusive disease
• A pCR was defined in the pathology report
• Multiple scar areas with no rest of
malignant cells
Assessment of liver surgery

23
• Rectal exam plus proctoscopy plus MRI
every 4 months
• CT-scan every three months
• No evidence of progression 20 months after
diagnosis
Follow up plan

24
• Locally advanced rectal cancer with synchronous multiple liver only metastatic disease
• Multidisciplinary discussion essential for all rectal cancer cases: at start and during treatment or follow up
• Do not miss any opportunities for your patients
• 5x5 Radiation plus CT may induce clinical CRs
• After chemotherapy, liver resection recommended if mets become resectable
• Surveillance of the primary tumor as an emerging option
• So far successful multimodality treatment
CONCLUSIONS

MULTIDISCIPLINARY TEAM FOR
COLORECTAL CANCERBIOMEDICAL RESEARCH INSTITUTE INCLIVA
UNIVERSITY HOSPITAL VALENCIA
• MRI: Salvador Campos
• Pathology: Samuel Navarro, Carolina Martínez
• Surgery: Alejandro Espí, Estephanie García-Botello,
Vicente Plá, David Moro, José Martín Arévalo.
• Radiation Oncology: Esther Jordá
• Medical Oncology: Susana Roselló, Desamparados Roda,
Marisol Huerta, Isabel Chirivella (Family Cancer Unit),
Ricard Borras, Alba Viala, Federica Papaccio, Angelica
Petrillo, Andrés Cervantes

26
• Woman 33 years old.
• Pregnacy in the 17th week.
• Complains about rectal bleeding and
hypertransaminasemia.
• Abdominal-pelvic MRI: Multiple liver metastasis.
Thickening of sigma.
• CEA 82 ng/mL
• LDH 2450 IU/ml AlK Ph 285 IU/ml
• Colonoscopy: Tumor at 25 cm of anal margin.
Biopsy����Adenocarcinoma. RAS/BRAF wt.
CLINICAL CASE

MARCH 2015
Abdominal CT-scan

28
1. Surgery for the primary followed by CT
2. FOLFOX or FOLFIRI + anti-EGFRs
3. FOLFOXIRI + BEV
4. Cape plus Bev
5. FOLFIRI or FOLFIRI +BEV
Your treatment plan:

02/15
Diag.
Abortion
03/15
FOLFOXIRI-BEVA
08/15
8 cycles
PR(-50%)
Non resect.
->
FOLFIRI-
Beva.
Evolution and treatmentsDISEASE EVOLUTION AND
TREATMENT

MARCH 2015 AUGUST 2015
RESPONSE ASSESSMENT: PR

Evolution and treatments
02/15
Diag.
Abortion
03/15
FOLFOXI
RI-BEVA
08/15
8 cycles
PR(-50%)
Unresect.
->
FOLFIRI-
Beva.
01/16
6 cycles
PR maint.
Haematological
tox.
H. And F. Sind.
Diarreha.
03/16
10 cycles
PR maint.
->5-FU-Beva.
????
DISEASE EVOLUTION AND
TREATMENT

AUGUST 2015 JULY 2016
RESPONSE ASSESSMENT: PD

33
1. REINTRODUCE FOLFOX + BEV
2. FOLFIRI + anti-EGFRs
3. FOLFOX + BEV
4. IRINOTECAN + anti-EGFRs
5. FOLFIRI or FOLFIRI +BEV
Your treatment plan:

AUGUST 2015 JULY 2016
RESPONSE ASSESSMENT: PD

Evolution and treatments
02/15
Diag.
Abortion
03/15
FOLFOXI
RI-BEVA
08/15
8 cycles
PR(-50%)
Unresect.
->
FOLFIRI-
Beva.
01/16
6 cycles
PR maint.
Haematological
tox.
H. And F. Sind.
Diarreha.
03/16
10 cycles
PR maint.
->5-FU-Beva.
07/16
8 cycles
Liver PD
->FOLFOX-Beva.
DISEASE EVOLUTION AND
TREATMENT

JANUARY 2017
• 11 cycles of FOLFOX-Bevacizumab.
• In CT scan no evidence of progression: increase of 20%
of metastasic lesions.
• LIVER PROGRESSIVE DISEASE
• Blood test:
– Hypertransaminasemia.
– LDH 1006 U/ml. ALP 321mU/ml.
– CEA 180 ng/ml (previous 93,7 ng/ml).
DISEASE EVOLUTION AND
TREATMENT

37
1. REINTRODUCE FOLFIR + BEV
2. FOLFIRI + anti-EGFRs
3. CAPE + BEV
4. IRINOTECAN + anti-EGFRs
5. BEST SUPPORTIVE CARE
Your treatment plan:

Evolution and treatments
02/15
Diag.
Abortion
03/15
FOLFOXI
RI-BEVA
08/15
8 cycles
PR(-50%)
Unresect.
->
FOLFIRI-
Beva.
01/16
6 cycles
PR maint.
Haematological
tox.
H. And F. Sind.
Diarreha.
03/16
10 cycles
PR maint.
->5-FU-Beva.
07/16
8 cycles
Liver PD
->FOLFOX-
Beva.
11/16
8 cycles
SD
01/17
11 cycles
Liver PD
->CPT11-cetuximab
03/17
4 cycles
PR (-50%
liver met.)

JANUARY 2017 MARCH 2017
DISEASE EVOLUTION AND
TREATMENT

Evolution and treatments
02/15
Diag.
Abortion
03/15
FOLFOXI
RI-BEVA
08/15
8 cycles
PR(-50%)
Non resect.
->
FOLFIRI-
Beva.
10/15
3 cycles
PR
maintenance
01/16
6 cycles
PR maint.
Haematological
tox.
H. And F. Sind.
03/16
10 cycles
PR
->5-FU-Beva.
07/16
8 cycles
Liver DP
->FOLFOX-
Beva.
11/16
8 cycles
SD
01/17
11 cycles
Liver DP
->CPT11-
cetuximab
03/17
4 cycles
PR (-50%
liver met.)
05/17
8 cycles
PR maint.

1. REGORAFENIB
2. LONSURF
3. CAPE + BEV
4. TEST HER2 STATUS
5. BEST SUPPORTIVE CARE
OPTIONS FOR FUTURE
TREATMENTS
• Herceptest� Positive 3+.
OPTIONS FOR FUTURE
TREATMENTS

Kavuri SM et al, Cancer Discovery 2015; 5:832-841
Anomalías moleculares de HER2 en cáncer de colon

Kavuri SM et al, Cancer Discovery 2015; 5:832-841
Anomalías moleculares de HER2 en cáncer de
colon: Sesibilidad a Lapatinib + Trastuzumab

HERACLES treatment and assessments
Siena et al Lancet Oncol, 2016; 17:438-446.
Lapatinib/Trastuzumab en cáncer de colon HER2+++Estudio Heracles
Recommended