4/23/2014
1
Healthier Patients, Improved Star RatingsWhat Medication Synchronization
Can Do for Your Patients and Your Pharmacy Business
Bri Morris, Pharm.D.Associate Director, Strategic Initiatives
National Community Pharmacists Association
Disclosures
Bri Morris is the Associate Director of Strategic Initiatives with NCPA. The conflict was resolved by peer review of the slide content.
Learning Objectives
• Describe how a ‘med sync’ program can improve patient outcomes and improve star ratings.
• Discuss how a ‘med sync’ program can positively affect pharmacy operations.
• Outline three staffing/workflow considerations needed to begin a ‘med sync’ program.
Questions We’ll Answer
• Why should I care about adherence?
• What’s in my ‘adherence toolbox’?
• What is medication synchronization?
• How can synchronization help my patients and my pharmacy?
• What resources are available to help me?
The $300 Billion Problem
For years, emphasis has been placed on the problem of medication non-adherence
$290 billion a year in direct and indirect costs
69% of medication-related hospital admissions due to poor adherence
75% of total health care spending on chronic disease
It’s Time for Pharmacy to Bring Solutions
• Transformation of health care delivery (quality vs. quantity)
• Government is recognizing financial value of medications
• Hospitals are being penalized for readmissions
• Result: Adherence is key part of Medicare plan ratings, ACOs, and other new payment models
4/23/2014
2
Adherence: Key Part of Part D Plan Ratings
• CMS developed 5-star ratingsystem to measure plans
• Ratings are posted on Plan Finder (www.medicare.gov)
Why Plans Care About Star Ratings
• Five-star plans receive:
High-performing icon
Special Enrollment Period
• Medicare Advantage plans can earn Quality Bonus Payments (QBPs)
Note: Does not apply to stand-alone PDPs
Star Ratings: Background
• Average Star Rating for PDPs: 2013: ~3.30
2014: 3.07
• 39 Medicare contracts have been identified
as ‘low performers’ Identified as 2.5 stars or less over the previous
3 years
Why does this matter to me?
Star Ratings: Background
How will PDPs and MA-PDP plans raise
their Star Ratings?
Choose pharmacies that are committed to
improving Star Ratings measures to be a
part of their network, offer them
incentives, etc.
What will happen to pharmacies who don’t
meet this challenge?
Payers Focus Areas
• High risk medications
• Diabetes patients taking ACE/ARB’s
• Adherence
– Oral diabetes medications
– Hypertension (RAS antagonists)
– Cholesterol (statins)
Roebuck MC, Liberman JN, Gemmill-Toyama M, Brennan TA. Medication adherence leads to lower health care use and costs despite increased drug spending. Health Affairs 2011;30(1):91-99.
Medications Confirmed as Cost Saver
Studies show that increased pharmacy spending results in fewer hospitalizations and lower health care costs
Congestive Heart Failure: 8.4 to 1 ROI
Diabetes: 6.7 to 1 ROI
Hypertension: 10.1 to 1 ROI
Dyslipidemia: 3.1 to 1
4/23/2014
3
Spend a Little—Save a Lot
Congressional Budget Office estimates that a 1 percent increase in the number of prescriptions filled would cause Medicare’s spending on medical services to fall by roughly 0.2%
That’s savings of
$1.7 billion
Offsetting Effects of Prescription Drug Use on Medicare’s Spending for Medical Services. Congressional Budget Office. November 2012.
More trips here…
…can mean fewer visits here.
Why Community Pharmacists?
• Trusted medication experts
• Most accessible provider in community
• Key touch point throughout continuum of care
• Last health care professional seen by patient before medications are taken
• Patient’s connectedness with pharmacy is the leading predictor of adherence1
Medication Adherence in America: A National Report Card. National Community Pharmacists Association. April 2013. www.ncpanet.org/reportcard
Align
• Adherence– First fill counseling
– Utilize pharmacy reminder systems, such as calling programs
• Utilize ways to improve outcomes during the hospital discharge process
Key Point: First fill counseling is the key to adherence improvement.
Clinical and Business Case
• Chronic care patients need you…and you
need them
– Diabetes patients spend $4,500-$12,000
annually per year (top 1% spends $28,000 in
the pharmacy)
• As you align your pharmacy with quality
measures, there are additional revenue-
producing opportunities to be found
What’s In Your Adherence Toolkit?
Adherence Services
Adherence counseling (first fill, etc.) 48%
Compliance packaging 41%
Synchronized refills 39%
Refill reminders (phone or text) 39%
Motivational interviewing 13%
Source: 2013 NCPA Digest, sponsored by Cardinal Health
What Is Medication Synchronization?
Medication Synchronization:
Coordinating all of a patient’s prescription medications to be filled on the same date each month
4/23/2014
4
Medication Synchronization Is Not Auto Refill
AutomaticRefills
SynchronizedRefills
Patients receive a monthly call from their pharmacy to discuss their medications and answer any questions about dosing instructions and/or potential side effects.
No Yes
Pharmacy confirms whether patients need each medication before dispensing it.
No Yes
Pharmacy asks patients about any recent physician visits or hospitalizations that may have resulted in a new medication or change in therapy.
No Yes
Patients opt in to receiving this service. Not always Yes
Patients have the option to pick up their medications from their local community pharmacy.
Not always Yes
Synchronization: Win-Win-Win
• Improves patient care by:
Reducing gaps between refills
Providing mechanisms to identify non-adherence
Reducing medication-related hospital readmissions
• Improves pharmacy operations by:
Resulting in more prescriptions filled
Changing dispensing function from reactive to proactive
Synchronization Improves Pharmacy Ops
What you can expect:
Streamlined workflow
Predictable workload
Decreased delivery runs
Better inventory control
More time for other pharmacy services
Professional satisfaction
Loyal patients
Healthier bottom line
What you won’t miss:
“Manic Mondays”
Frequent flyers
Last-minute refill requests on Friday afternoons or before holidays
Reversing for “no shows”
Patients running out of pills
• Floating
• IOUs
Allows You to Work Smarter, Not Harder
• Improved inventory control
Just-in-time ordering
Increased velocity: 12 to 36x/yr
Better cash flow
• Improved bottom line
Increased prescription volume (30%)
Reduced pharmacist hours (10 hrs/week)
Reduced delivery costs
Opportunities for add-on sales (OTC, etc.)
Implementing Medication Synchronization
• Start-up procedures
• Refill synchronization process
• Ongoing program operations
Getting Started
• Choose a program manager Dedicate a staff member tasked with coordinating
the program• Lead technician may be a good candidate
Will be pulling patient files, calling the patient to discuss and review medications, and making notes for the pharmacist
• Organizational skills are important
• Should have solid understanding of medications
• Determine program procedures/protocols
• Engage staff
4/23/2014
5
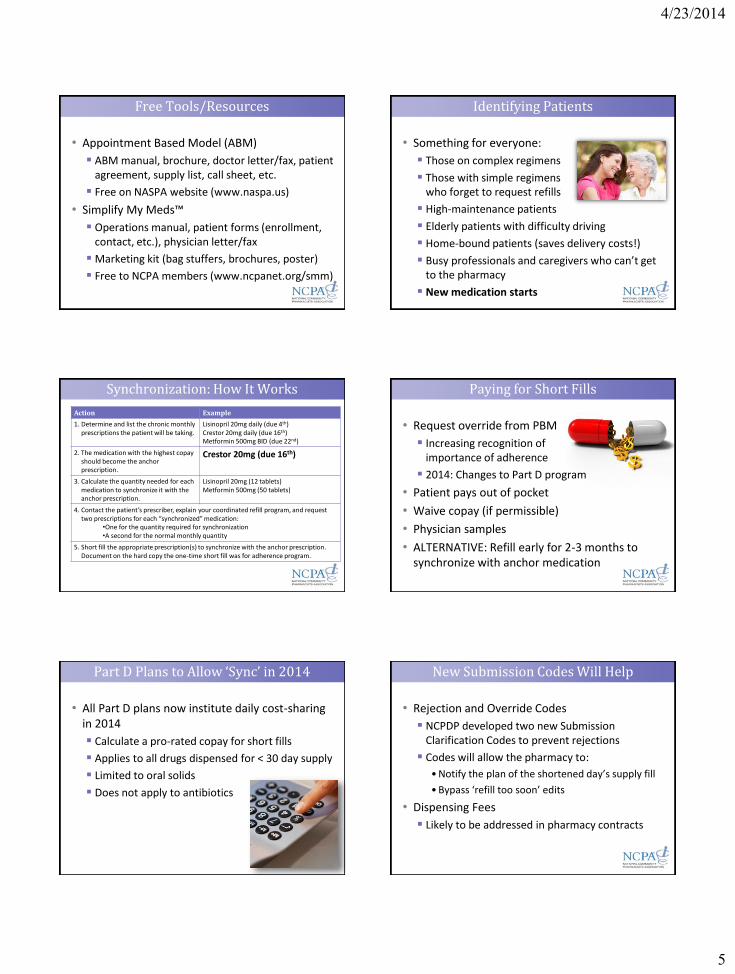
Free Tools/Resources
• Appointment Based Model (ABM)
ABM manual, brochure, doctor letter/fax, patient agreement, supply list, call sheet, etc.
Free on NASPA website (www.naspa.us)
• Simplify My Meds™
Operations manual, patient forms (enrollment, contact, etc.), physician letter/fax
Marketing kit (bag stuffers, brochures, poster)
Free to NCPA members (www.ncpanet.org/smm)
Identifying Patients
• Something for everyone:
Those on complex regimens
Those with simple regimens who forget to request refills
High-maintenance patients
Elderly patients with difficulty driving
Home-bound patients (saves delivery costs!)
Busy professionals and caregivers who can’t get to the pharmacy
New medication starts
Synchronization: How It Works
Action Example
1. Determine and list the chronic monthly prescriptions the patient will be taking.
Lisinopril 20mg daily (due 4th)Crestor 20mg daily (due 16th)Metformin 500mg BID (due 22nd)
2. The medication with the highest copay should become the anchor prescription.
Crestor 20mg (due 16th)
3. Calculate the quantity needed for each medication to synchronize it with the anchor prescription.
Lisinopril 20mg (12 tablets)Metformin 500mg (50 tablets)
4. Contact the patient’s prescriber, explain your coordinated refill program, and request two prescriptions for each “synchronized” medication:
•One for the quantity required for synchronization•A second for the normal monthly quantity
5. Short fill the appropriate prescription(s) to synchronize with the anchor prescription. Document on the hard copy the one-time short fill was for adherence program.
Paying for Short Fills
• Request override from PBM
Increasing recognition of importance of adherence
2014: Changes to Part D program
• Patient pays out of pocket
• Waive copay (if permissible)
• Physician samples
• ALTERNATIVE: Refill early for 2-3 months to synchronize with anchor medication
Part D Plans to Allow ‘Sync’ in 2014
• All Part D plans now institute daily cost-sharing in 2014
Calculate a pro-rated copay for short fills
Applies to all drugs dispensed for < 30 day supply
Limited to oral solids
Does not apply to antibiotics
New Submission Codes Will Help
• Rejection and Override Codes
NCPDP developed two new Submission Clarification Codes to prevent rejections
Codes will allow the pharmacy to:
• Notify the plan of the shortened day’s supply fill
• Bypass ‘refill too soon’ edits
• Dispensing Fees
Likely to be addressed in pharmacy contracts
4/23/2014
6
Program Mechanics
• 7 Days Prior
Pull patient files 7 days ahead of their refill date
Call patient to review meds; ask about recent hospitalizations/physician visits
• 3-7 Days Prior
Review for prescriptions with zero refills
Update the patient profile in the dispensing system
Final Fill Procedures
• 1-2 Days Prior
RPh reviews orders and resolves any clinical issues identified by the program manager
Review inventory/order products
Dispense product(s)
Call and remind patient to pick up prescriptions
Tips from the Experts
• Designate a technician to run the daily operations
• Leverage your software
Identify non-adherent patients
Group patients by ‘sync’ date
Reports to help with patient calls
• Test it out with 5-10 patients first
• Engage your front-line staff (they’re your best marketers!)
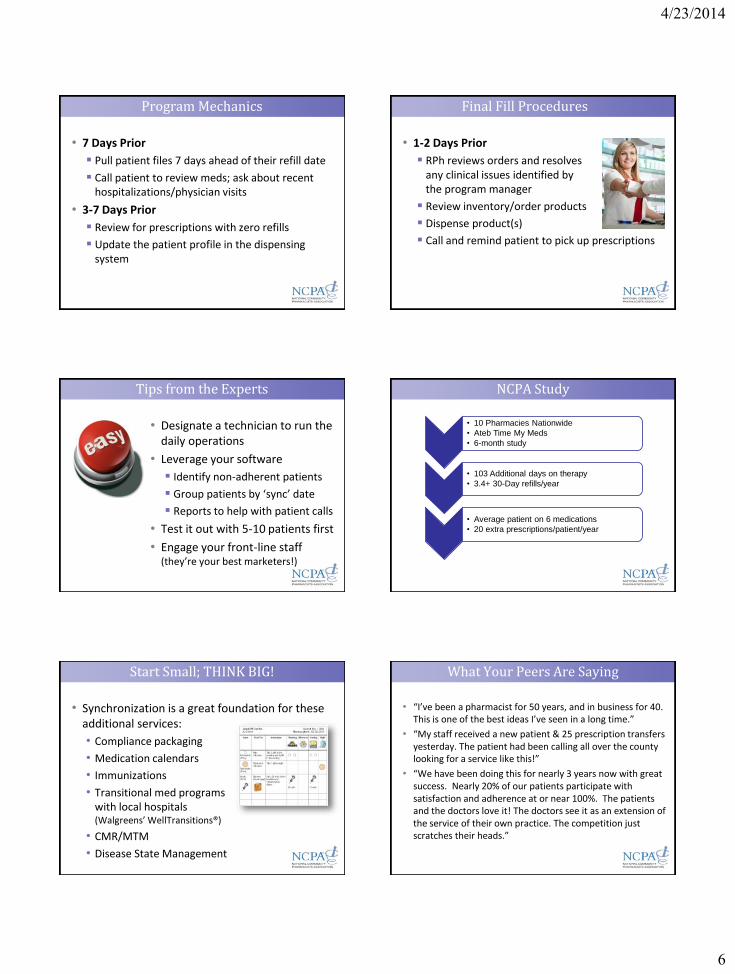
NCPA Study
• 10 Pharmacies Nationwide
• Ateb Time My Meds
• 6-month study
• 103 Additional days on therapy
• 3.4+ 30-Day refills/year
• Average patient on 6 medications
• 20 extra prescriptions/patient/year
Start Small; THINK BIG!
• Synchronization is a great foundation for these additional services:
• Compliance packaging
• Medication calendars
• Immunizations
• Transitional med programs with local hospitals (Walgreens’ WellTransitions®)
• CMR/MTM
• Disease State Management
What Your Peers Are Saying
• “I’ve been a pharmacist for 50 years, and in business for 40. This is one of the best ideas I’ve seen in a long time.”
• “My staff received a new patient & 25 prescription transfers yesterday. The patient had been calling all over the county looking for a service like this!”
• “We have been doing this for nearly 3 years now with great success. Nearly 20% of our patients participate with satisfaction and adherence at or near 100%. The patients and the doctors love it! The doctors see it as an extension of the service of their own practice. The competition just scratches their heads.”

4/23/2014
7
Questions?
Bri Morris, Pharm.D.Associate Director, Strategic InitiativesNational Community Pharmacists Assn.Tel: (703) 838-2689 [email protected]
Recommended

















