Preoperative Evaluationand Management with Cardiac
Evaluation
Lauren Hojdila, MSA, AA-CNova Southeastern University

The Preoperative EvaluationA Standard of Care
• The Joint Commission for the Accreditation of Healthcare Organizations (TJC) requires that all patients receive a preoperative anesthetic evaluation
• The American Society of Anesthesiologists (ASA) has approved Basic Standards for Pre-Anesthetic Care, which outlines the minimum requirements for a preoperative evaluation

Goals of the Preoperative Evaluation
• Primary Goals– Reduce patient risk– Reduction of perioperative morbidity and
mortality
• Secondary Goals– Promote efficiency– Reduce costs
*Conducting a preoperative evaluation is based on the premise that it will modify patient care and improve outcome.

Does the Preoperative Evaluation alter Patient Care ?
• Gibby et al found that anesthetic plans were altered in 20% of all patients due to conditions identified at the preoperative evaluation
• The most common conditions resulting in modification of the anesthetic plan were gastric reflux, IDDM, asthma, and suspected difficult airway
• These findings indicate the need to do the initial preoperative evaluation before the day of surgery

Components of the Preoperative Evaluation
• Personal Interview• Review of systems• Prior anesthetic experience (Difficult intubation, delayed
emergence, MH, delayed NMB, PONV)• Drug allergies
• Physical Examination• Airway exam• Body habitus
• Review of Medical Records• Medications• Substance use (alcohol, tobacco, illicit)• Surgical history• Surgical Diagnosis (Organ systems involved, Planned
procedure)

ASA ClassificationClass 1: Healthy patient, No medical problems
Class 2: Mild systemic disease
Class 3: Severe systemic disease, but not incapacitating
Class 4: Severe systemic disease that is a constant threat to life
Class 5: Moribund, not expected to live 24 hours irrespective of operation
Class 6: Organ donor
E may be added to the status number to designate an emergency operation

Thyromental DistanceAirway Examination
• Distance from the thyroid cartilage to the inside of the mentum
• Measured with the neck in the sniff position
• What is normal thyromental distance?
A higher Mallampati class combined with a mental distance <2 finger-breadthsmay better predict increased difficulty with intubation.

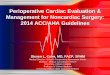
Mallampati ClassificationAirway Examination
• Class I: Soft palate, fauces, uvula, tonsillar
pillars• Class II: Soft palate, fauces, uvula• Class III: Soft palate, base of uvula• Class IV: Hard palate only

What other feature increase the likelihood of difficult intubation?
• Short, thick neck (Neck circumference)
• Diminished neck extension• Decreased tissue compliance• Large tongue• Teeth (Overbite, Large teeth)• Decreased TMJ mobility

NPO Guidelines
• Healthy Adults (No risk factors)• No solid foods for a minimum of 6 hours• Clear liquids up to 2 hours prior to elective
case• Oral medications up to 1-2 hours with sip of
water
• Pediatric patients• Clear liquids up to 2 hours preOp• Breast milk up to 4 hours preOp• Solid foods, nonhuman milk, formula up to 6
hours preOp

AspirationWho has a higher risk ?
• Gastrointestinal Obstruction• GERD• Diabetes mellitus• Recent solid-food intake• Abdominal distention• Pregnancy• Depressed consciousness• Recent opioid administration• Upper GI or naso-oropharyngeal bleeding, with or
without trauma• Emergency surgery

The Healthy PatientSystems Approach
• Airway• Examination as previously described
• Pulmonary• History – Tobacco use, asthma, SOB/DOE, sleep apnea,
wheezing, cough, etc.• Physical exam – Lung sounds, chest excursion, use of
accessory muscles, cyanosis, clubbing, etc.
• Cardiovascular• HTN, CAD, MI, angina, CHF, dysrhythmias, valvular dx,
heart sounds, carotid bruits, peripheral pulses
• Neurologic• Mental status, h/o seizures, neuromuscular disease, nerve
injury
• Endocrine• Diabetes mellitus, thyroid disease, adrenal cortical
suppression, etc.

The Patient with Known Cardiac Disease
• Define risk– Goldman risk index (Independent
predictors)• High-risk surgery, h/o ischemic heart dx, h/o
CHF, h/o cerebrovascular dx, preOp insulin therapy, and preOp serum creatinine > 2 mg/dL
• Need for further testing• Recent MI or ECG changes• Poor exercise tolerance
• Need for cardiac surgery• Prior to current elective surgery

The Patient withPulmonary Disease
• Site and Type of Surgery• Thoracic and upper abdominal procedures are
associated with increased pulmonary complications
• Type and Severity of Disease• Does the disease have a reversible component ?• When were they last hospitalized ?
• Interview• Exercise tolerance, chronic cough, smoking history• What are their current treatment modalities?
• Physical Exam• Lungs sounds – wheezing, rhonchi, decreased breath
sounds

Other Diseases of Concern
• Diabetic Mellitus• Increased risk of CAD, perioperative MI,
hypertension, and CHF• Consider beta-blockade in diabetics with CAD to help
limit myocardial ischemia
• Renal Disease• Altered drug metabolism• Fluid management
• Liver Disease• Coagulation abnormalities• Altered protein binding and volume of distribution

PerioperativeLab Testing
• No evidence supports the use of routine laboratory testing
• There is support for the use of selected lab analysis based on the patient’s preOp history, physical exam, and proposed surgical procedure
• A positive result is frequently a false-positive• High incidence of false-positives when performing tests in
normal patients (a population with a very low prevalence of disease)
• Risk/Cost vs. Benefit• Medical testing is associated with significant cost• The risk of intervention may outweigh the benefit
• Is it going to change what you do ???

Recommended Lab Tests
• CBC / Hemoglobin• Hgb of 7 g/dL is acceptable in patients without systemic
disease (depending upon proposed surgical procedure)• In patients with systemic disease, signs of inadequate
systemic oxygen delivery are an indication for transfusion
• Electrolytes• Creatinine and glucose in older asymptomatic adults• BUN and creatinine in patients with systemic disease or
on medications that affect the kidneys
• Coagulation Studies• Recommended in patients with bleeding disorders, liver
dysfunction, or on anticoagulant therapy

Recommended Lab TestsContinued
• Pregnancy Testing• Current practice:
– testing all females of child-bearing age
• Chest X-rays• Routine testing in the population without
risk factors can lead to more harm than good• Is indicated in patients with a history or
clinical evidence of active pulmonary disease, and may be indicated routinely in patients of advanced age

Preoperative Medications
• What is the goal of premedication ?• Anxiolysis, Sedation, Amnesia, Analgesia, etc.
• What drug, when, and how much ?• Several classes of drugs may be available to facilitate
the desired goal• Timing of drug delivery is as important as drug selection
• There is no BEST drug or combination of drugs for preoperative medication
• The specific drugs selected are based on the goals of premedication balanced with the potential side effects these drugs may produce

Preoperative Medications
• Benzodiazepines• Act on GABA receptors to produce selective
anxiolysis at doses that do not produce excessive sedation, depression of ventilation, or adverse cardiac effects• Note: May lead to any of the above when
given with opioids
• Opioids• Should be used when there is a need to
provide analgesia

Preoperative MedicationsContinued
• Antiemetics• Administered in the preOp or intraOp period as
prophylaxis against PONV• Droperidol (Black-Boxed), Reglan (? Antiemetic), 5HT3
inhibitors, Decadron, Scopolamine patch (apply several hours before induction of anesthesia)
• Drugs used to alter gastric volume/pH• Clinically significant pulmonary aspiration of gastric
fluid is rare in healthy patients undergoing elective surgery, maintenance of a patent airway is more important than routine pharmacologic prophylaxis
• Use in patients with specific indications

What has changed about your plan?
• Airway• Medications• Trends of Vital Signs

Pre-Operative Cardiac Evaluation

Cardiovascular Disease
• During a lifetime, a heart contracts more than 4 billion times – To support the active cardiac state, the
heart supplies more than 4 million liters of blood to the myocardium and more than 200 million liters to the systemic circulation
• Cardiac output can vary from 3 L/min to 30 L/min depending on activity level – Regional blood flow can vary up to 200%

Cardiovascular DiseaseMajor Disease Categories
• Coronary heart disease (CHD/CAD)• Hypertension (HTN)
• Rheumatic heart disease (RHD)• Bacterial endocarditis• Congenital heart disease

Coronary Heart Disease
• Leading cause of death in the United States
• Around 1 million deaths per year from cardiovascular pathology
• About ½ of these related to ischemic disease
• No. 1 cause of death among women in the U.S.
• Lifetime risk of death from CHD: 31%• Lifetime risk of death from breast CA: 2.8%

Coronary Heart DiseaseRisk Factors
• Past medical history• Chronic disorder
– Hypertension– Hyperlipidemia– Diabetes mellitus– Thyroid dysfunction
• Cardiac surgery• Rhythm disorder• Acute rheumatic fever

Coronary Heart DiseaseRisk Factors: Family History
• Diabetes mellitus• Heart disease• Hypertension• Congenital heart defects
– Particularly VSD
• Sudden death• Early age cardiovascular disease

Coronary Heart DiseaseRisk Factors: Social History
• Stressful or physical work• Tobacco use• Poor nutritional status• “High strung” personality• Lack of relaxing activities• Use of alcohol• Use of illegal drugs

Preoperative Clinical Evaluation
Identification of serious cardiac disorderCAD, CHF, ArrhythmiasInitial history, Physical examination, ECG
Define disease severity, stability, and prior treatmentFunctional capacityAgeComorbidities
DM, peripheral vascular disease, renal dysfunction, chronic pulmonary disease
Type of surgeryConsider higher risk
Vascular proceduresProlonged complicated thoracic, abdominal and head and neck
procedures

HypertensionManagement of Preoperative Cardiovascular Conditions
• Severe Htn(DBP >110mmHg) should be controlled before surgery when possible
• Continuation of preoperative antihypertensive treatment is critical to avoid severe postoperative hypertension.
• Consider the urgency of surgery and the potential benefit of more intensive medical therapy.

Valvular Heart DiseaseManagement of Preoperative Cardiovascular Conditions
• Symptomatic stenotic lesions (MS or AS): associated with risk of perioperative severe CHF or shock and often require percutaneous valvotomy or replacement to lower cardiac risk.
• Symptomatic regurgitant lesions (AR or MR): usually better tolerated perioperatively and may be stabilized before surgery with intensive medical therapy and monitoring

Myocardial Heart DiseaseManagement of Preoperative Cardiovascular Conditions
• Dilated and hypertrophic cardiomyopathy are associated with an increased incidence of perioperative CHF.
• Maximizing preoperative hemodynamic status and providing intensive postoperative medical therapy and surveillance.

Arrhythmias and Conduction AbnormalitiesManagement of Preoperative Cardiovascular Conditions
• Careful evaluation for underlying cardiopulmonary disease, drug toxicity, or metabolic abnormality.
• Therapy: reverse any underlying cause and treat the arrhythmia

Medical Therapy for Coronary Artery Disease
• If patients require β-blockers, calcium channel blockers, or nitrates before surgery, continue them into the operative and post-op period.
• The same is true for therapies used to control CHF
• β-blockers reduce postoperative ischemia– Protection against ischemia may also
reduce risk of MI

Cardiac Evaluation
• Clinical predictors
• Functional capacity
• Surgical risk
• Non-invasive testing
• Invasive testing

Method of Assessing Cardiac Risk
• Resting Left Ventricular Function
• Exercise Stress Testing
• Pharmacological Stress Testing
• Ambulatory EKG monitoring
• Coronary Angiography

Clinical Predictors of Increased Perioperative Cardiovascular Risk
(Myocardial Infarction, Congestive Heart Failure, Death)
• MinorAdvanced ageAbnormal EKG(LVH, LBBB, ST-T abnormalities)Rhythm other than sinus (eg, atrial fibrillation)Low functional capacity (eg, unstable to climb one flight of stairs
with a bag of groceries)History of strokeUncontrolled systemic hypertension
• IntermediateMild angina pectoris(Canadian Cardiovascular Society Class I or
II)Prior myocardial infarction by history or pathological wavesCompensated or prior CHFDiabetes mellitus

Clinical Predictors of Increased Perioperative Cardiovascular Risk
(Myocardial Infarction, Congestive Heart Failure, Death)
• MajorUnstable coronary syndromes– Recent myocardial infarction with evidence of important
ischemic risk by clinical symptoms or noninvasive study– Unstable or severe angina– Decompensated CHF
Significant arrhythmias– High grade atrioventricular block– Symptomatic ventricular arrhythmias in the presence of
underlying heart disease– Supraventricular arrhythmias with uncontrolled
ventricular rate
Severe valvular disease

Functional Capacity
1 MET1 MET Can you take care of yourself?Can you take care of yourself?
Can you eat, dress, or use the toilet?Can you eat, dress, or use the toilet?
Can you walk indoors around the house?Can you walk indoors around the house?
Can you walk a block or two on level ground at 2-3 mph?Can you walk a block or two on level ground at 2-3 mph?
Can you do light housework, such as dusting or washing dishes?Can you do light housework, such as dusting or washing dishes?
4 METs4 METs Can you climb a flight of stairs or walk up a hill?Can you climb a flight of stairs or walk up a hill?
Can you walk on level ground at 4 mph?Can you walk on level ground at 4 mph?
Can you run a short distance?Can you run a short distance?
Can you do heavy housework, such as scrubbing floors or lifting or moving Can you do heavy housework, such as scrubbing floors or lifting or moving heavy furniture?heavy furniture?
Do you participate in moderate recreational activities, such as golf, bowling, Do you participate in moderate recreational activities, such as golf, bowling, dancing, doubles tennis, or throwing a baseball or football?dancing, doubles tennis, or throwing a baseball or football?
>10 METs>10 METs Do you participate in strenuous sports, such as swimming, singles tennis, Do you participate in strenuous sports, such as swimming, singles tennis, football, basketball, or skiing?football, basketball, or skiing?

Surgical RiskLow Risk Procedures
• Low surgical risk:– Endoscopy– Bronchoscopy– Cystoscopy– Dermatologic procedures– Breast biopsy– Opthalmologic procedures

Surgical Risk
• Intermediate surgical risk:– Orthopedic surgery– Urologic surgery– Uncomplicated abdominal surgery– Uncomplicated head and neck

Surgical Risk
• High surgical risk:– Emergency surgery– Cardiac procedures– Aortic or vascular surgery– Anticipated prolonged surgery• Large fluid shifts or blood loss• Ex: Whipple, spinal surgery

ElectrocardiogramSignificant ECG Findings
• Past myocardial infarction• Left bundle branch block• Bifasicular block• Atrioventricular block –Mobitz-Type II or 3°AVB
• Prolonged QT interval• Right ventricular hypertrophy

Echocardiography
• Displays 2-dimensional ultrasound images of the heart
• Can be used to produce accurate assessment of the velocity of blood and cardiac tissue– Utilizes pulse wave Doppler ultrasound
• Diagnostic uses:– Wall motion abnormalities– Valvular dysfunction (valve area and function)– Septal defects– Calculation of cardiac output and ejection fraction

EchocardiographyTypes of Echocardiography
• Transthoracic (TTE)
• Exercise stress echo
• Dobutamine stress echo
• Transesophageal (TEE)

Stress Testing
• Used to evaluate myocardial perfusion during stress as compared to at rest
• Diagnostic usefulness debatable! • Types of evaluation:– Exercise (a.k.a. treadmill)– Dobutamine or adenosine– Radiotracer
• Tc99m Sestamibi (Cardiolite®)• Thallium

Cardiac Catheterization• Invasive angiography of myocardial
perfusion• Diagnostic usefulness:– Arterial occlusion– Thrombotic lesions– Aneurysmal enlargement
• Concurrent procedures:– Percutaneous transluminal coronary
angioplasty (PTCA)– Coronary artery stent placement– Dissection and stroke

Need for noncardiac
surgeryO.R.emergency
Postoperative risk stratification and
risk factor management
Urgent or elective
Coronary revascularization
within 5 yrs
Recurrent symptoms or
signs
Recent coronary
evaluation
Recent coronary angiogram or
stress test?
Intermediate
Clinical predictors
Major Minor or No
O.R.
yes
Unfavorable result and change in symptoms
Favorable result and no change in symptoms
no
no
yes
yes
no
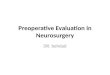
Stepwise Approach to Stepwise Approach to Preoperative Cardiac Preoperative Cardiac
AssessmentAssessment

Minor or no clinical predictors
Poor(<4METs) Moderate or excellent(>4METs)
High surgicalrisk procedure
Intermediatesurgical riskprocedure
Noninvasive testing O.R. Postoperative management
Subsequent care by findings and treatment results
Consider coronary angiography Minor clinical predictors:•Advanced age•Abnormal ECG•Rhythm other than sinus•Low functional capacity•History of stroke•Uncontrolled systemic hypertension
High risk
low risk
Stepwise Approach to Stepwise Approach to Preoperative Cardiac Preoperative Cardiac
AssessmentAssessment

Intermediate clinical predictors:•Mild angina pectoris•Prior MI•Compensated or prior CHF•DM
Intermediate clinical predictors
Poor(<4METs)
Moderate or excellent(>4METs)
High surgicalrisk procedure
Intermediate or lowsurgical procedure
Low surgicalrisk procedure
Noninvasivetesting
O.R. Postoperative risk stratificationand risk factor reduction
Consider coronaryangiography
Subsequent care dictated by findingsand treatment results
Low risk
High risk
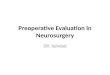
Stepwise Approach to Stepwise Approach to Preoperative Cardiac Preoperative Cardiac
AssessmentAssessment

Major clinical predictors:•Unstable coronary syndromes•Decompensated CHF•Significant arrhythmias•Severe valvular disease
Major clinical predictors
Delay or cancel noncardiac surgery
Medical managementand risk factor modification
Coronaryangiography
Subsequent care dictated by findingsand treatment results
Stepwise Approach to Stepwise Approach to Preoperative Cardiac Preoperative Cardiac
AssessmentAssessment

Summary
• How has the information gained in the pre-op evaluation changed your plan?
• Is there anything further that you need to deliver a safe anesthetic?
• Should you proceed with the case?• Don’t forget to monitor closely.• Have a back-up plan ready to
implement.
Recommended