Dallas A Forshew, RN, BSNManager, Clinical Research
Forbes Norris ALS Research Center
California Pacific Medical Center, San Francisco

OutlineStatement of the problemDefinition of FTD and variantsOverview of ALS CBS™How to administer ALS CBS™How to score ALS CBS™Resources

What is Frontotemporal Dementia?FTD: severe form of cognitive / behavioral impairment
Frontal and/or temporal areas of brain are damaged and start to slowly atrophy
May start with Poor decision making (executive dysfunction) Personality changes or behavior problems (behavior variant) or Language difficulty (trouble finding words)
Gets worse as time passes. Does not get better.Patients with easy crying or laughing (pseudobulbar) do not have
this problem more than other ALS patientsClear criteria for uncovering FTD (Neary, 1998)Not at all like Alzheimer’s disease (memory mostly stays normal)

FTD is not new in ALSOld descriptions
Withdrawn due to depression
StubbornSeeking control in some
area of lifeAnger outbursts due to
frustration of ALSDenialLanguage problems due
to dysarthria
FTD behaviorsApatheticDis-inhibited Poor judgementEasily frustratedQuick to angerLack of insightLanguage difficulty
Word findingSpellingAphasia

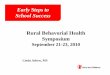
Incidence of FTD in ALS
AD 4%
Normal 48%
FTD 22%Not normal,
Not FTD 26%
Normal 48%
FTD 22%
AD
4%
Behavior
Variant 1
7%
Executive
Dysfunction
9%
The 26% that is not normal but also not ALS/FTD is redefined as ALSci (Executive Dysfunction 9%), ALSbv (Behavior Variant 17%) Lomen-Hoerth C, Murphy J

ALS in FTD
36 patients with sporadic FTD and no known motor neuron disease14% definite ALS36% possible ALS14% fasciculations (1 pt = definite ALS after 1 yr)17% swallowing trouble5% other abnormalitiesC. Lomen-Hoerth, T. Anderson, B. Miller, Neurology, 2002

Genetic Overlap of ALS and FTDFamilial: 10% of ALS, 40% of FTD Affected family members may have only ALS,
only FTD, or both in familial casesTDP-43 was discovered to be the major disease
protein in both ALS and the most common form of FTD. Mutations in TDP-43 cause ALS and FTD.
C9ORF72 is responsible for 20-40% of all familial ALS cases and 12% of FTD cases (2011)
4-8% of sporadic ALS cases and 3% of sporadic FTD cases have mutations in C90RF72

Why is this Important?
ALS patients with cognitive problems, behavioral
problems, or FTD• Are half as likely to accept interventions such as NIV
or PEG
• They die, on average, a year earlier Portet et al. ALS and Other MND 2001;2:23-29Hodges et al. Neurology 2001;61:349-354
Compliance NIV PEG
ALS-FTD 5 of 18 (28%) 4 of 16 (25%)ALS only 14 of 23 (61%) 8 of 12 (67%)Olney RK, Lomen-Hoerth C, Forshew DA, et al. ALS/MND 11/2003

Why Screen? PrognosisExecutive dysfunction is a negative prognostic
indicator in patients without dementiaElanin, et al, Neurology. 2001, 76:1269
Decreased survival of ALS patients with either ALS-FTD or cognitive impairment (executive dysfunction)(ALSci)
ALS-FTD: 23 vs. 34 months (p=0.026)ALSci: 24 vs. 38 months (p<0.0001)

ALS CBS™ ALS Cognitive Behavioral ScreenValidated for sensitivity, accuracy, specificityFast 5 minute SCREENCognitive component
Performed by MD, RN, SLP, research coordinator 4 sections each worth 5 points
Attention, concentration, tracking/monitoring, initiation and retrieval
Behavioral component Self-administered by family member Compares current behavior with past – changes 18 questions

Attention: Commands I am going to say some commands. Please listen
carefully and do what I say. If patient is unable to indicate with finger, movement can be
substituted with eyes, arm or other means.Point/indicate (with your finger) to the ceiling and then
to your left.Touch your shoulder, point to the floor, then make a
fist.Scoring
1 point for getting both correct.

Attention: Mental Addition/LanguageI am going to say some phrases. I want you to tell
me the number of syllables in each.For example ‘the table’ has 3 syllables.The weather is nice. (correct response: 5)Tomorrow will be sunny. (correct response: 7)
Scoring1 point for getting both correct.Score 0 if > 20 seconds on either

Attention: Eye Movements - SaccadesHold up two fingers in front of patient, about 36 inches
apart, at patient’s eye level. Wiggle one finger. Ask the patient to look at the finger that moves
without moving their head, and then look back at you. Randomly move left and right finger, pausing 2 seconds between each trial, for a total of 8 trails.
Patient Instructions: I am going to hold my fingers up. I want you to keep your head straight and look at me. When I wiggle a finger, I want you to look at that finger and then look back at me. Try not to move your head, only your eyes. Each time I wiggle a finger, look at it and then back to me. (Do 1-2 trials with the pt as an example) We will do that a few times. Ready? (Do 8 random trials).

Attention: Eye Movements – Anti-saccadesPatient Instructions: Good, next I am going to wiggle a finger
again, but this time, I want you to look AWAY from the finger that moves. For example, if I move this finger (wiggle one) then I want you to look at the other finger, not the one that moves, ok? Let’s try it (do 1-3 trials). Just like before, try to keep you head still and just move your eyes. After each one, look back at me. Ready? (Do 8 random trials).
ScoringSaccades: 1 pt for 8 correct; Anti-saccades 2 pts for 8 correct, 1 for 7Scoring errors: This includes any incorrect gaze, even if the patient
immediately self-corrects. An error is also counted if a patient attempts to anticipate your move and looks before you wiggle a finger.

ConcentrationI am going to say some numbers. After I say them, I want
you to say them to me backwards or in reverse order.For example, if I say 3-6, you would say 6-3.If written, do not allow allow pt to write forward span. Discontinue after failure on 2 consecutive trials. 2-9 (9-2) 7-8-6-4 (4-6-8-7) 9-4 (4-9) 8-4-1-7 (7-1-8-4)8-7-2 (2-7-8) 8-2-5-9-4 (4-9-5-8-2)5-8-1 (1-8-5) 5-8-6-3-9 (9-3-6-8-5)

ConcentrationScoring (Discontinue after failure on 2 consecutive trials.)Score for the maximum span correct (2 – 5)
2-9 (9-2) 7-8-6-4 (4-6-8-7) 9-4 (4-9) 8-4-1-7 (7-1-8-4)8-7-2 (2-7-8) 8-2-5-9-4 (4-9-5-8-2)5-8-1 (1-8-5) Score 4
2-9 (9-2) 7-8-6-4 (4-6-8-7) 9-4 (4-9) 8-4-1-7 (7-1-8-4)8-7-2 (2-7-8) 8-2-5-9-4 (4-9-5-8-2)5-8-1 (1-8-5) 5-8-6-3-9 (9-3-6-8-5) Score 4

Tracking / Monitoring: Months
Please say the months of the year backward, starting with December
ScoringErrors include omissions, repetitions, and intrusionsScore 2 if no errors, 1 if 1 error, 0 if 2 or more errorsScore 0 if patient took > 60 seconds

Tracking / Monitoring: Alphabet
Please say (or write) the alphabet for me.
ScoringMark uncorrected errors, omissions, repetitions, or
intrusionsScore 1 for no errors, 0 if any errors

Tracking / Monitoring:Alternation TaskI want you to alternate between numbers and letters
starting with 1-A, and then 2-B, 3-C, and so on. Please continue from there, alternating between number-letter, number-letter, in order, without skipping any until I tell you to stop.
4-D 5-E 6-F 7-G 8-H 9-I 10-J 11-K 12-L 13-MScoring
Errors: Any mistake in sequencing, i.e. 7-H or 8-9A consistent error counts as only 1 error i.e. 7-H, 8-I, 9-KScore 2 for all correct, 1 for only 1 error, 0 for > 1 error

Initiation and RetrievalSay (write) as many words as you can starting with the
letter F, as quickly as you can, in 1 minute. (Show patient Fluency Rules) You cannot say or write the names of people, places, or numbers. Please do not say or write the same word with just a different ending like truck, trucks. (S words can be substituted for F words.)
ScoringScore 3 for > 12 words, 2 for 12-8 words, 1 for 7-5 words, 0 for < 4)Errors include repeats, people, places, or numbers0 errors score 2 more, 1 error gets 1 more point, 2 or more errors-0 If 4 or less words, the total score is o, no matter how few errors

Guidelines for Total ScoreThis is a SCREENING toolDiagnosis of FTD requires extensive testing with a
qualified neuropsychologist Manual and Instructions:
Susan Woolley, PhD [email protected] interpretation
17-20: Do not support presence of clear cog impairment< 16: Suspicion of cognitive impairment< 10: Considerable suspicion, further testing needed

ResourcesFamily Caregiver Alliance
800-445-8106 www.caregiver.org
ALS Association800-782-4747 www.alsa.orgFYI informational fact Sheets
ALS and Cognitive Changes: A Guide for Patients and Families
ALS, Cognitive Impairment & Frontotemporal Lobar Dementia (for professionals)

Many ThanksForbes Norris ALS Research Center
Susan Woolley, [email protected]
ALS Center at UCSFCatherine Lomen-Hoerth, MD, PhDJennifer Murphy, PhD

ReferencesWoolley SC, York MK, Moore DH et al. Detecting frontotemporal
dysfunction in ALS: Utility of the ALS Cognitive Behavioral Screen (ALS-CBS™). Amyotroph Lateral Scler 2010; 11(3): 303-311.
Lomen-Hoerth C, Murphy J, Langmore S, Kramer JH, Olney RK, Miller B. Are amyotrophic lateral sclerosis patients cognitively normal? Neurology 2003; 60(7):1094-1097.
Olney R, Murphy J, Forshew D, Garwood E, Miller B, Langmore S, Kohn M, Lomen-Hoerth C. The effects of executive and behavioral dysfunction on the course of ALS. Neurology 2005; 65: 1774-1777.
Recommended